
Abstract
Restricted cubic splines (RCS) allow analysts to model nonlinear relations between continuous covariates and the outcome in a regression model. When using RCS with the Cox proportional hazards model, there is no longer a single hazard ratio for the continuous variable. Instead, the hazard ratio depends on the values of the covariate for the two individuals being compared. Thus, using age as an example, when one assumes a linear relation between age and the log-hazard of the outcome there is a single hazard ratio comparing any two individuals whose age differs by 1 year. However, when allowing for a nonlinear relation between age and the log-hazard of the outcome, the hazard ratio comparing the hazard of the outcome between a 31- and a 30-year-old may differ from the hazard ratio comparing the hazard of the outcome between an 81- and an 80-year-old. We describe four methods to describe graphically the relation between a continuous variable and the outcome when using RCS with a Cox model. These graphical methods are based on plots of relative hazard ratios, cumulative incidence, hazards, and cumulative hazards against the continuous variable. Using a case study of patients presenting to hospital with heart failure and a series of mathematical derivations, we illustrate that the four methods will produce qualitatively similar conclusions about the nature of the relation between a continuous variable and the outcome. Use of these methods will allow for an intuitive communication of the nature of the relation between the variable and the outcome.
Introduction
The use of the Cox proportional hazards model is ubiquitous in clinical and epidemiological research.
1
The Cox model relates the logarithm of the hazard function to a linear combination of explanatory variables (or functions derived from the explanatory variables such as higher-order terms or interactions):
When the Cox model assumes a linear relation between a given continuous covariate (e.g. age) and the log-hazard of the outcome then there is a single hazard ratio comparing any two individuals whose value of the given continuous variable differs by one unit. Thus, using the example of age, the hazard ratio comparing the hazard of the outcome between a 31- and a 30-year-old is the same as the hazard ratio comparing the hazard of the outcome between an 81- and an 80-year-old. While assuming a linear relation between a continuous variable and the log-hazard of the outcome results in an easily interpretable uniform hazard ratio, the assumption of linearity has been criticized by several authors.2–4 In many clinical and epidemiological settings, the assumption of linearity may not be realistic. Different methods, including restricted cubic splines (RCS) and fractional polynomials, have been proposed to allow for the modeling of nonlinear relations between a continuous covariate and the outcome in a regression model.2,4
An advantage to allowing for nonlinear relations between a continuous variable and the log-hazard of the outcome in a Cox model is that the assumption of linearity may be unrealistic in some settings. Thus, incorporating nonlinear relations may result in a regression model that more accurately describes the relation between covariates and the hazard of the outcome. A potential disadvantage to allowing for a nonlinear relation is that it becomes more difficult to describe the nature of relation between the given continuous predictor variable and the log-hazard of the outcome.
The objective of the current paper is to explore different graphical methods for describing the relation between a continuous variable and a time-to-event outcome when using restricted cubic splines with a Cox proportional hazards model to model the relation. The methods described in this article assume that preliminary analyses have led the analyst to allow for a nonlinear relationship between a continuous covariate and the log-hazard of the outcome. The presented methods will allow for communicating the nature of the relationship between the continuous covariate and the outcome. The article is structured as follows: in section 2, we propose four graphical methods to describe the relation between a continuous predictor variable and the outcome when using RCS with a Cox regression model. In section 3, we illustrate the application of these methods using data on patients hospitalized with heart failure (HF). In section 4, we present the results of mathematical derivations motivated by the findings of our case study. Finally, in section 5, we summarize our findings and present them in the context of the existing literature.
Graphical methods for illustrating relations between a continuous variable and outcomes when using restricted cubic splines with a Cox regression model
Restricted cubic splines
Restricted cubic splines require the specification of k knots. Harrell suggests that the knots be placed at equidistant percentiles of the continuous variable (thus, with four knots, one would place the knots at the 5th, 35th, 65th, and 95th percentiles of the continuous variable). 2 RCS allows for a smooth nonlinear curve that is linear in the tails (to the left of the first knot and to the right of the last knot) and that is a cubic polynomial between adjacent knots such that the function is continuous and smooth at the knots where two cubic polynomials meet. An RCS with k knots requires the specification of k−1 variables that are themselves functions of the given continuous variable and the knots, with one of the variables being equal to the original continuous variable. These k−1 variables are then entered as explanatory or independent variables in a regression model.
