
Abstract
The accelerated failure time model is an alternative to the Cox proportional hazards model in survival analysis. However, conclusions regarding the associations of prognostic factors with event times are valid only if the underlying modeling assumptions are met. In contrast to several flexible methods for relaxing the proportional hazards and linearity assumptions in the Cox model, formal investigation of the constant-over-time time ratio and linearity assumptions in the accelerated failure time model has been limited. Yet, in practice, prognostic factors may have time-dependent and/or nonlinear effects. Furthermore, parametric accelerated failure time models require correct specification of the baseline hazard function, which is treated as a nuisance parameter in the Cox proportional hazards model, and is rarely known in practice. To address these challenges, we propose a flexible extension of the accelerated failure time model where unpenalized regression B-splines are used to model (i) the baseline hazard function of arbitrary shape, (ii) the time-dependent covariate effects on the hazard, and (iii) nonlinear effects for continuous covariates. Simulations evaluate the accuracy of the time-dependent and/or nonlinear estimates, and of the resulting survival functions, in multivariable settings. The proposed flexible extension of the accelerated failure time model is applied to re-assess the effects of prognostic factors on mortality after septic shock.
Keywords
Introduction
In most cohort studies of disease occurrence, progression, treatment or mortality, times to relevant clinical outcomes depend on multiple risk or prognostic factors, and exposures. Thus, whether the main focus is on etiology or on prediction, multivariable time-to-event analyses are essential. Yet, multivariable survival analyses require specifying a formal statistical model that describes how covariates are associated with the event times. Here, different survival models postulate different modes of covariates’ action, typically assumed to be common to all covariates. To facilitate both estimation and interpretation, most standard regression models restrict the corresponding adjusted regression coefficients (e.g. ratios of hazards, odds or survival times) for all covariates to remain constant over time. However, it is often plausible that true effects of some covariates are not consistent with this underlying modeling assumption, requiring extending the model to incorporate time-varying coefficients. In addition, for each continuous covariate one has to specify a suitable functional form of its relationship with the outcome. 1 Both aforementioned modeling complexities have received considerable attention within the vast literature on hazard-based models that dominate medical applications of survival analysis 2 but they are equally relevant for other multivariable survival models. In this manuscript, we attempt to address these challenges within the framework of multivariable accelerated failure time (AFT) model.
The AFT model provides an alternative to the proportional hazards (PH) model to analyze time-to-event data.3,4 Instead of the log hazard ratios estimated in the PH model, in the AFT model the covariate effects are expressed directly on the event time scale and estimated by the log event time ratios. For example, if the event time ratio (treated vs. control) equals 1.25, then the time corresponding to any given survival probability is 25% longer for the treated than the control subjects, implying accelerated failure times among the controls. Recently, the AFT model has become increasingly popular, partly because it avoids the noncollapsibility5,6 and resulting built-in selection bias of PH-based hazard ratios.7,8 However, in contrast to the Cox PH model, the parametric AFT models require specifying the event time distribution,4,9 which is difficult in many real-life applications. To avoid this restriction, several semiparametric AFT models were proposed,10–16 including our recent spline-based model. 17
However, almost all the aforementioned semiparametric AFT models implicitly impose the conventional assumptions underlying the classic AFT model that (i) for all covariates, time ratios, i.e. “acceleration factors,” are constant over time and (ii) continuous covariates have linear relationships with the logarithm of event time 18 (see Appendix A.1 in Supplementary material for more details). Yet, in multivariable analyses either assumption may be violated, for some covariates. Indeed, real-life applications of flexible extensions of the Cox PH model,19–24 reported frequent violations of the corresponding assumptions of (i) constant hazard ratios (PH)25,26 or (ii) linear covariate effects on log hazard, 27 or even both assumptions, for the same continuous covariate.28,29
In contrast, relatively little work has focused on flexible modeling of covariate effects in the AFT framework. Specifically, whereas alternative AFT partial linear models permit estimating nonlinear (NL) effects, through spline smoothing or piecewise linear functions,30–32 they require additional assumptions about the error distribution 30 or seem restricted to the univariate setting.31,32
Similarly, only a few studies permit modeling nonconstant log time ratios, e.g. as a linear function of the follow-up time t.
33
Cox and Oakes
18
outlined a more general AFT model, which can handle either time-varying covariates
Recently, in an arxiv manuscript, Crowther et al.
16
have proposed a flexible AFT model with restricted cubic splines modeling of the event time distribution. They develop an elegant full likelihood estimation framework and provide practical implementation in Stata and R. Importantly, Crowther et al's.
