
Abstract
This study aimed to compare the efficacy of allogeneic stem cell transplantation (allo-SCT) versus autologous SCT (auto-SCT) in patients with relapsed or refractory B-cell non-Hodgkin lymphoma (B-NHL). Medline, CENTRAL, and EMBASE databases through December 31, 2019 were searched. The primary endpoints were overall survival (OS) and progression-free survival (PFS) rates. The secondary outcomes include transplant-related mortality (TRM), event-free survival, relapse/or progression, and nonrelapse mortality (NRM). The 18 retrospective studies enrolled 8,058 B-NHL patients (allo-SCT = 1,204; auto-SCT = 6,854). The OS was significantly higher in patients receiving auto-SCT than allo-SCT (pooled odds ratio [OR]: 1.69, 95% confidence interval [CI]: 1.29 to 2.22, P < 0.001), but no significant difference was found in PFS (pooled OR: 0.98, 95% CI: 0.69 to 1.38, P = 0.891). Auto-SCT patients also had lower TRM and NRM (TRM: OR = 0.23, P < 0.001; NRM: OR = 0.16, P < 0.001), but higher relapse or progression rate (OR = 2.37, P < 0.001) than allo-SCT patients. Subgroup analysis performed for different grades and subtypes of B-NHL showed higher OS in auto-SCT patients with high-grade B-NHL and diffused large B-cell lymphoma (DLBCL). There was, nevertheless, higher PFS in allo-SCT patients with low-grade B-NHL and follicular lymphoma (FL), and lower PFS in allo-SCT patients with DLBCL than their auto-SCT counterparts. In conclusion, the meta-analysis demonstrated that relapsed or refractory B-NHL patients who received auto-SCT have improved OS than those treated with allo-SCT, especially among those with DLBCL, but lower PFS among those with FL. However, the study is limited by a lack of randomized trials, patients’ heterogeneity, and possible selection bias.
Introduction
Data from global studies of cancer (GLOBOCAN) indicate that non-Hodgkin lymphoma (NHL) is among the most common of all cancer types. Over 385,000 NHL incident cases and nearly 200,000 NHL deaths were reported globally in 2012 1 . Men generally have higher rates of NHL than do women, both in developed and underdeveloped countries 1,2 . B-cell non-Hodgkin lymphoma (B-NHL) is the largest group of NHL with many subtypes ranging from aggressive diffused large B-cell lymphoma (DLBCL) to more indolent follicular lymphoma (FL), and outcomes of treatments for B-NHL vary widely due to many subtypes and possible patient comorbidities. Patients who were refractory to initial treatments may have a poor outcome even after getting salvage chemotherapy. Relapse also remains a significant issue, as patients with recurrent or relapsed B-NHL are generally considered incurable with conventional chemotherapy. For these patients, hematopoietic stem cell transplantation (SCT) has the potential to improve the prognosis.
Autologous SCT (auto-SCT) and allogeneic SCT (allo-SCT) have been used for several decades to treat patients with hematological malignancies 3 –5 , and both types of SCT have been shown to improve survival 6 . Auto-SCT is generally regarded as less likely to prevent relapse than allo-SCT; however, allo-SCT can result in higher rates of transplant-related mortality (TRM) 7,8 . This difference may explain why use of allo-SCT lags behind that of auto-SCT for B-NHL. Only 9% of all allo-SCTs registered with the European Society of Blood and Marrow Transplantation in 2011 were performed on patients with NHL, versus 30.3% for auto-SCT, and the total number of auto-SCTs to treat NHL was almost 5 times that of allo-SCT 9 . However, the EMBT survey did not collect or analyze data on the use of SCT specifically for relapsed or refractory NHL, and this gap in knowledge is reflected in the organization’s recent recommendations, in which neither auto- or allo-SCT is proposed as the standard of care for most types of refractory NHL 10 .
Currently, both auto-SCT and allo-SCT are used frequently to treat patients with B-NHL. However, evidence is lacking regarding which procedure is more suitable for patients with relapsed or refractory disease. The absence of evidence-based guidelines for treatment of relapsed and refractory B-NHL presents a challenge to physicians not only in Europe, but also worldwide. Therefore, the objective of this study was to compare the efficacy of allo- and auto-SCT in patients with relapsed or refractory B-NHL and evaluate outcomes in patients with different grades and subtypes of B-NHL.
