
Abstract
Biopsy, brushing, and transbronchial needle aspiration (TBNA) are the most common methods for diagnosis of lung adenocarcinoma and are taken during the same diagnostic bronchoscopic procedure. However, it is not clear what the morphological diagnostic criteria of cytology by brushing or TBNA are. A retrospective analysis was performed on 136 patients who underwent video bronchoscopy examination for diagnostic purposes. All the subjects were performed brushing or TBNA and confirmed as lung adenocarcinoma by biopsy or postoperative pathology. An additional 140 randomly selected patients with benign lung diseases were included in the study and used as a control group. The benign cells usually confused with adenocarcinoma cells were ciliated columnar cells, mucous columnar cells, ciliated cuboid cells, and reactive ciliated cells, respectively. The number of cases diagnosed as adenocarcinoma cells, carcinoma cells, suspicious cancer cells, and atypical proliferative cells by cytology was 101, 11, 20, and 4, respectively. The main basis for the interpretation of adenocarcinoma cells is the enlargement of individual nucleus, the arrangements of multistage papillary, and the general enlargement of nuclei, while the main clue for the interpretation of suspicious cancer cells and dysplasia cells comes from escape cells. The results suggested that the degree of nuclear enlargement, multiple papillary arrangement, and escape cells or escape trend cells are important clues for the interpretation of lung adenocarcinoma cells, while the atypical proliferative cells were similar to escape cells or escape trend cells, which were essentially benign cells beside the cancer.
Keywords
Introduction
Lung adenocarcinoma is one of the leading causes of cancer death and accounted for nearly 40% of all lung cancers 1 . In recent years, the incidence of lung adenocarcinoma is on the rise in many countries 2 . Accurate diagnoses and discrimination between lung adenocarcinoma and reactive bronchial epithelium for lung adenocarcinoma are of vital importance for optimal therapeutic decision-making and improved prediction of patients’ response to treatment 3 . Forceps biopsy, bronchial brushing, and transbronchial needle aspiration (TBNA) are the most common methods for diagnosis of lung cancer and are taken during the same diagnostic bronchoscopic procedure. The biopsy is limited by the status of certain lesions, such as the lesions of the distal bronchus or severe surface ulceration, and in order to avoid the bleeding, the biopsies often obtains paracancerous tissues, resulting in false negative results. Brushing and TBNA are the less invasive diagnostic technique and suitable for all lesions, so it is important for the complements forceps biopsy in the diagnostic work-up of lung cancer 4 . A combination of bronchial brushing and forceps biopsy is thought to be an essential step for the diagnosis of bronchoscopically visible lung cancer 5,6 , TBNA or E-bus may increase the diagnostic yield of lung adenocarcinoma 7,8 .
Although most of the lung adenocarcinoma occurred in peripheral type, the appearance of ultrasound bronchoscope and E-bus brought new dawn for the acquisition of abundant lung adenocarcinoma cells. However, the cytological diagnostic criteria and the common cell arrangement types of adenocarcinoma cells as well as cell types easily confused with adenocarcinoma cells are not clear. The main purpose of this study was to evaluate both the accuracy of cytological diagnosis and the main cause of false negative for the diagnoses of lung adenocarcinoma by bronchoscopy. In particular, we aimed to evaluate the common arrangements types and heteromorphic characteristics of lung adenocarcinoma cells.
Materials and Methods
This study was a retrospective analysis of cytological diagnoses of lung adenocarcinoma patients confirmed by histology, and this study was approved by the Ethics Committee of the First Hospital of China Medical University and informed consent was obtained from each patient. The pathological diagnosis of both histology and cytology from 136 patients who attended the department of pathology at the First Hospital of China Medical University during the period August 2018–December 2019 were included in the study. The study group comprised 74 men and 62 women, ranging in age from 25 to 80 years. An additional 140 randomly selected patients with benign lung diseases were included in the study and used as a control group.
