
Abstract
Intracerebral hemorrhage (ICH) is one of the most devastating forms of cerebrovascular pathology. However, its treatment remains a matter of debate among neurosurgeons and neurologists. The study was to explore the efficacy of minimally invasive surgery (stereotactic catheter drainage, SCD) for patients with severe intracerebral hemorrhage (Glasgow Coma Scale, GCS) score ≤ 8 and hematoma volume ≥ 30 cm3) and to determine predisposing factors for good clinical outcome. A total of 75 patients with severe ICH were included in this retrospective study. Patients were assigned to the SCD group (n=38) or the conventional craniotomy group (n=37). Patients were followed up for 12 months postoperatively, and their clinical parameters were compared. During the operation, the SCD group exhibited a lower bleeding volume (p<0.001) and shorter operating time (p<0.001) than the conventional craniotomy group. For postoperative efficacy, the rates of pneumonia and tracheotomy were lower (p=0.002 and p=0.027, respectively), and the duration of hospital and neurosurgery intensive care unit (NSICU) in days were significantly shorter in the SCD group (p=0.046 and p=0.047, respectively). Furthermore, patients in the SCD group showed improved modified Rankin Scale (mRS) scores at discharge (p<0.018) and at 12-month follow up (p<0.001). Predisposing factors for good clinical outcomes were hematoma volume (<50 cm3, 95% confidence interval (CI): 1.043–1.956, p<0.046), initial GCS score (>6, 95% CI: 3.248–187.466, p<0.001), hypertension (none, 95% CI: 1.440–2.922, p<0.001), and treatment modality (SCD, 95% CI: 1.422–3.226, p<0.001). Taken together, SCD surgery is safe and effective in patients with severe ICH and has fewer complications and better clinical outcomes than conventional craniotomy.
Introduction
Intracerebral hemorrhage (ICH) is one of the most devastating forms of cerebrovascular pathology, with twofold to sixfold higher mortality than that for ischemic stroke and a 1-year survival rate less than 50% 1 –3 . ICH accounts for 8 to 30% of all strokes, depending on regional and ethnic differences 4 . The most common location of ICH is the basal ganglia. However, despite the considerably high frequency of ICH within the basal ganglia, its treatment still remains a matter of debate among neurosurgeons and neurologists 1 .
There are two aspects of brain injury induced by ICH: primary brain injury is the initial irreversible tissue injury in the hemorrhage nidus, and secondary brain injury is the progressive cascade of elevated local pressure, edema, and excitotoxicity at the surrounding areas 5 . For patients with mild ICH (Glasgow Coma Scale, GCS score > 12 or volume < 10 cm3), medical treatments, including control of intracranial pressure (ICP) and prevention of complications, are preferably recommended 6 . However, large, life-threatening ICH (GCS score ≤ 8 and volume ≥ 30 cm3), which has a greater rate of disability and mortality, should be evaluated and investigated for therapeutic strategies. Craniotomy is a conventional surgical technique that removes hematoma under direct vision and quickly reduces ICP 7 . However, the International Study of the Treatment of Intracranial Hemorrhage (STICH) I and II trials concluded that there was little benefit for conventional aggressive surgery early after injury compared with conservative medical treatment because of massive surgical trauma 8,9 . Furthermore, the STICH studies also found that early surgery did not significantly decrease the rates of mortality or disability at 6-month follow up 8 .
Recently, stereotactic catheter drainage (SCD), a minimally invasive procedure, has shown great promise for the treatment of ICH and has completely replaced craniotomy for ICH patients with a hematoma volume of 30–50 cm3 and mild disturbance of consciousness 10,11 . However, for patients with severe ICH, few studies have compared the suitability and efficacy of minimally invasive surgery with those of craniotomy. Therefore, the purpose of this study was to identify patients with severe spontaneous basal ganglia hemorrhage after treatment with SCD and evaluate predisposing factors related to good clinical outcomes.