Notation and background on survival analysis
Let T denote the event time. The hazard function, which is a function of time (denoted by t), is defined as:

The Cox proportional hazards model relates the logarithm of the hazard function to a linear combination of explanatory variables:


We describe four graphical methods for illustrating the relation between a continuous covariate and the outcome when using a Cox regression model with RCS. For the sake of simplifying the mathematical expressions, we assume that the model contains a single continuous variable and that this variable is modeled using RCS. The four methods are easily generalizable to multivariable models.
First, one can select a given value of the continuous covariate as the reference level. Candidates include the minimum value of the continuous variable or the mean or median value. In the case study below this will be the minimum value or the average value, depending on the variable. We denote this quantity by
Second, one can estimate the cumulative incidence function at a clinically meaningful value of t, denoted as
Third, one can compute the instantaneous hazard of the outcome at each value of
The fourth approach is similar to the third, but one computes and plots the cumulative hazard function rather than the instantaneous hazard function. As with the second and third methods, one needs to decide on the values of the other variables at which the cumulative hazard function is calculated.
Case study
Data
We used data from a previous study that used 12,705 adults who presented to hospital emergency departments (EDs) in Ontario, Canada with a primary diagnosis of HF. 8 The study outcome for this case study was time to all-cause mortality, with subjects being followed for up to 2 years after ED presentation. Subjects were censored after 2 years if death had not yet occurred. Of the 12,705 patients, 35.4% died within 2 years of ED presentation.
Statistical analyses
We fit a Cox regression model in which the hazard of death was regressed on the following variables measured at the time of ED presentation: age, systolic blood pressure, heart rate, oxygen saturation, serum creatinine, serum potassium, sex, transport to hospital by emergency medical services, use of metolazone, previous myocardial infarction, previous heart failure, coronary artery bypass graft surgery, percutaneous coronary intervention, diabetes mellitus, hypertension, active and metastatic cancer, unstable angina, stroke, functional disability, cardiopulmonary respiratory failure and shock, pneumonia, chronic obstructive pulmonary disease, protein calorie malnutrition, dementia, trauma, major psychiatric disorders, peripheral vascular disease, renal failure, chronic liver disease, chronic atherosclerotic disease, and valvular disease. The first five variables were continuous, serum potassium was a three-level categorical variable, while the remaining variables were dichotomous. In the regression model, we used RCS to model the relation between the log-hazard of death and age, systolic blood pressure, heart rate, and creatinine. For age and creatinine, we used five knots, for systolic blood pressure we used four knots, and for heart rate we used three knots. Knots were placed at equidistant percentiles of the given variable, as suggested by Harrell. 2 When we used fewer than five knots, the decision to do so was influenced by the distribution of the given variable: in these instances, some of the recommended percentiles coincided.