Materials and Methods
Search Strategy
Relevant studies were identified by searching the Medline and the Cochrane Central Register of Controlled Trials (CENTRAL), and EMBASE databases through December 31, 2019 by using the following search terms: ([{autologous} AND stem cell transplantation] AND non-Hodgkin lymphoma) AND (relapsed OR refractory OR recurrent). The keywords were non-Hodgkin, transplantation, allogeneic stem cell, autologous, and relapse (Medline database) and “non-Hodgkin lymphoma,” transplantation, autologous, and allogeneic (CENTRAL, EMBASE database). The database search was supplemented by manual search of the reference lists of the included studies, performed by two independent reviewers. Identification of eligible studies was accomplished via a two-step process. First, the titles and abstracts of the citations identified in the database search were screened against the inclusion and exclusion criteria. Second, the full text was obtained for articles meeting the inclusion criteria. Reports of studies that met all of the inclusion criteria and none of the exclusion criteria were included in the meta-analysis. Studies were identified and reviewed by two independent reviewers. If there was uncertainty regarding eligibility, a third reviewer was consulted.
Selection Criteria
Studies included in the meta-analysis met all of the following inclusion criteria: (1) the study was a two- or multiple-arm prospective or retrospective study; (2) it enrolled patients with a pathologically confirmed diagnosis of NHL who were candidates for SCT due to a clinical status of relapsing or refractory disease; and (3) it compared auto-SCT to allo-SCT. A study was not included if it met any of the following exclusion criteria: (1) the results were published in a review, letter, comment, editorial, case report, proceeding, personal communication, or expert opinion; (2) the published results contained incomplete patient profiles or essential data; (3) it used a questionable diagnostic approach or cancer staging system; (4) the study enrolled patients who were submitted to allo-transplant after failure of auto-transplant; (5) the results were published in a language other than English or Chinese; (6) the published results contained no quantitative data; or (7) it was a single-arm study.
Outcome Measures
The primary clinical outcomes were overall survival (OS) and progression-free survival (PFS). The secondary clinical outcomes were treatment-related death or TRM, event-free survival (EFS), relapse/or progression, and nonrelapse mortality (NRM).
Data Extraction
Data were extracted from the included studies as follows: first author’s name, year of publication, study design, treatments, number of patients in each group, and patients’ demographic and clinical characteristics (age, sex, disease stage and status, tumor histology, and complete remission rate).
Quality Assessment
The quality of the included studies was assessed by using ROBINS-I tool (Risk Of Bias In Non-randomized Studies-of Interventions) 11 . This tool assesses six sources of bias related to study participation, study attrition, measurement of prognostic factors, measurement of and accounting for confounding factors, measurement of outcomes, and analysis. For each source of bias, quality is indicated by the level of agreement with a statement that describes overall quality. Agreement, disagreement, and uncertainty of agreement are indicated by “low risk” (green), “high risk” (red), or “unclear” (yellow) in a matrix of the included studies and the six domains. The quality of included studies was independently appraised by two reviewers; any disagreement was resolved by a third reviewer.
Statistical Analysis
Characteristics of all patients from studies included in the meta-analysis are summarized using numbers for categorical data and mean or median (range: min, max.) for age and other continuous variables. Results of clinical outcomes are summarized as percentage of patients within each outcome given follow-up times. Effect size was defined as the odds ratio (OR) for evaluating differences in clinical outcomes between allogeneic and autologous groups. For each individual study, an OR with 95% confidence interval (CI) was calculated and then derived for all studies combined (pooled effect). An OR >1 indicated that the autologous group was favored, meaning that patients in the autologous group had a higher rate than those in the allogeneic group; an OR <1 indicated that the allogeneic group was favored, meaning that patients in the allogeneic group had a higher rate than those in the autologous group; OR =1 indicated that the rate was similar in both autologous and allogeneic groups. A χ2-based test of homogeneity was performed, and Cochran’s Q inconsistency index and I2 statistic were determined. An I2 statistic >50% indicates that heterogeneity existed between the studies; therefore, a random-effects model (DerSimonian–Laird method) was calculated 12 . Otherwise, a fixed-effects model (Mantel–Haenszel method) was applied. A sensitivity analysis was carried out by using the “leave one-out” approach. Subgroup analysis was performed for patients with either high- or low-grade B-NHL and patients with either FL or DLBCL. All statistical assessments were considered significant if P <0.05. Publication bias was also assessed if the meta-analysis included more than 10 studies. The results are presented using a Funnel plot with t-statistics and one-tailed P-value based on the Egger’s test. All analyses were performed using Comprehensive Meta-Analysis statistical software, version 2.0 (Biostat, Englewood, NJ, USA).
