
Abstract
Despite evidence supporting numerous scientific issues (e.g. climate change, vaccinations) many people still doubt the legitimacy of science. Moreover, individuals may be prone to scepticism about scientific findings that misalign with their ideological beliefs and identities. This research investigated whether trust in science (as well as government and media) and COVID-19 vaccination intentions varied as a function of (non)religious group identity, religiosity, religion–science compatibility beliefs, and/or political orientation in two online studies (N = 565) with university students and a Canadian community sample between January and June 2021. In both studies, vaccination intentions and trust in science varied as a function of (non)religious group identity and beliefs. Vaccine hesitancy was further linked to religiosity through a lack of trust in science. Given the ideological divides that the pandemic has exacerbated, this research has implications for informing public health strategies for relaying scientific findings to the public and encouraging vaccine uptake in culturally appropriate ways.
Keywords
Throughout the COVID-19 pandemic, public trust in science has been put to the test. This has been due, in part, to our hyper-connected world, in which scientific research has been challenged through various forms of media and conflicting government reports. As many individuals have turned to these resources to stay informed, obscurity regarding the legitimacy of scientific information has led to public confusion and mistrust (Hillard, 2020). Moreover, some individuals may be especially prone to scepticism about scientific findings that do not align with their personal religious beliefs (or lack thereof) (Beauchamp and Rios, 2020). In this regard, adherence to public health measures, including the delay or refusal of vaccines, may be influenced by one’s (non)religious group membership (Nagar and Ashaye, 2022). Indeed, individuals are more likely to be influenced by those with whom they identify and share common characteristics and beliefs (Tajfel and Turner, 1986). Thus, efforts to contain the virus ought to acknowledge group-level factors that may influence trust in science and the subsequent adoption of health behaviours (Cruwys et al., 2020; Van Bavel et al., 2020). Building on previous research (e.g. Beauchamp and Rios, 2020; Mavor and Ysseldyk, 2020; Taha et al., 2014; Ysseldyk et al., 2010), in two studies, we investigated links among religious beliefs and identity, trust in science (as well as government and media), and COVID-19 vaccination intentions in religiously diverse online samples in Canada.
Religious beliefs and trust in science
Substantial differences in levels of scientific trust exist between religious and non-religious individuals (e.g. McPhetres and Zuckerman, 2018; Rutjens et al., 2018b), being manifested on diverse issues, including climate change, genetically modified foods and vaccinations, among others, with religious individuals typically perceiving scientific evidence as a less trustworthy source of information. Furthermore, research on religiosity (i.e. the salience, importance or centrality of a particular worldview) has indicated that the extent to which individuals are religious can impact subsequent health behaviours, with mixed findings including reduced smoking on one side (Bailey et al., 2015) and greater vaccine scepticism on the other side (Rutjens et al., 2022). Interestingly, although both science and religion seek to provide answers, different perspectives and ways of knowing are constructed to do so (Rutjens et al., 2018a). This disagreement in understanding has led to a contentious relationship between science and religion, especially as religiosity can serve a dual function as a social identity and also as an unfalsifiable belief system (Ysseldyk et al., 2010). Members of various religious communities may consequently reject scientific knowledge that challenges their beliefs (Evans and Evans, 2008; Hornsey, 2020). In addition, scientists themselves are often perceived as secular, which may contribute to some religious believers’ distrust of science (Beauchamp and Rios, 2020).
Understandably, trust is fundamental for the public understanding of science, as some laypeople may possess a limited amount of scientific knowledge on a given topic (Hendriks et al., 2016). Furthermore, trust itself can be an ambiguous construct, and is often based on a combination of knowledge, beliefs, emotions and relationships (Nadelson et al., 2014). Thus, several factors may contribute to trust in science, including the mediums through which individuals receive their scientific information (e.g. the media) and their pre-existing belief systems (e.g. political or religious). Similarly, individuals are often more sceptical about information when it holds negative implications for the self (e.g. disputes their religious belief system; Liberman and Chaiken, 1992), prompting them to assess research in self-affirming ways (Morton et al., 2006). It has also been suggested that religiosity can create perceptions of science-religion conflict as well as predict greater distrust of scientific information (Evans, 2011).
Links to ideological social identities
According to the social identity and self-categorization position (Tajfel and Turner, 1986), people define themselves, in part, based on their memberships in various groups. This involves both personal identity (i.e. as a distinctive individual) and many social identities (i.e. as members of groups that have significant meaning to the individual). Importantly, social identification with a particular group has been linked with increased social support (Haslam et al., 2014; Matheson et al., 2020) and conformity to group norms (Hogg and Smith, 2007; Stevens et al., 2019). These norms can include a variety of health behaviours; for example, an individual may be more or less likely to get vaccinated depending on the group with which they identify (Cruwys et al., 2020). Although many social groups can serve these functions, it has been argued that religious identity not only shares many of the social norm, support and belonging functions of other identities, but may also play a powerful role in shaping behaviour. Suggestions that religion can influence behaviour are derived from the notion that religious individuals share a set of phenomenological and ontological beliefs that guide them through life (Bryant-Davis and Wong, 2013; Ysseldyk et al., 2010).
In addition to religious identity, other group identities may also influence behaviour, especially when they are grounded in ideological belief systems. Indeed, trust, social influence and shared values are some of the main factors that contribute to behavioural change, which has become fundamental to mitigate the spread of COVID-19 (Tunçgenç et al., 2021; Van Bavel et al., 2020). In this regard, the COVID-19 pandemic has been politicized in the face of perceived scientific uncertainty (Kreps and Kriner, 2020). Furthermore, liberals and conservatives often have differing levels of trust in science (Nisbet et al., 2015). Among Americans specifically, a link has been observed between political conservatism and fewer precautions to keep oneself and others safe from the coronavirus (i.e. getting vaccinated, social distancing; Latkin et al., 2022). Thus, in addition to religious identity and beliefs, political orientation (as well as other demographic or ideological factors) may be associated with trust in science and subsequent vaccination intentions.