To illustrate the methods described in section 2, we focused on four continuous variables: age, systolic blood pressure, heart rate, and creatinine. For each of these four variables, we used the four methods described in section 2 to illustrate graphically the nature of the relation between the continuous variable and mortality. For the first method that requires a reference value of the given variable for the calculation of hazard ratios, we used the minimum observed value for age and heart rate (the minimums were 20 years and 80 beats per minute, respectively). For systolic blood pressure and creatinine, the minimums were 0 and 0.000226, respectively. As these values are not clinically plausible for living patients, we used the sample mean as the reference value for these two variables (the sample means of systolic blood pressure and creatinine were 141 and 1.16, respectively). For the second through fourth methods that require the specification of a time at which to estimate the cumulative incidence function, the hazard function, or the cumulative hazard function, we specified that
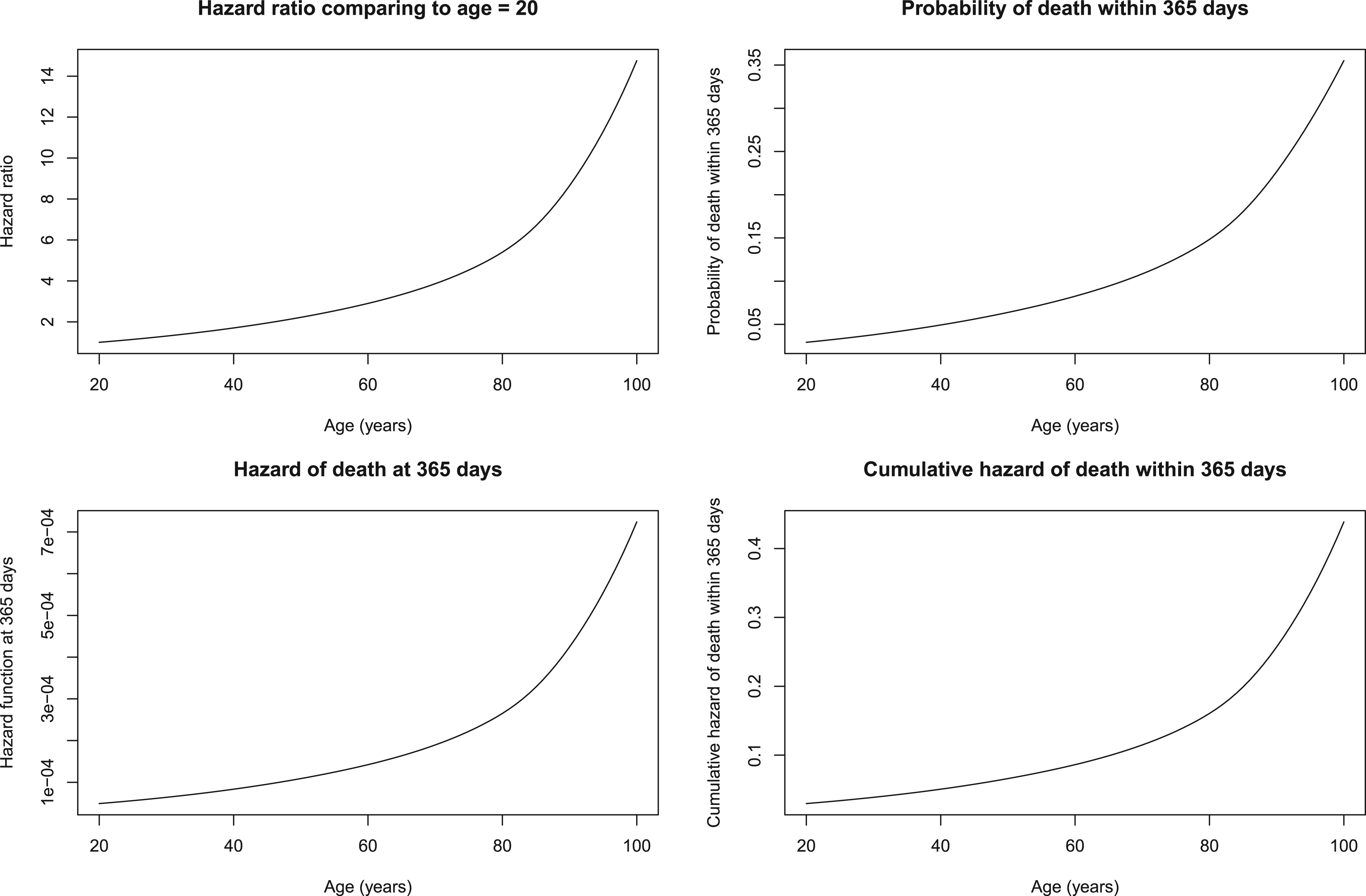
Relationship between age and mortality.