Results
Study Selection and Characteristics
A flow chart for study selection is shown in Fig. 1. A search of Medline, CENTRAL, and EMBASE databases and a manual search yielded 356 citations after duplicates were removed, of which 301 studies were excluded based on the exclusion criteria. After screening the full texts of the 55 remaining articles against the inclusion and exclusion criteria, an additional 37 articles were excluded for the following reasons: the study did not compare auto-SCT to allo-SCT (29 studies), did not enroll patients with relapsing/refractory NHL (3 studies), were not for B-NHL (2 studies), or did not report the outcome of interest (3 studies). As a result, 18 articles were finally eligible for inclusion in this meta-analysis 13 –30 .
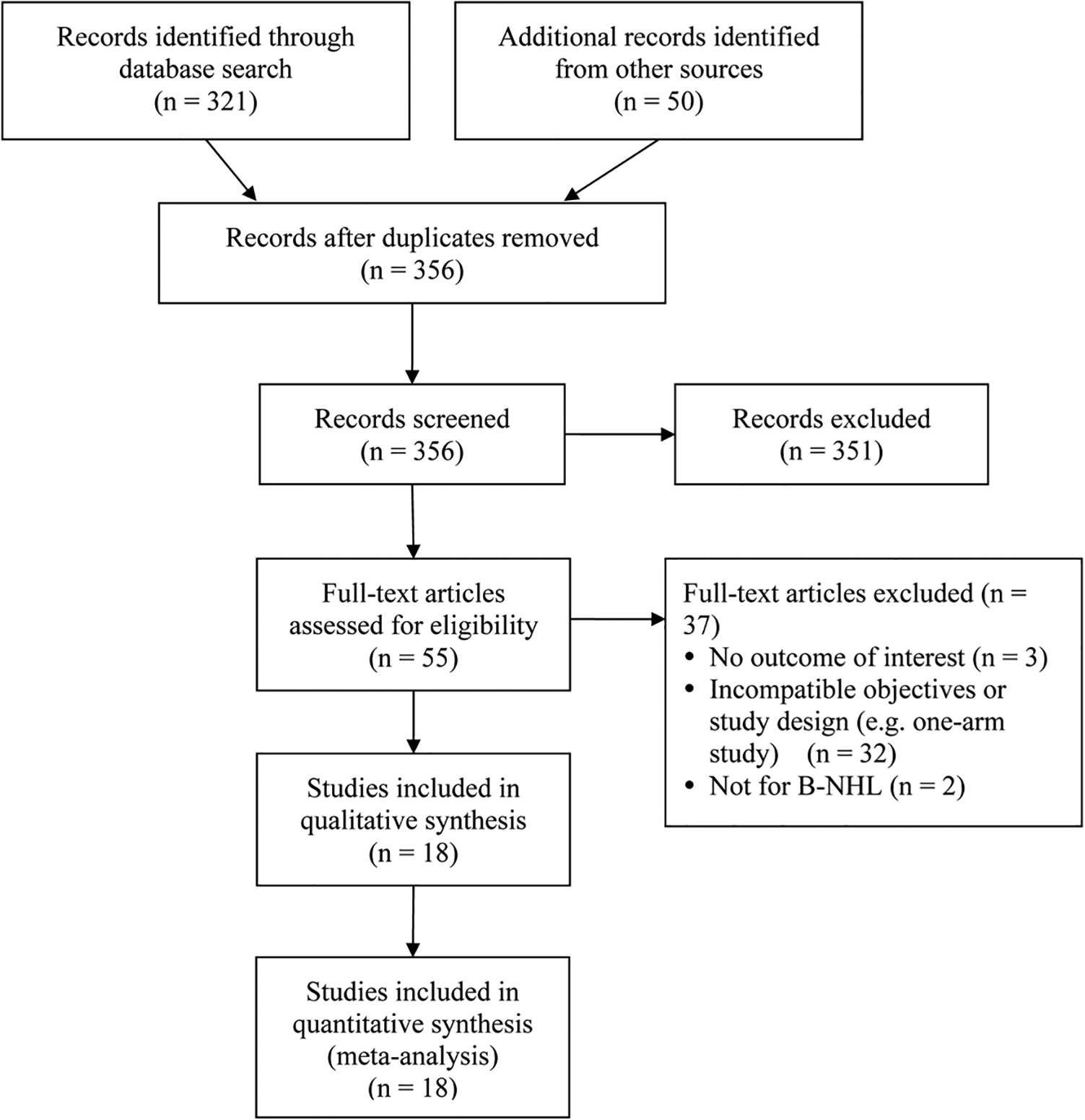
Flow diagram for study selection.