All bronchoscopies were performed by two experienced bronchoscopists using a standard video bronchoscope (1T260, Olympus, Tokyo, Japan), a flexible long biopsy forceps (FB21C-1, Olympus), and straight brushes (BC-202D-2010, Olympus). Both forceps biopsies and brushings were obtained from all subjects except some special lesions. TBNA method is used for some special lesions, such as hilar or mediastinal masses, lesions outside the bronchus, and enlarged lymph nodes. To obtain sufficient numbers of cells from the brushings, the brushings were performed before the forceps biopsies, and this point had been confirmed in our previous experiments 9 . The area of suspected malignancy was brushed 2 or 3 times; the smears were fixed in 95% alcohol and stained by Papanicolau’s method. Next, the forceps biopsy specimens were taken for histological examination from the same area of brushing and stained with hematoxylin and eosin (H&E) and/or immunohistochemistry after being processed. TBNA samples were used for both histological wax and cytological smear. The histology and cytology specimens were processed separately in different laboratories, and the findings were reviewed and reported separately by 2 different pathologists at different times daily.
Based on the histological diagnoses of forceps biopsy, TBNA, and resection specimens and the cytological diagnoses of brushing and TBNA, the diagnosis results were recorded into histological and cytological groups, respectively. Statistical analysis was performed using SPSS 16.0 software package (SPSS, Inc. Chicago, IL, USA).
Results
First of all, we need to interpret the normal cell groups that are easy to be confused with adenocarcinoma cells. The key to interpret these normal cell groups is to find ciliated cells. Common ciliated cells include the following four types, and their morphological characteristics are shown in Table 1 (Fig. 1A–D).