The relation between age and mortality is described in Figure 1, which consists of four panels, one for each of the graphical methods described in section 2. The shape of the curve was qualitatively similar across the four panels. In each of the four panels one observes an initial gradual increase in the “risk” of death with increasing age. However, from approximately age 80 onwards, there is a larger increase in “risk” of death with increasing age. Note that we use the term “risk” in a generic and nontechnical sense, thereby allowing us to describe all four panels simultaneously. “Risk”’ can be interpreted, depending on the setting, as the relative hazard of death, the probability of death within 1 year, the instantaneous hazard of death at 1 year, or the cumulative hazard of death within 1 year.
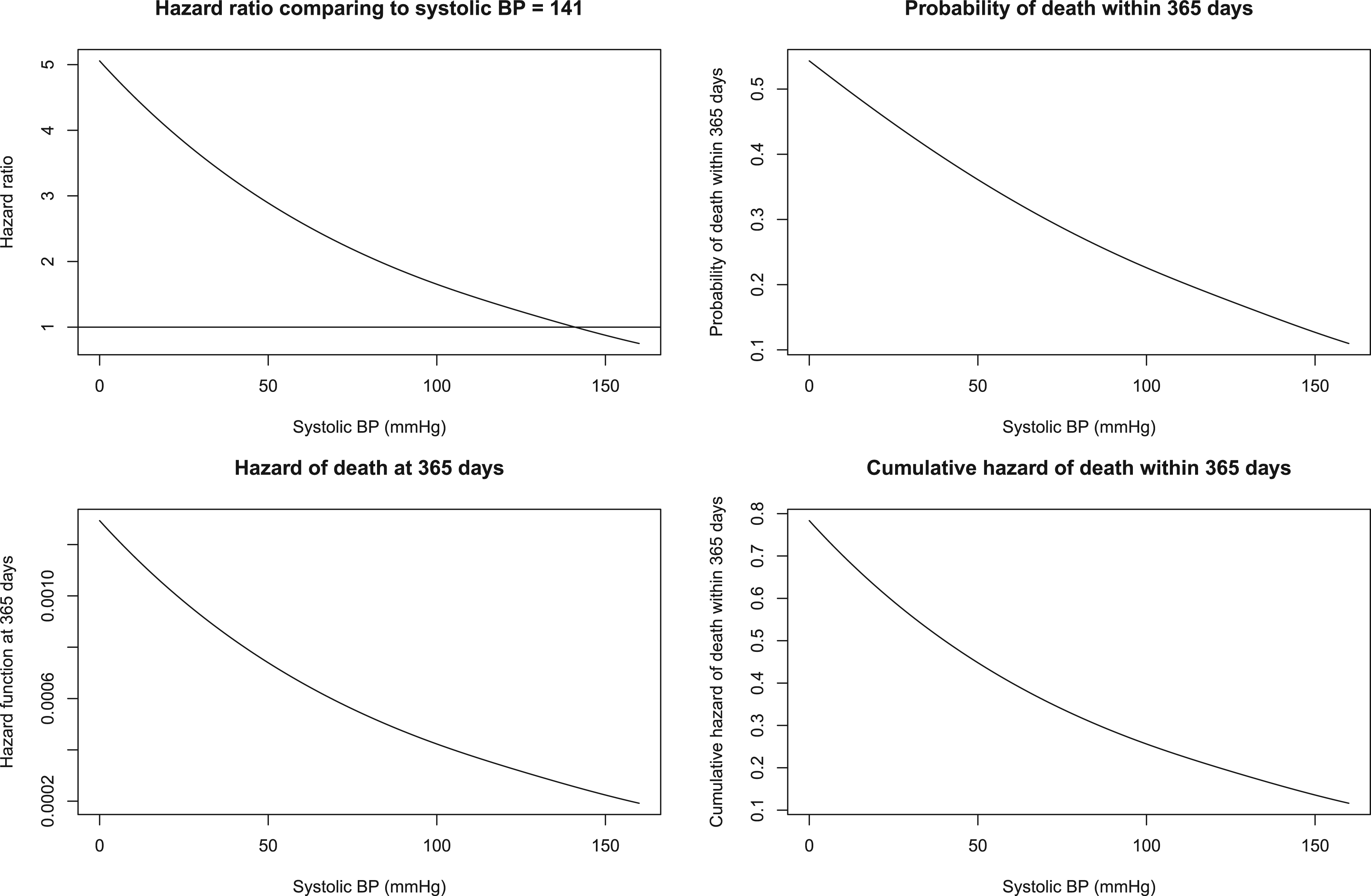
Relationship between systolic blood pressure and mortality.
