
Abstract
In this work, we discovered a new phenomenon—asymptomatic COVID-19 infection, or covert case, during the pandemic. All the 3 patients had a history of exposure, with no symptoms, and no abnormalities were found in computed tomography scan or lab tests. Except for case 2, the other patients’ severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) nucleic acid tests were negative. But their anti-SARS-COV-2 nucleocapsid antibody showed a dynamic trend, consistent with the process of virus infection and clearance. A growing number of asymptomatic or covert cases need more attention. Lack of surveillance may lead to another outbreak. We hope to demonstrate our cases to attract the attention of governments or health authorities that covert cases should be the focus as well.
Introduction
The coronavirus disease 2019 (COVID-19) is a pandemic caused by the novel coronavirus (severe acute respiratory syndrome coronavirus 2 [SARS-COV-2]) 1,2 . Despite the rapid increase in confirmed cases, there are still a large number of people with mild or no symptoms that are being neglected by the government. Some of the first detailed estimates of these covert cases suggest that they could represent 60% of all infections, but the extent of the phenomenon and its role in virus transmission are currently unclear. In our practice, we identified 3 close contact cases with no symptoms, no change in chest computed tomography (CT) scan, 2 negative and 1 positive reverse transcription-polymerase chain reaction (RT-PCR) results for SARS-COV-2 nucleic acid, and protective IgG antibodies.
Case Report
Human samples were collected by Hubei 672 Orthopaedics Hospital of Integrated Chinese & Western Medicine, the designated hospital for emergent infectious diseases, with the consent of all patients and approval of the ethics committee of the hospital.
Case 1 was a 39-year-old woman who had close contact with a COVID-19 patient and was sent to the designated hotel for self-isolation on February 9. She was tested negative for SARS-COV-2 nucleic acid by 3 RT-PCR tests on February 11, February 14, and March 4 and showed normal chest CT results. She was subsequently tested for anti-SARS-COV-2 nucleocapsid antibody by ELISA on March 4, and the result was IgM+− and IgG+−. A week later, the case was admitted to Hubei 672 Orthopaedics Hospital of Integrated Chinese & Western Medicine, which is a hospital designated for emergent infectious diseases, for further examination. During the isolation period, she reported no signs of discomfort, fever, shortness of breath, fatigue, or diarrhea. Her vital signs, blood, physical examination, and chest CT results were all normal. The only changes we observed were the seroconversion from IgM+− to IgM− and from IgG+− to IgG+ within a week.
Case 2 was a 31-year-old man who had close contact with a COVID-19 patient and was sent to the designated hotel for self-isolation on February 9. He was tested positive for SARS-COV-2 nucleic acid by RT-PCR on February 11 but was tested negative for SARS-COV-2 nucleic acid on the subsequent 4 tests on February 15, February 17, February 22, and March 3. His chest CT results on February 11 were also normal. He was subsequently tested for anti-SARS-COV-2 nucleocapsid antibody by ELISA on March 3, and the result was IgM+− and IgG+−. Eight days later, he was admitted to the Hubei 672 Orthopaedics Hospital of Integrated Chinese & Western Medicine for further examination. During the isolation period, he reported no signs of discomfort, fever, shortness of breath, fatigue, or diarrhea. His vital signs, blood, physical examination, and chest CT results were all normal. The only changes we observed were the seroconversion from IgM+− to IgM− and from IgG+− to IgG++ within 9 days.
Case 3 was a 6-year-old boy who had close contact with a COVID-19 patient and was sent to the designated hotel for self-isolation on February 12. He was tested negative for SARS-COV-2 by 3 RT-PCR tests on February 17, February 20, and March 3. He was subsequently tested for anti-SARS-COV-2 nucleocapsid antibody by ELISA on March 5, and the result was IgM+ and IgG+. Six days later, he was admitted to Hubei 672 Orthopaedics Hospital of Integrated Chinese & Western Medicine for further examination. During the isolation period, he reported no signs of discomfort, fever, shortness of breath, fatigue, nor diarrhea. His vital signs, blood, physical examination, and chest CT results were all normal. The only changes we observed were the seroconversion from IgM+ to IgM− and from IgG+ to IgG+++ within a week.