Materials and Methods
Patient Selection
The study was approved by the Ethics Committee. Written informed consent was obtained from all patients whose medical records and radiographic data were used in the present research. All patients were admitted to hospital within 24 h after disease onset. A total of 75 patients (male/female ratio: 48:27; mean age ± standard deviation: 50.9 ± 13.4 years, range 23–75 years) between October 2015 and April 2018 were recruited for this study. A diagnosis of ICH was confirmed by computerized tomography (CT; General Electric Company, Boston, MA, USA) scan of the head and was made according to the diagnostic criteria of the guidelines for the primary prevention of stroke 12 . Patients were divided according to the surgery performed: the SCD group and the craniotomy group.
The inclusion criteria in this study were as follows: (a) diagnosis of ICH that met the criteria of spontaneous ICH; (b) hematoma located in the basal ganglia (internal and/or external capsule, caudate nucleus, putamen, or more than one of the abovementioned structures); (c) hematoma volume ≥ 30 cm3; (d) preoperative GCS score ≤ 8; (e) age ≤ 75 years; and (f) hospital admission within 24 h of onset of symptoms. The exclusion criteria were as follows: (a) cerebral hemorrhage induced by intracranial aneurysm, arteriovenous malformation, infarction, tumor, or trauma; (b) hemorrhage originating from the cerebellum, brainstem or lobes; (c) coagulation disorders; (d) serious systemic diseases involving the heart, lungs, kidneys, etc. before symptom onset; or (e) prior history of stroke with neurological deficits.
Surgical Procedures
Stereotactic Catheter Drainage
The projection of the puncture target was marked on the temporal scalp according to CT imaging before surgery. The puncture plane was established by connecting the puncture point of the forehead and the projection point of the scalp surface. A 3 cm long, transverse incision was made within the hairline of the forehead with the puncture point as the center. Bone foramen was formed with a diameter of 1 cm. After dura dissection and sharp separation of arachnoid, a 12F external ventricular drainage tube (Yangzhou Xinxing silicone factory, Yangzhou City, Jiangsu Province, China) was used to penetrate the puncture plane from the upper part of the hematoma to the target lower part of the hematoma assisted by the stereotactic instrument and an ICP probe (Johnson & Johnson, New Brunswick, NJ, USA) placed into brain parenchyma along with the tube. Aspiration of the liquefied hematoma was performed with a 20 ml syringe (Becton, Dickinson and Company, Franklin Lakes, NJ, USA), and the ICP values were monitored dynamically. The drainage tube was drawn through the subcutaneous tunnel and connected with an external drainage bag (Shandong Freda Medical Equipment Co. Ltd., Jinan City, Shandong Province, China). After the operation, the hematoma cavity was perfused with 50,000 U urokinase (Nanjing Nanda Pharmaceutical Co. Ltd., Nanjing City, Jiangsu Province, China) daily for 4 h, and CT was monitored dynamically. When the residual hematoma was less than 10 cm3, the drainage tube and ICP probe were removed.
Conventional Craniotomy
Traditional frontotemporal craniotomy was used to remove the hematoma via cortical fistula or separation of the lateral fissure, and the drainage tube (Yangzhou Xinxing silicone factory) was retained in the hematoma cavity. Finally, the bone flap was removed 13 .
Concomitant Care and Interventions
All patients were cared for in a neurosurgical intensive care unit (NSICU) until they were considered stable enough to transfer to a stepdown unit or general floor unit. All patients received medical management according to the guidelines of the American Heart Association/American Stroke Association Stroke Council for the treatment of patients with spontaneous ICH 12,14 , including control of blood pressure, blood sugar, ICP and gastric protection (nutritional support), and the prevention of other complications.
Evaluation of the Curative Effect and Patient Follow Up
The evaluation of the curative effect includes assessment of the intraoperative and postoperative efficacy. For intraoperative effects, the following parameters were included: intraoperative bleeding, hematoma clearance, and duration of operation. For postoperative effects, the evaluated parameters of short-term outcomes were as follows: (a) operative complications, such as rate of pneumonia, rebleeding, intracranial infection, tracheotomy, and second operation; and (b) duration of hospital stay in days and duration of NSICU stay in days. Follow-up data were collected at 12 months after onset using the modified Rankin Scale (mRS). An mRS score of 0–2 was defined as favorable, while an mRS score of 3–6 was defined as unfavorable 15 .
