
Abstract
Adipose-derived stromal cell (ASC) therapy is currently investigated as a new treatment option for patients with ischemic heart disease (IHD). The aim of this study was to evaluate the effect of ASC therapy in patients with chronic IHD measuring myocardial perfusion and cardiac function using cardiac magnetic resonance imaging (CMRI). Patients were included in MyStromalCell trial, a phase II, randomized, double-blinded, placebo-controlled study investigated the effect of ASCs in patients with chronic IHD with preserved left ventricular ejection fraction (LVEF). In total, 41 of 60 patients underwent cine, late enhancement, rest and stress imaging with CMRI. There was a non-significant difference between stress and rest values in maximal signal intensity, a measure of myocardial perfusion, from baseline to follow-up comparing placebo with ASC group (–52.52 ± 88.61 and 3.05 ± 63.17, p = 0.061, respectively). LVEF, myocardial mass, stroke volume, left ventricle end-diastolic volume and end-systolic volume changed non-significantly (–0.5 ± 4.7%, –3.5 ± 13.1 g, –0.7 ± 8.6 mL, 1.9 ± 25.1 mL and 2.6 ± 16.5 mL, respectively) in the placebo group and in the ASC group (0.7 ± 8.6%, 0.9 ± 10.8 g, –0.3 ± 26.1 mL, –3.0 ± 31.5 mL and –2.7 ± 20.4 mL, respectively) from baseline to 6 months follow-up. The amount of scar tissue was unchanged in the placebo group by 0.0 ± 1.6 g, p = 1.0 and in the ASC group with –0.3 ± 2.3 g, p = 0.540. There was no difference between the groups. There was a non-significant trend toward increased myocardial perfusion but no significant changes in functional parameters or amount of scar tissue in patients treated with ASCs compared with patients allocated into the placebo group.
Keywords
Introduction
The main function of the heart is to pump blood around to supply the body and itself with oxygen and nutrients. Coronary arteries are essential in the process of supplying oxygen and nutrients to the myocardium, a process which had been already suggested in the 13th century 1 . A significant amount of atherosclerosis results in reduced myocardial blood perfusion and reduced function of the heart 2 . This in turn can cause chest pain (angina) and shortness of breath (dyspnea).
Cardiac magnetic resonance imaging (CMRI) is a non-invasive imaging modality, which can be used for the assessment of cardiac function, morphology and myocardial perfusion without using ionizing radiation 3 –5 . Images obtained using CMRI have a good temporal and a high spatial resolution, and thus may be a useful tool in the evaluation of therapies targeting perfusion abnormalities 6 .
Cell-based therapies are being intensively investigated as a new treatment option for patients with ischemic heart disease (IHD). Recently, the effect of mesenchymal stromal cell therapy has been evaluated by imaging modalities in patients with IHD without or with heart failure, and demonstrated improved left ventricular ejection fraction (LVEF), changes in the dimension of cardiac chambers and showed a tendency toward a reduced amount of scar tissue 7,8 .
We have recently finalized The Mesenchymal Stromal Cell (MyStromalCell) study, a phase II, randomized, double-blinded, placebo-controlled study investigating the effect of vascular endothelial growth factor-A165-stimulated adipose-derived stromal cells (ASCs) in patients with chronic IHD with preserved LVEF 9 . The study was neutral in its primary endpoint bicycle exercise test 10 . However, there was a significant increase in bicycle exercise test in time duration and exercise capacity in the ASC group from baseline to 6 months follow-up, which was not seen in the placebo group.
The aim of this sub-study in the MyStromalCell study was to evaluate the effect of ASC therapy on left ventricle myocardial perfusion and function in patients with chronic IHD using CMRI.
Materials and Methods
Patient Population
All included patients gave written informed consent. The study complied with the Declaration of Helsinki and was approved by the National Ethical Committee (02-268856) and Danish Medicines Agency (2612-2867). In addition, the study was registered in clinicaltrials.gov (NCT01449032).