The relation between systolic blood pressure and mortality is described in Figure 2. As with age, the shape of the curve is qualitatively similar across the four methods. In each panel we observe that the “risk” of death decreases with increasing blood pressure. Furthermore, the relation with blood pressure is approximately linear.
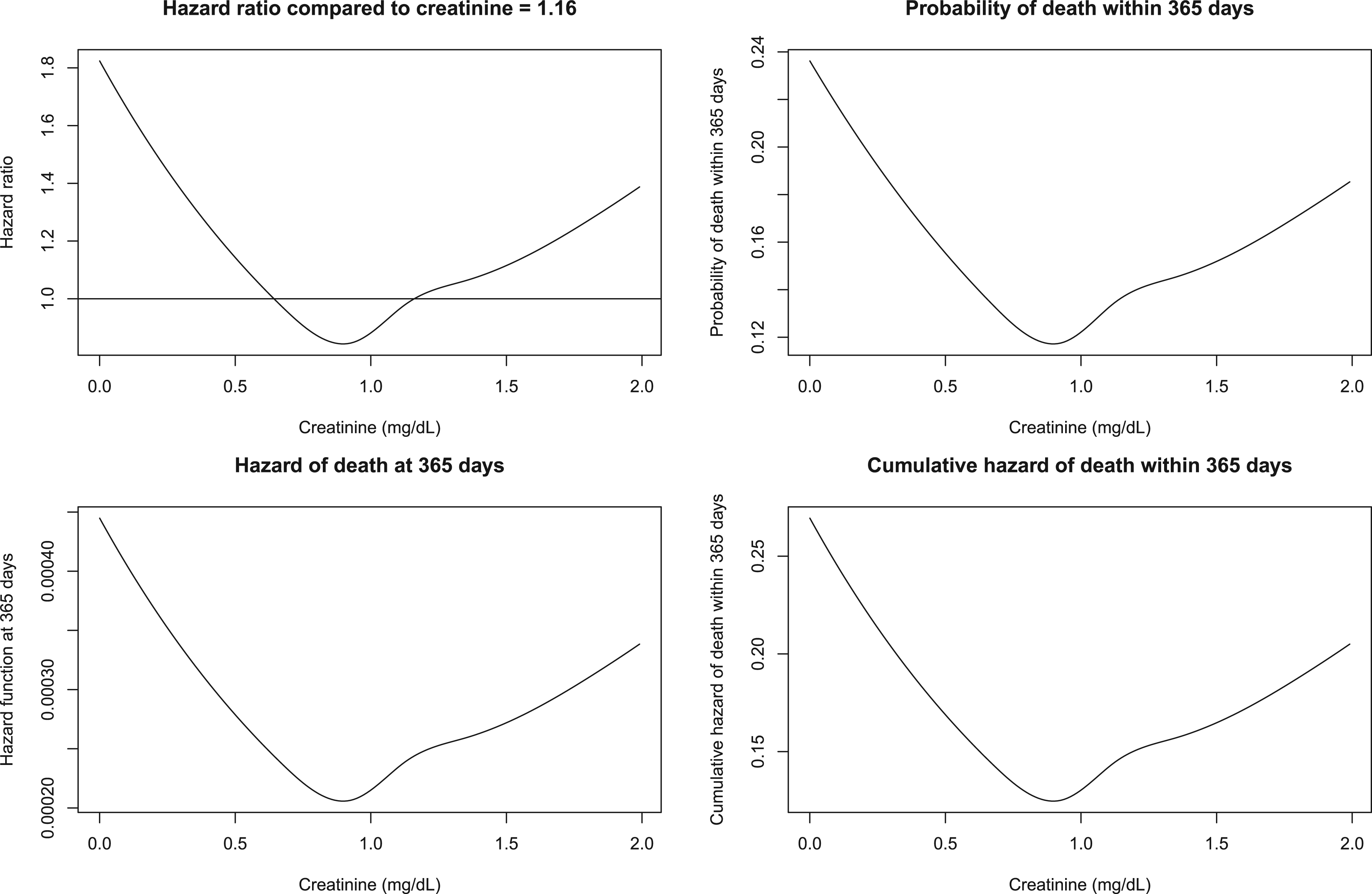
Relationship between creatinine and mortality.
