
Abstract
Currently, the only effective therapy for cirrhosis of the liver is liver transplantation. However, finding a compatible liver is difficult due to the low supply of healthy livers and the ever-increasing demand. However, stem-cell therapy may offer a solution for liver cirrhosis; for example, GXHPC1 therapy preparation contains adipose-derived mesenchymal stem cells (AD-MSCs) and was developed for the treatment of liver cirrhosis. In our previous report, animal studies suggested that treatment of a diseased liver via GXHPC1 transplantation can abrogate liver fibrosis and facilitate recovery of liver function. In our current human trial, patients with liver cirrhosis were included. Their adipose tissue was harvested from the subcutaneous fat of the abdominal wall during surgery. AD-MSCs were cultured and suspended at a concentration of 100 million cells in 1 ml of physiological saline (i.e., GXHPC1). This human study passed the Taiwan Food and Drug Administration IND inspection and received Phase I clinical trial permission. The trial was conducted with six patients with liver cirrhosis to demonstrate the safety and efficacy of administering GXHPC1. Intrahepatic injection of GXHPC1 did not cause any safety issues in the analysis of adverse drug reactions and suspected unexpected serious adverse reactions, and showed a tendency for improvement of liver function, METAVIR score, Child–Pugh score, MELD score, and quality of life for patients with liver cirrhosis.
Keywords
Introduction
Disease Background
Liver cirrhosis is the final common pathological pathway of end-stage chronic liver disease arising from a variety of causes 1 . Although the causes of liver cirrhosis are multifactorial, certain pathological characteristics are common to all cases, including degeneration and necrosis of hepatocytes, replacement of liver parenchyma with fibrotic tissues and regenerative nodules, and loss of liver function 2 . Fibrosis, as a precursor of cirrhosis, is a pivotal pathological process in the evolution of all chronic liver diseases that lead to cirrhosis 3 . Many types of cells, cytokines, and miRNAs are involved in the initiation and progression of liver fibrosis and cirrhosis. Activation of hepatic stellate cells (HSCs) is a pivotal event in fibrosis. For example, defenestration and capillarization of liver sinusoidal endothelial cells are major contributing factors to hepatic dysfunction in liver cirrhosis, and the consequent activation of Kupffer cells destroys hepatocytes and stimulates activation of HSCs. Repeated cycles of apoptosis and regeneration of hepatocytes contribute to the pathogenesis of cirrhosis. At the molecular level, many cytokines are involved in mediation of signaling pathways that regulate the activation of HSCs and fibrogenesis 2 .
At present, liver transplantation is the only effective therapy for cirrhosis. Reports have shown that liver transplantation can improve hepatic function and increase patient survival rate 4,5 , but its use is limited by high cost, transplant rejection, and a shortage of allografts. Consequently, it is necessary to develop alternative therapeutic strategies for liver cirrhosis. In this regard, the potential role for stem-cell therapy in the treatment of liver diseases has recently become topical in medical research because of the self-renewal characteristics and differentiation potential of stem cells.
Stem-Cell Therapy in Liver Cirrhosis
Stem cells and their possible use in cell therapy have drawn much attention recently because of their potential for self-renewal and differentiation. Mesenchymal stem cells (MSCs) have the potential to differentiate into hepatocytes in vitro 6,7 . Moreover, studies have shown that rat or human MSCs can differentiate into hepatocyte-like cells when transplanted into rat liver 8 –10 . Recently, transplantation of rat bone marrow MSCs (BM-MSCs) was shown to protect the rat liver from chemically induced liver fibrosis 11 . In our pre-clinical study, GFP-labeled human BM-MSCs were injected into rats with carbon tetrachloride-induced liver damage. GFP-labeled cells were found around the liver lobules, hepatic blood vessels, and the edge of the liver lobes. Biochemical and histopathological analyses revealed significantly increased recovery from liver damage in the transplanted group. In addition, transplanted human BM-MSCs expressed matrix metalloproteinases (MMPs) and had significantly decreased liver fibrosis 12 . In another pre-clinical study, Wharton’s jelly stem cells (WJSCs) were transplanted into rats with liver damage; these transplanted stem cells were distributed in the fibrotic area and around blood vessels, and hepatic recovery was accelerated 13 . The serum prothrombin time significantly recovered, serum albumin also improved, and collagen accumulation decreased. These results indicated that WJSCs produce albumin, hepatocyte growth factor, and MMPs to promote recovery after chronic liver damage 13 .
Preparation of GXHPC1
Adipose-derived MSCs (AD-MSCs) were first identified as MSCs in adipose tissue in 2001 14 . Since then, adipose tissue has been studied as a cell source for tissue engineering and regenerative medicine 15 . AD-MSCs can be easily obtained from liposuction aspirates or subcutaneous adipose tissue fragments and expanded in vitro. Unlike human embryonic stem cells, there are no ethical concerns regarding the use of AD-MSCs in diverse clinical applications. The isolated AD-MSCs can be expanded vigorously until cells enter into differentiation to specific cell lineages. AD-MSCs are capable of differentiating into adipocytes, osteoblasts, chondrocytes, and myocytes in vitro, and are genetically stable in long-term culture 16 . Given the multipotency of the AD-MSCs, they can be used widely in various clinical applications. It has been reported that AD-MSCs have a hepatogenic differentiation potential similar to that of BM-MSCs, and AD-MSCs have a longer culture period and higher proliferation capacity 17 . In addition, differentiated human AD-MSCs are able to exhibit hepatogenic capability in vitro and in vivo through subtle regulation of molecular pathways that control lineage commitment 18,19 . Furthermore, reduction in the expression of α-smooth muscle actin, a marker of HSCs, produces collagen fiber, and an increase in the expression of MMP-9 degrades collagen fiber after AD-MSC transplantation 20 .
