
Abstract
Total pancreatectomy with islet autotransplantation (TPIAT) is a promising treatment for refractory chronic pancreatitis (CP). Pathological features of CP include progressive fibrosis in pancreas parenchyma, atrophy, and/or ductal occlusion. Complete acinar atrophy (CAA) caused by chronic fibrosis and necroinflammation results in exocrine sufficiency and may influence islet isolation characteristics during TPIAT. In this analysis of patients who underwent TPIAT at our center, we compared transplant outcomes among those with CAA (n = 5) vs non-acinar atrophy (NAA; matching controls, n = 36). Data were analyzed using one-way analysis of variance with Bonferroni post hoc test or Student’s t test. Pancreas digestion was longer in CAA than in NAA cases (18.6 vs 14.6 min) despite a lower pancreas weight (55.2 vs 91.2 g). Obtained tissue volume was 1.0 ml in the CAA group and 12.1 ml in the NAA group. Both groups had similar islet viability (96%) and islet dose (CAA, 3,391 IEQ/kg; NAA, 4141.1 IEQ/kg). During islet infusion, serum cytokine (IL-6, IL-8, and MCP-1) levels and plasma hsa-miR-375 levels were lower in the CAA group than in the NAA group, but not significantly. Serum tumor necrosis factor α levels at 3 h after infusion were significantly higher in CAA group than in NAA group. After TPIAT, the metabolic outcomes of the CAA group were comparable with that of the NAA group. Narcotics usage decreased significantly over 24 months in both groups, with the CAA group reporting being pain free at 12 months. Complete atrophy of acinar cells of pancreas did not significantly impact islet yield or endocrine function after TPIAT.
Introduction
Chronic pancreatitis (CP) is a long-standing fibroinflammatory disease of the pancreas characterized by progressive fibrotic destruction of the parenchyma, calcification, and/or ductal obstruction 1 –3 . The TIGAR-O CP classification system includes toxic-metabolic (smoking, alcohol), idiopathic, genetic, autoimmune, recurrent, and severe acute pancreatitis–associated CP and obstructive factors (Oddi dysfunction, pancreatic divisum, pancreatic duct strictures, and tumors) 4 . The complex pathophysiology of CP involves an initial triggering episode of acute pancreatitis, followed by inflammation that either leads to subsequent recovery or to pathological progression. The dead acinar cells are replaced by fibrosis, mediated by pancreatic stellate cells, with deposition of extracellular matrix 1 . Fibrosis progression results in irreversible morphological changes that affect exocrine and/or endocrine function. Clinically, CP manifests as severe abdominal pain, exocrine pancreatic insufficiency (steatorrhea, weight loss, and malnutrition), and diabetes 3 . Therapeutic strategies include pain management using narcotics/celiac plexus blockade, pancreatic enzyme replacement, and stent placement. Surgical intervention (drainage procedures, partial or total pancreatectomy) is indicated in patients with poor pain management, pseudocysts, and refractory CP. Total pancreatectomy with islet autotransplantation (TPIAT) is a promising strategy to preserve endocrine function while also alleviating pain and improving quality of life 5 –7 .
TPIAT involves pancreatectomy, islet isolation using a combination of collagenase and neutral protease, and infusion of islets into the patient’s portal vein. Successful transplant outcomes (insulin independence) depend on islet isolation factors including islet yield, purity, and viability 8 . Islet isolation parameters including enzyme concentration/activity and cold ischemia time are monitored carefully to minimize damage to islets prior to transplantation. In selected CP patients, islets may be damaged by ongoing inflammatory and fibrotic processes even before surgery. In a severely fibrotic pancreas, ductal obstruction or strictures affect the efficiency of collagenase delivery, resulting in poor islet yield. In some cases, we have observed release of 100% pure islets and complete absence of acinar cells following digestion of the pancreas with collagenase. We have termed these cases complete acinar atrophy (CAA), where the exocrine pancreas is completely lost to ductal obstruction, chronic inflammation, and fibrosis. In the present study, we report the impact of pancreatic atrophy on islet isolation, clinical features, and transplant outcomes in these cases in relation to non-acinar atrophy (NAA) cases.