The lab test results of all 3 cases were within the normal range (Table 1).
Clinical Characteristics of Asymptomatic Coronavirus Disease 2019.
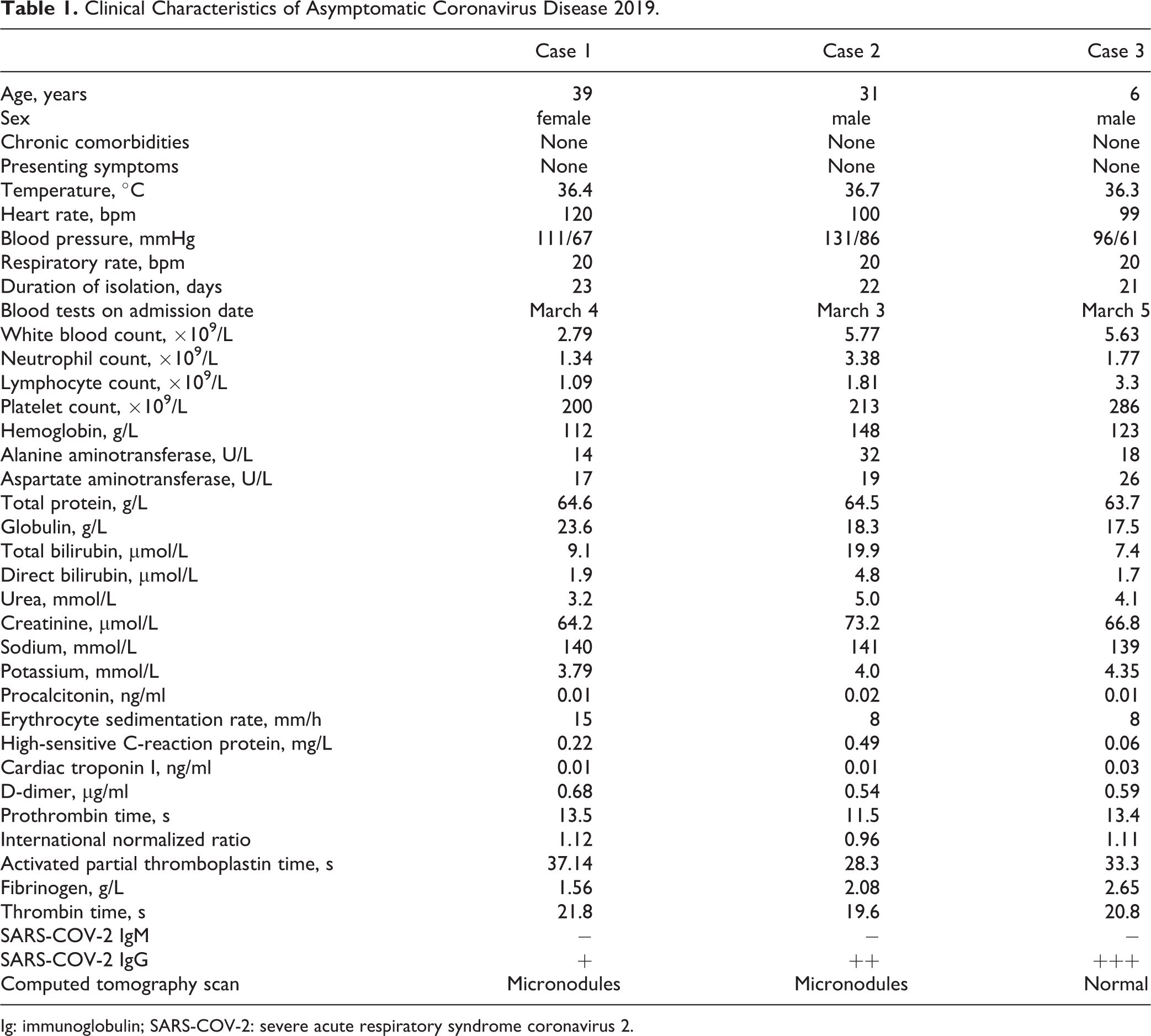
Ig: immunoglobulin; SARS-COV-2: severe acute respiratory syndrome coronavirus 2.
