
Abstract
It is important to investigate the clinical characteristics and identify the stroke mechanisms of patients with autoimmune disease-related stroke, which are necessary for early etiology diagnosis, accurate treatment and preventive strategies. In this article we retrospectively studied eight cases of acute ischemic stroke associated with autoimmune diseases, and without competing conventional stroke etiologies. The characteristics of stroke (clinical and radiological features), the laboratory tests especially serum D-dimer levels (as a marker of hypercoagulable state), and embolic signals on transcranial Doppler were evaluated for all eight patients. High-resolution magnetic resonance imaging (HRMRI), which can help to evaluate vasculitis was performed in four patients. The possible underlying mechanisms of these cases were discussed based on these manifestations. As a result, autoimmune diseases in our study included systemic lupus erythematosus (n=5), mixed connective tissue disease (n=1), central nervous system vasculitis (n=1), and Takayasu arteritis (n=1). All eight patients presented with acute infarction lesions in ≥2 vascular territories. Most patients presented with numerous small and medium infarction lesions located in the cortical and subcortical areas. Multiple stroke mechanisms were involved in these cases, including hypercoagulability (n=4), cardiac embolism (n=1) and vasculitis (n=3). Embolic signals could be detected on transcranial Doppler in all three stroke mechanisms. In conclusion, our study revealed the characteristics of autoimmune disease-related stroke. For patients with multiple acute cerebral infarcts within non-single arterial territories, autoimmune disease is an important etiology not to be neglected. Multiple stroke mechanisms were involved in these cases.
Introduction
It is usually difficult to identify the causes of stroke and up to one-quarter of patients with ischemic stroke have no probable cause found after standard workup 1,2 . Autoimmune disease is a rare cause of stroke. Several cases of ischemic stroke occurring in patients with autoimmune diseases have been reported. Patients with autoimmune disease such as rheumatoid arthritis and systemic lupus erythematosus (SLE) showed an excess risk of stroke over the general population. However, there are few systemic studies for evaluating autoimmune disease complicated with multiple acute ischemic stroke. It is important to investigate the clinical characteristics and identify the stroke mechanisms of these patients, which is necessary for early etiology diagnosis, accurate treatment and preventive strategies.
On the basis of existing experimental data, many laboratory and radiological examinations can help us to establish the mechanisms of stroke. The level of D-dimer has been used in many studies as a measure of hypercoagulability 3 . The detection of an embolic signal (ES) by transcranial Doppler (TCD) has been reported to have clinical significance, in that it clarifies cerebral embolism 4 . However, the clinical implications of ES have been evaluated mainly in conventional stroke patients 5 . There are few studies for evaluating ES in autoimmune disease complicated with stroke and the diagnosis of cerebral vasculitis by ES is difficult. High-resolution magnetic resonance imaging (HRMRI) is an emerging technique for characterizing intracranial arterial disease. It has been proven as an effective tool for identifying cerebral vasculitis 6 –8 .
Our aim was to investigate the clinical, laboratory and radiological features of patients with autoimmune disease complicated with multiple acute ischemic stroke, and explore the possible stroke mechanisms.
Materials and Methods
Patients
Our study was approved by the Institutional Ethics Committees of the China-Japan Friendship Hospital. We retrospectively studied acute ischemic stroke patients with autoimmune diseases treated at the China-Japan Friendship Hospital (Beijing, China) from July 2013 to March 2017. The following patients were excluded from the study: (1) those who had not suffered focal symptoms or relevant acute infarction lesions; (2) those who had not undergone TCD monitoring for ES; (3) those who had infarctions due to conventional stroke etiologies; and (4) those who had incomplete workups for stroke etiology (either vascular or cardiologic studies). Finally, eight patients were finally included in this study.
Data Acquisition and Clinical Management
For all patients, the type of autoimmune disease, years from diagnosis of autoimmune disease to stroke, age, sex, and conventional stroke risk factors including hypertension, diabetes mellitus, hyperlipidemia, atrial fibrillation, ischemic heart disease, and tobacco consumption were collected. D-Dimer and erythrocyte sedimentation rate (ESR) levels were assessed at the time of hospitalization. All patients underwent extra- and intracranial Doppler and duplex sonography of cerebral arteries, computed tomography angiogram (CTA) or magnetic resonance angiogram (MRA), 24 h of electrocardiographic monitoring, transthoracic or transesophageal echocardiography (TEE). Stroke mechanisms were then identified by two experienced doctors.