Materials and Methods
Study Design
CP patients (n = 120) who underwent TPIAT at our center from October 2006 to August 2015 were included in the retrospective data analysis. TPIAT was indicated in patients with intractable pain, chronic narcotic dependence, and poor quality of life. Pancreatic malignant disease, cirrhotic liver, or negative C-peptide were contraindications for TPIAT. This study was approved by our institutional review board (IRB 010-237). Pretransplant assessments include age, gender, body mass index, duration of symptoms, fasting blood glucose, hemoglobin A1c (HbA1c), glucose-stimulated C-peptide, and previous surgical interventions.
TPIAT and Assessment of Graft Function
TPIAT was performed as described previously 7,9 . See Supplemental Method 1 for description of TPIAT procedure. Transplant function was assessed during clinical visits at regular intervals. Fasting C-peptide, HbA1c, and insulin use were measured for endocrine function. Narcotic use and pain score were assessed for relief from pain.
Serum Cytokine Measurements
Serum samples were collected before transplantation and at 1, 3, 6, and 24 h after transplantation and assayed for cytokine levels (see Supplemental Method 2).
Plasma hsa-miR-375 Measurements
Plasma hsa-miR-375 was measured using miRCURY LNA miRNA PCR assay system following the manufacturer’s instructions (see Supplemental Method 3).
Statistics
Patient characteristics and isolation data were analyzed using one-way analysis of variance with Bonferroni post hoc test or Student’s t test where applicable, using GraphPad Prism software, version 6. Data were expressed as mean ± standard error of the mean. A P-value < 0.05 was considered statistically significant.
Results
Preoperative Patient Characteristics
Of the 120 patients who underwent TPIAT at our center, CAA was confirmed in five patients. To establish selection criteria for NAA patients, we chose islet dose (IEQ/kg bw) as the primary parameter to ensure unbiased comparison of clinical features between the groups. The interquartile range of islet dose in the CAA group was 2,728–4,799 IEQ/kg bw, and thus, 36 patients who had an islet dose in the range of 3,000–4,999 IEQ/kg bw were included in the study.
Table 1 and Supplemental Table 1 present the groups’ preoperative patient characteristics. The CAA and NAA groups did not differ significantly in age, body weight, body mass index, or duration of symptoms. Men comprised 20% of the CAA group and 36% of the NAA group. The CAA and NAA groups demonstrated varied etiologies: idiopathic (60% of CAA and 36% of NAA), Oddi dysfunction/pancreatic divisum, hereditary, alcoholic, and others. In the CAA group, three patients (two Whipple and one Puestow procedure), and in the NAA group, seven patients (two Whipple, three Puestow, one partial pancreatectomy, and one debridement) had past pancreas surgery. One patient in the CAA group and seven patients in the NAA group were on diabetes medication. Basal and stimulated C-peptide and HbA1c did not differ significantly between the groups. There was no significant difference in pain score or in pain management using narcotics.
Preoperative Characteristics of 41 Patients Undergoing Total Pancreatectomy with Islet Autotransplantation.