Discussion
As more understanding of the pandemic COVID-19, the control measures should be more prudent. In China, most close contact people were sent to designated hotels for self-isolation and medical observation. Once symptoms appeared or lab tests showed an abnormality, they were transferred to the designated hospital.
The 3 cases in our study were among those people mentioned above, which demonstrate that not all people exposed to SARS-CoV-2 are infected and not all infected patients develop into severe respiratory illness. Clinically, SARS-CoV-2 infection can be roughly divided into 3 stages: stage I, asymptomatic incubation period with or without detectable virus; stage II, symptomatic period with the presence of virus; and stage III, a convalescent period with virus elimination (Fig. 1). Therefore, patients with stage II COVID-19 may only be the tip of the iceberg. In fact, scientists and physicians have found increasing evidence that asymptomatic virus carriers or covert cases may seed another outbreak.
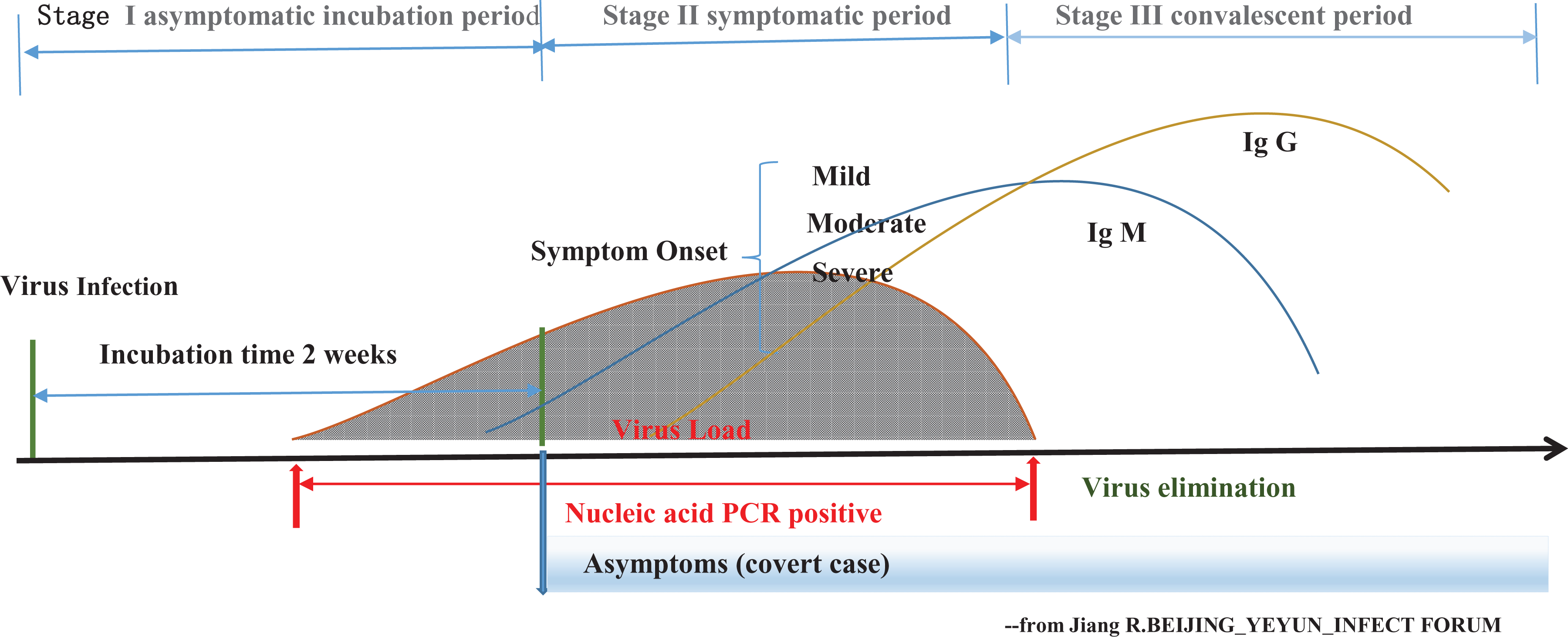
The outcomes of coronavirus disease 2019 (COVID-19) infection. The disease can be divided into 3 stages: Stage I, severe acute respiratory syndrome coronavirus 2infection with no symptoms, clinically will last for 2 weeks as the incubation period. Stage II, the virus colonized in the respiratory tract through droplets, aerosol, etc. With the increase in the viral load, some people show symptoms such as fever, cough, fatigue, myalgia, etc., who then COVID-19 diagnosis is confirmed by a positive nucleic acid polymerase chain reaction (PCR) test. Their condition maybe mild (need no treatment), moderate (need a hospital care), and severe or even critical (need an intensive care unit care). Another group of people also confirmed by a positive nucleic acid PCR test with no symptoms called covert cases. Stage III, the immune system may produce antibody during the process of virus’s elimination. The titer of immunoglobulin (Ig)G increased, while IgM decreased during the convalescent period.