Statistical Analysis
All statistical analyses were performed using the SPSS 19.0 software package. Values are presented as the mean ± standard deviation (SD). Quantitative data were analyzed by the two-sample t-test, while categorical data were compared using chi-square tests. Univariate analysis was performed to determine the effect of age, sex, initial GCS score, hematoma volume, treatment modality, and underlying conditions such as hypertension and diabetes mellitus on the mRS score at the 12-month follow up. Multivariate logistic regression analysis was then performed on variables with an unadjusted effect and a p value < 0.05 in the univariate analysis to determine independent associations between favorable outcome and other factors.
Results
General Preoperative Data
Demographic characteristics of patients in the SCD and craniotomy groups prior to treatment are presented in Table 1. Data from a total of 75 consecutive patients with ICH in the basal ganglia were collected in this study; 38 patients were enrolled in the SCD group, and the remaining 37 were enrolled in the craniotomy group. The mean patient age was 49.8±14.0 years and 52.0±12.9 years for the SCD and craniotomy groups, respectively (p = 0.489). The mean hematoma volume was 57.3±20.7 cm3 for the SCD group and 59.9±20.0 cm3 for the craniotomy group (p = 0.593). There were no significant differences between the two groups with regard to sex, initial GCS score, initial ICH score, and underlying conditions (e.g., hypertension and diabetes mellitus).
Patient Demographic Characteristics for Each Group Prior to Treatment.
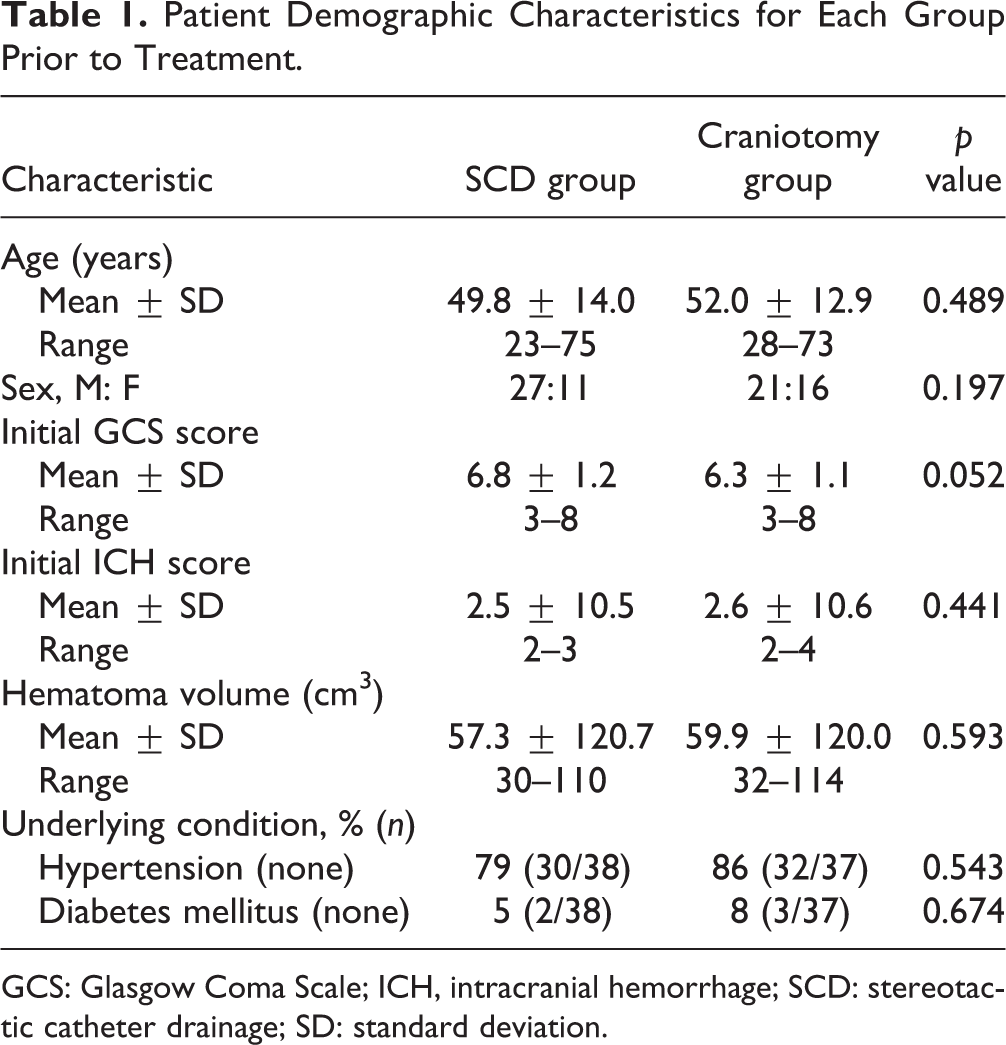
GCS: Glasgow Coma Scale; ICH, intracranial hemorrhage; SCD: stereotactic catheter drainage; SD: standard deviation.
Comparison of Intraoperative and Postoperative Efficacy
Table 2 shows the parameters of intraoperative efficacy in the SCD and craniotomy groups. The bleeding volume during the operation and the hematoma clearance rate were significantly lower in the SCD group than in the craniotomy group (p<0.001 for both). The SCD group also had a much shorter duration of surgery (p<0.001). The comparison of the postoperative efficacy between the two groups is shown in Table 3. The rates of pneumonia and tracheotomy in the SCD group were lower than those in the craniotomy group (p = 0.002 and p = 0.027, respectively), while complications of rebleeding and intracranial infection were not significantly different between the two groups (p = 0.113 and p = 0.308, respectively). The incidence of a second operation was indistinguishable between the groups (p = 0.973). The total hospitalization period was shorter for patients in the SCD group (p = 0.046), and the duration of NSICU stay was statistically longer for patients in the craniotomy group than those in the SCD group (p = 0.047).