16
model builds on the aforementioned Cox and Oakes’ model,
18
to incorporate modeling of time-varying effects, on the cumulative scale:


Furthermore, to the best of our knowledge, no published AFT model permits estimating both time-dependent (TD) and NL effects of continuous covariates. Yet, simulations suggest that, under the PH model framework, the relevant TD and NL effects of all continuous covariates should be simultaneously accounted for to avoid biased estimates and inaccurate inference.22,34
To address these challenges, we propose a flexible extension of the AFT model that permits accounting for potential TD and/or NL covariate effect(s) while allowing for arbitrary distribution of the event times. Section “Methods” describes our model and the estimation algorithm. Simulation studies are reported in the section “Simulation studies.” In the section “Real-life application,” our flexible extension of the AFT model identifies TD and/or NL effects of some prognostic factors in real-life multivariable analyses of mortality after septic shock. We conclude with a discussion of our results and their implications.
Methods
In the conventional AFT model, the natural logarithm of the event time, logT, is modeled as a linear function of the covariate vector

The equivalent hazard-based specification of the AFT model is
4
:

Both formulations of the AFT model (1) and (2) imply (i) a linear relationship between each continuous covariate and the log event time and (ii) constant-over-time log time ratios
Joint flexible modeling of NL and TD effects in the AFT model
First, to relax the linearity assumption, the AFT model (1) can be generalized to:



In the proposed model (5), similar to a more constrained hazard-based AFT model (2), the covariate affects the hazard function by not only shifting the baseline hazard



The full log-likelihood based on model (5) for right-censored data is derived as:
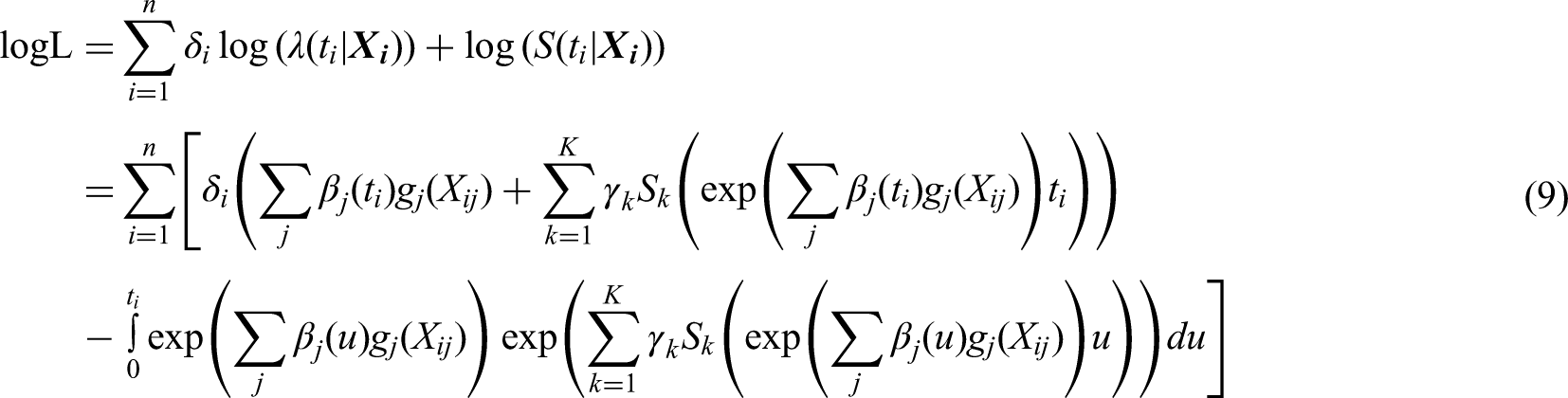
We can estimate the three sets of spline coefficients


Alternating conditional estimation
Estimating the parameters
Appendix A3.2 in Supplementary material describes the ACE algorithm in detail and Appendix A3.3 in Supplementary material discusses bootstrap-based pointwise 95% confidence bands around the estimates.
