
Abstract
Diabetes mellitus is a widely spread chronic disease with growing incidence worldwide, and diabetic foot ulcer is one of the most serious complications of diabetes. Cellular therapy has shown promise in the management of diabetic foot ulcer in many preclinical experiments and clinical researches. Here, we performed a meta-analysis to evaluate the efficacy and safety of cellular therapy in the management of diabetic foot ulcer. We systematically searched PubMed, MEDLINE, EMBASE, and Cochrane Library databases from inception to May 2017 for randomized controlled trials assessing the efficacy of cellular therapy in diabetic foot ulcer, and a meta-analysis was conducted. A total of 6 randomized controlled clinical trials involving 241 individuals were included in this meta-analysis. The results suggested that cellular therapy could help accelerating the healing of diabetic foot ulcer, presented as higher ankle-brachial index (mean difference = 0.17, 95% confidence interval [CI] = 0.11 to 0.23), higher transcutaneous oxygen pressure (standardized mean difference [SMD] = 1.43; 95% CI, 1.09– to 1.78), higher ulcer healing rate (relative risk [RR] = 1.78; 95% CI, 1.41 to 2.25), higher amputation-free survival (RR = 1.25; 95% CI, 1.11 to 1.40), and lower scale of pain (SMD = −1.69; 95% CI, −2.05 to −1.33). Furthermore, cellular therapy seemed to be safe, with no serious complications and low risk of short-term slight complications. Cellular therapy could accelerate the rate of diabetic foot ulcer healing and may be more efficient than standard therapy for diabetic foot treatment.
Introduction
The prevalence of diabetes mellitus (DM) worldwide is gradually increasing these years and this figure is predicted to continue growing, resulting in more than 360 million patients with DM in 2030. 1 Although it is manageable, diabetic foot ulcer is one of the most common and serious complications secondary to DM. Statistical data have indicated that 2% to 3% of patients with DM were suffering from active foot ulcer and a quarter of DM patients would develop foot ulcer throughout their lifetime. 2,3 Diabetic foot ulcer not only affects the physical health of patients, preceding 85% of major lower limb amputations in patients with DM, 4 but also has a significant effect on their social function and mental health. 5 Furthermore, the patients and society have to bear the substantial financial burden from treatment and care of diabetic foot ulcer. 6 The diabetic foot ulcer, in which neuropathy and peripheral vascular disease act as major pathogenic factors, is featured by the typical dysfunctions of wound healing, including coagulation, hemostasis, inflammation, proliferation, and remodeling. 7 Nowadays, the conventional standard therapy for diabetic foot ulcer consists of glucose-level control, infection management, high pressure remission, and dressings. However, the effectiveness of conventional standard therapy is not satisfying enough. Even with comprehensive treatment programs, the cure rate of diabetic foot ulcer in 12 to 20 wk was only as low as 24% to 30%. More seriously for patients, they are at high risk of serious complications, such as cellulitis, osteomyelitis, amputation, and others. 8 –10
Cellular therapy, characterized by using cells from diverse sources, with self-renewing potential and multidifferentiation ability, has shown promise in the management of diabetic foot ulcer. Accumulating evidences from basic science studies and clinical trials have pointed out that cellular therapy could focus on multiple facets during diabetic foot ulcer healing through cell proliferation, vascularization, neurorestoration, inflammation regulation, exosomes synthesis, and others. 11,12 Some clinical studies have demonstrated that cellular therapy represents an effective treatment for diabetic foot ulcer. However, reliable evidence on the clinical efficacy remains to be addressed. Therefore, the present study evaluates and synthesizes clinical evidence and aims to critically estimate the therapeutic efficacy of cellular therapy for diabetic foot ulcer compared to standard therapy.
Research Design and Methods
Search Strategy
An extensive literature search restricted to the English language was carried out up to May 2017 using the PubMed, MEDLINE, EMBASE, and Cochrane Library databases. The search terms we used were (stem cells, mononuclear cells [MNCs], and progenitor cells) and (diabetic foot, diabetic ulcer, and diabetic wound). In addition, we examined the reference list of all relevant articles.