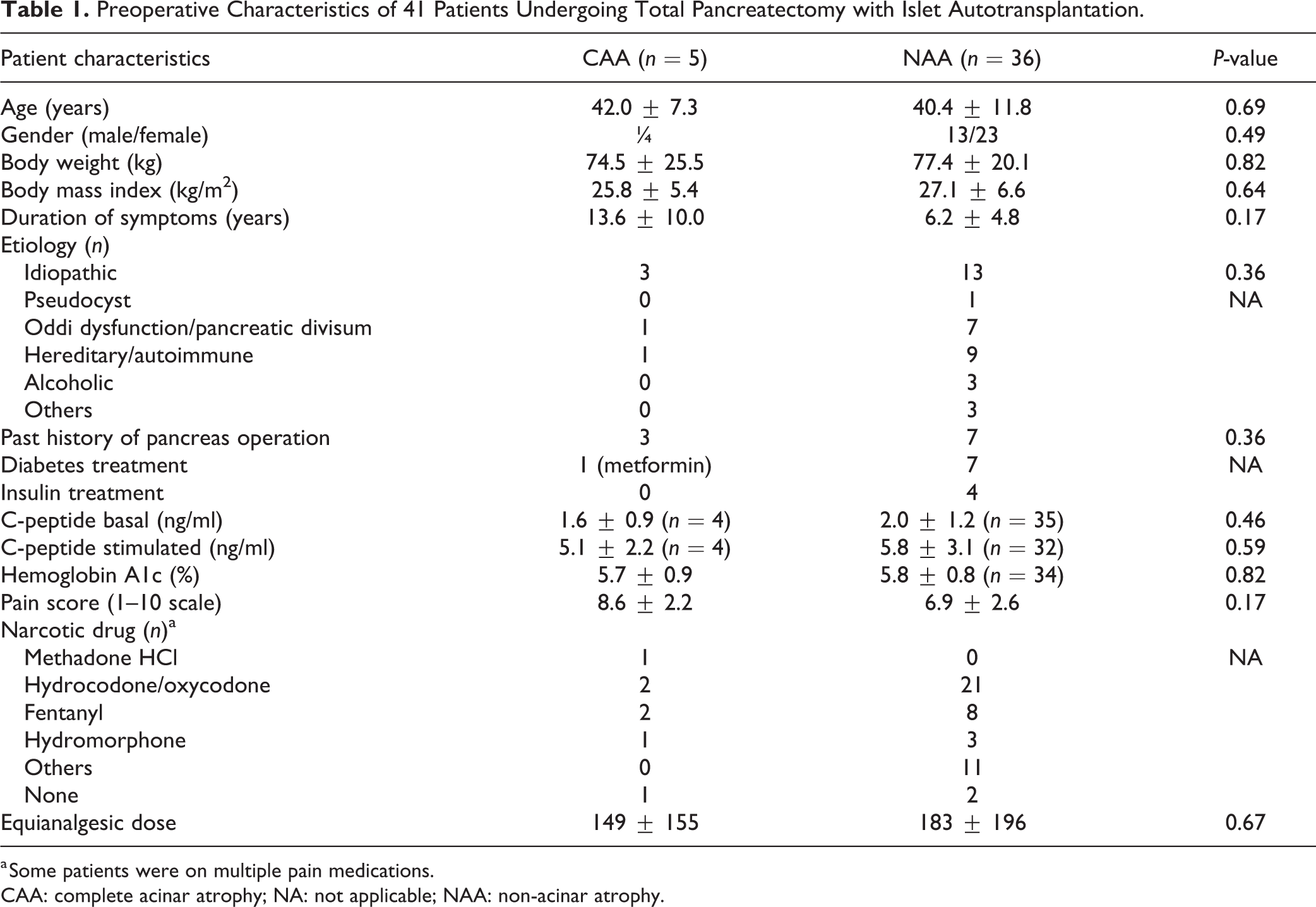
a Some patients were on multiple pain medications.
CAA: complete acinar atrophy; NA: not applicable; NAA: non-acinar atrophy.
Islet Isolation and Infusion Characteristics
The final trimmed pancreas weight was lower in the CAA group, but not significant (Table 2). Representative images showing the morphology of exocrine pancreas and insulin expression in the pancreas of a 49-year-old woman with CP and a normal healthy woman are shown in Fig. 1A. Cold ischemia time and pancreas digestion time did not differ between the groups (Table 2). During digestion, the pancreas digest was sampled every 2 min and stained with dithizone to monitor the islet isolation process (Fig. 1B). In the CAA group, only islets were present in the pancreas digest, while in the NAA group, islets including acinar tissue gradually increased over 16 min of digestion (Fig. 1B). While undigested tissue weight did not vary significantly between the groups, the final tissue volume was significantly lower in the CAA group (1.0 vs 12.1; P < 0.0001; Table 2). Islet yield
Islet Isolation and Infusion Characteristics of 41 Patients Undergoing Total Pancreatectomy with Islet Autotransplantation.

a Islets were infused into peritoneal cavity in cases where portal vein pressure increased significantly during infusion.
CAA: complete acinar atrophy; NAA: non-acinar atrophy; SD: standard deviation.