Patients aged 30–80 years with chronic IHD, refractory angina or angina-equivalent dyspnea despite optimal medical therapy, LVEF > 40% and at least one significant coronary artery stenosis without any options for revascularization were enrolled in MyStromalCell trial 9 . A total of 60 patients were included to investigate the effect of vascular endothelial growth factor-A165 (R&D Systems, Minneapolis, MN, USA) stimulated ASCs. All patients were considered for CMRI (MAGNETOM Avanto, 1.5 T, Siemens, Erlangen, Germany). However, 19 patients did not have a CMRI with contrast injection due to claustrophobia, contraindications for CMRI or creatinine > 130 µmol/L.
The patients were blindly randomized in 2:1 ratio to receive ASCs or saline injections, respectively. The ASCs were obtained from abdominal adipose tissue and culture expanded as previously described 9 . The cells were injected into the border zone between viable and ischemic myocardial tissue using a NOGA Myostar® catheter (NOGA® system, Biologics Delivery Systems, CA, USA) in 10–15 injections of 0.2 mL of ASCs or saline after electromechanical mapping of the left ventricle endocardium 9 .
Protocol
CMRI was performed at baseline prior to and 6 months after ASC therapy. During the examinations the clinical condition, electrocardiogram (ECG), blood pressure and heartbeat was monitored. The patients were instructed to abstain from caffeine-containing products for 24 h before the examination. Moreover, they had to refrain from long-acting nitrates for at least 18 h prior the examination.
Cardiac Magnetic Resonance Imaging
CMRI was performed using a clinical MAGNETOM Avanto 1.5-Tesla scanner (Siemens, Germany) with a 6-channel cardiac chest coil combined with back surface coils. The patient was placed in a headfirst supine position and had two 18- and 20-gauge intravenous catheters inserted into the left and right ante-cubital veins, respectively. Contrast agent and adenosine for the stress perfusion imaging were administrated through separate power injectors.
Scout images were obtained first. Then the short-axis cine images were acquired using an ECG-gated, balanced steady-state free precession gradient-echo sequence with retrospective gating at end-expiratory breath hold. The scan rate was 25 images per cardiac cycle covering the entire length of the heart.
After short-axis cine images, rest perfusion imaging was performed with three short-axis slices (basal, mid-ventricular and apical) during first-pass of gadolinium. The gadolinium chelate (Gadovist; Bayer Schering Pharma, Berlin, Germany) was administrated as a bolus of 0.1 mmol/kg body weight at a rate of 5 mL/s immediately followed by 15 mL of saline with the same rate of injection from the power injector. The rest imaging was ECG-gated and obtained at end-expiratory breath hold with single-shot hybrid gradient-echo saturation recovery TurboFlash sequence (echo-time, 1.14 ms; repetition time, 190.92 ms; flip angle, 12°; field of view, 360 × 360; matrix, 192 × 125 mm; GRAPPA acceleration factor, 2; slice thickness, 8 mm). Fifty dynamic acquisitions were acquired with the three slices per cardiac cycle.
To quantify the scar tissue, late gadolinium enhancement images were acquired as breath-hold, ECG-gated, inversion recovery fast gradient-echo images 10–20 min after rest perfusion imaging. The inversion time was set to null the myocardium best (250–380 ms) and images were acquired covering the entire length of the left ventricle.
At least 25 min after the first injection of contrast, stress perfusion imaging was performed with the same settings and image position used during rest perfusion imaging. The stress images were obtained 2.5 min after start of adenosine infusion, which was given as a continuous infusion of 140 μg/kg/min, after another bolus injection of 0.1 mmol/kg gadolinium followed by 15 mL of saline. Adenosine infusion was stopped immediately after the images were acquired.
CMRI Analysis
All images were analyzed using CVI42 (Circle Cardiovascular Imaging Inc., Calgary, Canada).
The myocardial perfusion is related to slope which was calculated from time-signal intensity curves obtained after injection of contrast as the rate of increase in signal intensity. Moreover, myocardial perfusion is related to maximum signal intensity (maxSI) which was also derived from time-signal curves. Slope and maxSI were obtained for both rest and stress images (Fig. 1). Myocardial perfusion difference (MPD) was calculated as difference between stress and rest data while myocardial perfusion reserve (MPR) was calculated as the ratio between stress and rest values.

Signal intensity-time curves for left ventricle blood pool and for each myocardial sector. Maximum signal intensity (MaxSI) and slope for each sector can be calculated and are correlated to the myocardial perfusion. MaxSI and slope is indicated for the anterior-septal sector (yellow sector).