The Benign Cell Characteristics Easily Confused with Adenocarcinoma Cells in the Bronchial Brush or Needle Aspiration Smears.
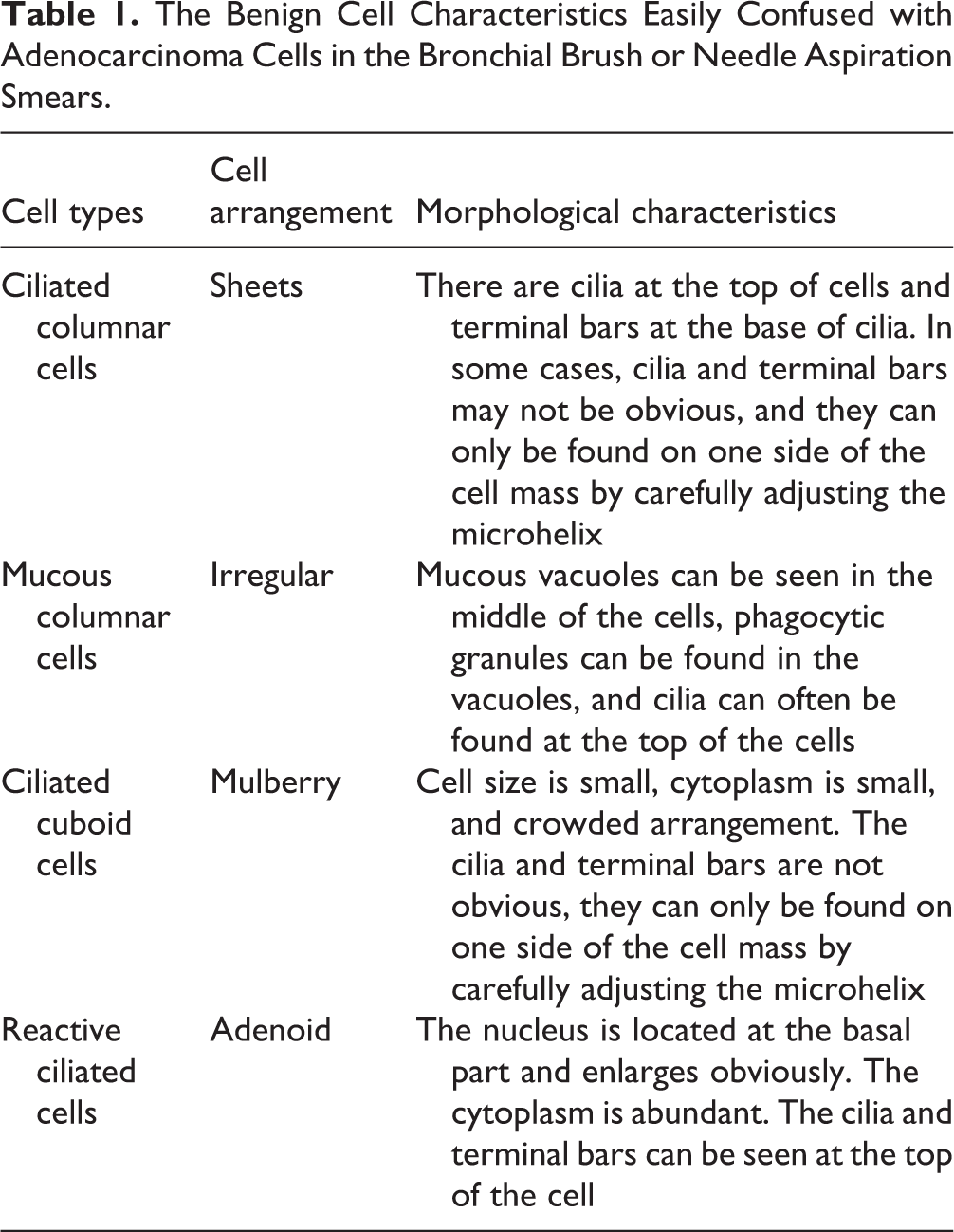

Morphological characteristics of ciliated cells and adenocarcinoma cells in both bronchial brushing and TBNA (Papanicolaou stain, × 400). (A) On the left side of the picture, a cluster of ciliated columnar cells are seen from the top, but the cilia and endplate are not clear; on the right lower corner, three ciliated columnar cells are seen from the side, and the cilia and endplate are clear. (B) A cluster of mucinous columnar cells are arranged in an adenoid way, the nuclei are located in the basement, and a lot of mucinous vacuoles are in the cytoplasm. (C) A cluster of ciliated cuboid cells is arranged in a plum pattern. Cilia and terminal bars can be found in the cracks at the bottom through careful observation. (D) Several rows of reactive ciliated cells are arranged in palisade, the enlarged nuclei are located in the basal part, and the cilia and terminal bars can be seen at the top of the cells. (E) A cluster of adenocarcinoma cells are arranged in an atypical adenoid cavity, the majority of nuclei in the cell cluster were more than three times larger than the red blood cells in the background. (F) A cluster of adenocarcinoma cells are arranged in an atypical adenoid cavity, two cells in the upper left corner of the cell cluster are more than three times larger than other cells. (G) Several clusters of adenocarcinoma cells are arranged in multistage papillary pattern, and the nucleus size is similar. (H) A cluster of adenocarcinoma cells is arranged in the shape of plum blossom petals, with a similar size of nucleus. One escape cell can be found in the upper left corner of the cell cluster, and one escape trend cell can be found in the upper right corner. The angle between the escape trend cell and the cell cluster is less than 90°. TBNA: transbronchial needle aspiration.
