
Abstract
Mechanical thrombectomy (MT) is effective in managing patients with acute ischemic stroke (AIS) caused by large-vessel occlusions and allows for valuable histological analysis of thrombi. However, whether bridging therapy (pretreatment with intravenous thrombolysis before MT) provides additional benefits in patients with middle cerebral artery (MCA) occlusion remains unclear. Therefore, this study aimed to compare the effects of direct MT and bridging therapy, and to elucidate the correlation between thrombus composition and stroke subtypes. Seventy-three patients with acute ischemic stroke who received MT, were eligible for intravenous thrombolysis, and had MCA occlusion were included. We matched 21 direct MT patients with 21 bridging therapy patients using propensity score matching and compared their 3rd-month clinical outcomes. All MCA thrombi (n = 45) were histologically analyzed, and the red blood cell (RBC) and fibrin percentages were quantified. We compared the clot composition according to stroke etiology (large-artery atherosclerosis and cardioembolism) and intravenous thrombolysis application. The baseline characteristics showed no difference between groups except for a higher atrial fibrillation rate and NIHSS score on admission in the direct MT group. We performed a supportive analysis using propensity score matching but could not find any differences in the functional outcome, mortality, and intracerebral hemorrhage. In the histological clot analysis, the cardioembolic clots without intravenous thrombolysis pretreatment had higher RBC (P = 0.042) and lower fibrin (P = 0.042) percentages than the large-artery atherosclerosis thrombi. Similar findings were observed in the thrombi treated with recombinant tissue plasminogen activator (P = 0.012). In conclusion, there was no difference in the functional outcomes between the direct MT and bridging therapy groups. However, randomized trials are needed to elucidate the high ratio of cardioembolism subtype in our group of patients. The histological MCA thrombus composition differed between cardioembolism and large-artery atherosclerosis, and this finding provides valuable information on the underlying pathogenesis and thrombus origin.
Introduction
Five previously reported randomized clinical trials demonstrated the efficacy and safety of direct mechanical thrombectomy (MT) in patients with acute ischemic stroke (AIS) caused by large-artery occlusions 1 –5 . Intravenous thrombolysis (IVT) with recombinant tissue plasminogen activator (rt-PA) administered within 4.5 hours of an AIS has been the standard treatment. However, patients with stroke due to a large-artery occlusion respond poorly to intravenous rt-PA alone 6 –8 . Therefore, the debates regarding whether intravenous rt-PA before MT is necessary are ongoing. Moreover, some patients underwent direct mechanical thrombectomy mainly for contraindications to IVT and other patients for a suspicion of large thrombi, borderline coagulation status, time window close to 4.5 hours, etc. Therefore, comparing the characteristics of these patients with those of bridging therapy patients is not optimal 9 . Several previously reported studies did not support the idea that IVT before MT in patients with large-artery occlusions could provide an additional clinical benefit compared with MT alone 2,10 . However, the occlusion sites in those studies included both the middle cerebral artery (MCA) and internal carotid artery (ICA), suggesting different stroke subtypes and responses to IVT. In Asians, the incidence of MCA occlusion is significantly higher than that of ICA occlusion. Therefore, separating patients with MCA occlusion from those with ICA occlusion to avoid between-group variance may be necessary.
The application of MT allows for a histological analysis of the clots retrieved from the intracranial arteries. Recent studies suggested that a histological examination of retrieved clots can offer new insights into the pathogenesis of acute strokes that are caused by intracranial large-artery occlusion 11–12 . However, few studies have actually analyzed the thrombus compositions, which were naturally affected by rt-PA, between the patients who underwent bridging therapy and direct MT. Furthermore, data on the correlation between clot composition and stroke subtypes in patients with MCA occlusion are still limited.
Therefore, the aim of our study was to evaluate whether the functional outcomes of bridging therapy and direct MT are similar in IVT-eligible patients with MCA occlusion, and to further examine thrombus composition and its relationship with stroke subtypes.