Comparison of Operative Efficacy between the Treatment Groups.

Values expressed as mean ± standard deviation.
CI: confidence interval; SCD: stereotactic catheter drainage.
Comparison of Postoperative Efficacy between the Treatment Groups.

CI: confidence interval; NSICU: neurosurgery intensive care unit; SCD: stereotactic catheter drainage.
Comparison of Clinical Outcomes and Identification of Predisposing Factors for Good Clinical Outcome
The mRS score at discharge and the 12-month follow up were more favorable for patients in the SCD group than for those in the craniotomy group (Table 4, p=0.018 and p<0.001, respectively). Univariate analysis showed that the initial GCS score, hematoma volume, treatment modality, and the presence of hypertension affected the mRS score at the 12-month follow up (Table 5). Multivariate regression analysis showed that the predisposing factors for a good clinical outcome were hematoma volume (<50 cm3, 95% CI: 1.043–1.956, p=0.046), initial GCS score (>6, 95% CI: 3.248–187.466, p<0.001), hypertension (none, 95% CI: 1.440–2.922, p<0.001), and treatment modality (SCD, 95% CI: 1.422–3.226, p<0.001). Hypertensive intracerebral hemorrhage refers to hemorrhage caused by long-term hypertension and cerebral arteriosclerosis, which destroys the structure of small arteries and blood vessels in the brain 16 . Its predisposing site is also located in the basal ganglia, which is one of the most serious complications of hypertension 17 . We further analyzed patients with previous hypertension to eliminate the interference of confounding factors. Univariate analysis showed that the initial GCS score, hematoma volume, and treatment modality affected the mRS score at the 12-month follow up (Supplemental Table 1). Multivariate regression analysis showed that the predisposing factors for a good clinical outcome were hematoma volume (<50 cm3, 95% CI: 1.224–33.464, p<0.028), initial GCS score (>6, 95% CI: 0.018–0.550, p=0.008), and treatment modality (SCD, 95% CI: 1.588–29.683, p<0.01), which shared similar results with all the patients (Table 5). Furthermore, ICP was monitored after the operation, and it was observed that drainage of the hematoma can effectively reduce ICP (Table 6).