Characteristics of the included studies are summarized in Table 1. These studies enrolled a total of 8,058 patients, of which 6,854 underwent auto-SCT (size range of auto-SCT arm: 16 to 3,980 patients) and 1,204 allo-SCT (size range: 7 to 230 patients). Patients’ mean ages ranged from 11 to 60 years, and the proportion of men ranged from 39% to 81%. Three studies enrolled only patients with chemosensitive status for both types of SCT 18,22,23 , and the remaining studies had a mixed enrollment of patients with chemosensitive and chemoresistant status. Tumor histology was heterogeneous among the studies. Four studies included patients with low-grade non-Hodgkin lymphoma [B-cell FL 1 and FL 2] 16,23,26,27 , and six studies were designed for patients with high-grade non-Hodgkin lymphoma (two studies for transformed lymphoma, one study for grade 3 FL, three studies for diffuse large-cell lymphoma) 17,19,21,22,25,30 . The remaining five articles included a mixed population of low- and high-grade non-Hodgkin lymphoma. Rates of complete remission were better in general for patients in the auto-SCT arms (range, 26% to 73%) than for those in the allo-SCT arms (range, 2% to 56%). Median number of prior therapies and use of rituximab are included in Table 1; 12 studies with patients diagnosed as DLBCL using rituximab as part of therapy and 2 with some patients receiving rituximab. Median follow-up for survivors (range: 18 months to 6.7 years) is also included in Table 1. Clinical data and outcomes of analysis of the included studies are presented in Tables 2 and 3, respectively.
Summary of Patients’ Characteristics from Studies Included in Meta-Analysis.

AITL: angioimmunoblastic T-cell lymphoma; ALCL: anaplastic large-cell lymphoma; CRR: complete remission rate before or at transplantation; DLCL: diffuse large-cell lymphoma; EBMT registry: the European Bone Marrow Transplant registry; FCL: follicle center lymphoma; FL: follicular lymphoma; FM: follicular mixed small cleaved and large cell; FSC: follicular small cleaved cell; MAC: myeloablative conditioning; MSD/MUD: matched sibling/unrelated donor; NOS: not otherwise specified; PTCL: peripheral T-cell lymphoma; RIC: reduced-intensity conditioning; SCT: stem cell transplantation; SL/SLL: small lymphocytic lymphoma; TL: transformed lymphoma;
NA: not available; N: no; Y: yes.
† Median age.
* Pretransformation systemic regimens.
Summary of Clinical Outcomes in Studies Used for Meta-Analysis.

HCT: hematopoietic stem cell transplantation; MAC: myeloablative; MSD: matched sibling donor; MUD: matched unrelated donor; RIC: reduced-intensity conditioning; y: years.
Subgroup Analysis for All Clinical Outcomes.

CI: confidence interval; DLCL: diffuse large-cell lymphoma; FL: follicular lymphoma; B-NHL: B-cell non-Hodgkin lymphoma.
* Pooled effects are represented as odds ratios with corresponding 95% CI (lower, upper limits) and P-values.
Meta-Analysis
Seventeen studies that reported data for the primary outcome OS were included in the meta-analysis, the results of which are shown in a Forest plot in Fig. 2A 13 –27,29,30 . Cochran’s Q statistic and the I2 statistic indicated no significant study heterogeneity (Q statistic = 36.86, I2 = 56.59%; P = 0.002); therefore, a random-effects model was used. The pooled analysis found significant differences in OS between the two SCT groups (pooled OR: 1.69, 95% CI: 1.29 to 2.22, P < 0.001) (Fig. 2A). Subgroup analysis was performed for different grades and histological subtypes of B-NHL based on their clinical data (Table 2). The results of pooled-effects analysis revealed significant differences in OS between SCT groups for patients with high-grade B-NHL (pooled OR =1.61, 95% CI: 1.20 to 2.16, P = 0.001) and DLBCL (pooled OR = 2.12, 95% CI: 1.40 to 3.20, P < 0.001), respectively, and showed auto-SCT patients of both high-grade B-NHL and DLBCL had higher OS than allo-SCT (Table 3).