Materials and Methods
Patients
A total of 73 consecutive patients with AIS and MCA occlusion were enrolled from December 2015 to January 2018. Patients had their MT performed using the Solitaire AB stent retriever (Covidien, Irvine, CA, USA). Patients were excluded if they were treated with IVT only, had contraindications for IVT and missed key outcome data, or had follow-up loss at 3 months. The patients’ baseline characteristics (i.e., demographic data, vascular risk factors, and National Institute of Health Stroke Scale (NIHSS) score on admission), use of IVT, time to endovascular treatment, time to reperfusion, revascularization status, stroke subtypes, and functional outcomes were recorded. Successful reperfusion was defined as a thrombolysis in cerebral infarction score of 2b-3, and a good functional outcome was defined as a modified Rankin Score (mRS) of 0–2 at 3 months. Stroke subtypes were determined in accordance with the Trial of ORG 10172 in Acute Stroke Treatment classification 13 using the following methods: computed tomography or magnetic resonance imaging, digital subtraction angiography, duplex ultrasound, 24-hour electrocardiography, and transthoracic or transesophageal echocardiography. The institutional ethics committee approved this study. Patients were excluded if they did not have thrombus material suitable for the histological analysis. As a result, a total of 45 patients underwent a histological thrombus analysis in this study.
Interventional Thrombectomy
The Solitaire AB retrievable stent (Covidien) was deployed at the site of the MCA occlusion and then removed under negative-pressure aspiration as previously recommended 3 .
Histological Analysis
Formalin-fixed, paraffin-embedded (FFPE) thrombi were obtained from the patients after the MT. All FFPE thrombi were cut to a 4 μm section thickness and stained with hematoxylin-eosin 14 . The stained slides were photographed at 200× magnification using the Leica DM500 microscope and digital camera (Leica, Wetzlar, Germany). The percentages of red blood cells (RBCs) and fibrin were semi-quantitatively analyzed using the ImageJ software (National Institutes of Health, Bethesda, MD, USA). Quantification of fibrin and RBC was performed manually. The pictures were converted to grayscale (8-bit), the threshold was set, and the particles were analyzed automatically (areas covered by the respective cells[%] were measured). Categorization and analysis were performed by an experienced pathologist (L.F.) blinded to the clinical data and imaging findings.
Statistical Analysis
We first compared the baseline characteristics, treatment data, and functional outcomes of 31 patients in the direct MT group with 42 patients in the bridging therapy group using Fisher’s exact test (categorical variables) and the Wilcoxon signed-rank test (continuous variables). Furthermore, we performed a 1:1 propensity score-matching analysis based on a multiple logistic regression model that accounted for additional explanatory variables. Thereafter, the percentage of each clot component that was regarded as a continuous variable was compared between the patients with cardioembolism and those with large-artery atherosclerosis. All statistical analyses were performed using the SPSS software (Version 23.0; IBM, Armonk, NY, USA). P-values of <0.05 were considered statistically significant.
Results
The baseline characteristics of the 31 patients in the direct MT group and 42 patients in the bridging therapy group are shown in Table 1. Univariate analysis showed no significant differences in the baseline characteristics between both groups, except for the higher rate of atrial fibrillation in the direct MT group compared with the bridging therapy group (87.1% vs. 47.6%, respectively; P = 0.001) and a higher NIHSS score on admission in the direct MT group compared with the bridging therapy group (15 vs. 13, respectively; P = 0.037). The laboratory findings, treatment data, time from symptom onset to endovascular treatment, time from symptom onset to vascular recanalization, and successful reperfusion rate showed no significant differences between the groups. The clinical outcomes at 3 months (Sup.1), intracerebral hemorrhage (ICH) rate, and mortality rate were not significantly different between the groups.
Univariate Comparison of Bridging Thrombolysis with Direct MT in Patients with MCA Occlusions.