GXHPC1 is a cell product that contains human AD-MSCs isolated and expanded from autologous donors, and GXHPC1 was developed for the treatment of patients with liver cirrhosis in this Phase I study. Previously, Gwo Xi Stem Cell Applied Technology Co., Ltd. collaborated with China Medical University Hospital for a clinical project entitled “Study of isolation and preservation of human adipose-derived stem cells applied in treatment of liver cirrhosis” (project No: DRM100-IRB-202), which focused on the method of isolation and culture of AD-MSCs, analysis of stem-cell properties, and the possible application of AD-MSCs for the treatment of human diseases. The project has established one full set of standard operating procedures for the harvest, isolation, cell culture, packaging, inspection, and transport of AD-MSCs applied for GXHPC1 for the treatment of patients with liver cirrhosis.
Materials and Methods
Approval of Ethics for the Study
The study protocol and informed consent form (ICF) were forwarded to the Institutional Review Boards (IRBs) of China Medical University Hospital (CMUH) and the health authorities in Taiwan (Ministry of Health and Welfare; MOHW) for review and approval before trial initiation. The approval number was CMUH102-REC1-064. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and the local laws and regulations. The current guidelines for Good Clinical Practice (Taiwan-and ICH-GCP guidelines) were also applied. The health authorities and the IRBs approved the study protocol and ICF before enrolling subjects. The views of the health authorities and the IRBs were dated and filed.
Patients and Study Methodology
This was a single-center, open-label study. Participants enrolled in this study were patients with liver cirrhosis whose Model for End-stage Liver Disease (MELD) score was between 10 and 15 and Child–Pugh score belonged to class B (7–9). The Child–Pugh score definition was according to Pugh et al. 21 The primary objective was to evaluate the safety of GXHPC1 for patients with liver cirrhosis. The primary endpoints of the safety evaluation included an adverse drug reaction (ADR), suspected unexpected serious adverse reaction (SUSAR), and blood biochemistry within 24 weeks of receiving GXHPC1 injection. Each of ADR, SUSAR, vital function, electrocardiogram (ECG) and blood biochemistry was evaluated and recorded in the case report form at each scheduled visit. The secondary objective was to assess the efficacy of GXHPC1 for patients with liver cirrhosis. The secondary endpoints included efficacy for liver function, METAVIR score 22 , abdominal echo, MELD score, Child–Pugh score, and quality of life within 24 weeks of receiving GXHPC1 injection. Six eligible participants were assigned to receive a single dose of 1 × 108 AD-MSCs that were isolated from the participant’s abdominal fat tissue and expanded in a good tissue practice (GTP) facility (Gwo Xi Stem Cell Applied Technology Co., Ltd.). Cells were resuspended in 1 ml normal saline and infused into liver lobules under sonographic guidance. The data from visits 1–9 were analyzed to evaluate safety and efficacy. Table 1 lists the visit schedule and study procedures.
Visit Schedule and Study Procedures.

a Should be obtained before or at screening visit.
b Laboratory test includes: Biochemistry, hematology, immunological cell markers, and TH1/TH2 cytokine.
c Abdominal echo includes: Score of chronic liver disease, and ultrasound staging of liver fibrosis.
Inclusion Criteria
Subjects who were aged between 20 and 80 years with liver cirrhosis Subjects with MELD score between 10 and 15 Subjects with Child–Pugh score categorized B (7–9) Subjects without mandatory communicable disease (HBV, HCV, HIV, and syphilis) Subjects without rare disorders Subjects with normal coagulation (PT prolonged < 3 s of control, INR < 1.5, bleeding time < 10 min, platelet > 60,000/mm3, hematocrit > 25%) Subjects without autoimmune disease Subjects without acquired immune deficiency disease Subjects without cancer Subjects with body mass index (BMI) > 15 Subjects with alcoholic cirrhosis were willing to abstain from alcohol at least 6 months
Exclusion Criteria
Female subjects of childbearing potential who were pregnant, lactating, and not willing to adopt contraception at screening Subjects who were alcohol abusers at screening Subjects with acute stroke in 1 month and unconsciousness Subjects with acute myocardial infarction or acute heart failure in 1 month Subjects with serious liver dysfunction (Child–Pugh > 10) combined with coagulation dysfunction and ascites mild higher Subjects with acute respiration failure or pneumonia Subjects with kidney failure (eGFR < 30 ml/min/1.73 m2) Subjects with liver abscess combined with other hepatobiliary metastatic carcinoma Subjects with liver abscess Subjects with acute hepatitis Subjects with acute infection Subjects with liver cirrhosis caused by HBV or HCV Subjects diagnosed with carcinoma and receiving treatment or chemotherapy Subjects with schizophrenia or melancholia Subjects received serious surgical operations in 3 months Subjects unable to control hypertension (SBP > 180 mmHg, DBP > 110 mmHg), or diabetes (AC sugar > 200 mg/dl) Others who cannot fit into the trial as evaluated by the investigator
Physical and Laboratory Examination
All patients underwent routine laboratory tests, including a complete blood count, biochemistry panel (including liver function tests glutamic oxaloacetic transaminase [GOT], glutamic pyruvic transaminase [GPT]), bilirubin, albumin, blood urea nitrogen, estimated glomerular filtration rate (eGFR), creatine, α-fetoprotein, ammonia, prothrombin time/partial thromboplastin time, international normalization ratio, abdominal echo, and liver biopsy.