Thirteen studies 14,15,17 –19,21,23 –26,28 –30 with complete data of PFS were included for meta-analysis. A Forest plot illustrating the results is shown in Fig. 2B. Since the study heterogeneity was significant (Q statistic = 44.70, I2= 73.15%, P < 0.001), a random-effects model was used. The pooled estimate revealed no difference in PFS between the auto-SCT and allo-SCT groups (pooled OR: 0.98, 95% CI: 0.69 to 1.38, P = 0.891) (Fig. 2B). Subgroup analysis of the pooled effects revealed significant differences between the SCT groups for patients with low-grade B-NHL (pooled OR = 0.67, 95% CI: 0.48 to 0.92, P = 0.013), FL (pooled OR = 0.55, 95% CI: 0.32 to 0.96, P = 0.036) and DLBCL (pooled OR = 2.11, 95% CI: 1.28 to 3.46, P = 0.003), and showed allo-SCT patients of these groups having higher PFS than auto-SCT patients (Table 3).

Forest plot comparing (A) the OS rate, (B) the PFS rate, of participants receiving autologous stem cell transplantation (“autologous”) or allogeneic stem cell transplantation (“allogeneic”).
For secondary clinical outcomes, 5 studies had complete data on TRM, 5 on EFS, 14 on relapse/or progression, and 8 on NRM, (Table 2). Based on results of the heterogeneity test, the fixed-effects model was applied for TRM and NRM, and the random-effects model was applied for EFS and relapse/or progression (TRM: Q statistic = 6.03, I2= 33.65%, P = 0.197; NRM: Q statistic = 5.77, I2 = 0.0%, P = 0.567; EFS: Q statistic = 11.17, I2 = 64.2%, P = 0.025; relapse or progression: Q statistic = 64.04, I2 = 79.70%, P < 0.001). Results of pooled effect showed that patients in the autologous group had lower TRM and NRM rates than those in the allogeneic group (TRM: OR = 0.23, P < 0.001; NRM: OR = 0.16, P < 0.001). However, the relapse or progression rate was higher in the autologous group than that in the allogeneic group (OR = 2.37, P < 0.001) (Table 4). Subgroup analysis of B-NHL grades revealed that auto-SCT patients with high-grade B-NHL had lower NRM rates than those in the allo-SCT group (OR = 0.25, P < 0.001), while auto-SCT patients with low-grade B-NHL had a lower EFS rate (OR = 0.24, P = 0.007) but higher relapse or progression rates than those in the allo-SCT group (OR = 5.06, P = 0.001). Subgroup analysis of histological subtypes of B-NHL revealed that auto-SCT patients with DLBCL had lower TRM rates than those in the allo-SCT group (OR = 0.26, P < 0.001), and auto-SCT patients with FL had lower NRM rates than those in the allo-SCT group (OR = 0.11, P < 0.001) (Table 3).