Histopathology of the pancreas and digestion characteristics. (A) Representative images showing morphology of exocrine pancreas (hematoxylin and eosin) and endocrine pancreas (insulin) in a CAA patient (i, iii) and a NAA patient (ii, iv). Arrows indicate islets. (B) Islets stained with dithizone during pancreas digestion at 4, 8, 12, and 16 min in the same patients with CAA and NAA. CAA: complete acinar atrophy; NAA: non-acinar atrophy.
During islet infusion, the initial and final portal vein pressure was not significantly different between the groups, and there was no significant difference in the islet dose infused into the portal vein (Table 2). However, in seven patients in the NAA group, portal vein pressure exceeded 20 mmHg, while none in the CAA group reached 20 mmHg. In five patients in the NAA group, a portion of the isolated islets (121,392 ± 54,079 IEQ) was infused into the peritoneal cavity at the surgeon’s discretion due to a considerable increase in portal vein pressure (P = 0.007 vs CAA, Table 2). In the CAA group, all islets were infused into the portal vein. In both groups, none of the patients had portal vein thrombosis after surgery. The total time for pancreatectomy was not significantly different between the groups (Table 2). Each CAA patient’s individual isolation and infusion characteristics are provided in Supplemental Table 2.
Plasma hsa-miR-375 and Serum Cytokine Levels After TPIAT
Plasma levels of hsa-miR-375, a marker of islet damage 10,11 , were monitored preinfusion and at 1, 3, 6, and 24 h after TPIAT. In both groups, hsa-miR-375 was not detected in plasma preinfusion but was considerably elevated at 1 h after transplantation in NAA group. In CAA group, levels of hsa-miR-375 were elevated at 1 h but not significantly (Fig. 2A), and reduced gradually over 24 h after transplantation in both groups (Fig. 2A). In the NAA group, serum IL-6 levels increased gradually up to 6 h after transplantation and were higher than those in the CAA group at respective time points, but not significantly (Fig. 2B). In the NAA group, serum IL-8 was elevated significantly at 1, 3, and 6 h after transplantation compared to the preinfusion time point within the group. Although serum IL-8 was elevated in the CAA group, it was not significant when compared either to the preinfusion time point within the group or to respective time points in the NAA group (Fig. 2C). Serum CXCL-10 levels were elevated in both groups 1 h after