Isolation of Patient AD-MSCs
Adipose tissue (2–5 g) was harvested from the subcutaneous fat of each patient’s abdominal wall during abdominal surgery. Tissue samples were placed in Ca2+/Mg2+-free phosphate-buffered saline (PBS) and immediately transferred to a GTP lab (Gwo Xi Stem Cell Applied Technology Co., Ltd.). Adipose tissue was then removed from the transport media, placed in a Petri dish, and cut into small pieces (1–2 mm3) in the presence of Ca2+/Mg2+-free PBS. The tissue samples were dissociated with 0.1% collagenase I (Invitrogen-Gibco, Carlsbad, CA, USA) via incubation for 60 min at 37°C. After enzymatic digestion, the resultant dispersed cells were collected and cultured in keratinocyte serum-free medium (Invitrogen-Gibco) supplemented with 10% fetal bovine serum (FBS) (HyClone, Logan, UT, USA), N-acetyl
AD-MSC Culture Suspension
The cells were maintained in keratinocyte serum-free medium (Invitrogen-Gibco) supplemented with 10% (v/v) FBS (HyClone, Logan, UT, USA), N-acetyl-
Preparation of GXHPC1
On the day of injection, AD-MSCs were harvested and washed three times with sterile saline. The AD-MSC viability was evaluated using the ADAM-MC™ Automatic Cell Counter (Digital Bio, NanoEnTek Inc., Seoul, Korea). AD-MSCs were resuspended in physiological saline at a final concentration of 1 × 108 cells/ml. For each GXHPC1 injection, 1 × 108 cells in 1 ml physiological saline were injected within 6 weeks of the patient’s enrollment. The health of patients was continuously monitored according to the visit schedule and study procedures (Table 1).
Viability, Immunophenotype, and Safety of GXHPC1
GXHPC1-related quality testing was executed by a third-party certification laboratory (accredited in respect of laboratory by TAF, Accreditation Criteria: ISO/IEC 17025, Accreditation Number: 2800). The viability of the GXHPC1 was assessed with the ADAM-MC™ Automatic Cell Counter (Digital Bio, NanoEnTek Inc., Seoul, Korea). The immunophenotypes of GXHPC1 were analyzed using a BD Accuri C6 flow cytometer (Becton Dickinson, Franklin Lakes, NJ, USA) after labeling with antibodies against the human clusters of differentiation: CD34, CD45, CD90, and CD105 (Becton Dickinson). In addition, presence of microorganisms was assessed by direct inoculation in compliance with the Chinese Pharmacopoeia Chapter 7001 and United States Pharmacopeia (USP) Chapter 71 Sterility Tests. Endotoxin was assessed with a chromogenic quantitative technique in compliance with the USP Chapter 85 Bacterial Endotoxins Test. Mycoplasma was assessed with nucleic acid amplification techniques in compliance with an in-house method (document no. 3-13-016) and a culture method in compliance with the USP Chapter 63 Mycoplasma Tests.
Intrahepatic Injection of GXHPC1
Before intrahepatic injection, GXHPC1 was adjusted to a volume of 2 ml with 1 ml of physiological saline and placed in two injection syringes, each with a volume of 1 ml. After administering general anesthesia intravenously, the right liver lobe of the patient was selected under ultrasound (Toshiba istyle) guidance. Avoiding large blood vessels and bile ducts, a 21G hepatobiliary needle (21 gauge, 200 mm) was used to pierce the right anterior leaf of the liver from the seventh and eighth ribs on the right side of each patient. Once the hepatobiliary needle was positioned, the prepared GXHPC1 was injected. Each injection was divided into three segments: 0.3 ml at 6 cm, 0.3 ml at 5 cm, and 0.4 ml at 4 cm. A total of two positions were injected, 1 cm apart from each other. After the injection, the patient remained in bed for 4 h and pressed the injection wound with a 1 kg sandbag. Vital signs were monitored every hour during the procedure. Thereafter, each patient was observed for 4 h, and follow-up was scheduled and carried out for 24 weeks.
Liver Biopsy and Histology
Paired liver biopsies were performed at baseline and 6 months after GHXPC1 injection. Liver biopsy specimens ≥15 mm in length and ≥1.2 mm in width were used for this study. Paraffin-embedded liver biopsy samples (5 µm thick) were prepared and stained with hematoxylin and eosin and Masson’s trichrome.