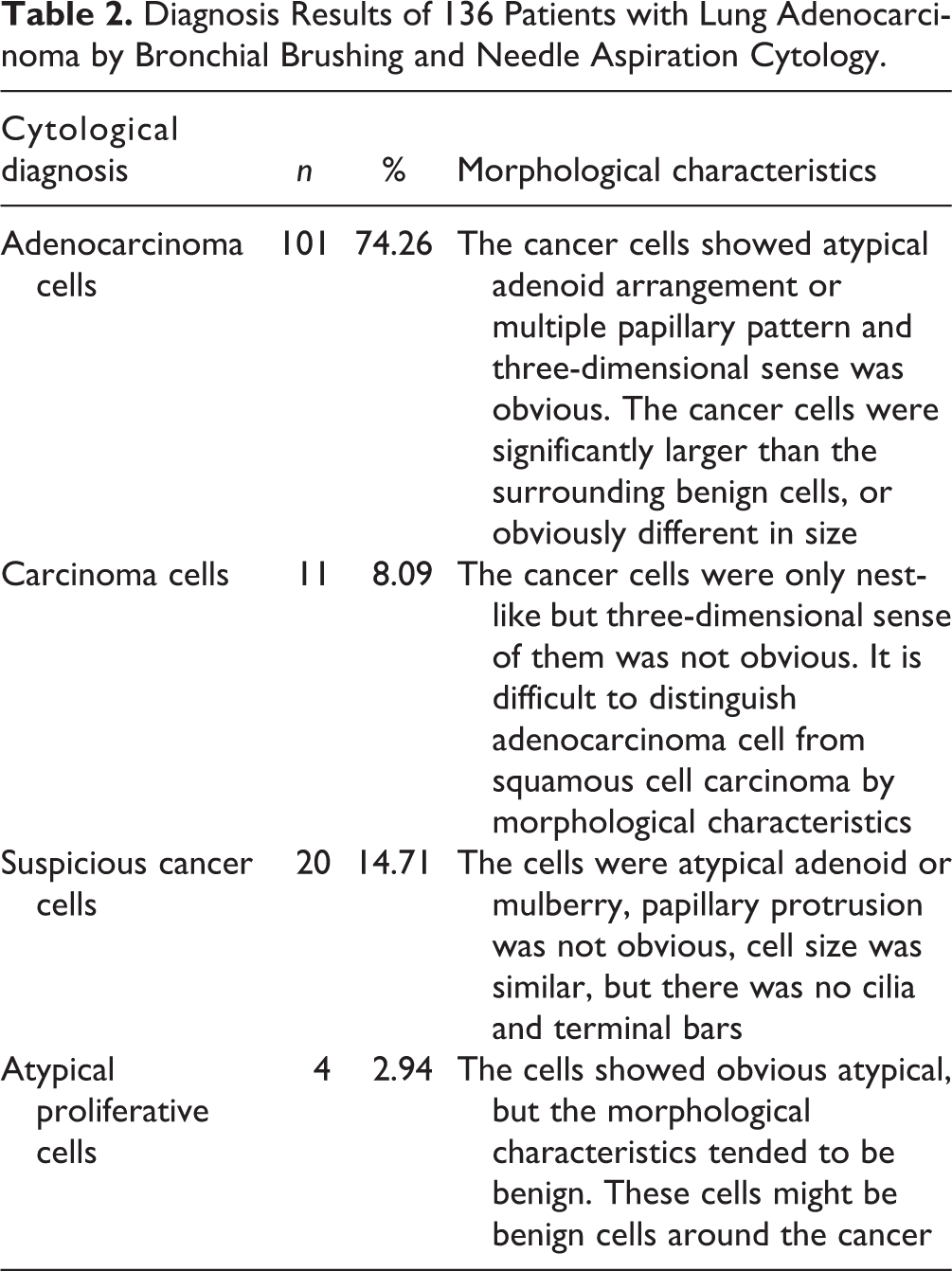
In 136 cases of lung adenocarcinoma confirmed by histology, cytology was diagnosed as adenocarcinoma cells, cancer cells, suspicious cancer cells, and atypical proliferative cells, respectively. Among them, 101 cases were diagnosed as adenocarcinoma cells by cytology, accounting for 74.26% of the total cases. The cytological morphological basis of various interpretation results is shown in Table 2.
Diagnosis Results of 136 Patients with Lung Adenocarcinoma by Bronchial Brushing and Needle Aspiration Cytology.
The common morphological characteristics of 136 cases of lung adenocarcinoma cells and their relationship with the background were reviewed. The results showed that the cytological diagnosis results were closely related to nuclear enlargement and cell arrangements. The main basis for the interpretation of adenocarcinoma cells is the enlargement of individual nucleus, the arrangements of multistage papillary, and the general enlargement of nuclei, while the main clue for the interpretation of suspicious cancer cells and dysplasia cells comes from escape cells. The detailed results are shown in Table 3 (Fig. 1E–H).
The Morphological Basis of Cytological Diagnosis for Bronchial Brushing and TBNA of Patients with Lung Adenocarcinoma.