Reconstructing time-dependent time ratios
The time-dependent estimate
We propose to describe time-dependent covariate effects, within the AFT framework, in terms of the times to reach a specific quantile of the event time distribution. For a binary exposure X, we focus on the ratio
Yet, in multivariable analyses based on our model (5), reconstructing the time-dependent time ratio comparing survival for subjects with different covariate patterns requires complex transformations of


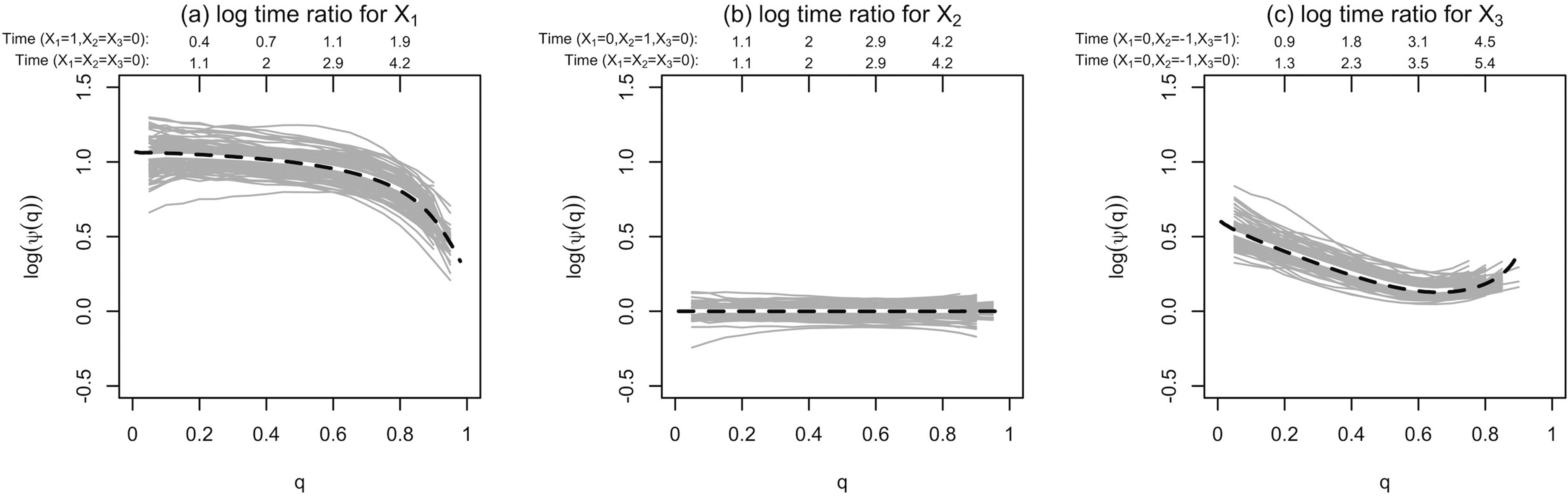
Results of the estimated log time ratios by the flexible accelerated failure time (AFT) model using 100 samples in simulation scenario 1, comparing two covariate patterns for each covariate. The two covariate patterns are shown in the labels on the top of each panel, along with the true survival times in both groups corresponding to specific q-quantile of the survival time. The gray curves are the individual estimates from 100 samples, and the pointwise mean is shown by the white curve. The black dashed curve represents the perspective true time ratios.
An R program that implements model (5) and includes functions to estimate the NL and TD effects and reconstruct time-dependent time ratios for an arbitrary contrast in any covariate is available at GitHub (https://github.com/MenglanPang/Flexible-AFT-Model).