Statistical Analysis
The full-analysis set (FAS) population was composed of all subjects received the GXHPC1 medication. The per-protocol (PP) population was composed of all subjects who had ever received the GXHPC1 medication and satisfied the following conditions: no major deviation from the protocol and no prohibited medications. All data were analyzed after the database was locked. According to the protocol and statistical analysis plan (SAP), the statistical analysis of demographic characteristics, and baseline characteristics were performed with the FAS population. The safety endpoints were performed in the FAS population. The efficacy endpoints were performed in the PP population. Statistical analysis was performed using the SPSS 16.0 software (SPSS Inc., Chicago, IL, USA). Safety and efficacy endpoints were evaluated for each patient by comparing the baseline values with post-procedure values. Statistical analysis was performed by analysis of unpaired t-test or by analysis of variance (ANOVA followed by Tukey’s post-hoc test). A p-value <0.05 was considered to reflect a statistically significant difference in values.
Results
Patients
In this study, a total of 14 patients participated in the eligibility screening. Among them, six patients failed to meet the inclusion criteria. For the eight non-screen failed patients, two (004-003 and 008-006) did not receive GXHPC1 and the other six patients were defined as the FAS population. The mean and standard deviation values for age, gender, body weight, height, and BMI for the six evaluated patients were 49.33±9.05 years of age, five (83.33%) male and one (16.67%) female, 62.17±7.47 kg, 162.00±4.56 cm, and 23.66±2.42 kg/m2, respectively (Table 2). Within the FAS population, one subject (009-007) who had mycoplasma pneumonia and violated inclusion criterion 6 (subjects with normal coagulation) and exclusion criterion 6 (subjects with acute respiration failure or pneumonia) was excluded from the PP population. Thus, a total of five patients (four males and one female) met the criteria for the PP population. The disposition and distribution of the enrolled subjects is shown in Fig. 1.