Summary of Meta-analysis for Minor Clinical Outcomes.

Results are represented as odds ratios with corresponding 95% CI (lower, upper limits) and P-values.
CI: confidence interval.
Sensitivity Analysis
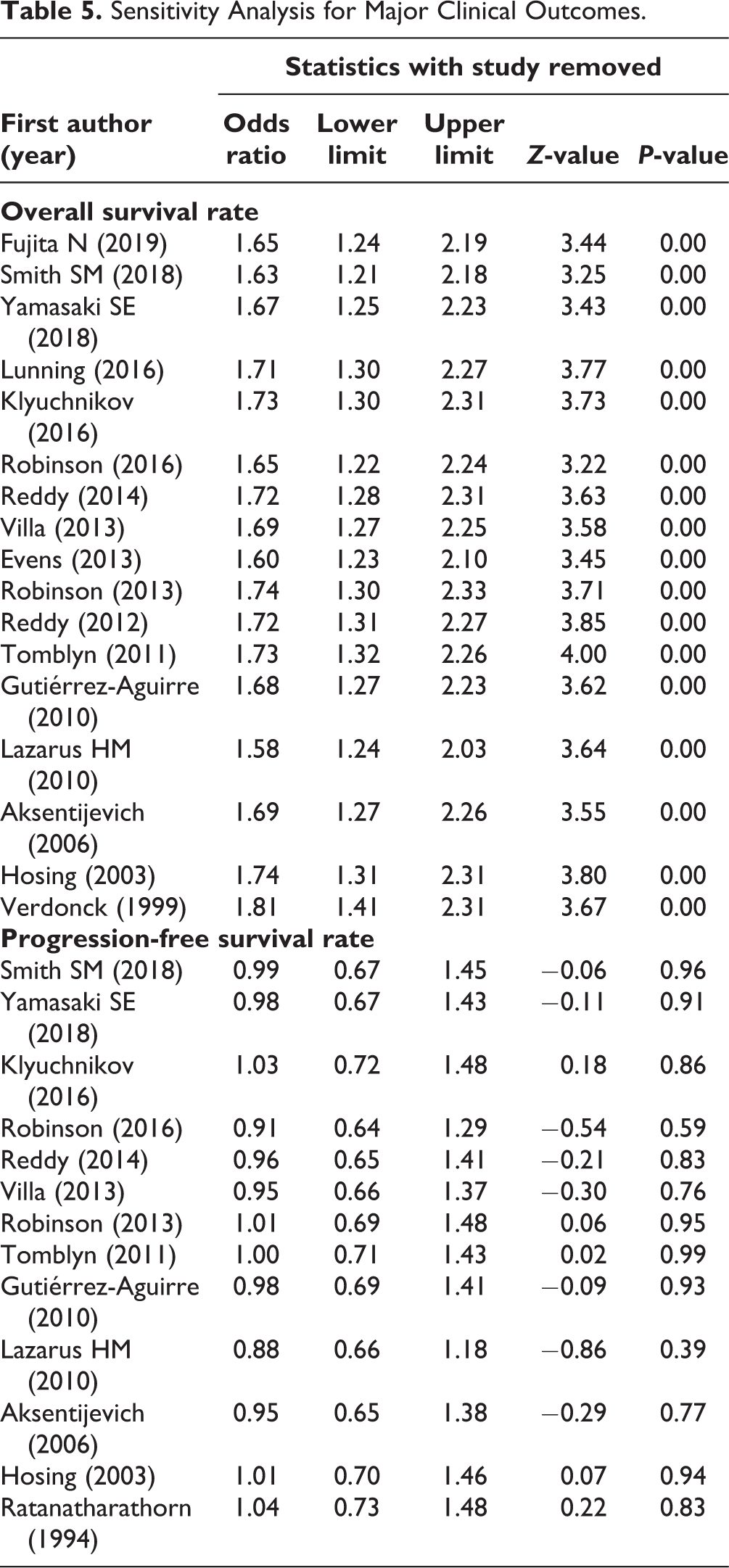
Sensitivity analysis was conducted for the primary clinical outcomes using the “leave-one-out” approach and results are shown in Table 5. The direction and magnitude of combined estimates for OS and PFS did not vary markedly with the removal of individual studies, indicating that no between-study heterogeneity was found among the included studies. Therefore, the meta-analysis for these outcomes had good reliability and the results were not overly influenced by individual studies.
Sensitivity Analysis for Major Clinical Outcomes.
Quality Assessment
Figure 3 shows the results of quality assessment of the included studies, which focused on six domains (study participation, study attrition, measurement of prognostic factors, measurement of and accounting for confounding factors, measurement of outcomes, and analysis). Overall, the study quality was excellent: 12 studies had the highest level of quality in all six domains, and the remaining three studies had two or less than two domains showing relatively high risk of bias (Fig. 3A). The least reported domain was “measurement and accounting of confounding factors,” which was lower than the highest quality in five studies (40%; Fig. 3B). Publication bias is presented using Funnel plot and the Egger’s test showed that no publication bias existed in the included studies (OS: t-statistic = 1.37, one-tailed P = 0.096; PFS: t-statistic = 0.75, one-tailed P = 0.235) (Fig. 4A, B).

Risk-of-bias assessment of the included studies. Quality assessments of each included study are summarized as the “risk of bias summary” (A). Green circles indicate that the factor was reported with low risk of bias; red circles indicate that the factor was reported with high risk of bias. The percentages of bias across all of the included studies are shown in a “risk of bias” graph (B).

Funnel plot with Egger’s test in publication bias analysis regarding the major outcomes, OS rate (A), and PFS rate (B).