The endo- and epicardial borders of the myocardium were manually traced on short-axis images, late enhancement images, rest and stress perfusion images.
LVEF, left ventricle end-diastolic volume (LVEDV), left ventricle end-systolic volume (LVESV), stroke volume and myocardial mass was obtained from the data output of the short-axis cine images. The amount of scar tissue was calculated from late enhancement images. The images were traced and analyzed by the consensus of two experienced physicians blinded to the treatment allocation.
Invasive Coronary Angiography
Standard clinical techniques were used to perform the invasive coronary angiogram. Stenosis of more than 70% was considered significant.
Statistical Analysis
Data analysis was performed using SPSS version 23 (SPSS Inc., Chicago, Illinois, USA). Continuous variables are presented as mean ± standard deviation. Categorical variables are presented as numbers and percentages. Paired and unpaired t-tests were used for comparison of continuous data within groups and for comparison between groups, respectively. One-way analysis of variance (ANOVA) was used to compare means between more than two groups and no further analysis was performed. Two-tailed probability values < 0.05 were considered significant.
Results
Study Patients
This study included in total 41 of the 60 original patients from MyStromalCell trial, 13 patients from the placebo group and 28 patients from the ASC group. Of the 19 patients not included, 10 were not eligible for CMRI due to either implantation of pacemaker or implantable cardioverter defibrillator unit, seven patients had claustrophobia and two patients were not suitable for the scanner due to a body mass index of 37.6 kg/m2 and 38.6 kg/m2.
The abdominal liposuction volume amounted 92 ± 27 mL and the stromal vascular fraction resulted in 95 ± 60 × 106 cells. The patients in the ASC group were treated with 61.1 ± 38.9 × 106 ASCs after the cells were culture expanded for two passages under good manufacturing practice conditions for 33 ± 16 days. On average, 13 and 14 injections were given to the patients in the placebo and ASC group, respectively. Before the intramyocardial injections of ASCs or placebo, a 3D map of the left ventricle was created with the NOGA-XP system and intramyocardial injections with Myostar injection catheters (Biologics Delivery Systems Group, Johnson & Johnson, USA) were performed of 0.2 mL of placebo or ASCs into viable myocardium (unipolar voltage of >0.6 mV) in the border zone of an area of scar tissue (unipolar voltage of <0.6 mV).
Table 1 summarizes the baseline characteristics of the study population. The mean age was 66.2 ± 7.6 and 64.1 ± 9.7 years in the placebo group and in the ASC group, respectively. At baseline, the creatinine was 95 ± 24 and 82 ± 17 µmol/L, and estimated glomerular filtration rate/1.73 cm2 71 ± 17 and 79 ± 13 mL/min in the placebo group and in the ASC group, respectively. There were no significant differences between the two groups.
Baseline Characteristics of Patients Undergoing Cardiac Magnetic Resonance Imaging.

AMI: acute myocardial infarction; ASC: adipose-derived stromal cell; BMI: body mass index; CABG: coronary artery bypass grafting; eGFR: estimated glomerular filtration rate /1.73m2; Hgb A1c: hemoglobin A1c; PCI: percutaneous coronary intervention.
Values are mean ± SD or number (%).
The invasive coronary angiography demonstrated that 10 out of 13 patients in the placebo group had one-vessel disease while 22 out of 28 patients in the ASC group had one-vessel disease. The rest of the patients had two-vessel disease, and other vessel territories were either well nourished through native vessels or bypass grafts.
Rest and Stress Perfusion Data
Table 2 shows the slope and maxSI data, as a measure of myocardial perfusion, at rest and stress for patients randomized into the placebo group and ASC group at baseline and at 6 months follow-up.
Global Rest and Stress Values for Slope and Maximum Signal Intensity (maxSI) as a Measure of Myocardial Perfusion at Baseline and 6 Months Follow-up in the Placebo Group and in the Adipose-Derived Stromal Cell (ASC) Treated Group. The Slope Values are Decreased and maxSI Increases when the Myocardial Perfusion Increases During Adenosine Stress Imaging Compared with Rest Values.