Links to vaccination intentions
While the pandemic has brought the issue of vaccine hesitancy to the forefront, past research on vaccination intentions in Canada for severe diseases had indicated considerable hesitancy to vaccinate. For example, following the 2009 H1N1 pandemic, relatively low rates of vaccination intent emerged in a Canadian population despite the severity and global concern surrounding the illness (Taha et al., 2014). In the end, only a small proportion of individuals in Canada were vaccinated against H1N1 despite public health efforts to encourage vaccination; individuals were hesitant to accept a ‘new vaccine’ (Henrich and Holmes, 2009). Although various socio-demographic factors (e.g. race, education, income) can have an impact on perceptions of the risks and benefits of vaccines, greater religiosity (at least within the United States) has been connected to lower rates of vaccination (Kumar et al., 2016). Moreover, Canadian research that examined the percentage of students (within the province of Ontario) with immunization exemptions to the measles vaccine found that religious or conscientious exemptions significantly increased during a 10-year study period (Wilson et al., 2015). As the COVID-19 vaccine was crucial in slowing the spread of the virus, the examination of individuals’ beliefs and how they may impact trust in science and health behaviours may be fundamental in developing vaccination programmes when the next pandemic appears.
Previous research has shown that COVID-19-related health behaviours can be influenced by group membership (Cruwys et al., 2021). Importantly, both trust in science and religious beliefs have been linked to attitudes towards vaccination, but these may differ across religious groups (Rutjens et al., 2018b; Upenieks et al., 2022). On the one hand, trust in scientists was accompanied by favourable attitudes towards vaccination in various countries around the world (Algan et al., 2021). On the other hand, some religious groups have harnessed their belief systems to delay or refuse vaccination (Kanozia and Arya, 2021). In the face of a threat, such as the COVID-19 pandemic, an individual may turn to religion as a means of coping with the situation in addition to – or instead of – trusting in science. In the pandemic context, an individual’s assessment of risk and subsequent decision-making is determined by the health information obtained from science, the government and the media as well as the trust that they have in these sources (Taha et al., 2013). Considering the confidence that religion can provide in the midst of uncertainty (Kay et al., 2010; Ysseldyk et al., 2010), individuals may use religion to cope with the COVID-19 pandemic, which may also influence their trust and intentions to be vaccinated.
The present research
Given the spread of COVID-19 and accompanying pressures on the scientific community, an examination of how (non)religious identities and beliefs shape people’s attitudes towards science information, the scientific community, the mediums through which scientific findings are presented and subsequent health behaviours, is timely. However, given vast differences in healthcare systems and differing political, cultural and historical landscapes, it is difficult to generalize findings across countries. Therefore, in two studies, the present research examined potential differences in COVID-19 vaccination intentions and trust in the government, media and science across (non)religious groups in multicultural Canadian samples. Moreover, links between religiosity and vaccination intentions were examined, as were the mediating roles of trust in science, government and media. These findings aim to fill a current research gap by examining these links in diverse, multi-faith samples, with the broader goal to inform public health initiatives and knowledge mobilization strategies for relaying scientific findings to the public in culturally appropriate ways.
Study 1
Study 1 assessed differences in COVID-19 vaccination intentions and trust (in government, media, and information from the scientific community) across a variety of (non)religious groups, as well as the potential mediating role of trust in the relationship between religiosity and vaccination intentions. Importantly, data collection occurred in January and February 2021, shortly after effective COVID-19 vaccines had been developed but before they were widely available in Canada. At the beginning of data collection, less than 0.1% of Canadians had been fully vaccinated, and only 1.4% were fully vaccinated at the end of the data collection period (Public Health Agency of Canada, 2021).
Method
Participants and procedure
A total of 285 students (229 female, 51 male, 5 other; 17–58 years, M = 20.78, SD = 4.98) were recruited at a Canadian university and completed an online survey for course credit. According to G*Power, this sample size provided us with 92% power to detect medium effect sizes (two-tailed; Erdfelder et al., 2009). 1 Although 345 responses were initially collected, 60 participants were removed due to incomplete or invalid data. 2 Participants self-identified their age, sex, ethnic/racial identity, 3 religious affiliation, highest level of education and average annual household income. (Non)religious group affiliation was divided for analyses into four groups, namely Atheists/Agnostics (n = 65), Christians (n = 87), those who were ‘Spiritual but not religious’ (n = 66) and participants who self-identified as belonging to a range of religions that represent ‘Minorities’ in Canada (i.e. Muslim, Jewish, Baha’i, Buddhist, Hindu, Sikh; n = 67).
Measures
Vaccination intentions
Participants reported how likely, from 1 (very unlikely) to 5 (very likely), they were to get vaccinated for COVID-19; participants who indicated no intent to get vaccinated were coded with 0 (Taha et al., 2013).
Trust
Participants were asked to report their level of trust (based on Taha et al., 2013), from 1 (not at all) to 4 (completely), in various sources (e.g. news outlets, scientific community, government) to provide accurate COVID-19 information. A mean score was computed for trust in government (α = .87), media (α = .86), and information from the scientific community (α = .76).
Centrality of religiosity
Participants completed the 13-item Centrality of Religiosity Scale (CRS; Huber and Huber, 2012), which asked them to report their perceived importance of five core dimensions of religiosity: public practice, private practice, religious experience, ideology and intellectual. Responses could range from 1 (not at all/never) to 5 (very much so/very often). Higher mean scores indicated greater levels of overall religiosity (α = .89). The full measures used in this study are provided in the Supplemental Material.
Results
Vaccination intentions across demographics
Preliminary analyses assessing vaccine intent as a function of participant demographics indicated that intentions for COVID-19 vaccination did not significantly differ as a function of sex, t(279) = −.851 p = .395, race, t(282) = .509, p = .579, age (r = −.03, p = .607), education (r = −.06, p = .339) or income (r = .13, p = .072). However, an analysis of variance (ANOVA) assessing COVID-19 vaccine intent as a function of (non)religious group revealed a significant effect, F(3,281) = 5.24, p = .002, η2 = .053. 4 As seen in Table 1, this was driven by participants who self-identified as belonging to a range of religions that represent ‘Minorities’ in Canada, who were less likely to be vaccinated than Atheists/Agnostics (p < .001), and those who identified as Spiritual (p = .019). Christians were also less likely than Atheists/Agnostics (p = .004) to be vaccinated. Nonetheless, at least 75% of all participants reported the intent to be vaccinated for COVID-19, regardless of (non)religious group membership.