Brain MRI Assessment and Analysis
Brain MRI examinations were performed in a 3 T scanner (Ingenia; Philips Healthcare, Best, The Netherlands) with a 15-channel phased-array head coil. The brain MRI scanning protocol included diffusion-weighted imaging (DWI), T1- and T2-weighted images, and T2-weighted fluid-attenuated inversion recovery (T2flair). The sizes and locations of all acute infarction lesions were noted. Lesions were considered ‘small’ when the largest axial diameter was <10 mm, ‘medium’ if 10–30 mm, and ‘large’ if >30 mm. Involved territories were arbitrarily assigned as (1) anterior/posterior circulation, or (2) unilateral/bilateral lesions 9 . Brain MRI was performed in seven patients. Comparison of two brain CT scans revealed new-onset infarction lesions in another one patient.
HRMRI was performed in three patients. Three-dimensional volumetric isotropic turbo spin echo acquisition (ACQ) images were obtained with the following parameters: repetition time/echo time = 1300 ms/36 ms, FOV = 140 × 200 × 135 mm3, matrix = 280 × 332 × 270, NSA = 2. ACQ voxel volume was 0.5 × 0.6 × 0.5 mm3. Reconstruction (REC) voxel volume was 0.5 × 0.5 × 0.5 mm3. The short axial cross-sections were constructed automatically with a 0.5-mm slice thickness.
TCD Monitoring Methods
TCD was used to monitor bilateral middle cerebral arteries (MCAs) using two 2 MHz probes with insonation depths of 40 to 60 mm for 30 minutes. All ESs were manually saved to a computer for review. ESs were identified by experienced doctors according to international standards 10 (the author Li-Li Sun successfully passed the theoretical and practical examination in Neurosonology held by the Neurosonology Research Group of the World Federation of Neurology [WFN]).
Results
Clinical Characteristics and Laboratory Examinations
A total of eight patients were included in this study. Clinical characteristics and laboratory examinations are showed in Table 1. The median age was 40.5 years (30–58 years) and 87.5% were female. Autoimmune diseases in our study included SLE (n=5), mixed connective tissue disease (MCTD; n=1), central nervous system vasculitis (n=1), and Takayasu arteritis (n=1). The time from the diagnosis of the autoimmune disease to a stroke was 0–9 years; five of the eight patients presented stroke as the first manifestation of their autoimmune disease. All eight patients had neurological symptoms, including muscle weakness (n=3), dysarthria (n=1), facial numbness (n=2), paresthesia of limbs (n=2), somnolence (n=1), and a mental and behavior disorder (n=1). Overall, six of eight patients tested (75.0%) had elevated D-dimer values (0.56 to 5.62 mg/L; reference level ≤ 0.5 mg/L). Only two patients had hypertension, but with no atherosclerosis vasculopathy.
Clinical characteristics and laboratory examinations.