The relation between creatinine and mortality is described in Figure 3. As with age and blood pressure, the shape of the curve is qualitatively similar across the four methods. In each panel we observe that the “risk” of death initially decreases with increasing creatinine, then reaches a nadir when creatinine is approximately 0.9, and then subsequently increases with increasing creatinine.
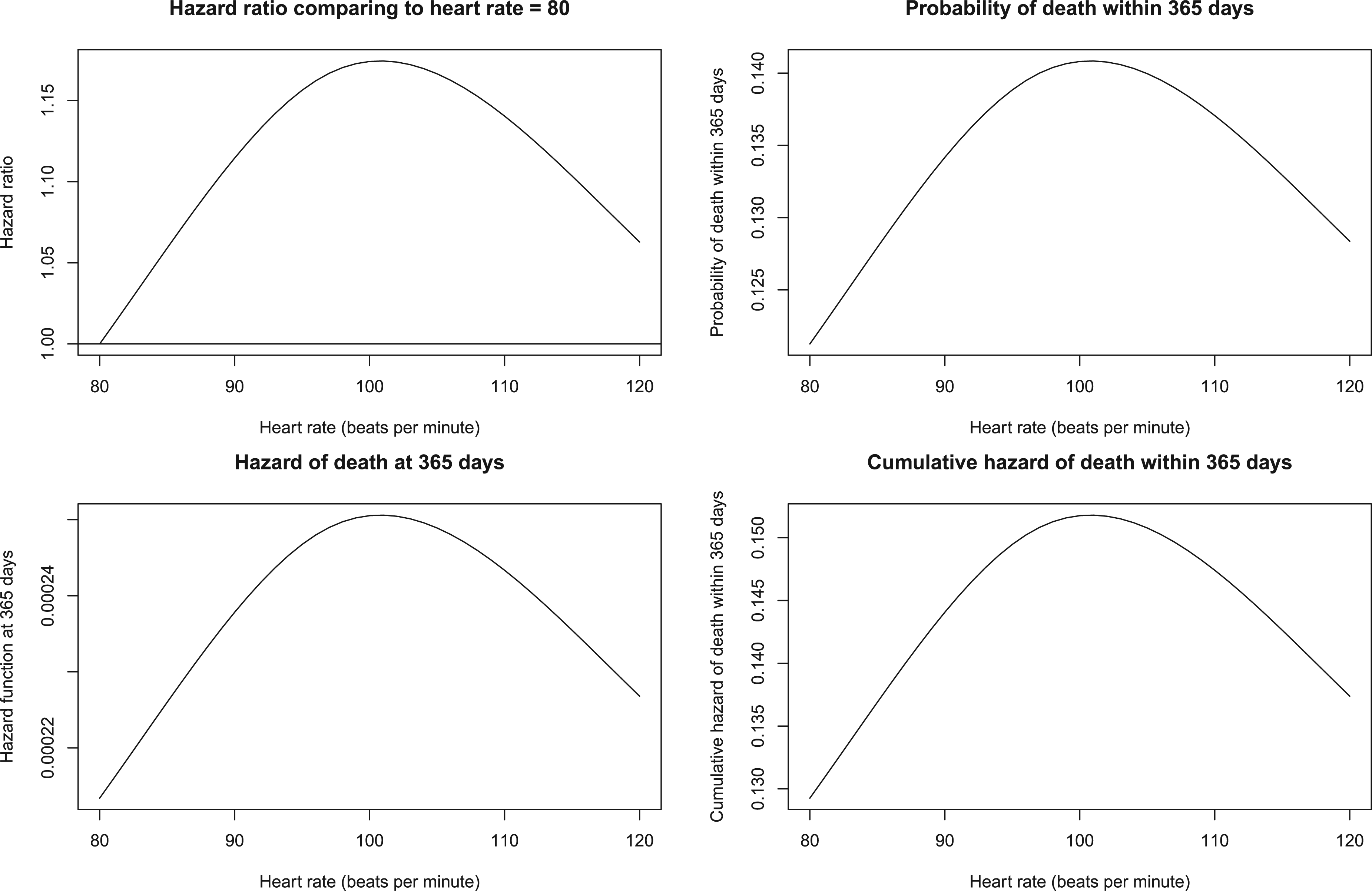
Relationship between heart rate and mortality.