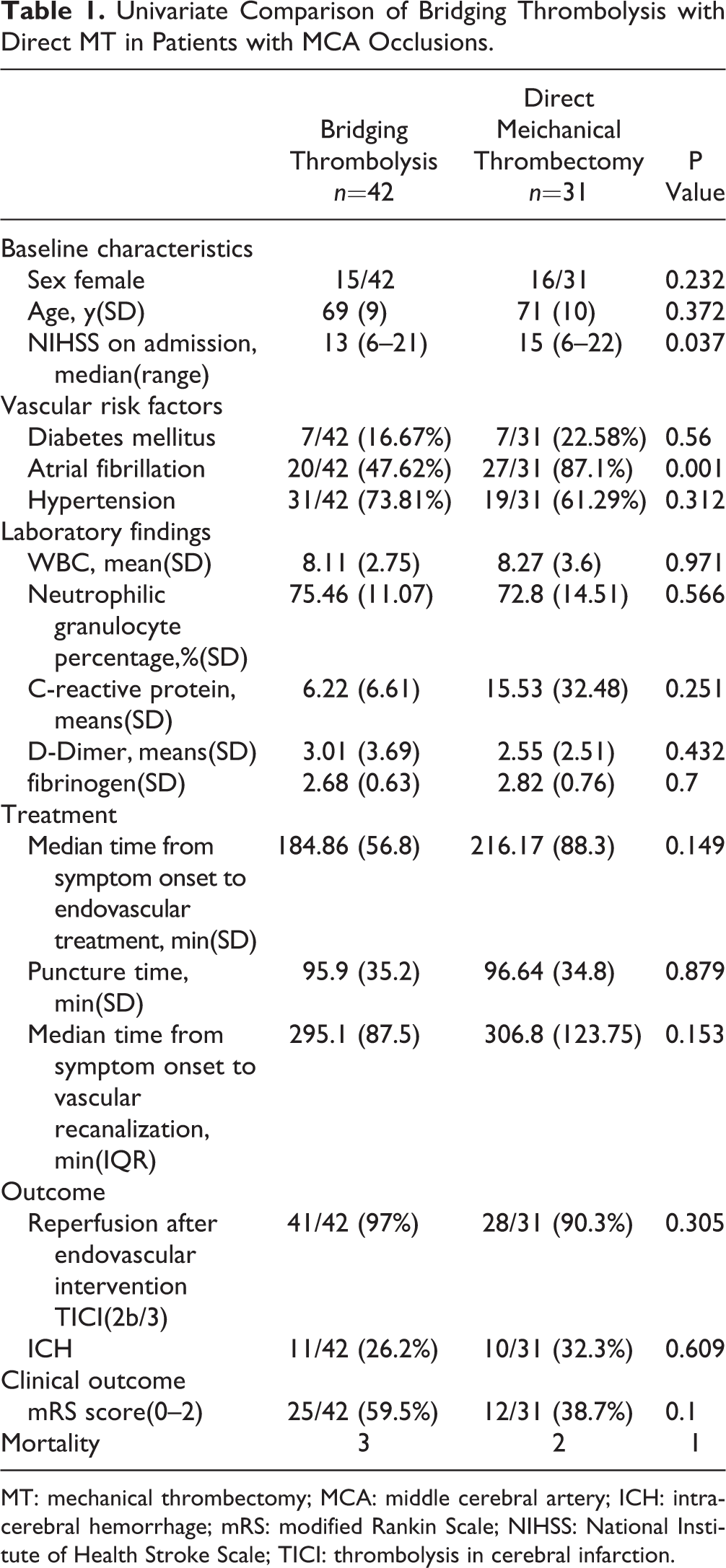
MT: mechanical thrombectomy; MCA: middle cerebral artery; ICH: intracerebral hemorrhage; mRS: modified Rankin Scale; NIHSS: National Institute of Health Stroke Scale; TICI: thrombolysis in cerebral infarction.
A total of 21 patients in the direct MT group were eligible for the propensity score-matching (1:1) analysis, and the baseline covariates, such as age, NIHSS score, sex, vascular risk factors, and laboratory parameters were equally distributed in the two groups as shown in Table 2. We observed no difference in the major outcomes between the groups: functional independence measured using the mRS score (0–2) after 3 months (bridging therapy 52.4% vs. direct MT 42.8%; P=0.758), ICH rate (bridging therapy 47.6% vs. direct MT 33.3%; P=0.53), and mortality rate (bridging therapy 1% vs. direct MT 0.5%; P=1.0).
Comparison of Bridging Thrombolysis With Direct MT in Patients with MCA Occlusion Using Multivariate Matching.

MT: mechanical thrombectomy; MCA: middle cerebral artery; ICH: intracerebral hemorrhage; mRS: modified Rankin Scale; NIHSS: National Institute of Health Stroke Scale; TICI: thrombolysis in cerebral infarction.