Selection Criteria
Publications were screened independently by 2 authors. Studies meeting the following criteria were included: (1) randomized controlled trials comparing cellular therapy with standard therapy conducted in humans, (2) patients with diabetic foot ulcer, (3) full articles reporting the clinical efficacy. Studies that carried out in animals, lacking standard therapy as controls or lacking sufficient data of interest, were excluded. Referring to duplicate publications, the latest or larger one was included in the analysis.
Data Extraction and Quality Assessment
Effectiveness outcomes including ankle-brachial index (ABI), amputation-free survival (AFS), transcutaneous oxygen tension pressure (TcPO2), ulcer healing rate at 12 to 24 wk posttransplantation, and pain scales and the adverse events representing safety profile occurring during each trial were extracted from all the included studies by 2 authors independently.
The risk of bias of the included clinical trials was assessed in accordance with the modified Jadad rating scales. 13 Randomization, blinding, and follow-up were rated as yes, no, and not reported. 13
Discrepancies about literature search, study selection, data extraction, and quality assessment between the 2 authors were settled by discussion and consensus or determined by a senior author.
Statistical Analysis
Extracted data were entered and processed by Stata statistical software, version 12.0 (StataCorp, College Station, TX, USA). In order to estimate the clinical efficacy, mean difference and 95% confidence intervals (CIs) were calculated for quantitative variables and relative risk, and 95% CIs were calculated for dichotomous variables. Two-sided tests and a significant heterogeneity level of P < 0.05 were used in all analyses. Heterogeneity was estimated by the I 2 statistics, with values of 25%, 50%, and 75% being considered low, moderate, and high heterogeneity, respectively. When high heterogeneity was present, weighted mean difference and random effects model were applied to minimize heterogeneity; otherwise, the fixed effects model was used. We also performed Egger’s intercept test and Begg’s rank correlation analysis to estimate publication bias and conducted sensitivity analysis to examine the reliability of outcomes.