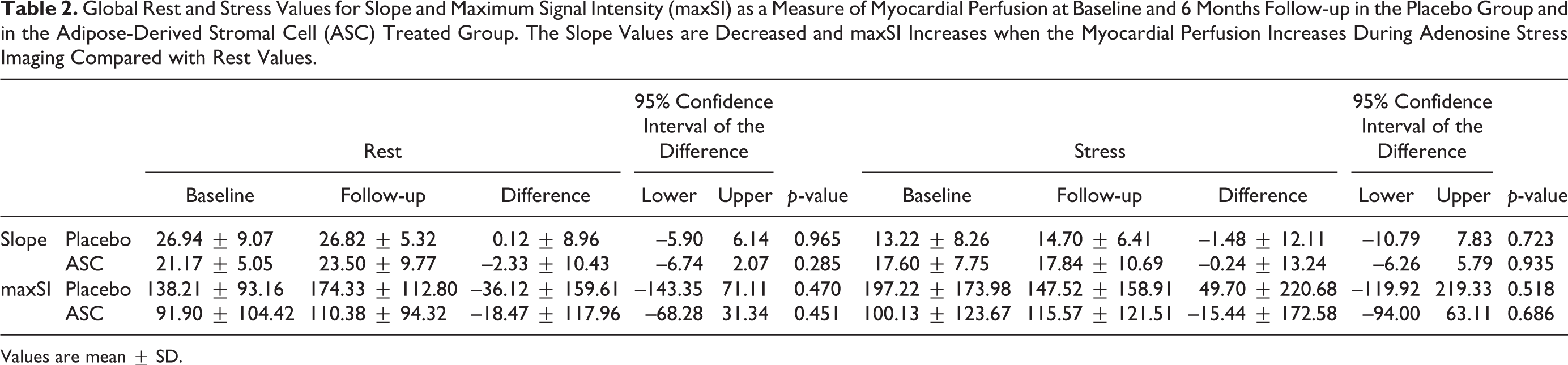
Values are mean ± SD.
There were no differences in global slope and maxSI from baseline to follow-up for rest or adenosine stress data within the groups or between the groups.
The difference between stress and rest values, MPD for slope and maxSI, and the ratio between stress and rest values, MPR for slope and maxSI did not change significantly from baseline to 6 months follow-up in the placebo group or ASC group (Table 3). There were no significant differences between the groups for the calculated changes from baseline to follow-up for MPD and MPR for slope and maxSI. However, the difference in MPD maxSI from baseline to follow-up was –52.52 ± 88.61 and 3.05 ± 63.17, p = 0.061, in the placebo group and in the ASC group, respectively (Table 4).
The Difference Between Stress and Rest Values as Myocardial Perfusion Difference for Slope (MPD_slope), Myocardial Perfusion Difference for Maximal Signal Intensity (MPD_MaxSI) and the Ratio Between Stress and Rest as the Myocardial Perfusion Reserve for Slope (MPR_slope) and for Maximal Signal Intensity (MPR_maxSI) at Baseline and 6 Months Follow-up in the Placebo Group and Adipose-Derived Stromal Cell (ASC) Group.

Values are mean ± SD.
The Change in Maximal Signal Intensity (maxSI) between Rest and Stress (Myocardial Perfusion Difference) from Baseline to Follow-up Scan for Patients in Placebo and Adipose-Derived Stromal Cell (ASC) Group Evaluated Global Values (all Slices) and for Each Slice Separately.
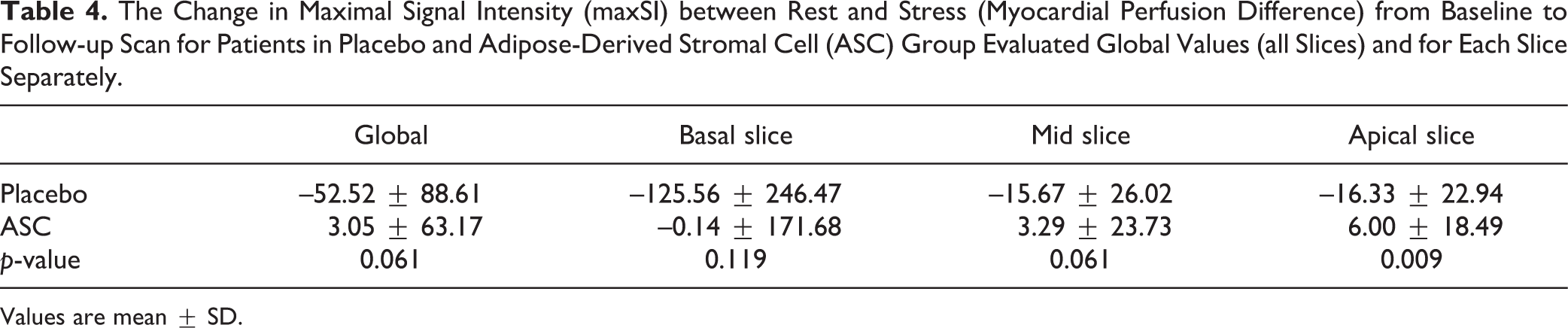
Values are mean ± SD.