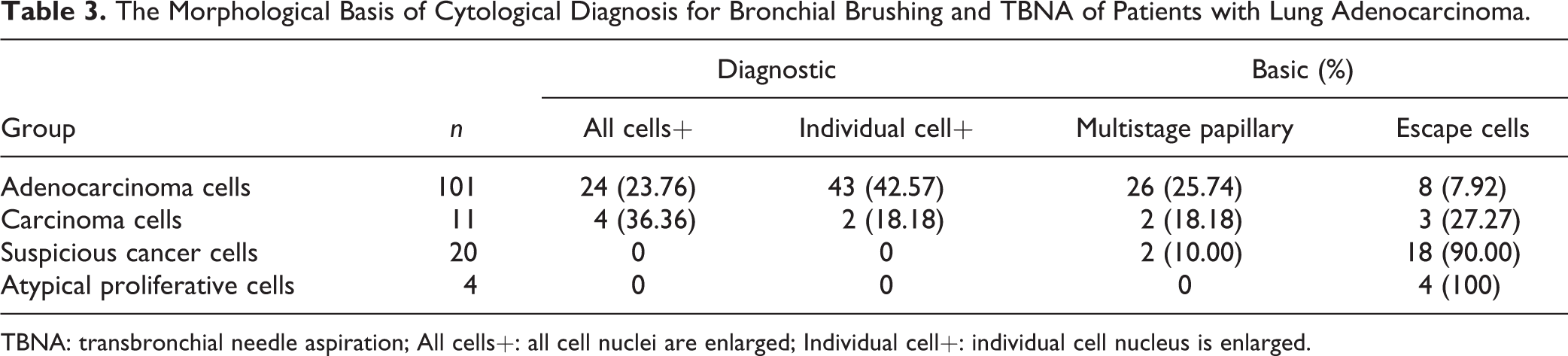
TBNA: transbronchial needle aspiration; All cells+: all cell nuclei are enlarged; Individual cell+: individual cell nucleus is enlarged.
Discussion
We had made a detailed discussion on the cytological characteristics and arrangements of small cell lung cancer 10 . However, accurate interpretation of the morphological characteristics and arrangements of lung adenocarcinoma cytology has not been reported. Ravaioli et al. believed that the best way to interpret lung adenocarcinoma cells was to combine nucleolus with medium/small cell mass 11 , and it was also reported that accurate cell typing of nonsmall cell lung cancer (NSCLC) could be achieved by TBNA, but the specific morphological characteristics of NSCLC were not discussed in detail 12 –14 . In this study, we found that the premise of accurate interpretation of lung adenocarcinoma cytology is to first understand the morphological characteristics of normal bronchial epithelial cells. The normal epithelial cells that are often confused with lung adenocarcinoma cells were ciliated columnar cells, mucinous columnar cells, ciliated cubic cells, and reactive ciliated cells, and both the cilia and terminal bars in these cells were often covered up due to the angle, which led to these cells being mistaken for adenocarcinoma cells. In order to avoid false positive results, it is necessary to carefully observe the surrounding or central fissures of these cell clusters. Once the cilia and terminal bars are found, it can be determined that these cells are normal cells. Even reactive ciliated cells, no matter how obvious the nuclear enlargement, are benign cells as long as cilia and terminal bars are found.
In 136 cases of lung adenocarcinoma in this study, 101 cases (74.26%) were diagnosed by cytology. In addition to the obvious malignant features of the cells in these lesions, the characteristics of the origin of the glandular epithelium are also obvious, such as the atypical arrangements of glandular cavities. The results suggest that the cytological diagnosis obtained by fibrobronchoscopy has an important clinical application value in the diagnosis of lung adenocarcinoma. The cytology of 11 cases showed only malignant features, lacking the characteristics of glandular epithelial origin, so they could only be diagnosed as cancer cells. Further classification needs to be confirmed by immunohistochemistry. In another 20 cases, the malignant features of the cytology were not very clear, just suspicious, so we only reported the suspicious cancer cells. These lesions need to further observe the arrangement and morphological characteristics of the cells, so as to find a reliable clue for the diagnosis of adenocarcinoma cells. In addition, there are 4 cases diagnosed as reactive cells, and they had some heteromorphism, but lack of malignant characteristics, so they might be benign cells around the cancer.