Religiosity, trust and vaccine intentions (Means, SDs) as a function of (non)religious group (Study 1).
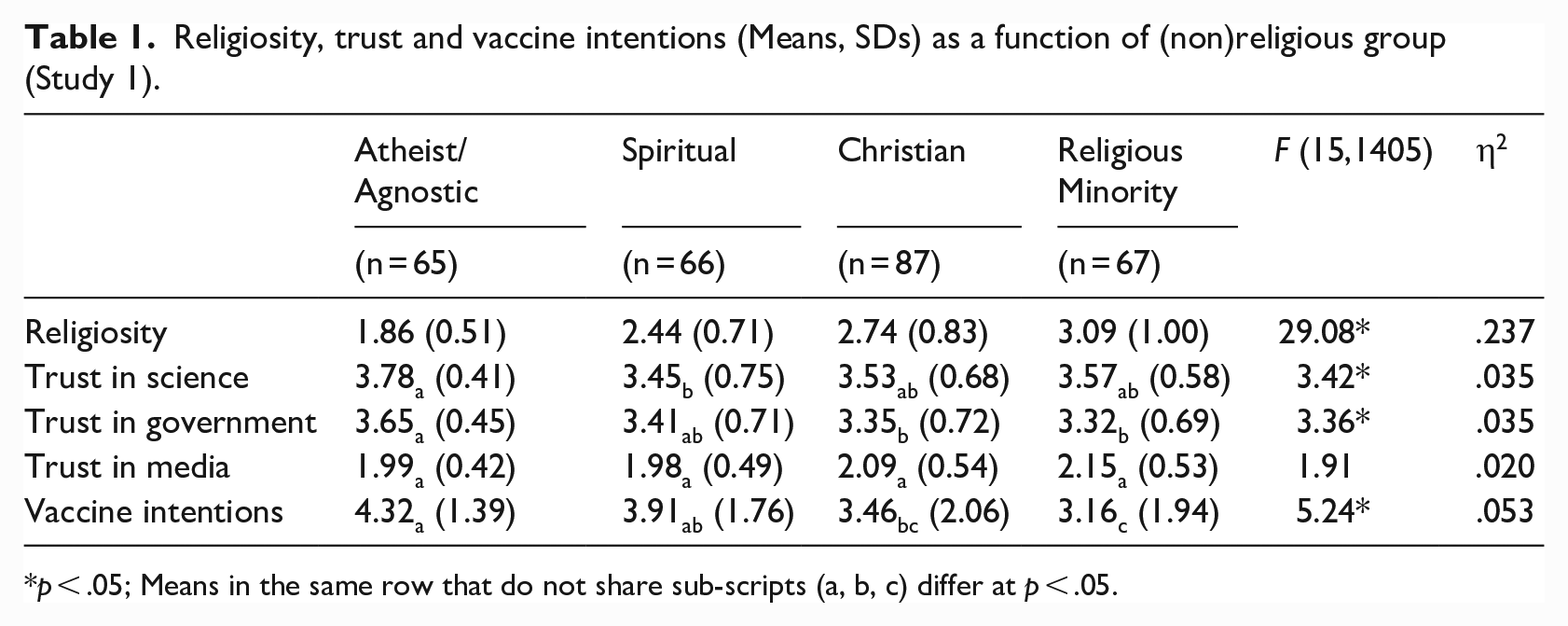
p < .05; Means in the same row that do not share sub-scripts (a, b, c) differ at p < .05.
Trust across (non)religious groups
A multivariate analysis of variance (MANOVA) assessed (a lack of) trust – in government, media, and information from the scientific community – across (non)religious groups. This analysis revealed a significant multivariate effect, Pillai’s = 0.108; F(9,843) = 3.51, p < .001, η2 = .036, which was attributable to differences across the (non)religious groups regarding trust in information from the scientific community, F(3, 281) = 3.42, p = .018, η2 = .035, as well as trust in government, F(3,281) = 3.36, p = .019, η2 = .035. 5 As seen in Table 1, in comparison to Atheists/Agnostics, those who identified as Spiritual reported less trust in information from the scientific community (p = .016), whereas religious ‘Minorities’ (p = .030) and Christians (p = .041) reported less trust in government compared to Atheists/Agnostics.
Religiosity across (non)religious groups
To confirm that individuals’ self-reported religiosity reflected their (non)religious group membership as anticipated, an ANOVA assessed overall religiosity across the groups, which revealed a significant effect, F(3,281) = 29.08, p < .001, η2 = .237. 6 As seen in Table 1, Atheists/Agnostics reported the lowest levels of religiosity, followed by Spirituals, Christians and religious ‘Minorities’.
Relations among religiosity, trust and vaccination intentions
As seen in Table 2, religiosity was significantly, negatively associated with intentions to be vaccinated for COVID-19. Likewise, religiosity was significantly, negatively associated with trust in government (and marginally, positively associated with trust in media). Not surprisingly, trust in government, media and information from the scientific community were all significantly, positively inter-related to each other and to vaccination intentions.
Means, standard deviations and correlations among religiosity, trust and vaccine intentions (Study 1).