Finally, the relation between heart rate and mortality is described in Figure 4. As with the other three variables, the shape of the curve is qualitatively similar across the four methods. In each panel we observe that the “risk” of death initially increases with increasing heart rate, then reaches a maximum when heart rate is approximately 100, and then subsequently decreases with increasing heart rate.
Motivated by the qualitatively similar relation between a given continuous variable and the outcome across the four graphical methods that we observed above, we conducted mathematical derivations to demonstrate the generalizability of these observations. For simplicity, in the derivations that follow, we assume that the Cox model incorporates a single continuous variable, denoted by X, using RCS with k knots. Thus, within each interval defined by the knots, the continuous variable can be represented using a cubic polynomial. The relation will be linear in the tails; however, linearity is a special case of a cubic polynomial.
Plot of hazard ratios comparing each level of X with a reference level of X
Within an interval determined by adjacent knots (or in the interval to the left of the lower knot or in the interval to the right of the upper knot), the Cox model can be written as:
The hazard ratio comparing the hazard of the outcome at
The first term in the derivative is strictly positive. Thus, the sign of the derivative will be determined solely by the second term
In the derivative above, the sign of the derivative will be determined only by the term
Plot of the cumulative incidence of the outcome at a specific time against X
Within an interval defined by adjacent knots, the cumulative incidence of the outcome at time t0 is defined as
Plot of the hazard function of the outcome at a specific time against X
Within an interval determined by adjacent knots (or in the interval to the left of the lower knot or the interval to the right of the upper knot), the hazard function can be written as
Plot of the cumulative hazard function of the outcome at a specific time against X
Within an interval determined by adjacent knots (or in the interval to the left of the lower knot or the interval to the right of the upper knot), the cumulative hazard function at time
Thus, for a given interval determined by adjacent knots (or in the lower and upper tails), each of the four curves will be decreasing when
In the above derivations, we assumed that the Cox model included a single continuous variable represented using RCS. If there were additional covariates in the model, the derivative of the linear predictor for these covariates with respect to X would be 0, resulting in identical conclusions.
Discussion
We described four methods to graphically describe the relation between a continuous covariate and the outcome when using a Cox proportional hazards model. These graphical methods allow investigators to provide a simple graphical description of the nature of the relation between a continuous covariate and the outcome. We demonstrated, both using a case study and mathematical derivations, that the four methods will result in qualitatively similar conclusions about the nature of the relation between the continuous covariate and the time-to-event outcome.
The methods that we have described assume that the analyst has decided to allow a nonlinear relationship between a continuous variable and the log-hazard of the outcome. This decision could be based on exploratory data analysis, results from previously published studies, or based on statistical practice. The methods that we have described are not intended to inform that decision. However, once the decision has been made to allow for nonlinear relationships, the methods that we have described allow for a graphical communication of the nature of the relationship between the variable and the risk of the outcome.