Simulation studies
Design of primary simulations
To evaluate the performance of the proposed model in multivariable AFT analyses, we simulated a hypothetical cohort of N = 1000 subjects followed until the event or administrative censoring, at 6 years. Event times were generated from the extended AFT model, conditional on three covariates (binary X1 and continuous X2, X3):


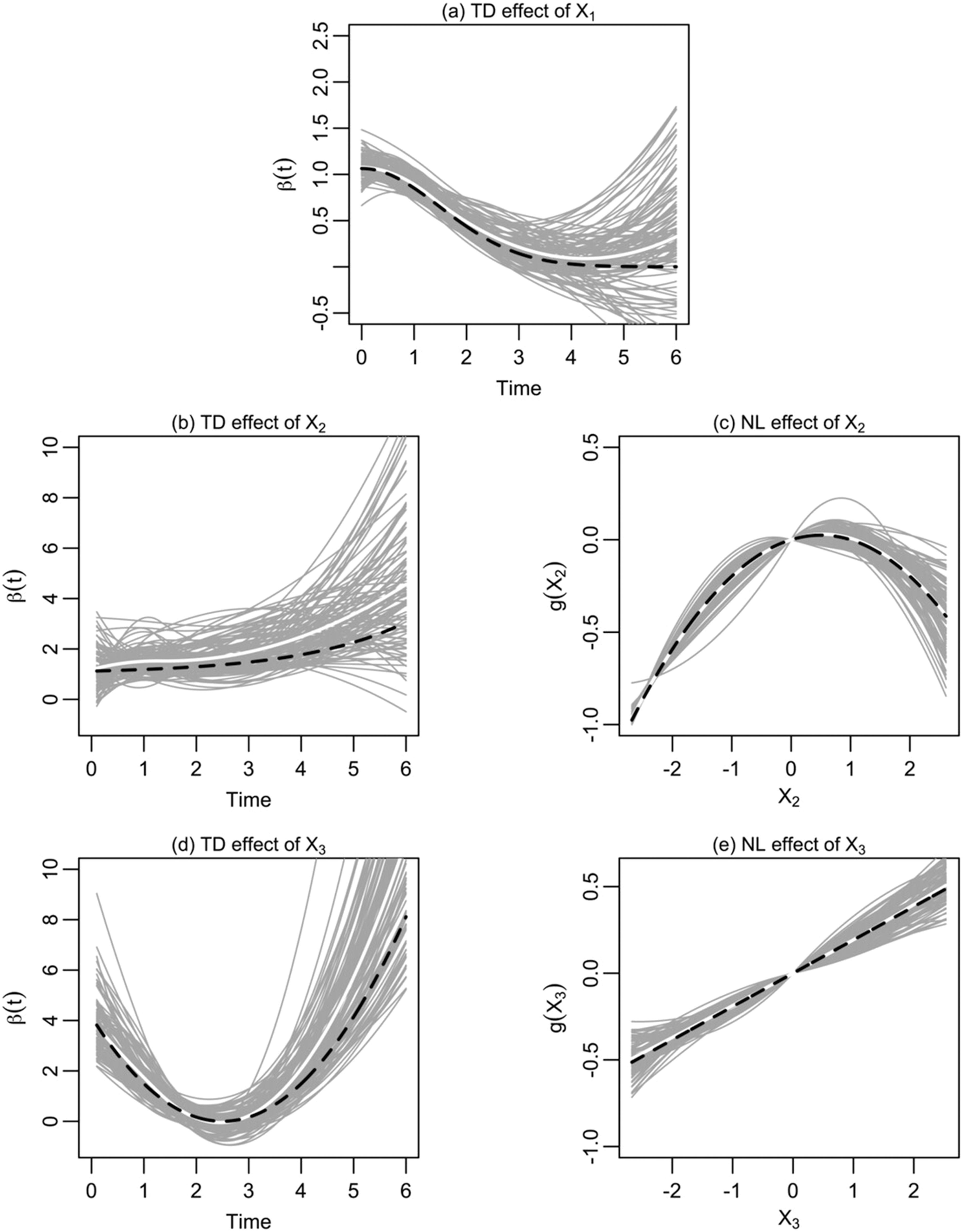
Results of the estimated TD and NL effects by the flexible AFT model using 100 samples in simulation scenario 1. The gray curves are the individual estimates from 100 samples, and the pointwise mean is shown by the white curve. The black dashed curve represents the true rescaled NL and TD functions.