There was a trend observed for increased myocardial perfusion (maxSI) between groups when dividing the ASC treated into two groups: patients receiving less than mean ASC and patients receiving more than mean ASC. For patients in the placebo group, the global maxSI difference between stress and rest changed from baseline to follow-up with –52.52 ± 88.61, while for patients in the low ASC group there was a change of –2.39 ± 48.81 but in the high ASC group it increased by 9.03 ± 78.39 (p = 0.167, for comparison between three groups). Looking at the three slices (basal, mid and apical), the maxSI were reduced in the placebo group from baseline to follow-up while there was a trend toward increased or less reduced maxSI for patients in the low ASC group or high ASC group (Table 5).
The Change in Maximal Signal Intensity (maxSI) between Rest and Stress (Myocardial Perfusion Difference) from Baseline to Follow-up Scan for Patients in the Placebo Group, for Patients who Received Less than Mean Number of Adipose-Derived Stromal Cells (ASCs) (Group 1) and for Patients Receiving more than Mean ASCs (group 2). The Mean Number of ASCs were 61.1 ± 38.9 × 106 ASCs. Global Values (all Slices) and for Each Slice Separately.

Values are mean ± SD.
Functional and Late Enhancement Data
LVEF and myocardial mass were reduced non-significantly in the placebo group from baseline to 6 months follow-up (–0.5 ± 4.7% and –3.5 ± 13.1 g, respectively) while they were increased non-significantly in the ASC group (0.7 ± 8.6% and 0.9 ± 10.8 g, respectively) (Table 6). Stroke volume was reduced both in the placebo and ASC group (–0.7 ± 8.6 mL, p = 0.861 and –0.3 ± 26.1 mL, p = 0.959, respectively).
Changes in Left Ventricle Function, Cardiac Muscle Mass and Scar Tissue in the Placebo Group and the Adipose-Derived Stromal Cell (ASC) Treated Group from Baseline to 6 Months Follow-up.
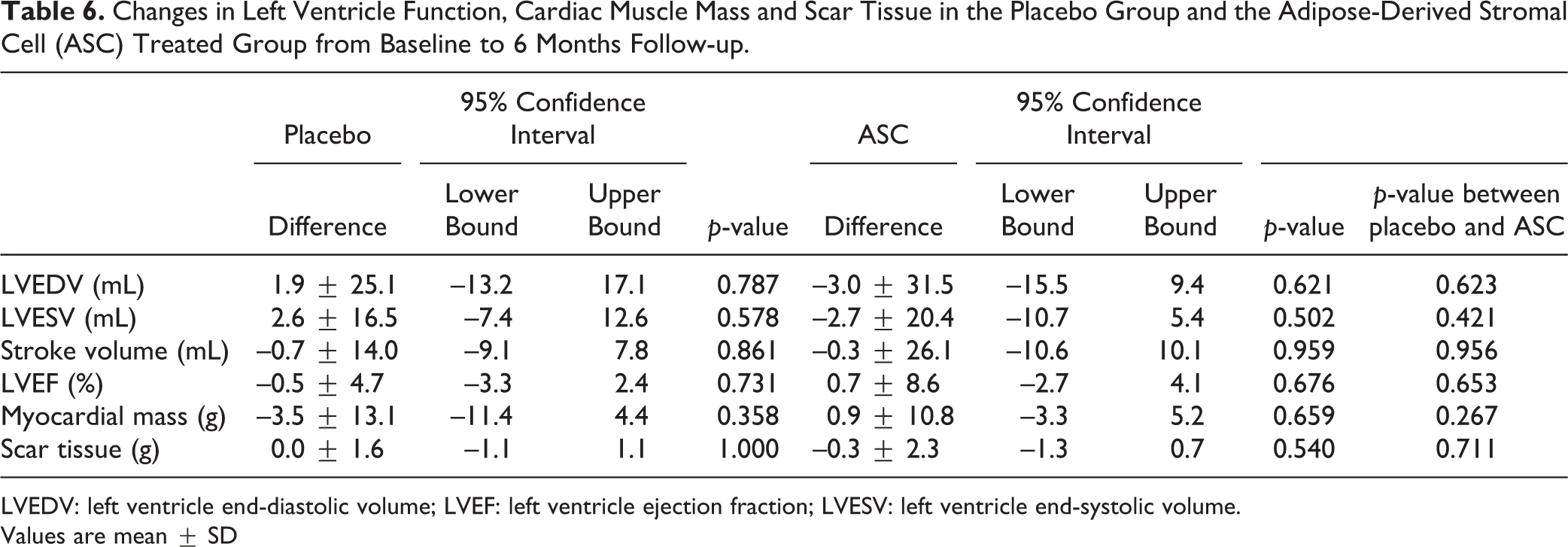
LVEDV: left ventricle end-diastolic volume; LVEF: left ventricle ejection fraction; LVESV: left ventricle end-systolic volume.