The best-documented evidence for asymptomatic cases is probably that from the Diamond Princess cruise ship, which had a COVID-19 outbreak in early February while in Japanese waters. The ship was quarantined and the 3711 passengers and crew members were repeatedly tested and closely monitored. About 18% of the 700 infected individuals on Diamond Princess never showed symptoms 3 . Another study looked at 565 Japanese citizens who were evacuated from Wuhan in early February and were repeatedly tested and monitored for the virus and symptoms. A team in Japan reported that of the 13 evacuees who were infected, 4 (31%) never developed symptoms 4 .
The frequency of asymptomatic infection is estimated to be 18%-31%, and even up to 59% in reality 5 as the virus is undetectable in most people. Woelfel et al. reported efficient transmission of SARS-COV-2 through active pharyngeal viral shedding at a time at which symptoms are still mild, which means that the virus could shed and be disseminated by coughing or sneezing to the vulnerable without awareness 6 .
According to the epidemic characteristics, those who get close contact with confirmed cases should be high-risk exposure cases. And high-risk exposure cases with positive PCR and/or serum IgM and IgG should be considered confirmed cases 7 . Our 3 cases’ epidemic characteristics were shown in Fig. 2, all of them with no symptoms and had a specific antibody seroconversion. Except for the second case, all PCRs remained negative for the rest of the patients. So serological testing may be helpful for the diagnosis of suspected patients with negative RT-PCR results and for the identification of asymptomatic infections 8 .
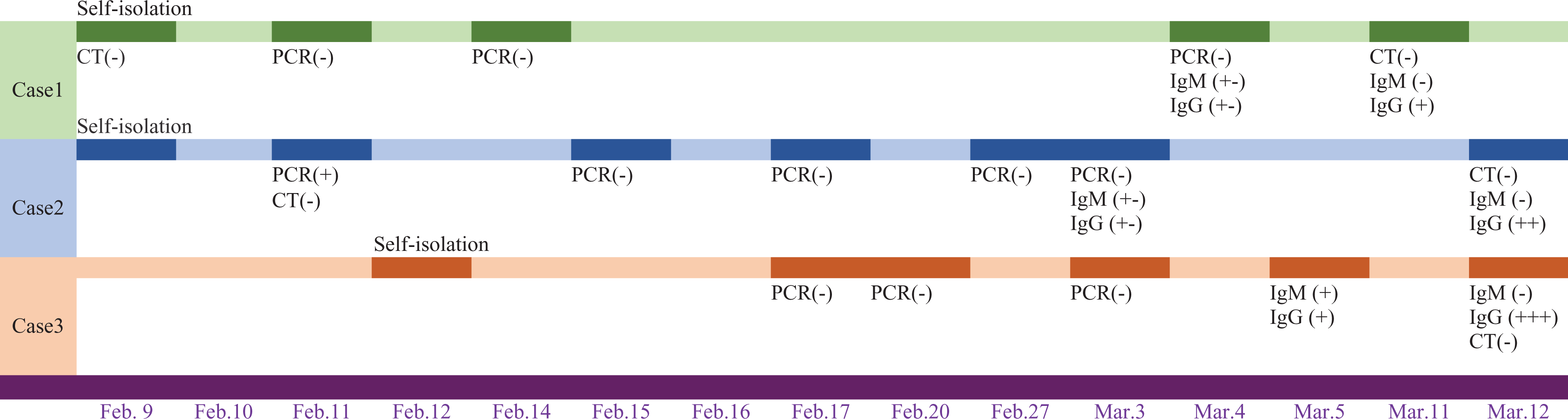
Timeline of lab test of covert cases.