Results
Literature Search
The initial literature search yielded a total of 528 articles. After deletion of 379 duplicates, the remaining abstracts were carefully screened. One hundred twenty studies were excluded for various reasons such as reviews, animal experiments, and case reports. Of all the 29 remaining studies, 6 randomized controlled clinical trials meeting all criteria and providing a clear description data were selected. 14 –19 The screening process of the trials is shown in Fig. 1.
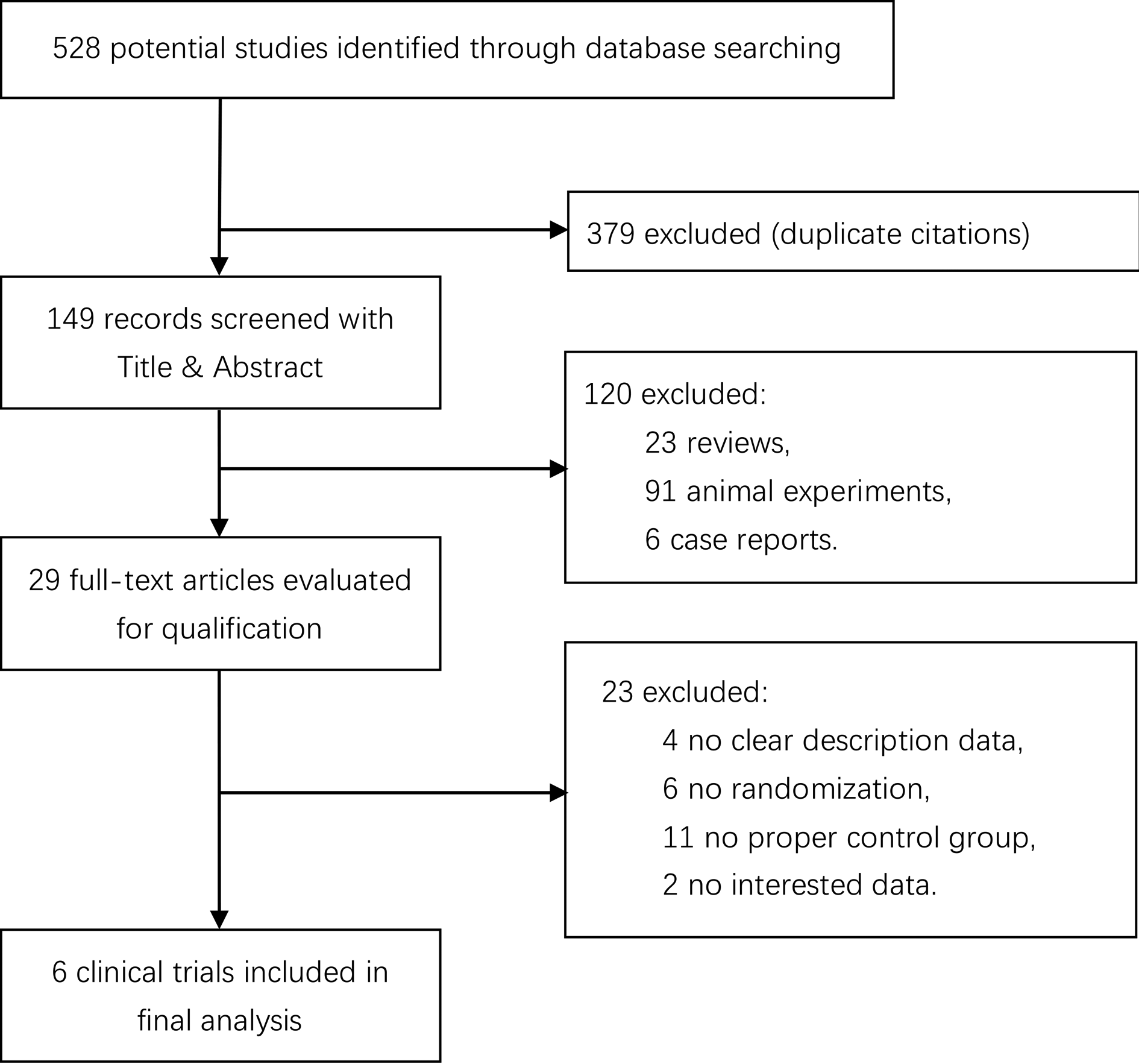
Flow chart of study selection.
Study Characteristics
After selection, 6 randomized controlled clinical trials involving 241 patients were included. Considering the cell type used in each study, 2 studies 14,19 used mesenchymal stem cells from bone marrow or umbilical cord, 3 studies 15,17,18 used MNCs from bone marrow or peripheral blood, and 1 study 16 used bone marrow-derived mesenchymal stem cells (BMMSCs) and bone marrow-derived MNCs (BMMNCs). Details of the study characteristics are listed in Table 1.
Study Characteristics of Included Studies.

Abbreviations: BMMSCs, bone marrow-derived mesenchymal stem cells; BMMNCs, bone marrow-derived mononuclear cells; PBMNCs, peripheral blood mononuclear cells; RCT, randomized controlled trials; SD, standard difference; UCMSCs, umbilical cord-derived mesenchymal stem cells.
aValues are presented in mean ± standard difference.
Quality Assessment
As evaluated by modified Jadad rating scales, 13 3 included studies were high-quality randomized clinical trials. 14,16,18 Quality assessment outcomes of all the included studies are presented in Table 2. All the included studies were described as randomized clinical trials, and 3 studies reported adequate sequence generation such as using random number table, 14 randomization table, 16 or internet-based system. 18 Allocation concealment was described only in 1 study. 14 One study claimed to be double-blinded, but details of blinding were not reported in this study. 16 All studies described the details of loss to follow-up.
Quality Assessment of the Included Studies.