Summary of Demographic Characteristics – FAS.


Disposition of subjects. The safety endpoints were performed in the full-analysis set (FAS; N = 6) population. The efficacy endpoints were performed in per-protocol (PP; N = 5) population.
Viability, Immunophenotype, and Safety of GXHPC1
The mean viability percentage of the AD-MSCs (GXHPC1) as assessed by the ADAM-MC™ Automatic Cell Counter was 95.00 ± 1.79%. The criterion for the clinical use of MSCs is that viability be >70% 23,24 . AD-MSCs (GXHPC1) from all patients were immune-labeled for surface-protein expression and examined by flow cytometry. The AD-MSCs (GXHPC1) were positive for CD90 and CD105 (>95% of cells positive) and negative for CD34 and CD45 (<1% of cells negative). The absence of microbial contamination (bacteria, fungus, or mycoplasma) was assessed and reported by a third-party certification laboratory (TAF 2800) before administration. These results indicated that culture expansion is a feasible approach to large-scale production of GXHPC1 for transplantation (Table 3).
Certificate of Analysis About GXHPC1.
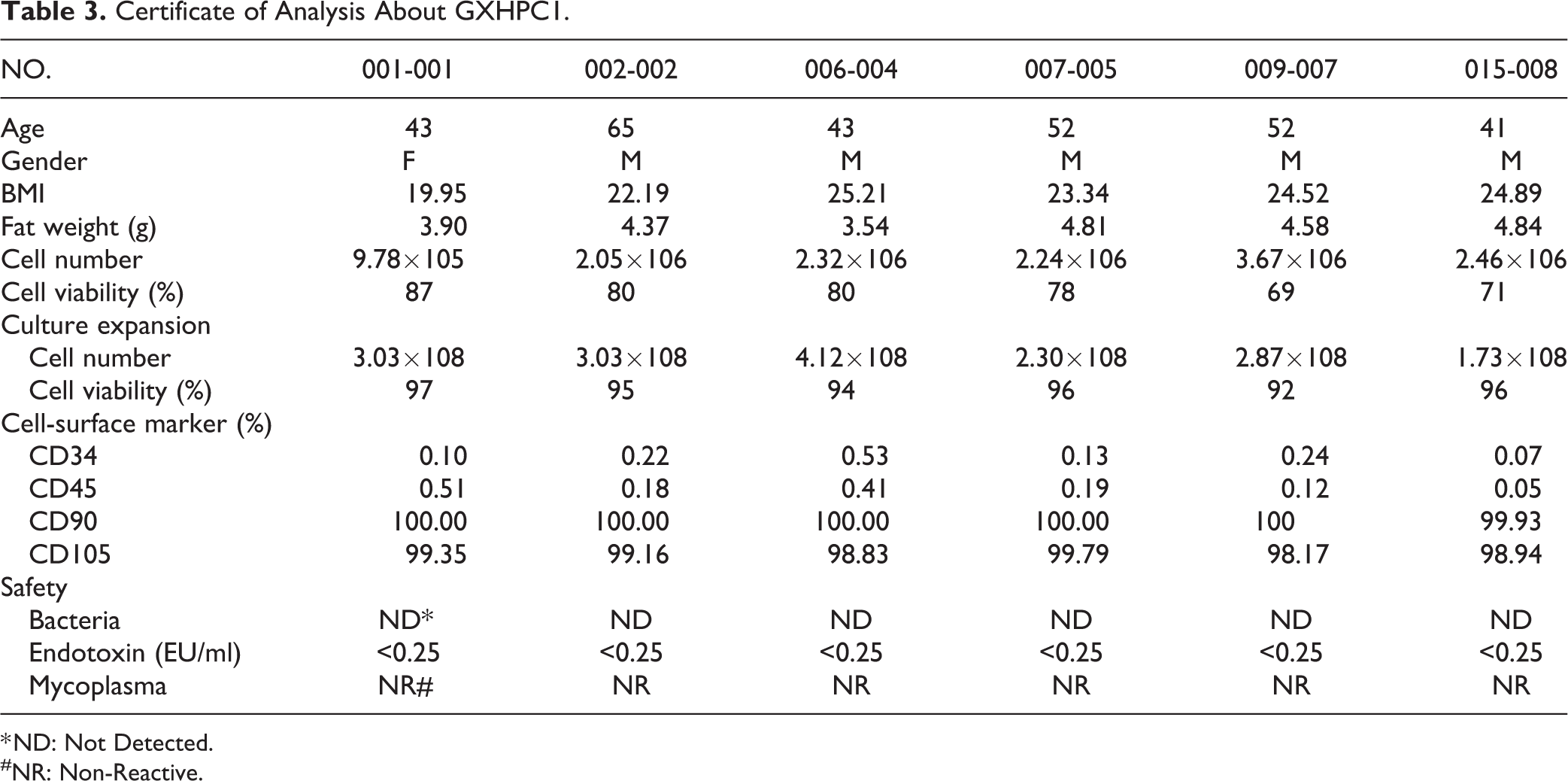
* ND: Not Detected.
#NR: Non-Reactive.
Safety Outcomes
The patients’ general medical history was recorded before entry for the study. The general medical history of enrolled patients was diseases of the gastrointestinal system (50.00%), and respiratory system (33.33%). During the study, all six patients reported adverse events (AEs) and four of these adverse events were classified as serious adverse events (SAEs). The most frequent AEs were “Gastrointestinal disorders” (100.00% incidence), followed by “Infections and infestations” (66.67% incidence) and “Skin and subcutaneous tissue disorders” (50% incidence). These three body systems were the systems that suffered most from AEs, with incidence ≥50%. Among the causality categories of AEs, base on previous medical history all AEs were judged unrelated (24.32%) or unlikely to be related (75.68%) to the study treatment. Patient 009-007 had three SAEs reported for hospitalization due to pneumonia, cellulitis, and gastrointestinal hemorrhage, respectively. Patient 015-008 had a SAE reported for hospitalization due to hemorrhage of esophageal varices. After the causality of these SAEs was assessed, all were considered unlikely to be related, or were unrelated, to the study administration. There were no SUSAR events reported in this study.