Our findings clearly demonstrate that the RNA-based tests that are currently used in tens of thousands of patients are not enough to rule out the diagnosis of COVID-19 infection. We also need to test the blood for anti-SARS-CoV-2 antibodies as such a test can detect active and past infections (table 2) as well. Fatima et al. developed a biosafety level (BSL)2 ELISA test for measuring anti-SARS-CoV-2 antibodies without cross-reactivity with alphacoronaviruses NL63 and 229E as well as the betacoronaviruses OC43 and HKU1. Of note, screening sera using this assay is faster and easier than performing standard neutralization assays in BSL3 containment laboratories 9 . Combination of both PCR and ELISA tests will help us identify more covert cases and provide more information about this burgeoning pandemic.
Clinical Situation of Asymptomatic Coronavirus Disease 2019 with Serum Antibody Test.

In conclusion, covert COVID-19 cases are those who show no symptoms such as fever, cough, and sore throat but are tested positive for SARS-COV-2 nucleic acid by PCR from their respiratory swab specimens and/or serum antibody IgM and IgG. These individuals should be isolated and observed for 14 days (incubation time). During the time, some may show no symptoms at all, while others may develop clinical symptoms later. We should take a very cautious approach under the following situations: (1) close contacts with COVID-19 during medical observation; (2) cluster outbreaks during investigation; (3) exposure to groups of people during contact tracing; and (4) travelers from pandemic hotspots. The covert cases have high transmission risks; however, they cannot be easily discovered by just 1 RT-PCR test. A total of 2147 close contacts were tracked and investigated in Ningbo, Zhejiang, China. The total infection rate was 6.15%, among whom were 22.31% friends, 18.0% family members, and 4.73% relatives. Living with the case (13.26%), taking the same transportation (11.91%), and eating together (7.18%) are high risk factors for infection 10 .
There are several reasons for the difficulty in identifying infected individuals. First, the disease may not trigger any symptoms in some individuals, making them difficult to be identified. Second, the symptoms are subjective and most individuals with mild infections would not be ill enough to seek medical help and would probably slip past screening procedures such as temperature checks. Third, the RT-PCR test has several limitations and cannot cover all covert cases. Therefore, we should modify the prevention plan, expand the screening coverage, and enhance the guidance to adopt a serum antibody test as a supplement to the diagnostic criteria. Individuals should maintain good hand hygiene, wash hands frequently, avoid touching the face, keep social distance, and wear masks. Any person feeling unwell should stay home and follow the instructions provided by the local health authorities.
Footnotes
Author Contributions
HT contributed to the data analysis and interpretation and writing draft.
LX and DX contributed to information and data collection. YL and YQ contributed to editing the manuscript.
Ethical Approval
Ethical approval to report this case was obtained from Hubei 672 Orthopaedics Hospital of Integrated Chinese & Western Medicine OF ETHICS COMMITTEE (APPROVAL ID 20200326).
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the special fund for novel coronavirus pneumonia from the Science and Technology Department, Hubei province (Grant No. 2020FCA035) and the COVID-19 Prompt Response Research Special Project from Huazhong University of Science and Technology (Grant No. 2020kfyXGYJ023).The funding sources had no role in the study design, data collection, analysis, interpretation, or writing of the paper.