transplantation but returned to baseline by 3 h after transplantation (Fig. 2D). Serum MCP-1 levels were elevated at 1, 3, and 6 h after transplantation in the NAA group, but the difference was not significant when compared with the preinfusion time point or the CAA group (Fig. 2E). Serum tumor necrosis factor α (TNFα) was significantly elevated 3 h after transplantation in the CAA group compared to the preinfusion time point (P < 0.05) and respective time point in the NAA group (P < 0.01, Fig. 2F). Area under curve analysis revealed no significant differences between the groups for any of the cytokines (except TNF-α, P < 0.05) (data not shown).
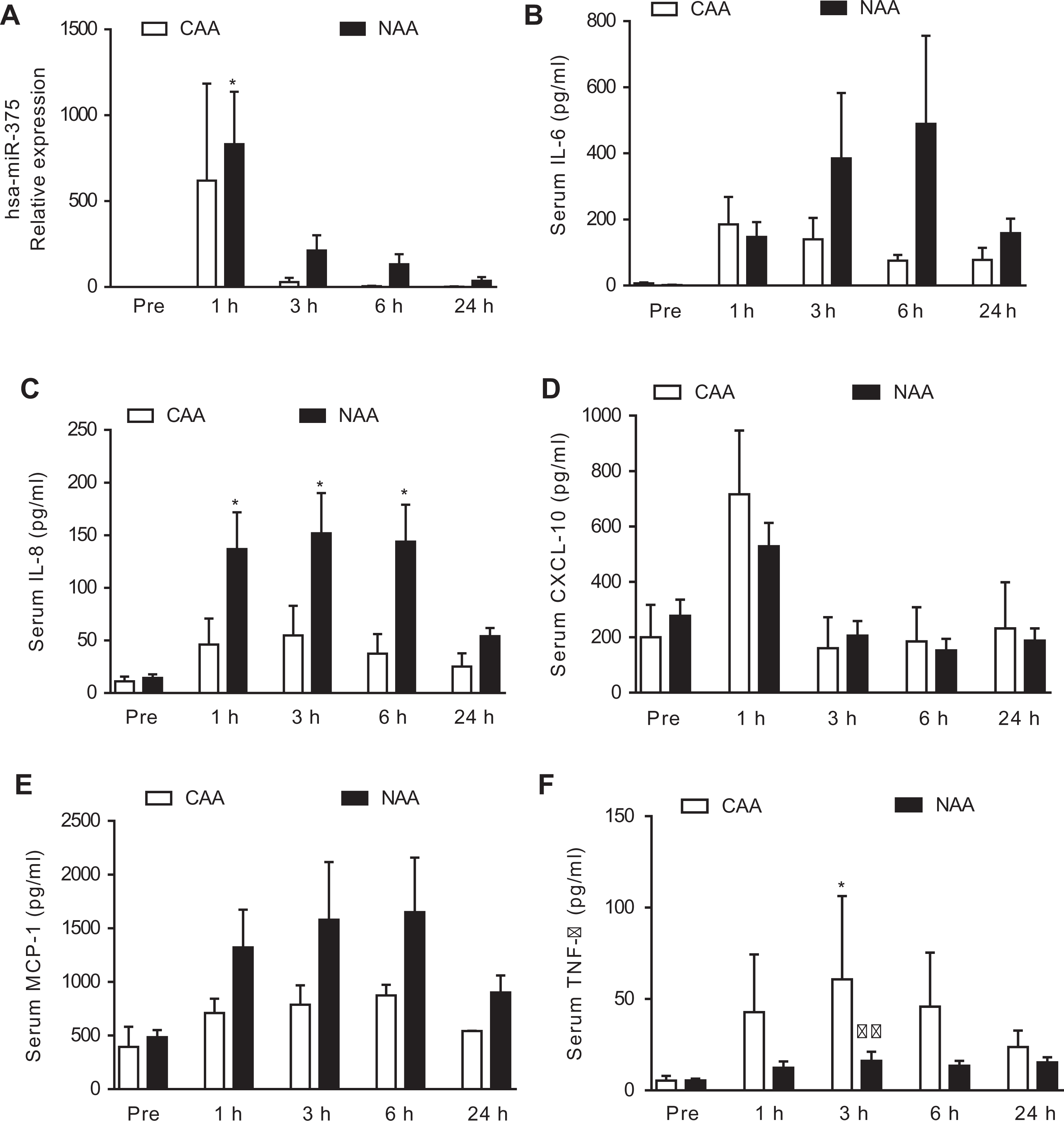
Circulating levels of hsa-miR-375 and proinflammatory cytokines. (A) hsa-miR-375 expression before and at 1, 3, 6, and 24 h after transplantation. Values are mean ± SEM (n = 2 in CAA group, n = 4 in NAA group). *P < 0.05 compared to pretransplant levels. (B–F) Serum levels before and at 1, 3, 6, and 24 h after transplantation: (B) IL-6, (C) IL-8, (D) CXCL-10, (E) MCP-1, and (F) TNFα. Values are mean ± SEM (n = 2 in CAA group, n = 10 in NAA group). *P < 0.05 compared to pretransplant levels. ϕϕ P < 0.01 compared to corresponding time in CAA group. CAA: complete acinar atrophy; NAA: non-acinar atrophy; SEM: standard error of the mean; TNFα: tumor necrosis factor α.
TPIAT Outcomes
In the CAA group, serum C-peptide levels increased gradually over 12 months and were detectable until 24 months after transplantation (Fig. 3A). In the NAA group, the C-peptide levels at 3 months post-transplantation were significantly higher than at 1 month post-transplantation (P < 0.05, Fig. 3A) and compared with the CAA group (P < 0.01, Fig. 3A). At 24 months, the NAA group had higher C-peptide levels than the CAA group (P < 0.05, Fig. 3A). HbA1c levels were similar in both groups at all the time points (Fig. 3B). The insulin requirement (units/kg bw) was lower in the CAA group 6 months after transplantation (P < 0.05; Fig. 3C). Narcotics dosage declined gradually over 12 months, with the CAA group becoming narcotics free. Narcotics dosage in the NAA group decreased significantly at 6 months compared to the pretransplant time point (P < 0.05, Fig. 3D), and lower dosages were maintained up to 24 months (P < 0.001, Fig. 3D). Compared to pretransplant pain scores, both groups reported significantly lower pain after transplantation; the CAA group became pain free at 12 months (Fig. 3E).