Discussion
In this meta-analysis, which compared safety and efficacy of auto- and allo-SCT in relapsed or refractory B-NHL patients, results showed significant difference in OS between patients in the allo- and auto-SCT arms, but found no significant difference in PFS between the two groups. Also, subgroup analysis performed for patients with high- and low-grade B-NHL revealed no significant difference in OS between the auto-SCT and allo-SCT groups in patients with low-grade B-NHL but significant difference was found for PFS in those same patients. In addition, pooled subgroup analysis showed that the autologous group had lower TRM and NRM rates than those in the allogeneic group but higher relapse or progression rate in the autologous group. Furthermore, subgroup analysis of different B-NHL grades revealed that patients with high-grade B-NHL in the auto-SCT group had lower NRM rates than their allo-SCT counterparts, and patients with low-grade NHL in the auto-SCT group had lower EFS as well as higher relapse or progression rates than those in the allo-SCT group.
Despite recent therapeutic and diagnostic improvements, a significant fraction of FL patients still relapse, and the disease is considered incurable using various anticancer agents 31,32 . An expert panel recommended that auto-SCT could be used as salvage therapy for FL based on pre-rituximab data, but auto-SCT was not recommended as first-line treatment for most patients because it did not improve OS significantly 8 . Another study showed that allo-SCT mortality rates were lower in patients with sensitive disease 33 . In the present study, three of the four studies on low-grade NHL supported using allo-SCT to obtain a higher OS rate but reached significance in only one study 27 .
Auto-HCT is considered the standard-of-care curative option for aggressive B-NHL such as DLBCL and an important therapeutic option for indolent B-NHL such as FL, but for patients with high-risk features such as heavy pretreatment, relapsed/refractory disease, or failure after auto-HCT, allo-HCT remains the only curative option 34 . Those authors also advised that, at least in FL patients, auto-HCT is best reserved for relapsed chemosensitive patients after receiving prior chemo-immunotherapies, and who are also not candidates for allo-HCT because of donor unavailability, associated comorbidities, or patient preference 34 .
Transformed lymphoma is follicular low-grade (FL 1-2) lymphoma transformed into an intermediate (diffuse large B-cell; DLBCL) or a more aggressive (Burkitt) lymphoma and is known to carry a poor prognosis 19 . Two studies in the high-grade NHL group of our meta-analysis were designed for patients with transformed lymphoma 19,22 . Some patients with transformed lymphoma are treated with high-dose chemotherapy followed by auto- or allo-SCT 19 , and an expert panel in a US study recommended that auto-SCT could be used for transformed follicular lymphoma patients 8 . For patients with grade 3 FL, management follows guidelines for treating DLBCL 17 . Available data suggest that patients with FL3 undergoing SCT will have inferior survival. In the above FL3 study 17 , the OS was 59% in the auto-SCT cohort and 54% in the reduced-intensity conditioning (RIC)-allo-SCT cohort, and differences in OS were not statistically significant. However, in another study 35 , between FL1 and FL2 patients, OS was 74% in the auto-SCT cohort and 66% in the RIC-allo-SCT cohort, and differences were statistically significant. In the present study, subgroup analysis for patients with FL found a significantly lower PFS in the auto-SCT group compared with that in the allo-SCT group. However, a significantly lower NRM was also found in the auto-SCT group, and patients with B-cell DLCL had higher OS and PFS and lower TRM in the auto-SCT group.
Auto-SCT can achieve a high rate of complete remission and favorable OS and PFS outcomes. However, considering the generally higher TRM associated with allo-SCT, allotransplant is indicated primarily for FL relapse after ASCT 36 . In recent years, the use of allo-HCT has increased for patients who are resistant to salvage treatment or who have relapsed after an auto-HCT 37 . However, current recommendations and timing involved in the selection of auto- versus allo-SCT are influenced by patient- or disease-related factors, physician preferences, and institutional practices such as pre-HCT regimens 18 .
Although our meta-analysis is the first to compare allo- and auto-SCT for patients with relapsed or refractory NHL, two other studies have compared these procedures for patients with all disease stages. Wu et al. 38 evaluated outcomes of patients with mycosis fungoides and Sezary syndrome, finding that allo-SCT offered benefits for both OS and EFS (neither group examined TRM). Meanwhile, Wei et al. 39 included studies of patients with peripheral T-cell lymphoma, concluding that OS was similar between allo- and auto-SCT arms of the included studies. Considering the differences, Wu et al. 38 included single-arm studies of either allo- or auto-SCT, and the allo-SCT group had a significantly greater number of systemic therapies than the auto-SCT group. In contrast, in the present analysis and Wei et al., 39 only studies evaluating both types of SCT were included.