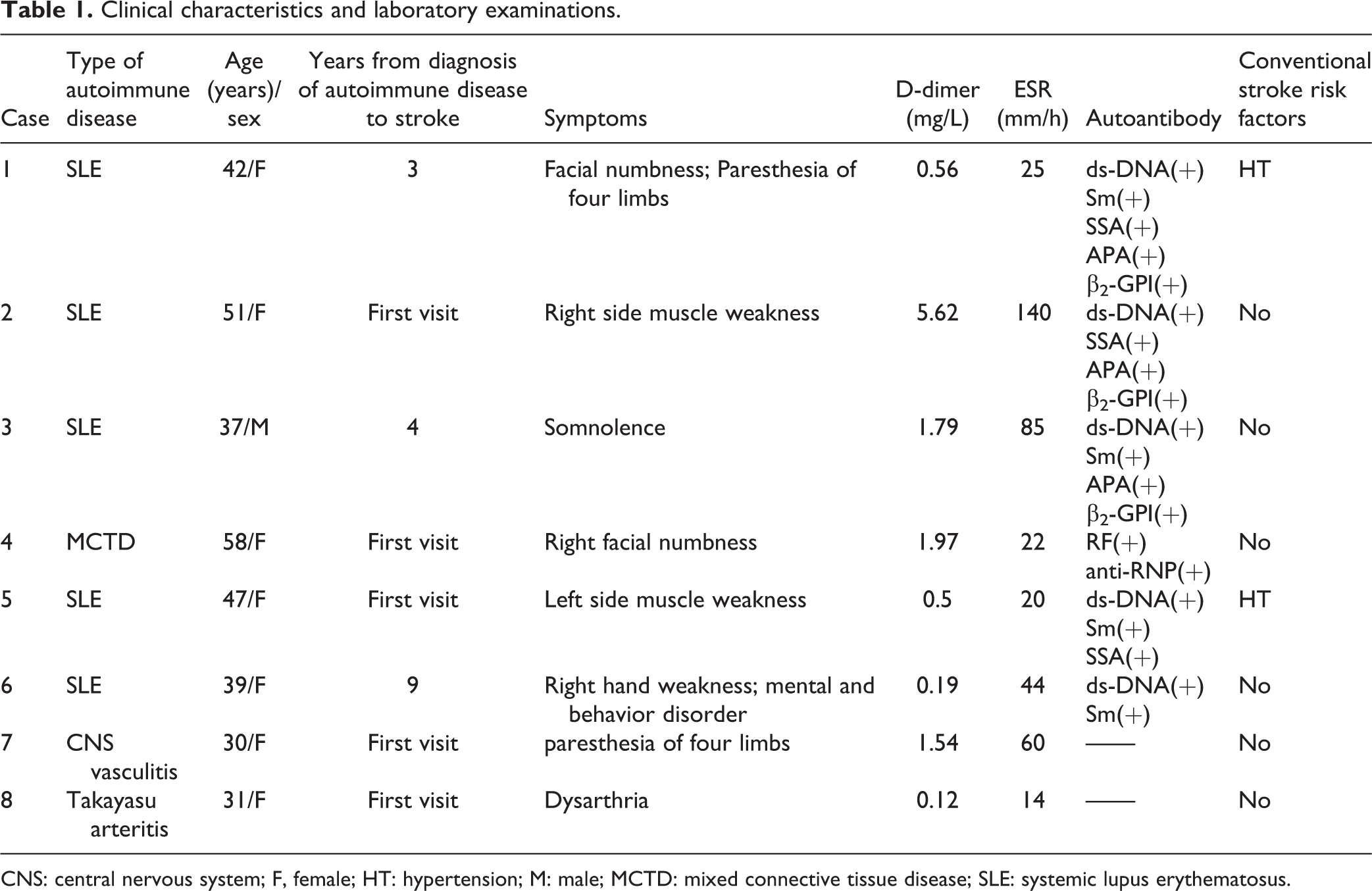
CNS: central nervous system; F, female; HT: hypertension; M: male; MCTD: mixed connective tissue disease; SLE: systemic lupus erythematosus.
Radiological Characteristics, ESs and Stroke Mechanisms
According to the MRI, CTA, and TCD, the stroke mechanisms in these eight cases were identified into hypercoagulability (n=4), cardiac embolism (n=1) and vasculitis (n=3).