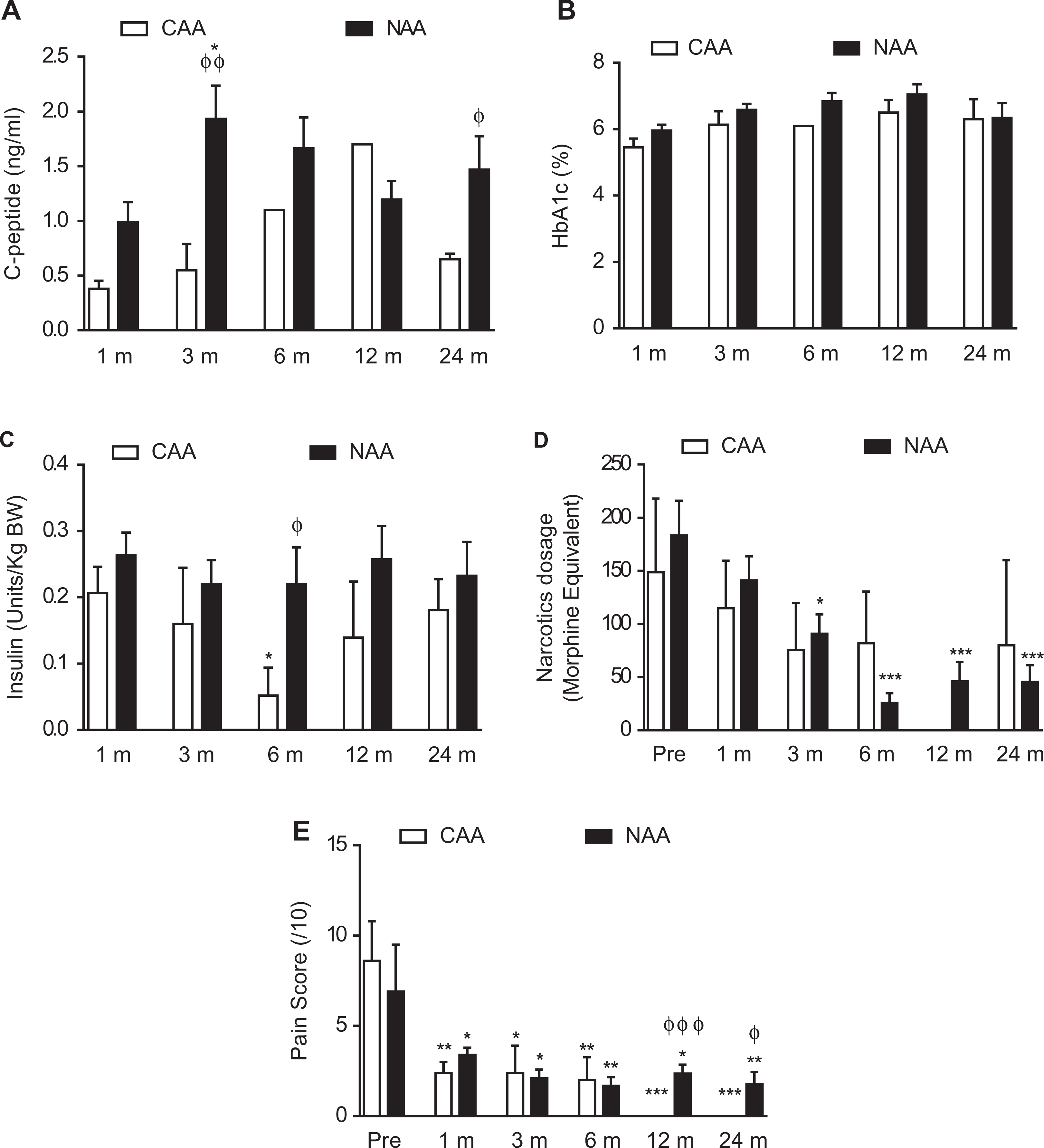
Metabolic outcomes and pain management after TPIAT. (A) C-peptide, (B) hemoglobin A1c, and (C) insulin at 1, 3, 6, 12, and 24 months after transplantation. Values are mean ± SEM (n = 1–5 in CAA group, n = 22–36 in NAA group). *P < 0.05 compared to 1 month after transplantation. ϕ P < 0.05, ϕϕ P < 0.01 compared to corresponding time for CAA group. (D) Narcotics dosage and (E) pain score before and at 1, 3, 6, 12, and 24 months after transplantation. Values are mean ± SEM (n = 2–5 in CAA group, n = 17–36 in NAA group). *P < 0.05, **P < 0.01, ***P < 0.001 compared to 1 month after transplantation. ϕ P < 0 .05, ϕϕϕ P < 0.001 compared to corresponding time for CAA group. CAA: complete acinar atrophy; NAA: non-acinar atrophy; SEM: standard error of the mean; TPIAT: total pancreatectomy with islet autotransplantation.