Values are mean ± SD
There was a non-significant increase in LVEDV (1.9 ± 25.1 mL, p = 0.787) and in LVESV (2.6 ± 16.5 mL, p = 0.578) from baseline to 6 months follow-up in the placebo group while LVEDV and LVESV decreased non-significantly in the ASC group by –3.0 ± 31.5 mL (p = 0.621) and –2.7 ± 20.4 mL (p = 0.502), respectively.
There was no change in scar tissue in the placebo group (0.0 ± 1.6 g, p = 1.000) or in the ASC group (–0.3 ± 2.3 g, p = 0.540).
However, there were no significant differences between baseline and 6 months follow-up for functional data and scar tissue or between the two groups (Fig. 2).
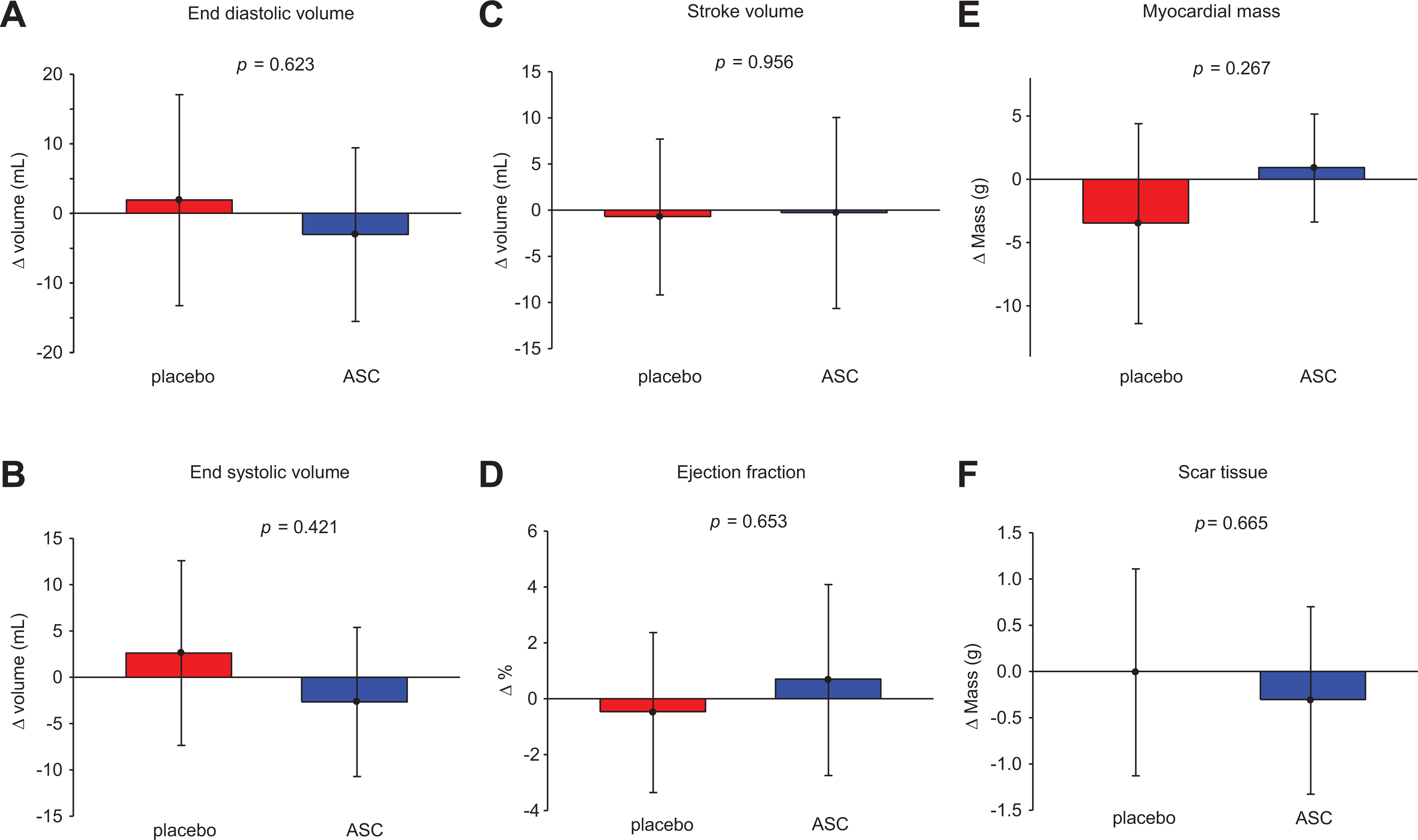
Differences between groups from baseline to 6 months follow-up for left ventricle (A) end-diastolic volume, (B) end-systolic volume, (C) stroke volume, (D) ejection fraction, (E) myocardial mass and (F) scar tissue.
Discussion
In this study, CMRI was used for evaluation of changes in global myocardial perfusion, left ventricle function and structure in the first-in-man randomized, double-blind, placebo-controlled clinical trial, MyStromalCell trial, using vascular endothelial growth factor-A165-stimulated autologous ASCs in patients with chronic IHD and refractory angina.
The primary endpoint bicycle exercise test in MyStromalCell trial showed a significant increase for patients treated with ASCs but not for the placebo patients from baseline to 6 months follow-up but no significant differences between the groups 10 . Even though we were not able to show any significant changes in left ventricle parameters, the amount of scar tissue or myocardial perfusion was measured using CMRI.
The main problem in our patient population is reduced myocardial perfusion due to coronary artery stenosis, resulting in angina. Our myocardial perfusion data were a global evaluation. We did not quantify absolutely the myocardial perfusion in mL per gram of myocardial tissue per minute to evaluate the changes, which could be of interest and especially