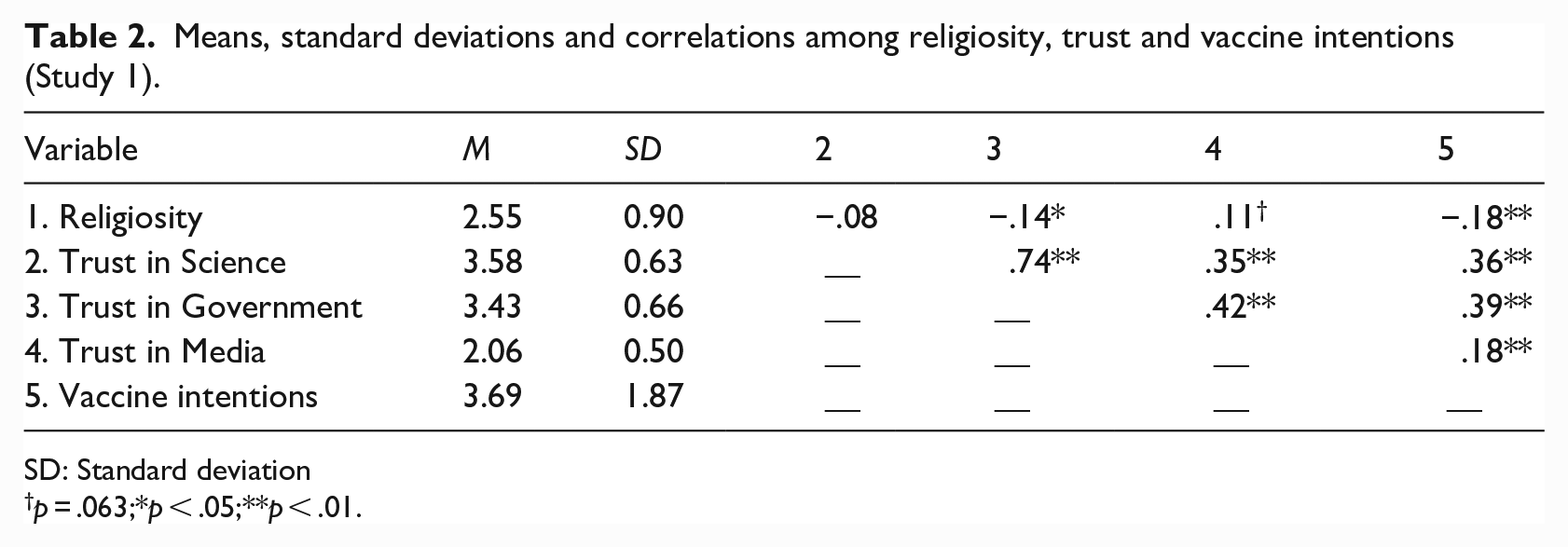
SD: Standard deviation
p = .063;*p < .05;**p < .01.
Mediating role of trust
When the potential mediating roles of trust in government, media and information from the scientific community were assessed in the relation between overall religiosity and vaccination intentions, the direct relation (c path; Hayes, 2022), B = −.37, SE = .12, p = .002, remained significant (c’ path), B = −.30, SE = .12, p = .010. Indeed, the 95% CIs for the potential mediated paths through trust each included zero, indicating that neither trust in information from the scientific community, government, nor media accounted for the (negative) relation between religiosity and vaccination intentions in our student sample.
In summary, several significant differences were apparent across (non)religious groups in vaccination intentions and trust. Most notably, religious individuals (i.e. Christians and religious ‘Minorities’) reported more hesitancy to be vaccinated against COVID-19 and less trust in government, while those who identified as Spiritual reported less trust in information from the scientific community than did Atheists/Agnostics (see Table 1). However, trust in government, media or information from the scientific community did not account for the relationship between religiosity and vaccination hesitancy.
Study 2
Study 2 expanded on Study 1 by conducting an online survey with a nationwide community sample to better represent the Canadian population. These data were collected between March and June 2021, one full year into the pandemic. Several measures assessing additional factors that may be implicated in vaccine hesitancy were incorporated in Study 2, including political orientation (Choma et al., 2009), religion–science compatibility beliefs (Rios and Aveyard, 2019), and a more comprehensive measure of trust in science – assessing trust in the scientific community, government and media (Nisbet et al., 2015). In addition, given evidence that Atheists and Agnostics may respond differently in a variety of contexts (Schnell et al., 2021), these two non-religious groups were analysed separately in Study 2.
Method
Participants and procedure
A total of 280 Canadian community participants (137 females, 142 males, 1 other; 18–72 years, M = 37.35, SD = 11.19) were recruited from Amazon Mechanical Turk (MTurk). This sample size provided 95% power to detect medium effect sizes (two-tailed; Erdfelder et al., 2009) (see Note 1). Although 392 responses were initially collected, 112 participants were removed due to incomplete or invalid data (see Note 2). Participants’ (non)religious affiliations included Atheists (n = 69), Agnostics (n = 45), Spirituals (n = 53), Christians (n = 69) and participants who self-identified as belonging to a range of religions that represent ‘Minorities’ in Canada (i.e. Muslim, Jewish, Baha’i, Buddhist, Hindu, Sikh; n = 44). As in Study 1, participants also reported other demographic information including race (‘white’, n = 174; racial ‘Minorities’, n = 106), education and annual household income. Our sample varied only slightly from the Canadian population in terms of sex and age (49.7% male, 50.3% female, mean age 41.7 years; Government of Canada, 2021). Racial and religious ‘Minorities’ as well as non-religious participants were oversampled in the current study compared to national averages (Government of Canada, 2022; Statistics Canada, 2021) to provide sufficient sample sizes for group comparison.
Measures
Vaccine hesitancy
The assessment of vaccination likelihood was modified slightly from Study 1 to reflect the partially vaccinated population at the time of data collection in Study 2. A new variable was created to encompass participants’ vaccination status including those who indicated they would never get vaccinated for COVID-19 (coded as 0) and those who were already vaccinated (coded as 6).
Political orientation
In Study 2, participants were asked to self-report their political orientation (Choma et al., 2009), ranging from 1 (extremely liberal) to 9 (extremely conservative).
Religion–science compatibility
To assess the extent to which participants perceived that religion and science were compatible, participants answered a four-item questionnaire (Rios and Aveyard, 2019). Responses could range from 1 (completely incompatible/impossible) to 7 (completely compatible/possible). Higher mean scores indicated greater religion–science compatibility beliefs (α = .85).
Trust in science, government and media
To assess trust in the scientific community, participants indicated their agreement with five statements (see Supplemental Material; Nisbet et al., 2015; α = .84), ranging from 1 (strongly disagree) to 5 (strongly agree). Participants were also asked to rate those five statements modified to assess trust in government (α = .88) 7 and media (α = .90). Items were reverse coded as needed and mean scores were computed.