Discussion
In CP patients, exocrine insufficiency accompanied by maldigestion is a common clinical presentation. In rare cases, chronic necroinflammation and fibrosis lead to complete loss of acinar tissue, a condition termed “acinar atrophy” 2,3,12 . In this study, for the first time, we present the clinical features and islet autotransplant outcomes in CP patients with acinar atrophy. In early stages (mild and self-limiting, acute episodes), even though the exocrine function may be affected transiently, the exocrine pancreas compensates via regeneration and repair 13,14 . With disease progression, exocrine insufficiency results in malabsorption and malnutrition, weight loss, and steatorrhea 1,15 . While exocrine insufficiency is usually managed using enzyme replacement therapies, the debilitating pain caused by chronic inflammation and fibrosis drastically affects quality of life. In long-standing CP, endocrine failure due to loss of islet cells to inflammation results in type 3c diabetes 16 . Nonsurgical treatments are not a permanent cure for chronic pain, and their efficacy varies between patients. Across many centers, surgical intervention for refractory CP using TPIAT procedure has been successful in preventing endocrine failure and in alleviating chronic pain 6,9,17 –19 .
In our cohort of acinar atrophy cases, two patients had long-standing CP (>20 years, Supplemental Table 1), while one patient had CP for only 3 years; thus, the severity of disease progression differs considerably between patients. Patients in the CAA and NAA groups did not differ in preoperative characteristics including age, body mass index, basal and stimulated C-peptide, HbA1c, and pain score. Acinar atrophy led to reduced pancreas weight in the CAA group compared to the NAA group, despite similar body weights between the groups. During pancreas digestion, we observed free islets in the CAA group with barely any acinar tissue up to 16 min of digestion. However, in the NAA group, acinar tissue was evident in the pancreas digest starting at 8 min and increased up to 16 min. As expected, due to a severely fibrotic pancreas in the CAA group, the pancreas digestion time was longer than in the NAA group, but with similar undigested tissue weight in both groups. We and others have previously reported that duration of CP and prior surgery affect islet yield 8,20,21 . We did not find a difference in islet yield. However, the final tissue volume was significantly lower in the CAA group than in the NAA group, supporting the lack of acinar tissue in these patients. Lower tissue volume reflected 100% pure islets in the CAA group, while the presence of acinar tissue lowered islet purity (39% ± 22.6%) in the NAA group. During islet infusion, portal vein pressure increased gradually in the NAA group but was maintained at approximately 10 mmHg in the CAA group. In a subset of patients (n = 5) in the NAA group, a portion of the islet cell product was infused into the peritoneal cavity due to portal hypertension during infusion, at the surgeon’s discretion. Although no significant differences in final portal vein pressure were observed in our study, tissue volume was the best independent predictor of change in portal vein pressure in an independent study 22 with low purity increasing the risk associated with infusing large tissue volume intraportally 23 .