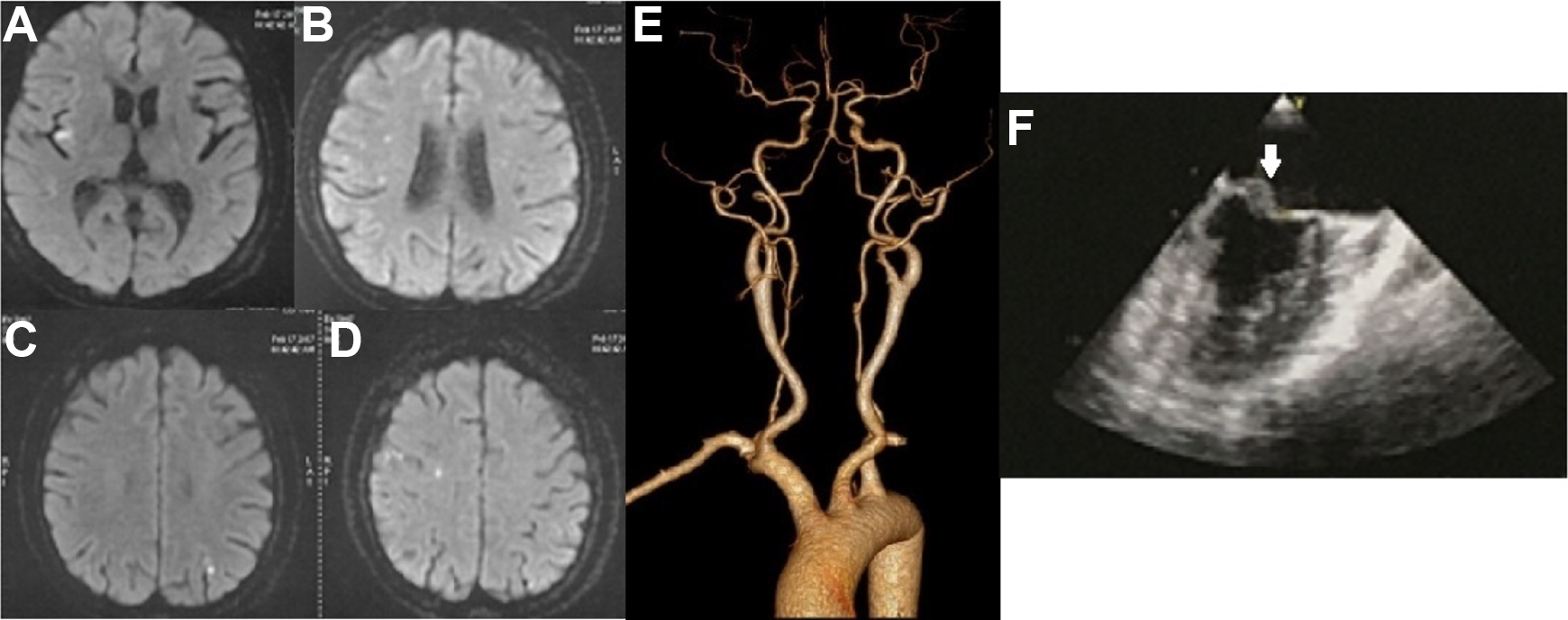
The radiological characteristics of the eight cases are depicted in Table 2. All these eight patients presented acute infarction lesions in ≥2 vascular territories and numerous small or medium infarction lesions located in the cortical and subcortical areas. The infarction lesions were located in the bihemispheric territories (n=5), or bihemispheric territories and posterior circulation (n=3). MRA and/or CTA were also normal in the other four patients (Cases 1–4), and combined with the elevation of D-dimer, the stroke mechanism was considered as hypercoagulability (Fig 1). In one patient (Case 5), the stroke mechanism was attributed to a cardiac embolism because of cardiac valvular vegetations on TEE, and normal D-dimer levels and normal arterial examinations (Fig 2). There were three patients (Cases 6–8) that showed bilateral anterior circulation vasculopathy on CTA and/or MRA which were regarded as vasculitis. HRMRI in one of the three patients showed circumferential vessel wall thickening and enhancement of bilateral MCAs (Fig 3).
Radiological characteristics and embolic signal characteristics.

ACA: anterior cerebral artery; CCA: common carotid artery; ICA: internal carotid artery; LMCA: left MCA; MCA: middle cerebral artery; ND: not done; RMCA: right MCA; UCG: ultrasonic cardiogram.

Patients with the hypercoagulability stroke mechanism (Patients1–4). Patient 1. 42/F/SLE. (A, B) Diffusion-weighted images showed multiple acute infarcts in the bilateral cerebral hemispheres and pons; (C) MR angiography showed normal cerebral arteries; (D) White arrows showed ESs in the LMCA and RMCA. Patient 2. 51/F/SLE. (E, F) Brain CT showed multiple infarcts in bilateral cerebral hemispheres; (G) CT angiography showed normal cerebral arteries; (H) White arrows showed ESs in the LMCA and RMCA. Patient 3. 37/M/SLE. (I, J, K, L) Diffusion-weighted images showed multiple acute infarcts in the bilateral cerebral hemispheres and pons; (M) MR angiography showed normal cerebral arteries; (N) HRMRI (sagittal view) showed normal MCA without circumferential vessel wall thickening or enhancement (white arrow). Patient 4. 58/F/MCTD. (O, P, Q, R) Diffusion-weighted images showed multiple acute infarcts in the bilateral cerebral hemispheres and left cerebellum; (S) CT angiography showed normal cerebral arteries; (T) HRMRI (sagittal view) showed normal MCA without circumferential vessel wall thickening or enhancement (white arrow).