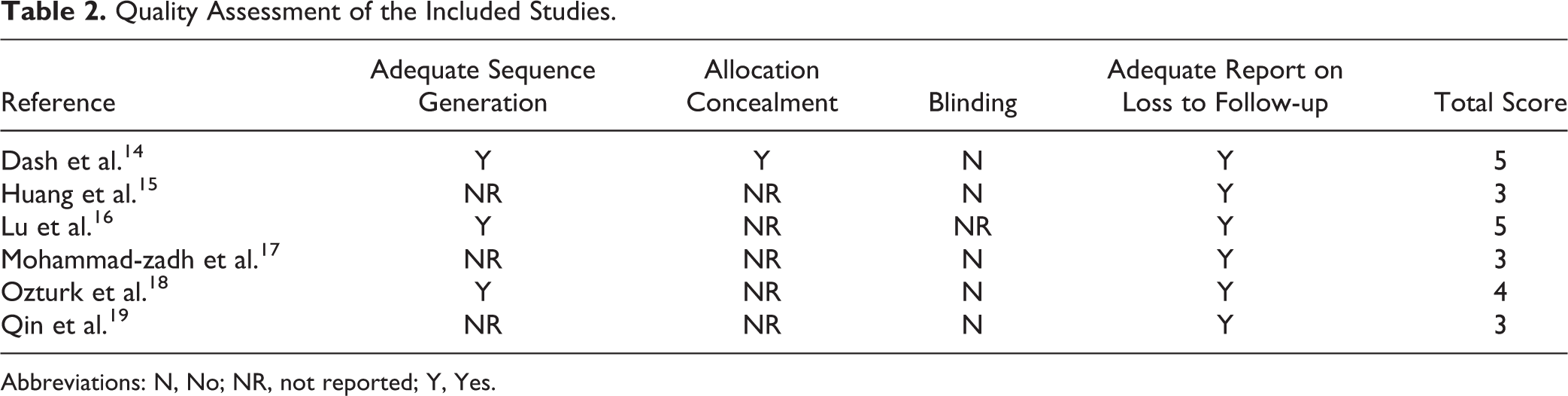
Abbreviations: N, No; NR, not reported; Y, Yes.
ABI
The ABI is defined as the ratio of the highest pressure detected by Doppler at the dorsalis pedis and posterior tibial arteries and the highest pressure at the brachial artery. The ABI provides such a great deal of information that it has become a routine measurement in the patients with diabetic foot ulcer. Five of the included studies 15 –19 involving 235 patients reported the ABI. Owing to no heterogeneity between studies (I 2 = 0.0%, P = 0.751), fixed effects model was applied in meta-analysis. The outcomes revealed that ABI was significantly raised by cellular therapy (mean difference = 0.17, 95% CI, 0.11 to 0.23; Fig. 2).

Forest plots for meta-analysis of ankle-brachial index (ABI) comparing cellular therapy with standard therapy. Area of the symbols for each study (square) is proportional to study weight. The pooled mean difference (fixed effects) and 95% confidence intervals are represented by the rhombus. Heterogeneity test across studies was significant (I 2 = 0.0%, P = 0.751). CI, confidence interval; WMD, weighted mean difference.
Transcutaneous Oxygen Pressure (TcPO2)
TcPO2 is known to be an indicator of the local microcirculation and the degree of ischemia and is valuable to predict healing at various levels of foot ulcer. 20,21 In the patients treated with cellular therapy, the TcPO2 values significantly increased (standardized mean difference [SMD] = 1.43; 95% CI, 1.09 to 1.78) in the analysis of 3 studies 16,18,19 (Fig. 3).

Forest plots for meta-analysis of TcPO2 comparing cellular therapy with standard therapy. Area of the symbols for each study (square) is proportional to study weight. The pooled standardized mean difference (fixed effects) and 95% confidence intervals are represented by the rhombus. Heterogeneity test across studies was significant (I 2 = 0.0%, P = 0.375). CI, confidence interval; SMD, standardized mean difference.
Pain Scale
Three trials reported the pain scale of patients with diabetic foot ulcer. Ozturk et al. 18 used numerical pain rating scale which ranged from 0 to 10, 0 being no pain and 10 being maximum pain. 22 In the randomized controlled trials conducted by Lu et al. 16 and Huang et al., 15 rest pain scores on rating scales ranged from 0 for the best (completely resolved) to 4 points for the worst condition (severe pain unresolved with paracetamol or nonsteroidal anti-inflammatory drugs). 22 There was no heterogeneity among these studies (I 2 = 0.0%, P = 0.973). The pain scale was significantly decreased (SMD = −1.69, 95% CI = −2.05 to −1.33) in the selected studies in the cellular therapy group (Fig. 4).