There are relative advantages and disadvantages to the four methods. The first method computes the hazard ratio comparing the relative change in the hazard of the outcome for each value of the continuous covariate compared to the hazard of the outcome for a specified reference level of the continuous covariate. An advantage to this method is that it uses the hazard ratio, which is the common measure of association when using the Cox model. A second advantage to this approach is that, unlike the other three methods, it does not require estimation of the baseline hazard function, which can be considered a nuisance parameter. A third advantage of this approach is that the general shape of the curve is independent of the choice of reference level used for computing hazard ratios. A disadvantage of this approach is that the curve is a relative curve, with the hazard at a given value of the covariate being compared to the hazard at the reference value of the covariate. A second disadvantage to this approach is that one must specify the reference value of the variable. However, as demonstrated above, the choice of reference level will not affect the general shape of the curve. The other three methods describe the relation between the continuous covariate and the cumulative incidence, the hazard function, and the cumulative hazard function. A disadvantage of each of these three methods is that each requires the specification of a time at which the cumulative incidence, the hazard, and the cumulative hazard are computed. A second disadvantage of these three methods is that each requires the specification of a covariate pattern at which each of these functions is evaluated (e.g. the model covariates are set to the cohort median). However, the shape of the curve would be similar regardless of the covariate pattern chosen, with the resultant curve shifted upwards or downwards. A third disadvantage of these three methods is that each requires estimation of either the baseline hazard function or the baseline survival function, which are considered nuisance parameters in the Cox model. An advantage to these three methods is that each reports the absolute measure of association rather than a relative measure of association. A limitation of the method that reports the relationship between the covariate and the hazard of the outcome at a specific time is that the hazard function is defined as a limit. While the hazard function can be estimated or approximated, the reported value may vary across estimation procedures. If different estimation procedures are used, this may cause problems when comparing graphical results for this method across studies. In the case study, for all four variables, both the hazard of death at 365 days and the cumulative hazard of death within 365 days were strictly between 0 and 1 for all values of each of the four variables. A limitation of the two methods based on these quantities is that readers who lack familiarity with methods for survival analysis may be tempted to incorrectly assign a probabilistic interpretation to these quantities. Similarly, when reporting the cumulative hazard of the outcome, readers need to be aware that a ratio of cumulative hazards is not a reliable proxy for the hazard ratio.
The use of methods to allow for nonlinear relationship between continuous covariates and the log-hazard of the outcome are well established in survival analysis. The Cox model also allows for time-varying covariate effects, which relaxes the proportional hazards assumption and allows the hazard ratio to vary as a function of time. In a recent paper, we described a method to allow the regression coefficients to vary as a smooth function of time, by using restricted cubic splines to model the log-hazard ratio as a function time. 8 This method allowed for a graphical depiction of the hazard ratio as a smooth function of time. Future research is required to develop methods for combining these two approaches and producing a surface expressing the hazard ratio (or other any of the other measures) as a function of both the variable and time.
Our recommendation would be to use the method based on computing the hazard ratio comparing the relative change in the hazard of the outcome for each value of the continuous covariate compared to the hazard of the outcome for a specified reference level of the continuous covariate. This method does not require estimation of the baseline hazard function or of the baseline survival function. Furthermore, the general shape of the resultant curve is not influenced by the choice of reference level. However, we have demonstrated that qualitatively similar conclusions would be drawn regardless of the method used. This is an important message, since it allows for comparing results across different published studies that used different methods for describing the relationship between a given variable and the risk of the outcome. Thus, authors who have a different preference can implement that method knowing that it will produce qualitatively similar conclusions to those of the other methods.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. Parts of this material are based on data and/or information compiled and provided by the Ontario Ministry of Health. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. Parts of this material are based on data and/or information compiled and provided by CIHI. However, the analyses, conclusions, opinions and statements expressed in the material are those of the author(s), and not necessarily those of CIHI. This work was supported by the Canadian Institutes of Health Research (grant number PJT—166161). The data sets used for this study were held securely in a linked, de-identified form and analysed at ICES. While data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at ![]() .
.