Comparison of Clinical Outcome between the Treatment Groups.

CI: confidence interval; mRS: modified Rankin Scale; OR: odds ratio; SCD: stereotactic catheter drainage.
Predisposing Factors for Good Clinical Outcome at the 12-Month Follow up.

CI: confidence interval; GCS: Glasgow Coma Scale; SCD: stereotactic catheter drainage.
Postoperative Intracranial Pressure Monitoring in SCD Group.

ICP: intracranial pressure; SCD: stereotactic catheter drainage.
Discussion
In the present study, we found that for patients with severe ICH (GCS score ≤ 8 and hematoma volume ≥ 30 cm3) with a hematoma volume less than 50 cm3, an initial GCS score > 6, and the absence of hypertension, experienced a good clinical outcome after SCD surgery. Among these patients, compared with conventional craniotomy, treatment with SCD appeared to have a beneficial effect on early recovery at discharge and functional outcomes at the 12-month follow up. Moreover, the total hospitalization period and NSICU stay were shorter in the SCD group, which could translate into reduced costs and improved NSICU turnaround time.
For patients with severe ICH, theoretically, conventional decompressive craniectomy may be beneficial because it can lower ICP, improve perfusion, and relieve perihematomal edema 18 . Among these physiological conditions, perihematomal edema is the main factor that causes high ICP and is also the therapeutic target of decompressive craniotomy 19 . Recent studies have shown that removing the hematoma via minimally invasive drainage could significantly alleviate perihematomal edema 20,21 . The main pathology of this edema is the reduction in glutamate accumulation in brain tissue and the decrease in the permeability of the blood–brain barrier 22 . The activation of the JNK signal pathway may be responsible for the underlying molecular mechanism of the pathology after cerebral hemorrhage, which causes an inflammatory response and promotes cell apoptosis, leading to brain edema and neurological dysfunction 23 . Minimally invasive removal of hematoma could inhibit the JNK pathway to reduce brain edema and protect nerve function 24 . Moreover, the application of a thrombolytic agent in the hematoma cavity after surgery would not exacerbate perihematomal edema and neurotoxicity 20,21 . In addition, craniotomy is risky because of the long operation time, increased amount of parenchymal injury, and procedure-related complications. SCD is one type of minimally invasive surgery in which both the scalp incision and skull drilling are less traumatic (Fig. 1), which may not lead to encephalocele induced by a skull defect; this can avoid trauma and unnecessary medical costs relating to secondary skull-repair surgery 25 . Consistent with previous reports, in our study, the duration of operation was shorter, the volume of intraoperative hemorrhage was lower, and the time under anesthesia was less pronounced in the SCD group 7 . For postoperative complications, the rates of pneumonia and tracheotomy were significantly lower in the SCD group than in the craniotomy group (Table 3). The reasons for this might possibly be that the duration of operation and anesthesia was shorter, which is less traumatic and avoids unnecessary brain damage, resulting in faster recovery of consciousness and less postoperative neurogenic pulmonary edema; and, compared to the craniotomy group, the SCD group had a much lower incidence of respirator-related pneumonia, resulting in better management of the respiratory tract.

CT scan images from patients with severe spontaneous intracerebral hemorrhage in basal ganglia.