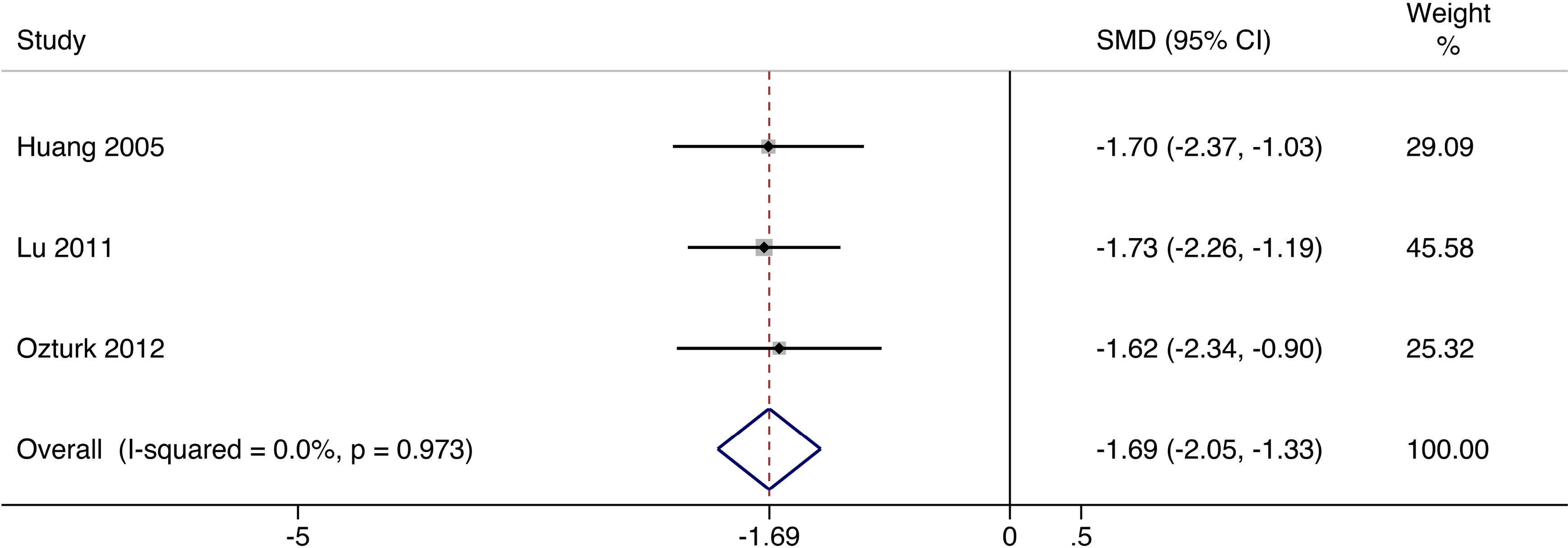
Forest plots for meta-analysis of pain scale comparing cellular therapy with standard therapy. Area of the symbols for each study (square) is proportional to study weight. The pooled standardized mean difference (fixed effects) and 95% confidence intervals are represented by the rhombus. Heterogeneity test across studies was significant (I 2 = 0.0%, P = 0.973). CI, confidence interval; SMD, standardized mean difference.
Ulcer Healing Rate
With regard to the efficacy of cellular therapy in contrast to the standard therapy, the relative risk of 3 trials 15,16,18 demonstrated a significant increase (relative risk [RR] = 1.78, 95% CI = 1.41 to 2.25) in ulcer healing rate 12 to 24 wk after cellular therapy using a fixed effects model (I 2 = 0.0%, P = 0.449; Fig. 5).

Forest plots for meta-analysis of ulcer healing rate comparing cellular therapy with standard therapy. Area of the symbols for each study (square) is proportional to study weight. The pooled relative risk (fixed effects) and 95% confidence intervals are represented by the rhombus. Heterogeneity test across studies was significant (I 2 = 0.0%, P = 0.449). CI, confidence interval; RR, relative risk.
AFS
The combined end point of AFS was considered to be the best outcome assessment indexes for patients with diabetic foot ulcer. 23 Four studies 15 –18 provided amputation data. With no heterogeneity (I 2 = 0.0%, P = 0.400), calculations under fixed effects model revealed that cellular therapy significantly improved the AFS rate in patients with diabetic foot ulcer (RR = 1.25, 95% CI = 1.11 to 1.40; Fig. 6).

