
Abstract
The ephemeral placenta provides a noncontroversial source of young, healthy cells of both maternal and fetal origin from which cell therapy products can be manufactured. The 2 advantages of using live cells as therapeutic entities are: (a) in their environmental-responsive, multifactorial secretion profile and (b) in their activity as a “slow-release drug delivery system,” releasing secretions over a long time frame. A major difficulty in translating cell therapy to the clinic involves challenges of large-scale, robust manufacturing while maintaining product characteristics, identity, and efficacy. To address these concerns early on, Pluristem developed the PLacental eXpanded (PLX) platform, the first good manufacturing practice–approved, 3-dimensional bioreactor-based cell growth platform, to enable culture of mesenchymal-like adherent stromal cells harvested from the postpartum placenta. One of the products produced by Pluristem on this platform is PLX-R18, a product mainly comprising placental fetal cells, which is proven in vivo to alleviate radiation-induced lethality and to enhance hematopoietic cell counts after bone marrow (BM) failure. The identified mechanism of action of PLX-R18 cells is one of the cell-derived systemic pro-hematopoietic secretions, which upregulate endogenous secretions and subsequently rescue BM and peripheral blood cellularity, thereby boosting survival. PLX-R18 is therefore currently under study to treat both the hematopoietic syndrome of acute radiation (under the US Food and Drug Administration [FDA]’s Animal Rule) and the incomplete engraftment after BM transplantation (in a phase I study). In the future, they could potentially address additional hematological indications, such as aplastic anemia, myelodysplastic syndrome, primary graft failure, and acute or chronic graft versus host disease.
Placenta-Derived Fetal Stromal Cell Therapy: An Introduction
Placenta-derived cell therapy products have been produced from a variety of placental regions (such as the decidua, amnion, and chorion), and the characteristics of mesenchymal stromal cells (MSCs) derived from these have been previously compared (reviewed in Hass et al. 1 ). This organ is not considered a controversial cell source and has the advantage of providing large quantities of “young” cells. In addition, collection of cells from the ephemeral placenta avoids the inconvenience and risks inherent to the invasive procedures used to harvest bone marrow (BM) or adipose tissue. Due to their intrinsic immunologic properties, placenta-derived cells can be administered safely without human leukocyte antigen (HLA) matching or immunosuppression, enabling the development of an allogeneic “off-the-shelf” product, that requires no additional manipulations at the patient bedside (or when product is thawed). Placental MSCs were shown to secrete higher levels of anti-inflammatory cytokines and be more potent immunomodulators than MSCs derived from other sources 2,3 , which may explain their higher potency in certain preclinical models 4,5 . Due to their therapeutic potential, the immunomodulatory and immunosuppressive potential of placental MSCs has been the focus of intense preclinical study 3,6 –24 . The advantages of placental stromal cell types originating from various regions (e.g., decidua, amnion, and chorion) have encouraged researchers to study their efficacy in numerous preclinical scenarios mimicking human clinical indications, including critical limb ischemia, stroke, graft versus host disease (GvHD), multiple sclerosis, Alzheimer’s disease, and others 8,18,21,25 –41 . The great advantage of using live cells as a therapeutic entity, as opposed to the more conventional biologics (such as monoclonal antibodies or single cytokines/growth factors), is 2-fold: (a) the cells respond to a changing environment and adjust their multifactorial secretome accordingly and (b) a single injection of live cells acts as a “slow-release drug delivery system,” providing support over a longer time course, than a single injection of a noncellular product would provide.