in the target regions or at a vessel territorial level. It is difficult to identify the areas of ASC injections, and thus it is very difficult to measure the myocardial perfusion locally in the area of injections. Moreover, it is well known that there exists a trans-mural myocardial perfusion gradient, and an evaluation of myocardial perfusion of that gradient might have shown some other results of our data. However, there was a trend toward a significant difference in MPD maxSI from baseline to follow-up between placebo and ASC group, which may be a sign of increased myocardial perfusion in the ASC group.
Previously, two studies using freshly isolated unselected adipose-derived cells in patients with ischemic heart failure (PRECISE study, NCT00426868) and in patients with acute myocardial infarction (APOLLO study, NCT00442806) have been published 11,12 .
In the PRECISE study, a randomized controlled trial to test the effect of intramyocardial-delivered adipose-derived freshly harvested non-culture-expanded cells in 27 patients with ischemic heart failure, left ventricle myocardial mass measured by CMRI increased significantly in the active group but not in the placebo group. The APOLLO trial, a randomized study to test the effect of intracoronary-delivered adipose-derived freshly harvested non-culture-expanded cells in 14 patients with ST-elevation myocardial infarction, demonstrated a non-significant improved LVEF of 5.7% between placebo group and the active group measured by sestamibi single photon-emission computed tomography (p = 0.114). When using CMRI, an increase in LVEF of 4.6% (p = 0.091) between groups from baseline to 6 months follow-up was demonstrated. Moreover, there was a decrease in infarct size in the active group but not in the placebo group, but no significant difference between the groups (p = 0.48). The visual rest perfusion defect was reduced in the active group but not in the placebo group. Nevertheless, there were no significant differences between the two groups.