Forest plots for meta-analysis of amputation-free survival comparing cellular therapy with standard therapy. Area of the symbols for each study (square) is proportional to study weight. The pooled relative risk (fixed effects) and 95% confidence intervals are represented by the rhombus. Heterogeneity test across studies was significant (I 2 = 0.0%, P = 0.400). CI, confidence interval; RR, relative risk.
Adverse Events
During 1 to 2 y long-time follow-up, no serious complications resulted from cellular therapy, such as rejection, allergic reactions, and tumorigenesis were observed. 14 –19 No complications such as puncture site hematoma, pseudoaneurysm, arterial dissection, or cardiovascular or cerebrovascular events related to the transplantation procedure were detected. 14 –19 No infection, bleeding, or other complications arose from the microbiological condition of the cells were detected. 14 –19 Only 8 of 118 patients suffered from short-term episodes of slight pain after cell transplantation 15,16 and 3 patients bled at the iliac crest after bone marrow aspiration. 15,16
Sensitivity Analysis
Sensitivity analysis was performed by reestimating the outcome by removing 1 study in each turn and was indicative of the reliability of the outcomes. Sensitivity analysis did not identify any marked difference in the direction and magnitude of the mean difference and relative risk with respect to ABI, TcPO2, pain scale, ulcer healing rate, and AFS, indicating good reliability of the outcomes in this meta-analysis.
Publication Bias
We assessed publication bias by Egger’s intercept test and Begg’s rank correlation analysis. The P values of the Egger’s test and Begg’s test were all greater than 0.05 for ABI (Begg’s test P = 1.000, Egger’s test P = 0.847), TcPO2 (Begg’s test P = 1.000, Egger’s test P = 0.549), pain scale (Begg’s test P = 0.296, Egger’s test P = 0.309), ulcer healing rate (Begg’s test P = 1.000, Egger’s test P = 0.975), and AFS (Begg’s test P = 0.308, Egger’s test P = 0.302), indicating no significant evidence of publication bias.
Discussion
The purpose of the present study was to perform a meta-analysis to assess the efficacy and safety of cellular therapy in treatment of diabetic foot ulcer. Our study included 6 randomized controlled trials involving 241 patients and analyzed 5 end point indexes which were important in the long-term prognosis and quality of life of patients with diabetic foot ulcer. It was shown that cellular therapy was significantly associated with a higher ABI, a higher transcutaneous oxygen pressure, more reduction in pain, a decreased risk of amputation, and a higher proportion of healed ulcers, when compared with standard therapy. The complete ulcer healing rate and AFS in cellular therapy group is 1.78 and 1.25 times more than control group at 12 to 24 wk, respectively. These findings are robust, as sensitivity analysis had confirmed that deletion of any study would not change the direction of the outcomes. Possible security threats resulted from cellular therapy frighten some clinicians away. However, our pooled statistics showed that cellular therapy seemed to be safe, with no serious complications and low risk of short-term slight complications.
Cellular therapy is an attractive approach delivering self-renewing cells in regenerative medicine. In the recent years, researchers have utilized direct systemic administration, local intramuscular injection, or direct application over the wound to deliver cells in cellular therapy. 24 Among all of the included studies in this meta-analysis, cells were delivered into the area surrounding the wound by means of muscle injection. Intramuscular injection 25,26 into the wound periphery was found to be safer and more efficient than systemic administration in animal research models and clinical studies. 27 The primary shortcomings of systemic delivery were cell trafficking and risk of malignancy resulted from wide distribution of exogenous cells, together with low intended location arrival rate. 28,29 Moreover, appropriate scaffold such as fibrin sealants has shown its advantage in promoting wound healing in animals and humans. 30 Possible mechanisms include confining cells, promoting engraftment, and maximizing their therapeutic effects. 31
Owing to no ethical controversy and diverse sources, adult cells are more preferred in clinical practice. Preclinical outcomes and clinical researches utilizing adult cells already have revealed attractive therapeutic promise in treating diabetic foot. In this review, adult cells were utilized in all the included literatures, consisting of BMMSCs, 14,16 umbilical cord-derived mesenchymal stem cells (UCMSCs), 19 bone marrow-derived MNCs (BMMNCs), 16 and peripheral blood MNCs (PBMNCs). 15,18