It is now well accepted that the main mechanism of action (MoA) of most MSC products is not through differentiation and engraftment but mainly through paracrine and endocrine secretions 42 –46 . These multifactorial secretions are what enable MSCs to be efficacious in treating complex indications whose symptoms cannot be alleviated by a single factor. While many characteristics are shared among MSCs from different sources, such as expression of the basic MSC cell surface markers (e.g., CD105, CD73, and CD29), MSCs derived from different placental compartments and cultured by different methodologies secrete different proteins to different levels 47 . Despite these differences, many types of MSCs have been shown to be capable of supporting hematopoietic recovery in numerous preclinical and clinical trials (recently reviewed in Fajardo-Orduna et al. 47 ). This is not surprising, given the fact that the ability of both fetal- and maternal-derived stromal cells originating from the placenta was shown to support human hematopoiesis 48 . Therefore, there has been much activity in advancing placenta-derived cell therapy in recent years, for hematopoietic as well as other indications 49 .
The placental organ is composed of cells of both fetal and maternal origin. PLX-R18, a placenta-derived cell therapy product originating from fetal cells within term placenta, is currently under development for treatment of hematopoietic disorders. PLX-PAD, another placenta-derived cell therapy product, differs from PLX-R18 in that it is mainly maternal in origin; secretes significantly lower levels of interleukin (IL-6), IL-8, and monocyte chemoattractant protein-1 (MCP-1); and is not capable of inducing BM migration. Preclinical studies of PLX-R18 and its prototype PLX-RAD have indicated an MoA by which multiple hematopoietic factors are secreted when exposed to an imbalanced hematopoietic environment. In vivo, intramuscular (IM) administration of PLX-R18 alleviates radio-induced lethality and weight loss in a mouse model of acute radiation syndrome (ARS) and enables faster recovery of cellularity in the BM and blood. The injected cells respond to radiation-induced hematopoietic failure by transiently secreting hematopoiesis-related cytokines, growth factors, and additional proteins to enhance reconstitution of the hematopoietic system. Importantly, cells administered to nonirradiated controls only weakly secrete these various proteins, with important implications for treatment in mass-casualty scenarios. In vitro, PLX-R18 secretes hematopoiesis-promoting proteins, stimulates colony formation, and induces BM migration, explaining its In vivo MoA. Taken together, placenta-derived stromal cells have the capacity to promote recovery from BM failure and are currently under study to treat both the hematopoietic syndrome of acute radiation (under the Animal Rule) and the incomplete engraftment after BM transplantation (in a phase I study). In the future, they could potentially address additional hematological indications, such as aplastic anemia, myelodysplastic syndrome, primary graft failure, and acute or chronic GvHD.
Compliance of PLX-R18 Preclinical Data with the FDA Animal Rule.

Abbreviations: RBC, red blood cell; WBC, white blood cell; MoA, mechanism of action; NHP, non human primate; CFU, colony forming unit; BMM, bone marrow migration.
Clinical Manufacturing Process
One of the main hurdles to translating somatic cell therapy to the clinic are the significant challenges inherent in translating a research-grade method to a reproducible and robust manufacturing process suitable for routine large-scale production of cell therapy products 50 . This is particularly pertinent when applied to cell therapies, since the majority of these are developed not by large pharmaceutical companies according to approved standard operating practices and in compliance with good manufacturing practice (GMP)/good clinical practice and high-quality industrial standards but by hospitals, university laboratories, or Small Medium Enterprises (SMEs). Mainly due to budgetary constraints, most of these small organizations usually decide to opt first to seek validation of the safety and efficacy of their cell-based therapeutic product, only to be confronted by the critical manufacturing process issues at a later stage. However, it is well accepted by the medical community that the manufacturing process has a major effect on cell properties, and that necessary modifications during the scale-up may result in changes in the product characteristics and functionality. In contrast to other biotechnology products, where unequivocal characterization of the active product molecule is possible, in cell therapy, such changes may for regulatory purposes necessitate repeat toxicological and even clinical studies, in order to reestablish safety and efficacy of the product coming from the newly designed large manufacturing scale.
Pluristem’s PLX platform, the first GMP-approved, 3-dimensional (3-D) bioreactor-based cell growth platform, enables culture of mesenchymal-like adherent stromal cells (ASCs), harvested from the postpartum placenta. All PLX products are ex vivo expanded ASCs derived from the placenta. Different cell populations have different properties and thus different therapeutic potential 51,52 . The PLX platform enables controlled modification of culture conditions to select for specific cell populations. The PLX cell expansion manufacturing process comprises 2 stages (see Figure 1).