Results
Vaccination intentions across demographics
Analyses assessing vaccine intent as a function of participant demographics indicated that intentions for COVID-19 vaccination did not significantly differ as a function of sex, t(277) = 0.22 p = .826, age (r = .06, p = .309), education (r = .10, p = .094) or income (r = −.01, p = .820). However, in contrast to Study 1, a significant difference emerged as a function of race, t(276) = −2.52, p = .012. Specifically, participants who self-identified as ‘white’ (M = 4.26, SD = 2.03) were less likely to get vaccinated compared to racial ‘Minorities’ (M = 4.82, SD = 1.33).
Consistent with Study 1, an ANOVA assessing how likely individuals were to get vaccinated as a function of (non)religious group was significant, F(4,275) = 3.66, p = .006, η2 = .051. As seen in Table 3, this was driven by Spiritual participants being less likely to get vaccinated than Atheists (p = .014), Agnostics (p = .009), Christians (p = .034) and ‘Minorities’ (p < .001). 8 Despite these group differences, at least 60% of all participants in Study 2 reported the intent to be vaccinated for COVID-19 regardless of (non)religious group membership, and approximately 25% of this sample reported that they had already been vaccinated.
Religiosity, religion–science compatibility, political orientation, trust and vaccine intentions (Means, SDs) as a function of (non)religious group (Study 2).
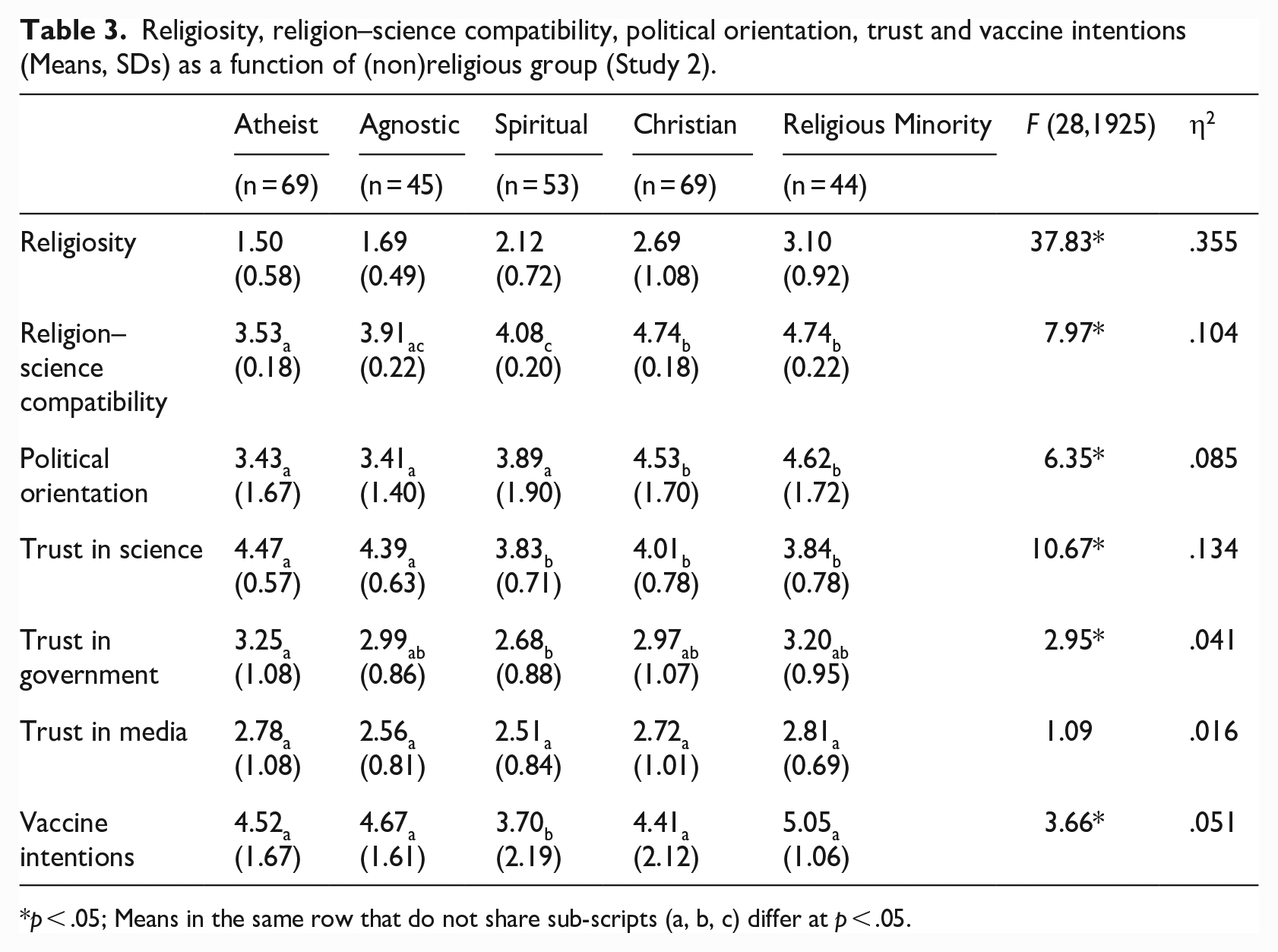
p < .05; Means in the same row that do not share sub-scripts (a, b, c) differ at p < .05.
Differences across (non)religious groups
Political orientation
An ANOVA to assess political orientation as a function of (non)religious group was significant, F(4,275) = 6.35, p < .001, η2 = .085. As seen in Table 3, religious ‘Minorities’ and Christians reported the most conservative political orientation, which was significantly higher than that reported by Atheists (ps < .001), Agnostics (ps < .001) and Spirituals (p = .04). 9
Religion–science compatibility
An ANOVA to assess perceptions of religion–science compatibility as a function of (non)religious group was also significant, F(4,275) = 7.97, p < .001, η2 = .104, which was primarily attributable to Atheist and Agnostic beliefs that religion and science are less compatible compared to religious and Spiritual group members (see Table 3). Specifically, Atheists reported that religion and science were less compatible compared to Christians (p < .001), religious ‘Minorities’ (p < .001) and Spirituals (p = .041), whereas Agnostics reported less compatibility than Christians (p = .003) and ‘Minorities’ (p = .008). Spirituals also reported lower levels of compatibility compared to Christians (p = .014), and ‘Minority’ group members (p = .029).