There is growing evidence that possible therapeutic mechanisms behind MSCs may be paracrine secretion of growth factors and cytokines 32 and their direct differentiation into vascular endothelial cells and skin components. 33 –35 Lots of researches believed that paracrine secretion played a greater role in diabetic wound healing. Numerous studies have proven the high-level secretion of various growth factors and cytokines, such as epidermal growth factor (EGF), basic fibroblast growth factor (bFGF), keratinocyte growth factor (KGF), insulin-like growth factor (IGF-1), transforming growth factor-β (TGF- β), vascular endothelial growth factor (VEGF), smooth muscle cell-derived growth factor-1α, interleukin-8 (IL-8), and angiopoietin-1. 36 –38 These growth factors and cytokines exert diverse therapeutic effects in diabetic wound healing including improving neovascularization, angiogenesis, regeneration, ameliorating inflammation, and interestingly, recruiting endogenous stem cells from the circulation for repair. 39 Reyes et al. also observed that transplanted mesenchymal stem cells could be differentiated into angioblasts and vascular endothelial cells and then functioned as mature endotheliocytes, contributing to neoangiogenesis in diabetic foot ulcer model. 40 However, differentiation may be of limited use as there is a low proportion of engraftment and differentiation. 35,41
MNCs are a group of cells consisting of several stem/progenitor cell populations and some other cell types. They are so abundant in peripheral blood and bone marrow that they can be collected directly for transplantation with no need for in vitro expansion. MNCs were found to promote local capillary and blood vessel reconstitution in infarcted limbs in a study by Stamm et al. 42 Sivan-Loukianova et al. reported accelerated epidermal healing and revascularization after MNC transplantation in a diabetic mouse wound healing model. During a 5 d observation period, an increase in vessel diameter was the main manifestation at early stages. Later, increases in vessel size and number both accounted for increased vascularization. 43
Studies also showed that endothelial progenitor cells (EPCs) from bone marrow or peripheral blood could proliferate, migrate, and be mobilized under ischemic stimulation in some pathological conditions. 44,45 Accumulating evidence has proven their therapeutic ability in diabetic foot ulcer. 46,47 Wound healing promotion and neovascularization were found by using embryonic stem cell–derived EPCs in Lee’s study. 46 They found rapid reepithelialization of wounds and reformation of granulation tissue after transplantation in a wound healing model. After further exploration, they put forward the idea that secretion of growth factors and cytokines by EPCs, including EGF, bFGF, VEGF, IL-6, IL-8, granulocyte-macrophage colony-stimulating factor (GM-CSF), and platelet-derived growth factor-AA (PDGF-AA), may account for the main therapeutic effect. 46 EPCs display endothelial-like characteristics, and their neovascularization effect seemed to be particularly suited in improving microcirculation in the management of diabetic foot ulcer. Taking the features of directed migration and vascularization into consideration comprehensively, EPCs not only play a part in tissue repair but also brought reperfusion into ischemic regions. 48 Asahara et al. reported enhanced capillary density and recovery of blood flow after EPC transplantation in athymic nude mice with hind limb ischemia. 45
As far as we know, this study is the first meta-analysis of randomized controlled studies comparing the clinical efficacy of cellular therapy in the management of diabetic foot ulcer. Limitations still existed in this study. First, the number of the included randomized controlled trials was small. Although there has been a growing number of studies reporting cellular therapy in diabetic foot ulcer, only a few studies fully meet our requirements. Second, the sample size and quality of the included studies remained a concern for the strength of the outcomes. Only 1 study contains more than 30 participants in each group. And information of allocation concealment was only reported in 1 study. Third was the variability of measurements and criterion of ulcer healing. Forth, baseline ulcer conditions that would affect the outcomes were not reported in all of the studies.
Conclusions
Compared to standard therapy, cellular therapy could help accelerate the healing of diabetic foot ulcer, which presents as higher ABI, TcPO2, ulcer healing rate, and lower scale of pain and amputation risk. These results need to be treated with caution, as the number of available randomized controlled studies and the follow-up duration were limited. More large-scale, well-designed randomized controlled studies with long follow-up duration are in urgent need to further examine the clinical value of cellular therapy in the management of diabetic foot ulcer.
Footnotes
Ethical Approval
Ethical Approval is not applicable.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from National Natural Science Foundation of China (No.81471201).