Patient 5, with a cardiac embolism stroke mechanism. Patient 5. 47/F/SLE. (A, B, C, D) Diffusion-weighted images showed multiple acute infarcts in the bilateral cerebral hemispheres; (E) CT angiography showed normal cerebral arteries; (F) White arrow showed mitral valve vegetation on echocardiography.

Patients with a vasculitis stroke mechanism (Patients 6–8). Patient 6. 39/F/SLE. (A, B, C) Diffusion-weighted images showed multiple acute infarcts in the bilateral cerebral hemispheres; (D) CT angiography showed occlusion of the bilateral ICAs, bilateral MCAs, and left ACA. Patient 7. 30/F/CNS vasculitis. (E, F) Diffusion-weighted images showed multiple acute infarcts in the bilateral cerebral hemispheres; (G) MR angiography showed stenosis of the siphon segment of the left ICA, and bilateral MCAs; (H) HRMRI (sagittal view) showed circumferential vessel wall thickening and enhancement of MCA (white arrow). Patient 8. 31/F/Takayasu arteritis. (I, J) Diffusion-weighted images showed multiple acute infarcts in the bilateral cerebral hemispheres; (K, L) CT angiography showed circumferential vessel wall thickening of bilateral CCAs.
ESs were observed in six (75.0%) patients with various mechanisms (Table 2). The time from stroke to TCD monitoring of these patients was 2–28 days. The time from stroke to TCD monitoring of another two patients without ES was 30 days.
Discussion
Autoimmune disease is an important etiology for stroke 11,12 , especially for young female patients. In our study, five patients even presented with stroke as the first manifestation. The types of autoimmune diseases in our study included SLE, MCTD, central nervous system vasculitis, and Takayasu arteritis. In addition, cerebral infarction occurred in patients with other autoimmune diseases, such as Churg–Strauss syndrome and rheumatoid arthritis 13 –16 .
The patients included in our study mostly presented multiple, disseminated small and medium infarction lesions involving multiple arterial territories, located in the cortical and subcortical areas. This is in line with the TCD monitoring results, showing a high prevalence of ESs detected in bilateral MCAs. Infarction lesions involving multiple vascular supply territories were mostly attributed to atrial fibrillation, hematological diseases, or cancer 17 . However, autoimmune disease receives little attention. What is more, in our study, we found that large lesions were less common in autoimmune disease-related stroke than cancer-related stroke or atrial fibrillation-related stroke 9,18,19 . Only one patient (Case 6) with mechanism vasculitis had large infarction lesions in the basal ganglion. Since hypercoagulability was not the unique mechanism, the number of infarction lesions was not significantly correlated with D-dimer levels.
We found that the stroke mechanisms in our study included hypercoagulability, cardiac embolism and vasculitis. The level of D-dimer, which is a direct laboratory measure of activated coagulation, has been used in many previous studies as a measure of hypercoagulability 3 . D-dimer is the smallest fibrinolysis-specific degradation product found in the circulation. The D-dimer is very sensitive to intravascular thrombus and may be markedly elevated in disseminated intravascular coagulation 20 . In four patients (Cases 1–4), stroke mechanisms were attributed to hypercoagulability with elevated D-dimer levels and normal arterial, cardiac examinations. Recent studies have revealed that inflammation may change the hemostatic balance in a thrombogenic direction. The immune system and coagulations system are linked, with many molecular components being important for both systems 21,22 . Antiphospholipid syndrome is an important cause of hypercoagulability. In our study, three patients with antiphospholipid syndrome all presented multiple, disseminated small and medium infarction lesions involved multiple arterial territories.