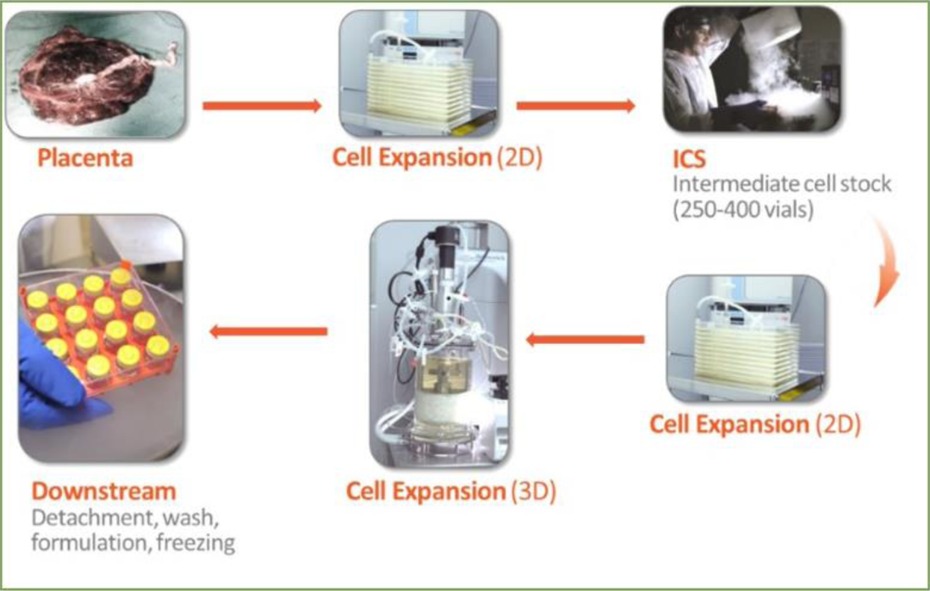
PLX manufacturing process. stromal cells are isolated from a placenta and expanded by 2-dimensional (2D) growth to produce the intermediate cell stock (ICS). The final PLX product is produced by further culture expansion of the ICS in a 3-dimensional (3D) bioreactor.
In the first stage, ASCs are isolated from a placenta and expanded by 2-dimensional (2-D) growth to produce the intermediate cell stock. During the second stage, the intermediate cell stock is thawed and undergoes further culture expansion using 3-D growth in a bioreactor to produce the PLX cell products. The final formulation of the PLX-based drug substance occurs immediately after harvest of the PLX-based cells from the 3-D growth bioreactor. The cell suspension is dispersed into cryogenic vials and cryopreserved in the vapor phase of liquid nitrogen (≤ −150 °C) until use.
There are several significant advantages to the use of 3-D bioreactor-based growth. First, the use of bioreactors allows for online culture control, enabling consistent processes with minimal batch-to-batch variation. Bioreactors also allow for a closed, automated, and scalable process, enabling a reproducible, predictable end product with minimum risk of contamination. Second, the surface to volume ratio in the bioreactor is 70-fold larger than in 2-D cultures, leading to a requirement for dramatically smaller facilities and an increase in the efficiency of use of materials and man power. This competitive advantage enables industrial scale production and shortens the processing time, which is a major limitation of 2-D systems. These advantages enable production of the quantities and qualities of cells necessary for a successful clinical trial.