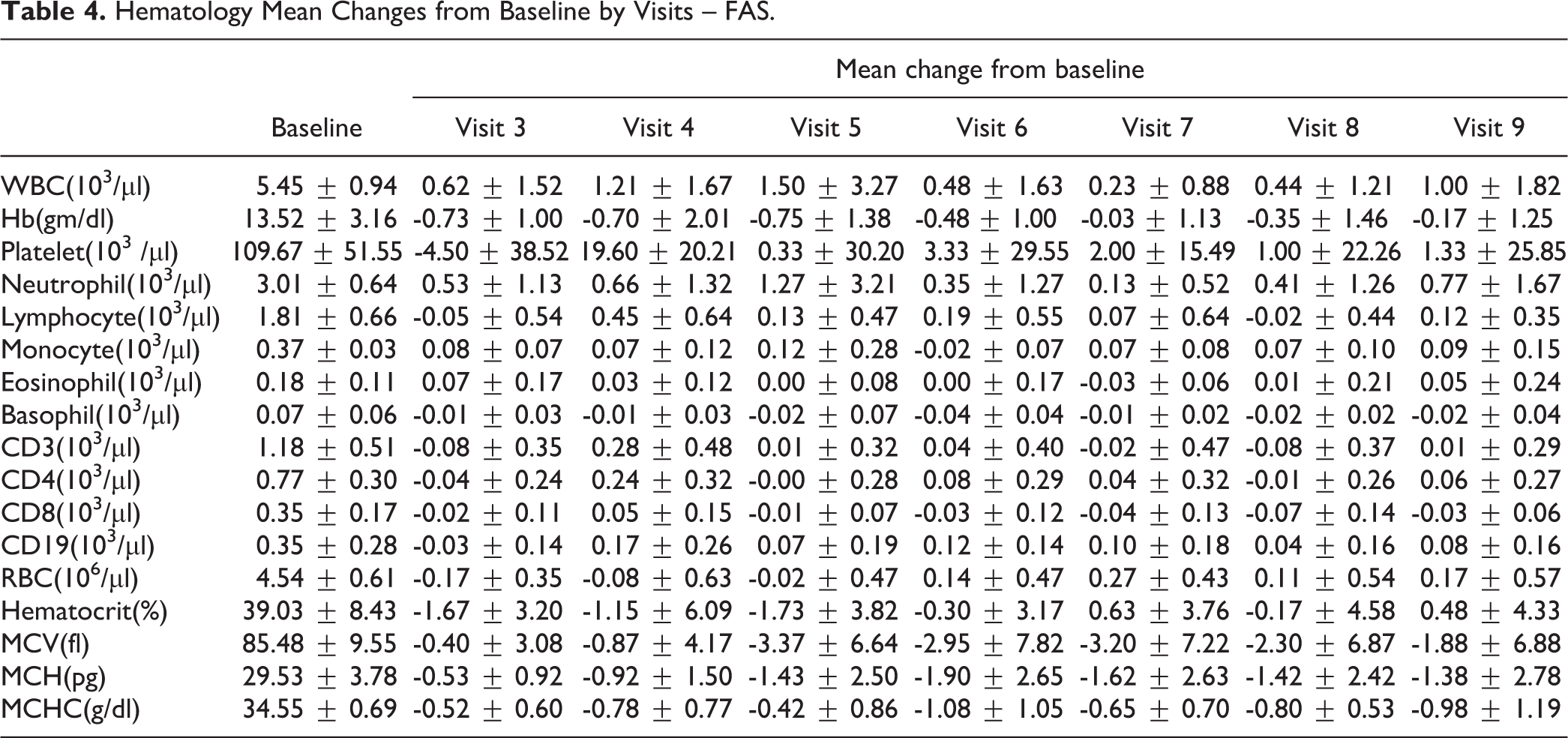
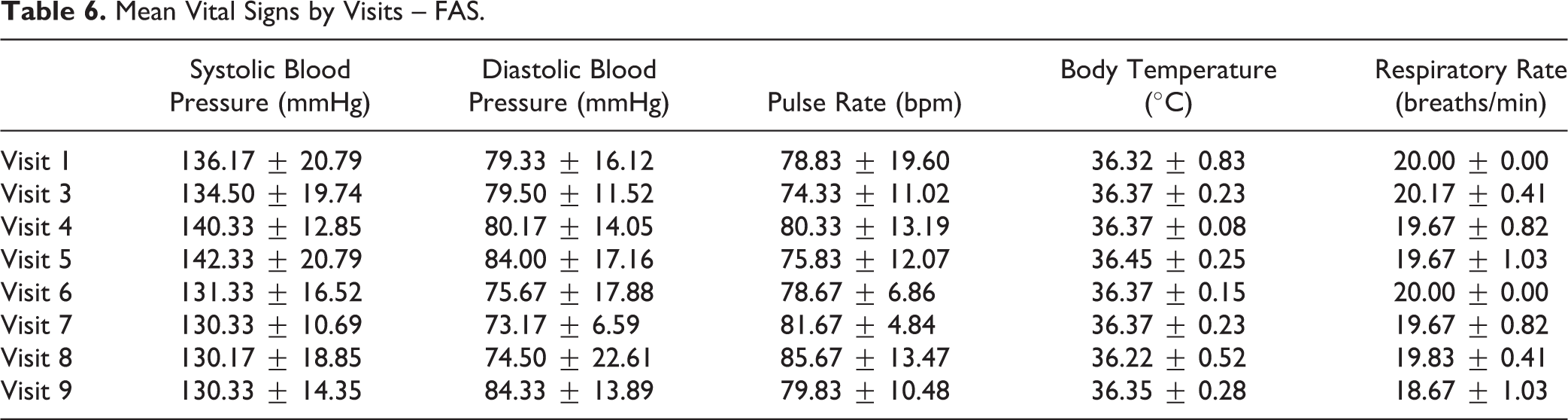
The clinical laboratory safety results were analyzed from visit 1 (baseline) to visit 9. Most of the evaluated items, including hematology (Table 4) and biochemistry (Table 5), revealed no clinically significant abnormalities of the values from the baseline to visit 9. However, TH1/TH2 cytokines, including IL-2, IL-4, IL-5, TNF-α, and IFN-γ, showed a net increase but no clinical significance from the baseline to visit 9. In addition, the administration of GXHPC1 did not affect basic vital functions, and ECG results for the FAS population were all normal and not clinically significant (Table 6).
Hematology Mean Changes from Baseline by Visits – FAS.
Laboratory Mean Changes from Baseline by Visits – FAS.

Mean Vital Signs by Visits – FAS.
The results of the safety evaluation of GXHPC1 indicated that there were no specific findings of changes in the monitored items that caused a safety concern for the use of GXHPC1. Therefore, administration of GXHPC1 can be considered safe for patients with liver cirrhosis.
Efficacy Outcomes
The efficacy of administering GXHPC1 was evaluated for five patients of the PP population (Table 7). Efficacy was assessed based on the improvement of liver function, METAVIR score, abdominal echo, MELD score, Child–Pugh score, and quality of life. Liver function was assessed by net change of GOT and GPT at visits 1, 3, 4, 5, 6, 7, 8, and 9 for the PP population. Four patients (001-001, 002-002, 006-004, and 015-008) had reduced GOT (9.26%–81.20%) and GPT (21.95%–54.39%). Patient 002-002 had the most improved results for GOT and GPT. In contrast, patient 007-005 did not improve with respect to liver function and had higher GOT and GPT from visit 8 to visit 9. These results demonstrated that there was a trend toward improvement in liver functions for the PP population.