No significant difference was observed in the rate of rebleeding despite the fact that hemostasis cannot be achieved under direct vision during SCD surgery. One possible reason may be that during craniotomy, the hematoma and bone flap were removed, leading to a rapid decrease in pressure in the hematoma cavity. The sharp fluctuation of high and low ICP at the hematoma site may potentially induce rebleeding in the ruptured vessels. After SCD surgery, the increased ICP was gradually but effectively reduced, as demonstrated in Table 6, which in turn permitted the maintenance of a specific pressure in the ruptured vessels; this slow reduction was attributed to the prevention of rebleeding events. Likewise, the rate of intracranial infection also did not achieve statistical significance. After SCD surgery, urokinase was injected into the hematoma cavity, and the drainage tube was retained for a few days, which may increase the risk of infection. However, no difference was observed between the two groups because of the reduction of unnecessary procedures relating to the drainage tube and strict sterility principles.
Previous studies showed that with minimally invasive surgery, less damage was caused to brain tissue, which increases the likelihood of neurologic function recovery 26,27 . Therefore, it was easy to explain better functional recovery in the SCD group than in the craniotomy group for patients at discharge and 12-month follow up (Table 4). A patient with a good initial GCS score (>6), hematoma volume < 50 cm3, and no hypertension may benefit from SCD in terms of good clinical outcomes (Table 5). Therefore, for patients with hypertension, strict hypertension control may improve the long-term prognosis after ICH. For patients in the acute phase, medication administration via intravenous micropump can be performed to control hypertension and maintain a stable blood pressure; after the condition is stabilized, oral medication can be administered for blood pressure control.
There are several limitations in our study. First, it is a retrospective study without randomization, and significant selection bias may potentially exist. It is possible that the best surgical candidates, or the patients with the best prognoses, were selected for SCD surgery. Therefore, patients would have had to be randomized with a matched control group to avoid this limitation. Second, the overall number of patients is too small to generalize our conclusions. In addition, this is a single-center experiment that may contain false-positive results. To overcome this limitation, large-scale trials, including multicenter experiments, are needed to show the benefit of SCD in patients with severe ICH. Third, the SCD procedure itself has some limitations. In patients with intracranial hypertension, the hematoma cannot be evacuated completely in one operation, and patients are more prone to experience brain herniation if the medication intervention fails to control hypertension 16,28 . In particular, for patients with active bleeding, SCD surgery cannot solve the problem radically, while precise hemostasis under direct vision can be achieved with craniotomy alone. Moreover, for patients with a small hematoma but severe cerebral edema or massive cerebral infarction, effective relief of intracranial hypertension cannot be achieved by SCD 20 . Therefore, flexible clinical application of SCD based on individual therapeutic approaches may identify the advantages of both SCD and craniotomy surgery, which is beneficial to the therapeutic response of patients with severe ICH and may improve their prognosis.
Conclusion
Our findings suggest that SCD surgery for patients with severe ICH (GCS score ≤ 8 and hematoma volume ≥ 30 cm3) was safe and efficacious. Compared with craniotomy, the SCD approach has several advantages, including minimal invasiveness, better recovery, fewer complications, shorter duration of hospitalization, and avoidance of trauma and medical costs relating to a second skull-repair surgery. These preliminary results warrant further study of large, prospective, randomized trials in the near future.
Supplemental Material
Supplemental_Table_1 - Stereotactic Catheter Drainage Versus Conventional Craniotomy for Severe Spontaneous Intracerebral Hemorrhage in the Basal Ganglia
Supplemental_Table_1 for Stereotactic Catheter Drainage Versus Conventional Craniotomy for Severe Spontaneous Intracerebral Hemorrhage in the Basal Ganglia by Jia Shi, Zhonghai Cai, Wei Han, Bo Dong, Yumin Mao, Jiachao Cao, Suinuan Wang and Wei Guan in Cell Transplantation
Footnotes
Authors' Note
Jia Shi, Zhonghai Cai, and Wei Han authors contributed equally to this work.
Ethical Approval
This study was approved by the Regional Ethics Committee of the Third Affiliated Hospital of Soochow University and all patients signed informed consents.
Statement of Human and Animal Rights
All patients involved in this study gave their informed consent. Institutional review board approval of our hospital was obtained for this study.
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.