Plasma levels of hsa-miR-375, a marker of islet cell damage 10,11 , were significantly increased in NAA group at 1 h after transplantation and returned to baseline by 24 h after transplantation. In addition, serum level of proinflammatory cytokines/chemokines IL-8 was significantly elevated after transplantation and normalized 24 h after transplantation in NAA group compared to preinfusion time point. Serum cytokine levels were elevated in the CAA group but not significantly (except TNF-α) when compared to preinfusion time point and to NAA group. Area under curve analysis revealed no significant differences between the groups in serum cytokine levels (except TNF-α). We have previously reported that isletokines (cytokines/chemokines released by islets) are elevated in circulation in TPIAT patients within 1 h of islet infusion 24 . Further investigations using a larger cohort are needed to investigate whether islet purity and tissue volume influence serum cytokine and miRNA levels.
Despite differences in islet purity, both groups exhibited islet function (detectable C-peptide levels) up to 2 years after transplantation. The CAA group required a lower insulin dosage at 6 months after transplantation. At 2 years, both groups had a similar insulin dosage, with HbA1c maintained below 7.5 during this period. Narcotics dosage decreased gradually over 2 years in both groups. In the CAA group, the patients became pain free at 6 months after transplantation and narcotics free at 12 months. Although it is well established that long-standing CP affects islet yield and islet survival, in a subset of patients with acinar atrophy, we observed islet survival comparable to that of other patients with some degree of acinar function. In these patients, we were able to achieve islet doses recommended for successful transplant outcomes (approximately 4,500 IEQ/kg bw in patients with >20 years of CP).
In CP patients, it is imperative that TPIAT is performed before the onset of islet dysfunction and death due to ongoing inflammation, fibrosis, and associated morphological changes in the pancreas. Pain pattern and severity exhibit a poor correlation to radiological findings 25 . In addition, in a long-term study, approximately 85% of 145 CP patients were pain free 4.5 years from onset of disease, accompanied by a marked increase in pancreatic dysfunction 26 . Thus, follow-up on patients, even if they report being pain free, remains critical in evaluating the true status of disease progression.
Knowledge of the pathophysiology and progression dynamics of acinar atrophy is limited due to the complex mechanisms involved. While it is common knowledge that signaling pathways including transforming growth factor β and Fas are involved 27 –29 , the fact that the progression dynamics vary between patients suggests that individual patient characteristics play important roles. In our small cohort of five patients with acinar atrophy, clearly islets survive inflammation and fibrosis even at >20 years of disease duration, with minimal bystander toxic effect on islets. In contrast, in autoimmune diabetes, islets are specifically lost to inflammation while the exocrine pancreas is unaffected 30,31 . Earlier reports of lower islet yield in long-standing CP may be due to inefficient perfusion of the pancreas resulting from duct blockade, intrapancreatic bile duct stricturing, calcifications, pseudocysts, prior pancreas surgery, and most importantly, differences in extent of islet damage between patients. Endocrine dysfunction manifests clinically in patients undergoing distal pancreatectomy for refractory CP and alcoholic pancreatitis cases even without prior surgical intervention 32,33 . Islets may also be lost due to morphological changes in the pancreas including local changes in circulation and glucose diffusion 34 .
In this study, we report for the first time, islet isolation and transplantation outcomes in patients with CAA, undergoing TPIAT. Limitations of the current study include small sample size of five patients with CAA. Further investigations using a larger cohort are thus needed to understand the heterogeneity of islet damage in patients with CP.
Supplemental Material
Supplementary_Tables_070720 - Outcomes of Islet Autotransplantation in Chronic Pancreatitis Patients with Complete Acinar Atrophy
Supplementary_Tables_070720 for Outcomes of Islet Autotransplantation in Chronic Pancreatitis Patients with Complete Acinar Atrophy by Gumpei Yoshimatsu, Mazhar A. Kanak, Srividya Vasu, Kenjiro Kumano, Michael Lawrence, Nicholas Onaca, Morihito Takita, Marlon F. Levy and Bashoo Naziruddin in Cell Transplantation
Footnotes
Acknowledgment
We thank Ana Rahman for her technical support in the clinical islet isolation.
Ethical approval
Ethical approval to conduct and report this study has been approved by Baylor Institutional Review Board – IRB 010 237.
Statement of Human and Animal Rights
All procedures reported in this article were conducted in accordance with Baylor Institutional Review Board’s approved protocols.
Statement of Informed Consent
All patients enrolled in this study provided written informed consent for publication of data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support by Baylor University Medical Center is gratefully acknowledged
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.