Trust in science, government and media
A MANOVA assessed participants’ trust in the scientific community, government, and media. This analysis revealed a significant multivariate effect, Pillai’s = .183; F(12,825) = 4.460, p < .001, η2 = .061, due to differences across (non)religious groups in their (lack of) trust in the scientific community, F(4,275) = 10.67, p < .001, η2 = .134, and government, F(4,275) = 2.95, p = .021, η2 = .041, but not media, F(4,275) = 1.09, p = .361, η2 = .016. As seen in Table 3, Spirituals (ps < .001), Christians (p = .001; p = .045) and religious ‘Minorities’ (p < .001; p = .002) lacked trust in the scientific community compared to Atheists and Agnostics. Spirituals also reported lower levels of trust in government compared to Atheists (p = .016).
Religiosity
Finally, participants’ self-reported religiosity mapped onto their (non)religious group identification, F(4,275) = 37.83, p < .001, η2 = .355. As anticipated, Atheists again reported the lowest levels of religiosity, followed by Agnostics, Spirituals, Christians and religious ‘Minorities’ (Table 3).
Relations among religiosity, political orientation, trust and vaccination intentions
As seen in Table 4, greater religiosity, religion–science compatibility and more conservative political orientation were all positively related. In contrast to Study 1, greater religiosity was also significantly associated with a lack of trust in the scientific community (but not the government or media) and was unrelated to vaccination intent. Interestingly, religion–science compatibility beliefs were also associated with less trust in the scientific community (but not in government or media). Finally, a more conservative political orientation was associated with lower vaccination intentions as well as less trust in the scientific community, government and media. As in Study 1, trust in the scientific community, government and media were associated with a greater intent to be vaccinated.
Means, standard deviations and correlations among religiosity, trust and vaccine intentions (Study 2).
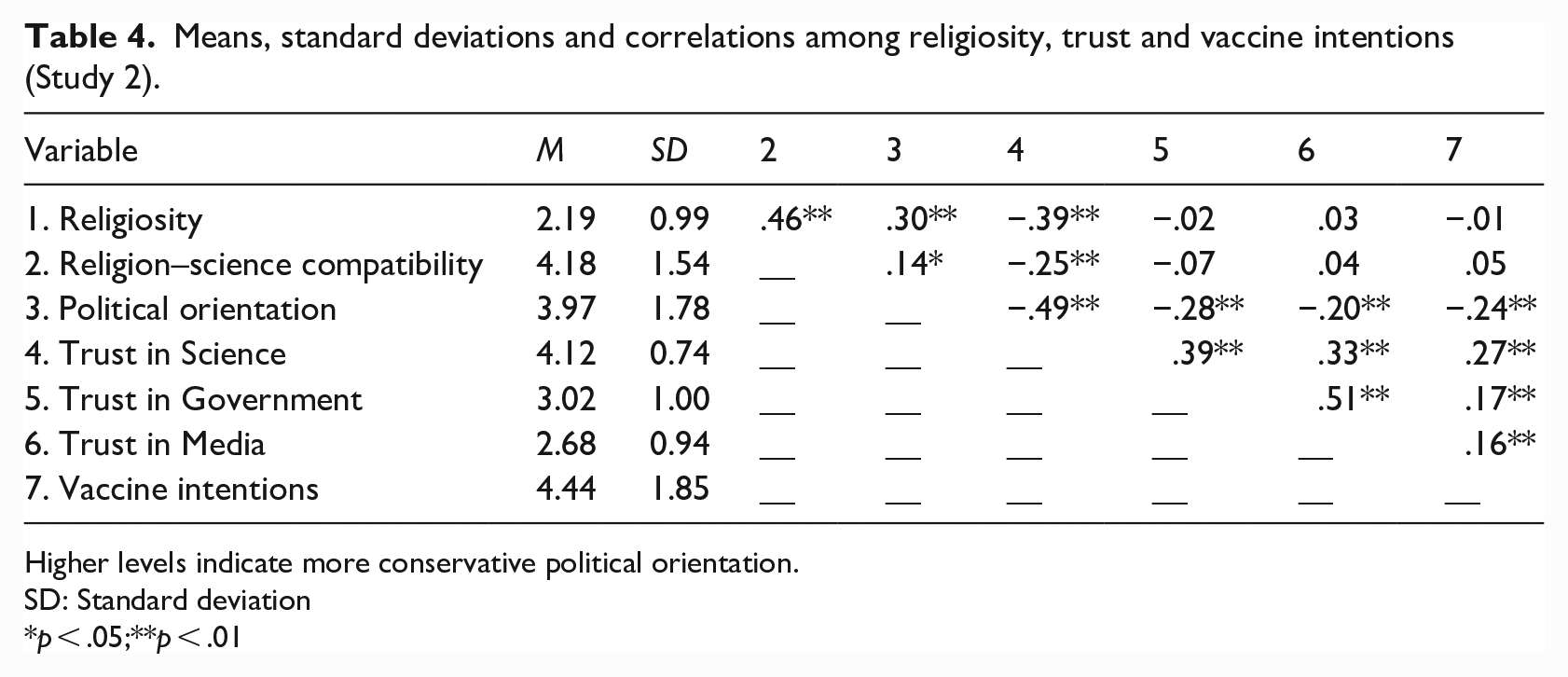
Higher levels indicate more conservative political orientation.
SD: Standard deviation
p < .05;**p < .01
Mediating role of trust
Given the significant relations outlined, the mediating role of trust was examined in the relations between vaccine intent and each of religiosity, religion–science compatibility and political orientation as potential predictors.