Cell Characterization: Quality, Identity, and Biological Activity
Fetal mesenchymal adherent cells manufactured on the PLX platform are characterized by a high expression of typical mesenchymal cell markers, namely, CD105, CD73, and CD29, and lack of surface expression of CD45, CD34, CD14, CD19, and Human Leukocyte Antigen – D Related (HLA-DR) 53 . In addition, they do not express CD31 (an endothelial marker) and GlyA (an erythrocyte cell marker) on their surface. PLX cells do not express HLA class II molecules (HLA-DP, DQ, and DR) or costimulatory markers (CD80, CD86, and CD40) on their membrane, enabling them to be immune evasive. Unlike BM-derived MSCs, PLX cells exhibit limited capacity to differentiate by standard protocols into osteocytes and adipocytes, and as such, their proposed MoA is based on cytokine secretions.
Routine testing performed on all PLX cells manufactured includes measurements of cell quality and safety, identity, and potency. Cell quality and safety measurements include viability, postthaw recovery, karyotype, sterility, endotoxin, and mycoplasma. Cell identity tests include % fetal cells and immunophenotyping analyses. Functional tests are defined by the downstream clinical application and, in the case of fetal PLX cells, include the ability to induce BM migration in vitro and the secretion of various cytokines 54 . BM migration is tested in a Transwell assay, in which mouse heparinized BM cells (from BALB/c mice) are seeded into the upper compartments of a 24-well Transwell plate with 5-μm pores, conditioned medium from 24 h PLX-R18 growth is added to the lower compartments of the Transwell plate, and migrated cells are counted after 24 h using a Vi-Cell™ XR. Cytokine secretion analysis is performed after 24 h incubation of PLX-R18 cells using Quantikine® enzyme-linked immunosorbent assay (ELISA) kits (R&D Systems, Minneapolis, MN, USA).
PLX-R18 In Vivo
ARS is a syndrome involving damage to multiple organs caused by exposure to a high dose of ionizing radiation over a short period of time; even low doses of radiation damage the radiosensitive hematopoietic system (causing hematopoietic subsyndrome-ARS [H-ARS]). The efficacy of IM administration of PLX-R18 and their PLX-RAD prototype in promoting recovery of the hematopoietic system following acute radiation has been tested in C3H/HeN and C57BL/6 mice, 2 murine models with different radiosensitivities. Optimization of the dosing and dose schedule, performed on the C3H
Preliminary murine studies indicated that no animal deaths occurred past day 23; therefore, most subsequent MoA studies focused on assessing differential parameters up to this time point. Figure 2 shows an overview of in vivo findings in preclinical H-ARS models. Weight, survival, and peripheral blood and BM cellularity were monitored at several time points up to 23 d (general study design illustrated in Fig. 2A). Treatment significantly increased survival after irradiation and rescued radio-induced weight loss relative to vehicle-injected controls (Fig. 2B). In addition, treatment significantly increased the number of colony forming hematopoietic progenitors in the BM (not shown) and raised peripheral blood cellularity (Fig. 2C) to values near those of unirradiated naive controls. This was true of platelets, red blood cells, and white blood cells. The injected cells responded to radiation-induced hematopoietic failure by transiently secreting hematopoiesis-related proteins, supporting reconstitution of the hematopoietic (Fig. 2D) 54,55 , whose peak secretions were on days 6 to 9 after irradiation. These secretions subsequently prompted further endogenous murine secretions (Fig. 2E). Importantly, negligible levels of human-derived secretions were measured in nonirradiated-treated animals (Fig. 2D), with important implications for use in possible victims of H-ARS.

Overview of major effects of placenta-derived fetal adherent stromal cells in vivo. (A) General study design of hematopoietic subsyndrome-acute radiation syndrome (H-ARS)-induced animal models. Mice are irradiated on day 0 and treated with fetal stromal cells (or vehicle control) on days 1 and 5 after irradiation. (B) Administration of fetal stromal cells rescues radio-induced lethality (left) and weight loss (right) in the H-ARS mouse model. (C) Administration of fetal stromal cells rescues platelet, red blood cell, and white blood cell (WBC) counts on day 23 in the H-ARS mouse model. (D and E) A time-course analysis of secretions of human (D) and murine (E) proteins in the peripheral blood over time in irradiated and nonirradiated mice indicates that treatment enhances secretion of exogenous and endogenous hematopoiesis-promoting cytokines in irradiated mice. Human (PLX-derived) secretions are highest on days 6 to 9. Nonirradiated mice treated with fetal stromal cells secrete only negligible levels of human proteins. (F) A comparison of efficacy of 2 PLX products in the H-ARS model indicates that fetal stromal cells are significantly more potent than maternal cells and secrete hematopoietic proteins to much higher levels on days 6 and 9.