Of the 45 thrombus materials collected from the MCA, 36 (80%) clots were classified as a cardioembolism and nine (20%) as a large-artery atherosclerosis. The mean percentage of RBCs and fibrin across all retrieved clots in the histological analysis was 69% and 31%, respectively. The percentages of the RBC and fibrin compositions differed significantly between the patients with cardioembolism and those with large-artery atherosclerosis (Fig. 1). The clots from the patients in the direct MT group with cardioembolism had a higher percentage of RBCs (69% vs. 55.5%, P=0.012) and a lower percentage of fibrin (31% vs. 44.5%, P=0.012) than those with large-artery atherosclerosis. The group with rt-PA pretreatment showed similar results (P=0.042).

Difference in the mean percentages of the RBC and fibrin compositions in the stroke subtypes of cardioembolism and large-artery atherosclerosis. Fibrin (A), RBC (B) composition in bridging thrombolysis group, and fibrin (C), RBC (D) composition in direct mechanical thrombectomy group. RBC indicates red blood cell; LAA, large-artery atherosclerosis; CE, cardioembolism.
Discussion
In this single-center observational study, we examined whether the treatment of patients with AIS due to MCA occlusion with intravenous rt-PA before MT yielded better outcomes or added any risks. With the exclusion of IVT-ineligible patients, our matched analysis reveals that there are no significant differences in the functional outcomes, mortality rate, and recanalization rate between bridging therapy and direct MT in patients with MCA occlusion. Given the poor response to intravenous rt-PA alone in patients suspected of having a large thrombus burden or the increased hemorrhage rate after IVT in subjects with atrial fibrillation, the experienced team in our stroke center would sometimes decide to perform a direct MT after their full assessment. Therefore, our univariate analysis showed a higher rate of atrial fibrillation and higher NIHSS scores on admission in the direct MT group. However, after propensity-score matching, the observed decrease in the difference of functional outcomes between the two groups further proved the univariate analysis findings.
Several previous clinical observations that compared direct MT with bridging therapy suggested that bridging therapy could provide benefits for the endovascular procedure and increase the recanalization rates 15 –17 . Moreover, another meta-analysis concluded that bridging therapy is superior to direct MT 18 . In contrast, these findings are not supported by the subgroup analysis findings of the SWIFT and STAR studies, and of a previous meta-analysis of five randomized controlled trials (HERMES) 10,19 . Considering that inclusion of IVT-ineligible patients was an inherent bias, several additional matched-pair analyses indicated that there was no difference in the outcomes of IVT-eligible patients who underwent either MT alone or bridging therapy 20 –22 . However, a lower mortality rate was observed in patients with ICA occlusion who were treated with direct MT 9 .
The major limitation of these studies was the inclusion of patients with MCA and ICA occlusions. MCA occlusions are more commonly found in Asian populations and mainly originate from atherosclerosis or stenosis in situ, suggesting inherent differences from ICA occlusions. Patients with ICA occlusion that is treated with IVT alone have a lower recanalization rate (4.4–8%) than patients with MCA occlusion (30.8–32.3%) 6,23 . Therefore, the difference in the outcomes may be influenced by these confounders in the baseline characteristics. In our study, the enrolled patients were eligible for IVT and had MCA occlusion. We observed no difference in the functional outcomes and mortality rates in the patients receiving different treatments. The suggestion that pretreatment with IVT results in superior outcomes in patients with MCA occlusion undergoing MT remains unsubstantiated. Even if pretreatment with thrombolysis could result in a higher rate of recanalization 24 , we found no difference in these rates (both groups as high as 90%). One potential explanation could be the efficient recanalization by MT, which might influence the functional outcomes. Moreover, with the accompanying atrial fibrillation (19/21) in the propensity score-matched group with MCA occlusion, another explanation could be the poor response of the cardioembolic thrombi to IVT alone.