When the mediating roles of trust in the scientific community, government, and media were assessed in the relation between religiosity and vaccination intentions, the (non-significant) direct relation (c path; Hayes, 2022), B = −.02, SE = .11, p = .884, remained non-significant (c’ path), B = .19, SE = .12, p = .118. However, the 95% CI for the mediated path through trust in the scientific community did not include zero (B = −.20, SE = .06; 95% CIs: −.33, −.09), indicating that religiosity and vaccination intentions were indirectly linked through a lack of trust in the scientific community.
When the mediating roles of trust in the scientific community, government, and media were assessed in the relation between religion–science compatibility and vaccination intentions, the (non-significant) direct relation (c path; Hayes, 2022), B = .06, SE = .07, p = .393, became significant (c’ path), B = .15, SE = .07, p = .044. Moreover, the 95% CI for the mediated path through trust in the scientific community did not include zero (B = −.08, SE = .03; 95% CIs: −.14, −.03), indicating that religion–science compatibility and vaccination intentions were indirectly linked through a lack of trust in the scientific community through a suppression effect (i.e. failing to account for trust in the scientific community ‘suppressed’ the relation between religion–science compatibility and vaccination intentions; Agler and De Boeck, 2017).
Finally, when the mediating roles of trust in the scientific community, government and media were assessed in the relation between political orientation and vaccination intentions, the direct relation (c path; Hayes, 2022), B = −.25, SE = .06, p < .001, remained significant (c’ path), B = −.14, SE = .07, p = .040. However, the 95% CI for the mediated path through trust in the scientific community did not include zero (B = −.09, SE = .04; 95% CIs: −.17, −.01), indicating that political orientation and vaccination intentions were partially mediated through a lack of trust in the scientific community.
General discussion
In two studies, vaccine hesitancy was linked to a lack of trust in scientific information or the scientific community more broadly, which was tied to (non)religious group identity and beliefs as well as political orientation (Study 2). The results of both studies revealed differences in vaccine intentions across (non)religious groups. In Study 1 (university student sample), religious ‘Minority’ and Christian participants were the least likely to report the intent to be vaccinated for COVID-19 (compared to Atheists and Agnostics), and within a community sample (Study 2) vaccine hesitancy was greatest among Spirituals. The link between religiosity and lower vaccine intentions was not unexpected given that greater religiosity has been associated with less favourable views towards scientific innovations (McPhetres and Zuckerman, 2018) and spirituality has been linked to greater vaccine hesitancy (Rutjens et al., 2022). Although vaccination does not directly conflict with most religious teachings, there is some evidence that objections towards vaccination may be driven by concerns about morality and ‘playing God’, perceived misalignment with religious doctrine, or misinformed religious leadership (Pelčić et al., 2016). This said, religiosity and vaccine intent were not directly related in Study 2, mirroring other recent research suggesting inconsistent links between religion and vaccine hesitancy (Williams et al., 2021).
In evaluating the ties between religion and vaccine hesitancy, it should be considered that features of the pandemic stressor itself might have affected religious beliefs. Earlier research has indicated that religious coping may have been negatively influenced given the inability to participate in in-person religious practices owing to social distancing and isolation measures (DeRossett et al., 2021). Some individuals may have even become angry at God for the negative consequences of the pandemic, just as this has been observed under other uncontrollable stressful conditions (Exline et al., 2011). Conversely, amid troubling times, other individuals may have felt the need to trust that God would provide hope and that the situation would pass (Edara et al., 2021). In fact, religious belief may serve a variety of functions including the need to cope with mortality (Rababa et al., 2021), the search for meaning in times of uncertainty (Park, 2007), and motivations to affiliate with stable and trustworthy figures (Kay et al., 2010). Thus, in the face of a threat such as the COVID-19 pandemic, an individual may turn to religion as a means of coping with the situation in addition to – or instead of – trusting in science.
The role of trust in science
The results of both studies revealed that greater trust in science, government and media were linked with greater intentions to be vaccinated for COVID-19. Conversely, religiosity was associated with less trust in government (Study 1) and less trust in the scientific community (Study 2). These findings are in line with research suggesting that religion may empower feelings of epistemic personal control, which could lead to a decreased need to trust in authority (Kay et al., 2010). Despite religiosity and vaccine intent not being directly related (Study 2), trust in the scientific community indirectly linked religiosity with vaccine intentions. Although religion and science are not necessarily incompatible, holding strong religious beliefs (e.g., beliefs in an “engaged God”) appear to be at odds with trust in science (Upenieks et al., 2022), thereby furthering the religion–science compatibility debate (Leicht et al., 2021; Rios and Aveyard, 2019). While there is no single universally held view of the relationship between science and religion, there may be a lack of trust in scientific claims that are perceived to contradict theological accounts or authorities (Evans, 2011; Pelčić et al., 2016), which may have implications for the connections between religion, trust in science and subsequent adoption of positive health behaviours.
Trust in the scientific community also mediated the (non-significant) relationship between religion–science compatibility and vaccine intent. In this case, however, it appeared that failing to account for trust in the scientific community ‘suppressed’ the relation between religion–science compatibility and vaccination intentions, given that this relation became significant only when trust in the scientific community was considered (Agler and De Boeck, 2017; Agley et al., 2021). Finally, although political orientation and vaccination intentions were directly related, trust in the scientific community also partially mediated this positive relationship. Thus, conservative political ideology appeared to be an independent predictor of reduced vaccine uptake as well as trust in science (Latkin et al., 2022; McLamore et al., 2022).
Overall, trust in the scientific community played a significant role in linking vaccine intentions with religiosity, as well as with religion–science compatibility and political orientation. However, the links between these orientations and vaccination intent may have been undermined and trust may have wavered as a function of one’s religious and/or political ideology. In addition, the combination of rapid vaccine development, the social urgency for uptake, and the abundance of misinformation could have contributed to low levels of trust in science and thus fostered hesitancy to be vaccinated against COVID-19 in some religious groups (Beauchamp and Rios, 2020; Van Bavel et al., 2020). Accordingly, the role of trust in science in this investigation must be viewed alongside other influential factors, including political orientation.
Religious or political ideology?