An additional, a placental product derived from maternal cells also prepared by Pluristem on the PLX platform, PLX-PAD, was significantly less efficacious in decreasing H-ARS lethality and improving complete blood count (CBC) recovery (Fig. 2F, left), strengthening the specificity of each product for its target indications. As secretions of fetal PLX cells were highest on days 6 to 9, the secretions of the 2 PLX products were compared on these days, to gain insight as to the possible MoA and important cytokines. PLX-PAD secreted significantly lower levels of cytokines putatively involved in the PLX-R18 MoA (granulocyte colony-stimulating factor [G-CSF], IL-6, IL-8, and MCP-1), possibly explaining the difference in efficacy between the 2 products (Fig. 2F) 54 . Taken together, placenta-derived fetal cells manufactured on the PLX platform have the capacity to improve recovery from BM failure in the H-ARS murine model.
PLX-R18 In Vitro
To gain a better understanding of the PLX-R18 MoA, in vitro analyses were performed. In vitro as well as in vivo (see above), PLX-R18 cells and their PLX-RAD prototype have been shown to secrete proteins relevant to hematopoietic rescue to a much higher extent than maternal-derived PLX-PAD produced on the PLX platform (Fig. 3A). Many of the secreted proteins are known to be involved in support of hematopoietic reconstitution (e.g., G-CSF, granulocyte-macrophage colony-stimulating factor [GM-CSF]). Consistent with in vivo studies, fetal cells are more potent than maternal cells in inducing the migration of BM cells and colony formation from BM cells in vitro (Fig. 3B and C) 54 . Importantly, human BM is even more responsive to PLX-R18-derived conditioned medium than is mouse BM (see Fig. 3D), implying the potential for higher potency in clinical trials. Overall, in vitro studies of PLX-R18 support the proposed MoA, whereby cytokine secretion supports reconstitution of BM and peripheral blood cellularity via an induction of colony formation and BM migration.

Fetal mesenchymal adherent cell activity in vitro: cell secretions and induction of bone marrow migration and colony formation. (A) Cytokine levels secreted by fetal and maternal PLX products into medium in vitro were measured by Luminex assay. The fetal stromal product secretes significantly higher levels of numerous cytokines involved in hematopoietic reconstitution. (B and C) The ability of PLX cells to induce bone marrow migration (B) and colony formation (C) was compared and indicated that only fetal stromal PLX cells exhibit potency in these in vitro assays. (D) Fetal PLX cells induce migration of fresh human bone marrow to higher levels than those induced in murine bone marrow.

Level of PLX-R18 (as measured by human DNA quantity) in muscle injection site after intramuscular administration over time.
PLX-R18 Biodistribution and Toxicology Studies
In order to support the initiation of a phase 1 first-in-human study, general toxicology and biodistribution studies have been performed with PLX-R18 in non-obese diabetic/severe combined immunodeficiency, NOD/SCID mice. This model was chosen in order to maximize the persistence of human-derived cells in the murine preclinical setting. The general toxicology study was performed in order to assess potential toxic effects of the PLX-R18 in target and nontarget tissues at various time points. The safety profile of the cells indicated no adverse effects in either IM or intravenous (IV) administration of 1 million PLX-R18 cells per animal IM or 40 million PLX-R18 cells/kg IV in 2 doses. Based on the toxicology studies, the no observed adverse effect level is at least 1 million PLX-R18 cells/25 g mouse administered twice (1 wk between doses). The doses used in the toxicology study are equivalent to ∼40 million cells/kg. Therefore, the first in-human study with PLX-R18, described below, has a 10-fold margin of safety relative to the toxicity studies performed.