Summary of Efficacy Evaluation (Baseline→Visit 9) with GXHPC1 Administration – PP.

Note: + indicates “improved” and – indicates “worse.”
The METAVIR score was accessed by fibrosis and activity scores at visits 2 and 9 for the PP population. For the fibrosis score, two patients (001-001 and 015-008) showed improvement from F4 to F3, whereas the other patients maintained the same fibrosis score. For the activity score, one patient (007-005) showed improvement from A3 to A1, and another (015-008) showed improvement from A2 to A1. One patient (002-002) had a worse score from A2 to A3. Two patients (001-001 and 006-004) maintained the same activity score. Thus, only patient 015-008 showed improvements both in the fibrosis score (F4→F3) and activity score (A2→A1). These results indicated that the administration of GXHPC1 improved some METAVIR scores for the PP population.
Abdominal echo data were presented and assessed by the score of chronic liver disease and ultrasound staging of liver fibrosis at visits 1, 3, 4, 5, 6, 7, 8, and 9 for the PP population. All patients (score ≥ 8) did not have any change in the score of liver fibrosis from visit 1 to visit 9. The Child–Pugh classification was assessed by the prognosis of cirrhosis of the liver at visits 1, 3, 4, 5, 6, 7, 8, and 9 for the PP population. All patients had improvements in the levels of Child–Pugh score from visit 1 to visit 9. Although four of the patients improved from class B to class A, patient 007-005 had improvement from score of 9 to 7 but still remained in class B from visit 4 to visit 9. These results indicated that administration of GXHPC1 improved the Child–Pugh scores for the PP population.
The MELD score was assessed at visits 1, 3, 4, 5, 6, 7, 8, and 9 to evaluate the 3-month mortality for the PP population. Four patients (001-001, 002-002, 006-004, 015-008) had improvements in the MELD score from visit 1 to visit 9, but patient 007-005 had a trend of increasing MELD score from visit 1 to visit 9. These results indicated that administration of GXHPC1 improved the MELD score for most of the PP population.
Quality of life was evaluated based on the four domains of QOL-BREF (physical health, psychological, social relationships, and environment) plus two domains for Taiwan (social relationships and environment) at visits 1, 3, 4, 5, 6, 7, 8, and 9 for the PP population. Most patients in the PP population had improvements in all six domains that comprised the QOL-BREF score from visit 1 to visit 9. Patient 002-002 had improvement only in Domain 3, whereas patient 015-008 improved in Domains 1 and 4. These results revealed that administration of GXHPC1 could improve the quality of life of the PP population; the mean change of for each PP patient from baseline is summarized in Table 7.
Discussion
Recent clinical trials have demonstrated that MSC transplantation has been beneficial to patients with liver failure. However, MSCs from bone marrow procurement may be distressing to patients, and indeed it has proven difficult to obtain a sufficient amount of autologous adult stem cells 25 –28 . GXHPC1 is a cell product that contains autologous AD-MSCs and was developed for the treatment of liver cirrhosis. In this study, we successfully manufactured each patient’s GXHPC1 and achieved consistent quality (Table 3). It is often discussed whether AD-MSCs obtained from patients with cirrhosis are actually functional in clinical cell therapy. To investigate this issue, we previously compared the culture expansion of AD-MSCs from patients with cirrhosis (mean age: 49.3±9.0) with AD-MSCs from healthy donors (mean age: 54.0±3.6). We found no difference in proliferation capacity or cell-surface markers between patients with cirrhosis and healthy subjects (data not shown). All of these results demonstrate that AD-MSCs are a stable and sufficient cell source that can be widely used as a clinical treatment. In addition, culture expansion of AD-MSCs by a commercial process can reach clinical requirements and comply with regulatory guidelines that ensure safety and quality.
This Phase I study was conducted to demonstrate the safety and efficacy of administering GXHPC1 to six patients with liver cirrhosis. Liver cirrhosis refers to late-stage fibrosis of the liver. The safety of this study was evaluated for the FAS population. Although this preliminary trial with six patients led to some severe AEs including “Gastrointestinal disorders,” “Infections and infestations,” and “Skin and subcutaneous tissue disorders,” these AEs were not related to GXHPC1 administration. There were four SAEs observed in this study. Patient 009-007 had three SAEs reported for hospitalization due to pneumonia, cellulitis, and gastrointestinal hemorrhage, respectively. Patient 015-008 had an SAE reported for hospitalization from hemorrhage of esophageal varices. The principal investigator assessed the causality of these SAEs; all were considered unrelated or unlikely to be related to the administration of GXHPC1. Among the evaluated laboratory items, no abnormalities were found in the hematology or biochemistry parameters. In addition, the administration of GXHPC1 did not affect basic vital functions, and ECG results for the FAS population were all normal and not clinically significant. These results lead us to conclude that GXHPC1 treatment is safe and well tolerated for patients with liver cirrhosis.