Earlier research has indicated that political orientation may have an impact on vaccine intentions (Albrecht, 2022; Baumgaertner et al., 2018), alongside the overlap between religiosity and political beliefs (Forbes and Zampelli, 2013). In the present Canadian investigation, more conservative political orientation was positively associated with religiosity and religion–science compatibility, in addition to lower intentions to be vaccinated, as well as less trust in the scientific community, government and media. While trust in the scientific community partially mediated the relation between political orientation and vaccine intent, high political conservatism was also directly associated with a reduced inclination to get vaccinated. As such, political ideology may have played an even stronger role than religiosity in relation to vaccine intent.
The COVID-19 pandemic has been a confusing time for individuals as the situation has constantly evolved, with political and public health messaging often inconsistent, and not always in line with or supported by science (Dudley et al., 2021). In addition, mandated vaccine requirements have created an added layer to the complexity of the pandemic and to trust in government, science and media. In fact, religious messaging has sometimes been conflated with political motivations as frequently seen in anti-mandate protests worldwide. The parallel between religious and political ideology may be due to the desire to minimize threats in times of uncertainty (Bonanno and Jost, 2006). To be sure, belief in religious and political worldviews can also substitute for one another based on the level of perceived external control that each ideology provides (Kay et al., 2010), and in the present study, the ties to political ideology may have been (in at least some cases) confounded with religion.
Implications for public health
The COVID-19 pandemic has highlighted and amplified many long-standing inequities concerning health systems within and across countries (Gravlee, 2020). The present research was broadly designed to examine whether public health messages throughout the pandemic would be differentially interpreted (and trusted) by a range of (non)religious groups. In light of the differences in vaccination intentions across religious and non-religious groups, tailoring public health messages in ways that acknowledge diversity – including diversity of religious (non)belief – ought to be considered. Considering the ideological overlap between religiosity and political orientation (Forbes and Zampelli, 2013), it may likewise be important to consider the corresponding links with health behaviours, including vaccination intent. Finally, the results from this research suggest that many of these links to vaccination intentions may be dependent on trust in science. Efforts to slow the spread of the virus more effectively should better acknowledge group-level factors that may influence trust in science and subsequent health behaviours. Further research in the social sciences on the distrust of authorities and science (Liu et al., 2022; Van Bavel et al., 2020), and their links to vaccination hesitancy is required.
Limitations
As much as religion was linked to trust and vaccine hesitancy, the correlational nature of the studies precluded causal interpretations of the results. In addition, although it would have been ideal to assess responses from a broader array of religious groups, small sample sizes from the range of groups that are typically considered to be ‘Minorities’ in Canada precluded this possibility. Pooling data from religious groups might have obscured important differences between some of these groups themselves. Moreover, slightly different operationalizations of trust in science across the studies (i.e. information from the scientific community in Study 1 versus the scientific community in Study 2) could have impacted our results. Furthermore, the data for the two studies were collected at different time points during the COVID-19 pandemic. This may have been critical given that knowledge of the vaccine varied over time and vaccine uptake became more widely available. Collecting longitudinal data to better represent the ongoing and evolving nature of the COVID-19 pandemic and continuing vaccinations would have been desirable. This is essential considering that ideology can vary, especially in times of extreme uncertainty (Engstrom and Laurin, 2020).
Several other factors could also account for the somewhat divergent results observed in the two studies. As shared social identity may drive group behaviour through collective coordination of social perception and action (Haslam et al., 2000), in Study 2, Spiritual individuals may have been more vaccine hesitant due to group norms rather than explicit religious group discouragement. It is conceivable as well that in Study 1, the novelty of a new vaccine coupled with mixed messaging from religious leaders early in the pandemic may have prompted some religious individuals to be wary of vaccination efforts. When the second study was undertaken, the benefits of novel vaccines were likely better understood and 25% of the test sample had been vaccinated, which may have manifested in the between-study differences that were observed.
The age differences between our two study samples (i.e. university students; M = 20.78, SD = 4.98, versus community members; M = 37.35, SD = 11.19) could also have accounted for some of the variation in the relationship between religiosity and vaccine intentions, as religiosity often increases with age (Bengtson et al., 2015; Malone and Dadswell, 2018). Moreover, the COVID-19 pandemic exacerbated feelings of death anxiety for many individuals, especially among older adults considering the dramatic increase in their morbidity and mortality rates (Rababa et al., 2021). As well, the student participants consisted of over 80% females. This uneven gender distribution could have impacted our results in Study 1 given that previous research revealed gender differences in religiosity, with women typically being more religious (Li and Graham, 2017). Nonetheless, no gender differences emerged in our analyses. Moreover, our community sample allowed us to provide a more generalizable portrait of the Canadian population, even if the sample size was somewhat limited and perhaps not entirely representative.
Conclusion
Taken together, this research is a step towards understanding vaccination intentions and reluctance in multicultural Canadian samples, with a particular focus on religious diversity. Our findings indicated that vaccination intentions differed across religious and non-religious groups, which was linked to a lack of trust in science. However, our results also showed strong links between political orientation and both trust in science and vaccine intent. Moving forward, it would be advantageous to account for a variety of social factors in assessing vaccine hesitancy, including both political and religious group membership. In this way, our research has implications for informing urgent public health initiatives and knowledge mobilization strategies for relaying scientific findings to the public, as well as potentially encouraging vaccine uptake in targeted and culturally appropriate ways during the COVID-19 pandemic and beyond.
Supplemental Material
sj-pdf-1-pus-10.1177_09636625231174845 – Supplemental material for Believing in science: Linking religious beliefs and identity with vaccination intentions and trust in science during the COVID-19 pandemic
Supplemental material, sj-pdf-1-pus-10.1177_09636625231174845 for Believing in science: Linking religious beliefs and identity with vaccination intentions and trust in science during the COVID-19 pandemic by Emily Tippins, Renate Ysseldyk, Claire Peneycad and Hymie Anisman in Public Understanding of Science
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Ontario Graduate Scholarship (OGS) Program, the Carleton University I-CUREUS Program, and the Carleton University Department of Health Sciences..
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.