The quantitative polymerase chain reaction (qPCR)-based biodistribution study was performed to determine the distribution and persistence of the PLX-R18 in target and nontarget tissues at various time points after injection. This study indicated that PLX-R18 cells injected IM remained local, and very few cells remained in the body at 13 wk (Fig. 4).
Taken together, the nonclinical in vivo and in vitro data suggest that there is a potential therapeutic benefit of PLX-R18 in supporting regeneration of the hematopoietic system in indications involving BM failure. The toxicology and biodistribution studies support the initiation of a first-in-human phase 1 clinical study in patients suffering from incomplete engraftment following hematopoietic cell transplantation (HCT). These, in addition to further preclinical studies, may support the use of PLX-R18 under the FDA’s Animal Rule in the case of H-ARS.
Clinical Pipeline
Several clinical studies of placental cell therapies have been performed, including studies of placental stromal cells for treatment of peripheral artery disease, total hip replacement, Crohn’s disease, Peyronie’s disease, and erectile dysfunction (clinicaltrials.gov identifier NCT03006770 and NCT02264288, NCT01525667, NCT01155362, NCT02395029, and NCT02398370, respectively). To date, clinical trials with placental cells have been phase I and II studies, although PLX-PAD is now being tested in a phase III study (clinicaltrials.gov identifier NCT03006770, currently recruiting). Trials of MSCs, and in particular of placenta-derived MSCs, have tested both the IV and IM routes of administration, and these have been proven safe 38,56 –61 , with modest adverse effects generally deemed acceptable in the patient groups under study. Clinical trials of placenta-derived cells have included indications such as Crohn’s disease, pulmonary fibrosis, pulmonary sarcoidosis, GvHD, diabetes, and others 57,60 –69 .
Based on preclinical safety studies and on the efficacy of PLX-R18 in BM failure models, Pluristem has chosen to initiate the clinical development of PLX-R18 in a population of patients suffering from incomplete hematopoietic recovery following HCT as well as for ARS (under the FDA’s Animal Rule, see below). Future possible hematological indications such as aplastic anemia, myelodysplastic syndrome, and others are also under consideration for PLX-R18 clinical studies.
Incomplete Engraftment
HCT is a standard treatment for various malignant and nonmalignant conditions. A successful HCT leads to the recovery of full BM function, including the return of blood counts to normal (or near normal) values. However, in a number of cases, complete hematopoietic recovery is not achieved after HCT. This may occur despite an intensive preparative regimen, an adequate cell dose, and successful engraftment as evident by complete donor chimerism 70 . Incomplete recovery may affect any of the blood lineages to various degrees of severity. In patients who have survived for more than 6 mo after HCT, the underlying mechanism mainly involves BM hypocellularity and impaired maturation of BM progenitor cells 71 –73 . Based on the deficiencies in blood count, patients who experience incomplete hematopoietic recovery following HCT are exposed to increased risks of bleeding, infection, and poor general function. Prolonged thrombocytopenia after HCT was found to be associated with higher mortality and infection rates as well as with a generally poorer prognosis 72 .
The mainstay of therapy for incomplete hematopoietic recovery is the treatment of the patient’s hematological deficiencies. Factors such as G-CSF, GM-CSF, and erythropoietin may be administered 74,75 , and use of other products, such as the thrombopoietin receptor agonist, are still under investigation 76,77 . A significant proportion of patients do not respond to growth factors and remain cytopenic 78 . They often need to receive frequent blood product transfusions, with inherent risks of infections and allosensitization. Thus, there is an unmet medical need for additional treatment options for these patients.