Intramyocardial-delivered bone marrow-derived mesenchymal stromal cells, in an open study of 31 patients with chronic IHD, refractory angina and preserved left ventricle function, showed improved CMRI-measured LVEF and wall thickness 8,13 .
In the MSC-HF trial, a significant improvement in LVEF, LVESV, stroke volume and myocardial mass was demonstrated in patients with ischemic heart failure treated with bone marrow-derived mesenchymal stromal cells compared with the placebo group 7 .
Preclinical studies in rats have demonstrated that intramyocardial-delivered culture-expanded ASCs result in an increase in LVEF, wall thickness and reduction of infarct size assessed by echocardiography and 18F-FDG microPET imaging 14,15 .
Good correlation between slope and quantified myocardial perfusion based on Fermi function deconvolution in healthy individuals has been shown 16 . In addition, CMRI-measured semi-quantitative myocardial perfusion has shown good correlation to quantitative CMRI-measured myocardial perfusion, rubidium-82 positron emission tomography and to 320-multidetector computed tomography-measured qualitative myocardial perfusion 17 –19 . However, in scar tissue the slope derived from the time-signal curve after injecting contrast is decreased compared with normal tissue due to reduced blood perfusion 20 .
There are several limitations in our study that might have had an influence on our results. The number of patients is rather small, and the 2:1 randomization might then be a problem due to the relatively few placebo patients compared with the ASC patients.
Moreover, the present sub-study was not powered to detect changes of left ventricle functional parameters, scar tissue or perfusion data assessed by CMRI. This is a small explorative study with very highly selected patients with preserved cardiac function and a limited number of female patients included. A higher number of patients, the exact area of target and patients with reduced left ventricle function may be needed to detect the changes induced by ASCs. Moreover, the gap between the slices when obtaining the myocardial perfusion scans may also play a role. Furthermore, no correlation between the 3D NOGA map of left ventricle and CMRI images was performed prior to the injections.
The patients received the amount of ASCs reached after two passages of culture expansion. Therefore, the variation of ASC amount received by the patients is also a factor to be considered, and a standardized amount of allogeneic ASC with a higher amount of cells given may show other results than the present.
The linearity between CMRI signal intensity and the contrast agent concentration has only been tested and found valid for low concentrations of gadolinium 21 . In this study, we used a relatively high dose of gadolinium contrast, and this potential non-linearity could have resulted in our non-significant changes for perfusion data. Furthermore, partial volume effect could have played a role in the calculations, thus the ASCs were injected endocardially.
There may be several factors influencing on our perfusion data, for example heart rate, coronary perfusion pressure, ventricle contraction and vascular tone 22 –25 . In addition, the ability to auto-regulate the myocardial perfusion may be impaired in patients with diabetes mellitus, hypertension, and so on, and due to the altered composition of myocardial tissue after, for example, myocardial infarction and microvascular dysfunction 25 –27 . These patients constituted approximately 40–75% of the study population, and their perfusion data may not follow linearity and thus not be suitable for comparison of treatment effect of ASCs on myocardial perfusion. However, it is a general problem in these patients without any clear solution, and we did not adjust our data for those factors. It can be speculated whether some subgroups are better responders to cell therapy due to the factors mentioned above.
Conclusion
In conclusion, the present study did not show a significant change in left ventricle functional parameters, amount of scar tissue or myocardial perfusion in patients treated with ASCs compared with patients allocated to placebo treatment. However, a trend toward significant difference in myocardial perfusion evaluated by maxSI between placebo and ASC group was observed.
Footnotes
Ethical Approval
This study was approved by the National Ethical Committee (02-268856) and Danish Medicines Agency (2612-2867).
Statement of Human and Animal Rights
The study complied with the Declaration of Helsinki. This study did not contain any studies with animal subjects.
Statement of Informed Consent
All included patients gave written informed consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The study is partly supported by grants from Arvid Nilssons Foundation, Rigshospitalets Research Foundation, The Faculty of Health and Medical Science Research Foundation and Aase and Ejnar Danielsens Foundation.