An important development in allo-SCT is the use of RIC-allo-SCT, which has been proposed as an effective way to decrease mortality rates of patients undergoing this procedure, and has been recommended for HCT in older adults and/or patients with comorbid disease 40 . In the present meta-analysis, seven studies reported the use of RIC-allo-SCT. One study used RIC-allo-SCT to treat grade 3 FL 17 , and another used RIC-allo-SCT to treat transformed B-cell lymphoma 22 . Three of the five studies using RIC-allo-SCT did not show significantly better OS than in those using auto-SCT. RIC-allo-HCT significantly reduced risk of disease relapse and potentially improved OS and PFS in a subset of long-term (>24 months) survivors 17 , and HLA-matched unrelated donors were as effective as HLA-matched related donors for RIC-allo-SCT in treatment of FL 27 . Evidence demonstrates that RIC-allo-SCT may not be uniformly superior to non-RIC or myeloablative allo-SCT, since three groups of investigators found no differences in OS for patients with T-cell leukemia-lymphoma, NHL, and chronic lymphocytic leukemia 41 –43 .
A second important development in the management of patients with B-NHL is the use of rituximab (anti-CD20) 44 . Among the 18 studies included in this meta-analysis, 8 studies published after 2000 did report including patients who previously received rituximab. Two articles reported that rituximab was used by few, if any, patients. Six of the eight studies using rituximab prior to SCT did not show significant differences in OS between patients receiving auto- versus allo-SCT. Evens et al. 20 and Robinson et al. 21 demonstrated that auto-HCT significantly improved OS in FL and B-cell DLCL patients who had been treated with prior (and relapsed from) rituximab, respectively. In fact, Reddy et al. 22 found that pre-SCT rituximab maintenance did not affect long-term SCT outcomes. Further study must address the rituximab issue.
Strengths and Limitations
This is a detailed, comprehensive meta-analysis and the results may help to suggest optimal SCT strategies to guide clinical practice in managing refractory or relapsed B-NHL. Nevertheless, several limitations must be noted. First, the included studies were not randomized trials and some had only a small number of patients. Second, the patient population was heterogeneous in grades and subtypes of B-NHL, with/without prior rituximab treatment, transplantation procedure, outcome measurement, and duration of follow-up; patients also underwent transplant at different time in their disease history. In addition, tumor histology was heterogeneous among the studies even though we performed subgroup analysis. Between-study heterogeneity in subtypes and grades of B-NHL suggests that our findings should be confirmed with further prospective randomized trials. Third, we did not evaluate complications following SCT, including the presence and severity of graft-versus-host disease and septic events as reported by numerous other studies, including some from the present meta-analysis 16,23,24,27 . Furthermore, some studies did not report pretreatment with rituximab, and bias may have been introduced into survival outcomes. We must also consider the presence of selection bias, as the clinical characteristics of patients being treated with allo-SCT versus auto-SCT are usually different, as candidates of allo-grafting often have worse prognosis at the time of transplant than auto-grafting transplant recipients. Thus, it is important for future studies to stratify patients on the basis of subtypes and grades of B-NHL. The number of studies included in the subgroup analysis was also limited, so additional studies were needed to confirm the results of this meta-analysis.
Conclusion
This meta-analysis demonstrated that patients who receive auto-SCT have longer OS than those treated with allo-SCT. Auto-SCT patients also had lower TRM and NRM, but higher relapse or progression rate than allo-SCT patients. However, whether the beneficial effect of auto-SCT is different between patients with low-grade and high-grade B-NHL remains unclear. This study is also limited by a lack of prospective and/or randomized trials, heterogeneity of patients, and possible presence of selection bias. More prospective randomized trials are needed to compare auto- and allo-SCT among patients with relapsed or refractory disease, stratifying patients based on the subtypes and grades of B-NHL.
Footnotes
Authorship
Rong Liang was a guarantor of integrity of the entire study and contributed to study concepts and manuscript editing; Jianhong Wang to statistical analysis; Xiangxiang Liu to manuscript preparation; CaixiaHao to manuscript preparation; Hongjuan Dong to data acquisition; Tao Zhang to defining intellectual content; HongtaoGu to literature search; Baoxia Dong to data acquisition; Lan Yang to manuscript editing; GuangxunGao to study design; QingxianBai to literature search and Xiequn Chen to manuscript review.
Authors Note
Jianhong Wang, MD and Xiaohui Duan, MD are first coauthors.
Ethical Approval
This study was approved by our institutional review board.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.