The use of MSCs for the treatment of patients with incomplete hematopoietic recovery/poor graft function after HCT has been investigated in several pilot studies; in these, most patients demonstrated improvement in blood counts 74,78 –80 . Pluristem has initiated a first-in-human open-label dose escalation phase 1 study in adult patients with a prolonged incomplete hematopoietic recovery following either autologous or allogeneic HCT (clinicaltrials.gov identifier NCT03002519, currently recruiting). The patient population includes subjects at 6 mo or more after the HCT and will have sustained levels of platelets ≤50,000/μL and/or hemoglobin ≤8 g/dL, with sufficient neutrophil count (≥1,000/mm3) at the time of enrollment.
Since it is the first in-human study with PLX-R18, it is planned to utilize a dose escalation design, in which 3 doses will be tested, administered in 2 sessions of IM injections at a 1-wk interval: the first 3 patients will be treated at a dose of 1 million cells/kg, the next 12 patients at a dose of 2 million cells/kg, and additional 15 patients at a dose of 4 million cells/kg, for a total of 30 patients.
The primary objective of the study is to assess the safety of PLX-R18. Safety end points will include adverse events, vital signs, and electrocardiograms as well as hematological and biochemical testing. In addition, exploratory efficacy parameters will be assessed, including changes in blood counts, in the numbers of transfusions required, and in the quality of life during the follow-up period. Immunological laboratory testing will also be performed. The patients will be followed up for 1 y after treatment with PLX-R18.
ARS
As animal model data suggest that PLX-R18 has the capacity to alleviate radio-induced lethality and improve hematopoietic recovery, PLX-R18 is being developed under the Animal Rule, in the United States in parallel to phase I first-in-human clinical trials. The Animal Rule applies to the development of drugs relevant to life-threatening conditions where human efficacy trials are not ethical. It stipulates the necessity for 4 facets: (1) a reasonably well-understood mechanism of toxicity of the agent and of its prevention by the product, (2) the effect is demonstrated in one or more animal species predictive of human response, (3) the animal study end point is relevant to the desired benefit in humans, and (4) pharmacokinetic and pharmacodynamics data are available which allow selection of the effective dose in humans (see Table 1).
Concluding Remarks
Taken together, the in vivo and in vitro data support the proposed mechanism of PLX-R18 cells as one involving a timely secretion of multiple factors to support hematopoietic system recovery in response to an environment experiencing BM failure (see Fig. 5). In preclinical studies in which irradiated mice were treated on days 1 and 5 with placenta-derived fetal ASCs, treatment-derived secretion occurred within 24 h of the first treatment and continued for roughly 2 wk after irradiation, peaking on days 6 to 9. The rise in exogenous cell-derived factors preceded a later rise in endogenous hematopoietic factors, which were secreted earlier and/or higher in treated animals than in irradiated vehicle-treated controls. Together, secretion of exogenous (treatment-derived) and endogenous factors enabled an earlier increase in the number of multilineage hematopoietic progenitor cells in the BM and enabled migration of BM cells. The higher levels of BM cellularity evident following treatment allow earlier hematopoietic rescue after irradiation. Proliferation, differentiation, and migration of BM cells ultimately lead to an elevation in the levels of multiple blood lineages in the peripheral blood. The end result of this regenerated hematopoietic system is a higher survival rate in treated irradiated mice. Based on the cumulative data, PLX-R18, an allogeneic off-the-shelf product, is expected to support the recovery of all 3 blood lineages, including platelets, in humans experiencing BM failure. Existing single hematopoiesis-inducing factors are incapable of rescuing all lineages, demonstrating the benefit of the multifactorial secretion profile of PLX-R18, which indicates that it may be useful for a wide range of hematopoietic indications.

Graphical overview of proposed mechanism of action of PLX-R18 in vivo. A timely secretion of exogenous and endogenous factors supporting hematopoiesis enable an earlier rise in bone marrow cellularity. This in turn allows for rescue of radio-induced lethality and a rise in peripheral blood cell counts.
Footnotes
Authors’ Note
NS and RO are paid employees and shareholders of Pluristem.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.