Our study demonstrates that the histological compositions of the clots from the patients with MCA occlusion differ between the two major causes of ischemic stroke (i.e., large-artery atherosclerosis and cardioembolism). Moreover, we found that the difference in histological composition existed in both the patients treated with bridging therapy and those treated with direct MT. Our data from the MCA thrombi show that the percentage of RBCs was higher in the patients with cardioembolism than in those with large-artery atherosclerosis (Fig. 2). Conversely, the percentage of fibrin was higher in the patients with large-artery atherosclerosis than in those with cardioembolism. Although several previous studies have reported that the composition of retrieved clots was correlated with the stroke mechanism 11–12,25 –27 , the results are inconsistent or contradicting. In contrast to our results, a previously reported histopathological analysis of retrieved clots indicated that clot composition was unrelated to any stroke etiology 25 , but detailed data were not provided in that analysis. Furthermore, the majority of the population in that study included Caucasian subjects (82%) and only a small proportion of Asian subjects (6%). Another study that investigated 22 thrombi found that clots originating from large-artery atherosclerosis had a higher percentage of RBCs than clots originating from other stroke subtypes. Moreover, the number of patients with large-artery atherosclerosis (n=8) and cardioembolism (n=6) in that study was too small to draw a conclusion, and this was a major limitation that could be related to the contradictory finding 26 . One of the most recent previous studies suggested an association of high fibrin and low RBC percentages with cardioembolic thrombi 12 and was contrary to the findings of a postmortem study on red cardioembolic thrombi 28 . Conversely, the rates in patients with cardioembolism treated with IVT are significantly higher than the rates in patients with large-artery atherosclerosis. Considering the probable bias by rt-PA application, these findings should be interpreted with caution 12 . The findings of Kim et al. that showed a higher percentage of RBCs in thrombi arising from cardioembolism were in accordance with our results 11 . One potential explanation could be that the enrolled candidates with MCA occlusion were mostly Asian in that study, similar to our study’s population.
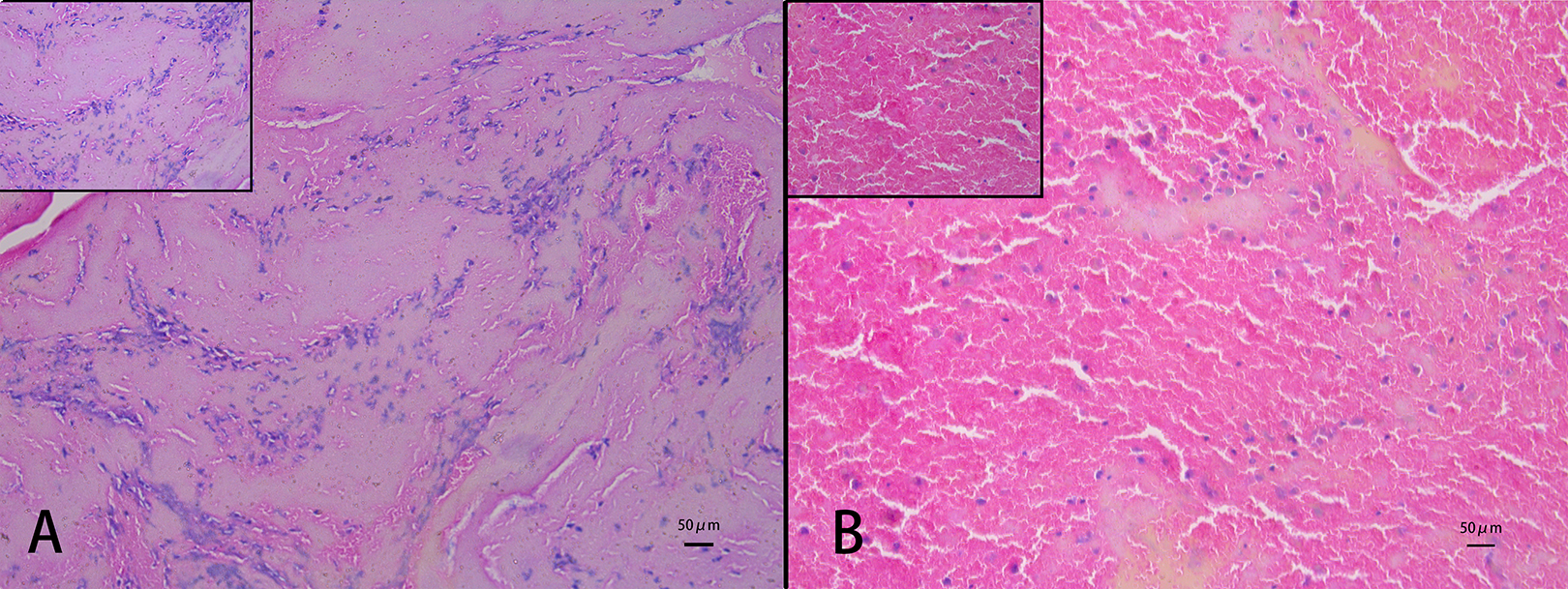
Microscopic view of retrieved thrombi from middle cerebral artery. (A) indicates most thrombi consist of fibrin (white thrombi) in a hematoxylin-eosin stained section (200× magnification); (B) RBC (red thrombi). Scale bar: 50 μm. Inserts show higher magnification (400×) of representative staining.