In order to provide an accurate cytological diagnosis for the clinic as much as possible, reviewing the cytological diagnosis results of 136 cases of lung adenocarcinoma in this study, we found that the nuclear characteristics and arrangements are very important for the interpretation of the diagnosis results. In the nuclear characteristics, we must observe the extent of nuclear enlargement, and choose the appropriate contrast cells. One comparison method was that if the majority of nuclei in the cell mass were more than three times larger than the lymphocytes or red blood cells in the background, this was probably the most reliable basis for the interpretation of adenocarcinoma cells. However, only 24 cases met this standard, accounting for 23.76% of the adenocarcinoma cell group. The other method was the cells in the cell mass were compared with each other, if a few nuclei in the cell mass were more than 3 times larger than other nuclei, this was probably another reliable standard for judging adenocarcinoma cells. In this study, the number of cases meeting this standard was the most, 43 cases, accounting for 42.57% of the adenocarcinoma cell group. This result suggests that it may be the most helpful for us to focus on the intercomparison within cell clusters in the interpretation of adenocarcinoma cells.
The arrangements of cells can be divided into multistage papillary arrangements of most cells and escape state of a few cells from the original cell cluster. The arrangements of cells were the problem that were easy to be ignored by cytologists and rarely reported in the literature. Most cytologists thought that cytological diagnosis was only based on the morphological features of cells. However, the results of this study showed that 25.74% of adenocarcinoma cells were interpreted according to multistage papillary arrangements. The results suggest that the multiple papillary arrangements have an irreplaceable role in the interpretation of adenocarcinoma cells. In this study, 11 cases were diagnosed as cancer cells, and the cytology only showed malignant manifestations, but the characteristics of glandular epithelial origin were lacking. The number of cases in this group was small, which needs to be further explored in the future.
In the group of suspected cancer cells, the size of cancer cells was similar, arranged in plum or papillary pattern, and the only clue to the adenocarcinoma cell was the discovery of escape cells. The arrangements of these cells were characterized by complete separation from the original cell cluster. In the 4 cases of atypical proliferative cell group, no escape cells were found, only marginal cells protruded outwards, and the angle between them and cell cluster was sharp, showing escape trend, so they were called escape trend cells. Reviewing the benign lesions in the control group, we found that the marginal cells in the benign lesions also showed escape trend, but these cells did not break away from the original cell clusters and the angle between them and cell cluster was obtuse, therefore, such cells can neither be called escape cells nor escape trend cells. Through the comparative analysis of benign and malignant cell clusters, we have had a deeper understanding of the concept of both escape cells and escape trend cells, which is of great clinical significance for the future diagnosis of adenocarcinoma cells and the reduction of the proportion of false negative caused by suspicious cancer cells or atypical proliferative cells.
Conclusion
The degree of nuclear enlargement and the arrangements of cells are very important for the cytological interpretation of both bronchial brushing and TBNA of lung adenocarcinoma. Nuclear enlargement more than three times is often a malignant feature, multiple papillary arrangements is another manifestation of lung adenocarcinoma cells, and the interpretation of escape cells and escape trend cells is an important clue for the diagnosis of adenocarcinoma cells. Therefore, it is of great significance for clinical cytological diagnosis to accurately identify the cilia and endplates of benign cells as well as the nuclear enlargement, arrangement model, and escape status of adenocarcinoma cells.
Footnotes
Ethical Approval
Ethical approval was obtained for the experimental procedures by the Ethics Committee of the First Hospital of China Medical University, Shenyang, China.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the First Hospital of China Medical University’s (APPROVAL NUMBER/2016-125) approved protocols. This article does not contain any studies with animals.
Statement of Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Natural Science Foundation of China to Guang-Ping Wu, Grant No.81171650 and 81672082.