Recently, a large systematic review and meta-analysis showed that compared with conventional treatment, the benefit of stem-cell therapy appeared to be not significant in improving the liver function and survival. This study pointed out that differences of cell delivery route, dosage, and characterization of included patients may influence the treatment response 29 . The efficacy of GXHPC1 was evaluated by the improvement of liver function, METAVIR score, abdominal echo, Child–Pugh score, MELD score, and quality of life for the PP population. Among the five patients of the PP population, four showed improved liver function. Regarding the METAVIR score, improved fibrosis scores and activity scores were observed for the PP population. Patient 015-008 had improvements both in the fibrosis score and activity score. Furthermore, 80% (4/5) of patients exhibited improvements in the Child–Pugh and MELD scores from visit1 to visit 9. According to Suk et al., patients with alcoholic cirrhosis received a hepatic arterial injection of autologous BM-MSCs one time (5 × 107 BM-MSCs total) or two times (1 month apart, a total of two injections, 1 × 108 BM-MSCs total) 30 . After follow-up of 6 months, the Child–Pugh scores improved ∼18% and ∼13%, respectively. Compared with Suk et al.’s result, we treated patients with alcoholic cirrhosis with autologous AD-MSCs in a one-time (1 × 108AD-MSCs total) intrahepatic injection. The average Child–Pugh scores improved ∼28% (7.6 ± 0.9 versus 5.4 ± 0.9). The above finding may suggest that a greater number of cells and a one-time MSC transplantation may have more beneficial effects. In addition, most patients had improvements in each domain of the QOL-BREF score from visit 1 to visit 9. Notably, patients 001-001and 015-008, with a history of liver cirrhosis less than 2 years (1.57 and 1.42 years, respectively), showed improvements in five items of the efficacy evaluation.
In this experiment, all patients had liver cirrhosis caused by alcoholism. In addition to alcohol abuse, there are many reasons for formation of liver cirrhosis. For example, hepatitis B infections are considered as primary causes of hepatic fibrosis 31 –33 . There are ∼350 million hepatitis B virus (HBV) carriers in the world. However, it has been reported that HBV replication can be detected in MSCs from bone marrow and hematopoietic stem cells from umbilical cord blood 34,35 . BM-MSCs from patients with chronic hepatitis B proliferate defectively and have decreased the expression of growth factor receptors 36 . Xie et al. isolated MSCs from bone marrow of patients with hepatitis B and found that both BM-MSCs and BM-MSCs that were undergoing differentiation into hepatocytes were in fact resistant to HBV infection in vitro 37 . Conversely, BM-MSCs obtained from healthy donors fully supported HBV infection, replication, expression, and secretion, which could make the MSCs a reservoir of virus 35 . Furthermore, it has been reported that BM-MSCs can serve as an extrahepatic virus reservoir by harboring and transporting HBV to injured tissues after transplantation of HBV-exposed MSCs into a mouse model of myocardial infarction 38 . The treatment of autologous BM-MSCs transplantation for chronic hepatitis B is controversial. Wang et al. isolated AD-MSCs from patients with chronic hepatitis B and compared the morphology, growth potency, cell-surface phenotype, and differentiation potential of these cells with those of BM-MSCs isolated from patients with chronic hepatitis B 34 . The results showed that AD-MSCs from patients with chronic hepatitis B could differentiate into functional hepatocyte-like cells. These cells express hepatic-specific markers and produce glycogen and secrete albumin normally. Moreover, AD-MSCs and hepatic-differentiated AD-MSCs are not susceptible to infection by HBV in vitro.
We did not include patients with hepatitis B in this clinical trial. In our laboratory experiment, we isolated and expanded AD-MSCs from the fat tissue of three hepatitis B carriers. In these three cases, HBV loads were not detected (LOD <20 IU/ml, Chung Shan Medical University Hospital, Department of Clinical Laboratory) in each of the cell supernatant, cell wash solution, and the cell pellet. HBV load was also not detected in extra- or intra-AD-MSCs and did not increase with culture expansion. AD-MSCs of hepatitis B carriers are not significantly different from healthy donor AD-MSCs in terms of morphology, viability, doubling time, cell markers, and differentiation potential (unpublished data).These data suggest that the AD-MSCs from HBV carrier donors can be used as one of the sources to improve disease with autologous transplantation of stem cells. This may prove that the liver cirrhosis patients with HBV can also use autologous AD-MSCs for GXHPC1 treatment and obtain a considerable effect. This population should be considered in future studies.
In summary, administration of GXHPC1 did not cause any safety issues based on data for ADR and SUSAR, and resulted in a tendency of improvements of liver function, METAVIR score, Child–Pugh score, MELD score, and quality of life in patients with liver cirrhosis. Thus, this study showed that intrahepatic injection of GXHPC1 could be considered as a safe and feasible for the treatment of liver cirrhosis.
Footnotes
Ethical Approval
Ethical approval to report this case was obtained from the Institutional Review Boards (IRBs) of China Medical University Hospital (CMUH). The approval number was CMUH102-REC1-064.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Institutional Review Boards (IRBs) of China Medical University Hospital (CMUH). The approval number was CMUH102-REC1-064.
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.