In Case 5, the stroke mechanism was attributed to a cardiac embolism identified by cardiac valvular vegetations displayed on TEE (Fig 2), and with normal D-dimer levels and normal arterial examinations. Cardiac valvular disease of this patient presented as non-bacterial thrombotic endocarditis (NBTE), a rare condition characterized by non-infective inflammatory and/or thrombotic vegetations on the heart valve leaflets. NBTE can be seen in autoimmune diseases such as SLE, antiphospholipid syndrome, and rheumatoid arthritis 23,24 . Previous studies showed that NBTE in SLE was associated with a higher risk for embolic stroke and suggested that NBTE might be a source of cerebral emboli 24,25 .
In another three patients, the stroke mechanism was attributed to vasculitis. Case 8 was diagnosed as Takayasu arteritis. Carotid ultrasound of this patient revealed circumferential vessel wall thickening of the bilateral common carotid arteries (CCAs). Another two patients presented with Moyamoya syndromes on CTA. It has been reported that large-vessel stroke due to Moyamoya syndrome presented as a rare manifestation of SLE 26,27 . Cerebral vasculitis in the setting of lupus may lead to large cerebral vessel occlusions and lead to Moyamoya syndrome. HRMRI of
Case 7 showed circumferential vessel wall thickening and enhancement of bilateral anterior circulations, which confirmed the diagnosis of central nervous system vasculitis (Fig 3). Recent studies have proven HRMRI as an effective tool for identifying cerebral vasculitis 28 .
Since ES has clinical significance, in that it clarifies cerebral embolism, ES can help to distinguish cerebral infarction from other complications of autoimmune diseases. ESs were detected in 5.7% of unselected stroke patients and in almost 50% of cancer-related stroke patients in the previous studies 4,29 . However, the frequency and the number of ESs detected in autoimmune disease-related stroke in our study are much higher. The time from stroke to TCD monitoring of ES-positive patients was 2–28 days, while ES was seldom positive after 1 week in conventional stroke patients. More interestingly, we found that ES was detected not only in hypercoagulability and cardiac embolism patients, but also in vasculitis patients.
Conclusion
Autoimmune disease is an important etiology and should not be neglected for stroke, especially in young patients in the absence of conventional stroke risk factors. Our study revealed the characteristics of autoimmune disease-related stroke, which were distinct from those of conventional stroke. These patients mostly presented multiple, disseminated small and medium infarction lesions involving multiple arterial territories, located in the cortical and subcortical areas. We found that multiple stroke mechanisms were involved in these patients, including hypercoagulability, cardiac embolism and vasculitis. For these patients, we suggest complete workups for the identification of stroke etiology, which is necessary for further accurate treatment and preventive strategies.
Limitations
First, the number of cases enrolled in our study was limited, but the examination data of these eight cases were comprehensive. TCD microembolic monitoring and HRMRI were done in our study, which were not included in the other studies. More patients will be enrolled in our further study. Second, we will further explore the unique treatment and prognosis evaluation strategies of patients with autoimmune diseases compared with traditional cerebral infarction patients. In our study, corticosteroid and immunosuppression, together with antiplatelet and statin therapy were effective for these patients, and most patients recovered more quickly than traditional cerebral infarction patients.
Supplemental Material
Supplemental_Figures - Clinical Manifestations and Mechanisms of Autoimmune Disease-Related Multiple Cerebral Infarcts
Supplemental_Figures for Clinical Manifestations and Mechanisms of Autoimmune Disease-Related Multiple Cerebral Infarcts by Li-Li Sun, Wen-Xiong Tang, Min Tian, Lu Zhang and Zun-Jing Liu in Cell Transplantation
Footnotes
Ethical Approval
This study was approved by the Institutional Ethics Committees of China-Japan Friendship Hospital, Beijing, China (No. 2017-65).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Institutional Ethics Committees of the China-Japan Friendship Hospital, Beijing, China (No. 2017-65) and their approved protocols.
Statement of Informed Consent
Verbal informed consent was obtained from the patients for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant support or other sources of funding: supported by National Natural Science Foundation of China (No. 31771045) and the China-Japan Friendship Hospital Youth Science and Technology Project (No. 2015-2-QN-36).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.