The considerable limitation of all these studies was the inclusion of patients with and without rt-PA application. The clot composition with IVT is inherently different from that without IVT, and this is likely to be the cause of the major differences in their findings. To determine whether thrombolysis could have any additional effects on thrombus composition, our study compared the clot composition according to the presence or absence of rt-PA application. Although we still found similar associations of red thrombi arising from cardioembolism with IVT application prior to MT, no previous study has stratified this bias. Thus, even if the clot composition may have been affected by the use of intravenous rt-PA, the thrombus composition could still provide information on the subtypes of stroke.
Limitations and Strengths
Our study has several limitations. This study is a single-center, observational design with a natural bias. Considering the small size of the population, it is difficult to draw a strong conclusion that there is no significant difference in mRS score by univariate analysis between the two groups: 59.5% in bridging therapy and 38.7% in direct MT. Therefore, this difference may need to be examined using a large-scale group in future studies. Furthermore, the main reasons not to perform IVT on eligible patients before thrombectomy were the suspicion of a large thrombus burden and major vessel occlusions. This decision took into consideration the poor recanalization and increased hemorrhage rates after intravenous rt-PA in these patients. However, given the retrospective nature of our research, the exact reason to decide against IVT cannot be provided for every single patient. Recently, the updated guidelines suggested that eligible patients with AIS should receive intravenous rt-PA even if MT is being considered. Therefore, this new suggestion should be considered in clinical practice and in further studies. The components of the retrieved thrombi might not completely reflect those of the entire thrombus and, although this bias was unavoidable, it should be considered. The strengths of our study include the exclusion of the imbalance in the clinical characteristics of the patients according to IVT ineligibility and the homogeneous histological analysis in the patients with only MCA occlusion with or without rt-PA application.
Conclusion
This study supports the hypothesis that direct MT is non-inferior to bridging therapy, especially in the cardioembolic stroke subtype of patients with MCA occlusion. However, the evidence should be carefully considered due to the small number of patients in this study and should be established by further randomized controlled trials. Our histologic findings that show the proportion of RBC composition in retrieved clots is higher in patients with cardioembolism lend support to those of previous studies. Moreover, this composition characteristic was found in the presence and absence of rt-PA application. Our findings would have references for clinical choice and study design in the future.
Supplemental Material
Supplemental Material, Sup_1._mRS - Bridging Therapy Versus Direct Mechanical Thrombectomy in Patients with Acute Ischemic Stroke due to Middle Cerebral Artery Occlusion: A Clinical- Histological Analysis of Retrieved Thrombi
Supplemental Material, Sup_1._mRS for Bridging Therapy Versus Direct Mechanical Thrombectomy in Patients with Acute Ischemic Stroke due to Middle Cerebral Artery Occlusion: A Clinical- Histological Analysis of Retrieved Thrombi by Li Gong, Xiaoran Zheng, Lijin Feng, Xiang Zhang, Qiong Dong, Xiaoyu Zhou, Haichao Wang, Xiaojun Zhang, Zhongwen Shu, Yanxin Zhao and Xueyuan Liu in Cell Transplantation
Footnotes
Author Contribution
Li Gong, Xiaoran Zheng, Lijin Feng: equal contribution.
Acknowledgment
This work was supported by a grant from the National Natural Science Foundation of China (No.81771131, No.81571033) and by the Science and Technology Commission of Shanghai Municipality (No.17411950100, No.17411967500).
Ethical Approval
This study was approved by the Ethics Committee of Shanghai Tenth People’s Hospital (Shanghai, China).
Statement of Human and Animal Rights
This study contained human subjects and was conducted in accordance with the Declaration of Helsinki.
Statement of Informed Consent
Written informed consent was obtained from the patient or legally authorized representative(s) for anonymized patient information to be published in this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.