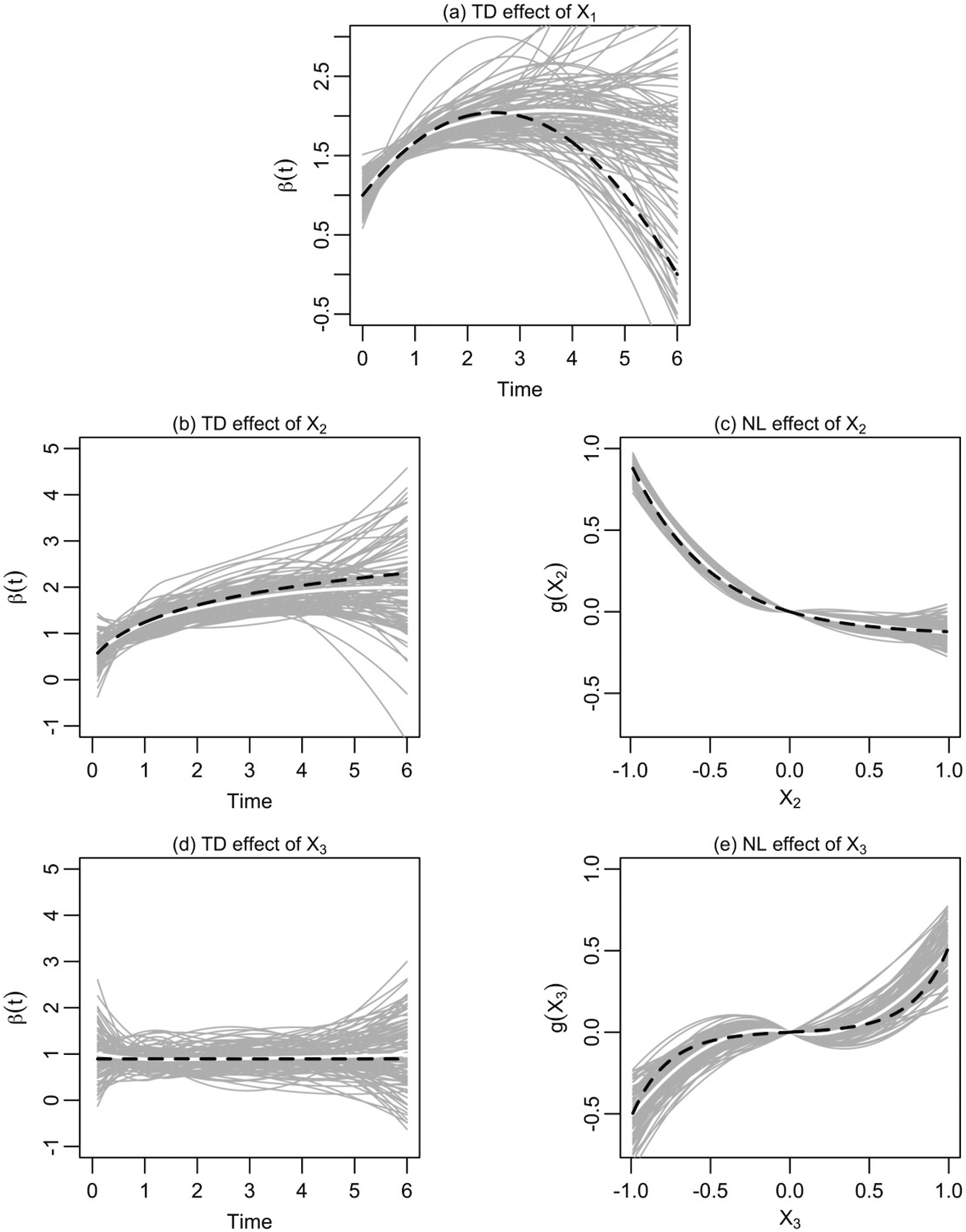
Results of the estimated TD and NL effects by the flexible AFT model using 100 samples in simulation scenario 2. The gray curves are the individual estimates from 100 samples, and the pointwise mean is shown by the white curve. The black dashed curve represents the true rescaled NL and TD functions.
Results of primary simulations
For both scenarios, three multivariable models were fit to each of the 100 simulated samples: (i) the “conventional” parametric Weibull AFT model with linear covariate effects and constant time ratios; (ii) the “nonlinear” Weibull AFT model with NL effects for
Estimation of the TD and NL functions
To assess the accuracy of the covariate effects estimated with our model (5), Figures 1 and 2 compare the 100 TD and NL estimates (gray curves) against the corresponding true functions (black dashed curves), respectively for scenarios 1 and 2. (The estimates are rescaled, as explained in Appendix A3.4 in Supplementary material). In scenario 1, most of the estimates correctly recover the TD effects of different shapes (Figure 1(a), (b) and (d)), and the NL estimates for X2 and X3 (Figure 1(c) and (e)). The TD estimates show more variability in the tails, where the events are less frequent and regression splines are less stable.
36
Yet, the mean values of all spline-based estimates (white curves) trace fairly close the corresponding true TD/NL functions, indicating lack of under- or over-fit bias, even for the truly linear effect of
Figure 2 shows that for scenario 2 almost all spline-based TD and NL estimates are also reasonably unbiased, including TD estimates of the truly constant-over-time effect for
Appendix A4.2 in Supplementary material shows that generally similar results for scenario 1 were obtained with different sample sizes (N = 650, 1500) and event rate (40%). Appendix A4.3 summarizes results from the more constrained AFT models (i) and (ii) that illustrate the impact of mis-specifying the covariate effects.
Hazard and survival estimates
Figure 3 compares model-specific hazard and survival estimates (gray curves) in scenario 1, for covariate vector
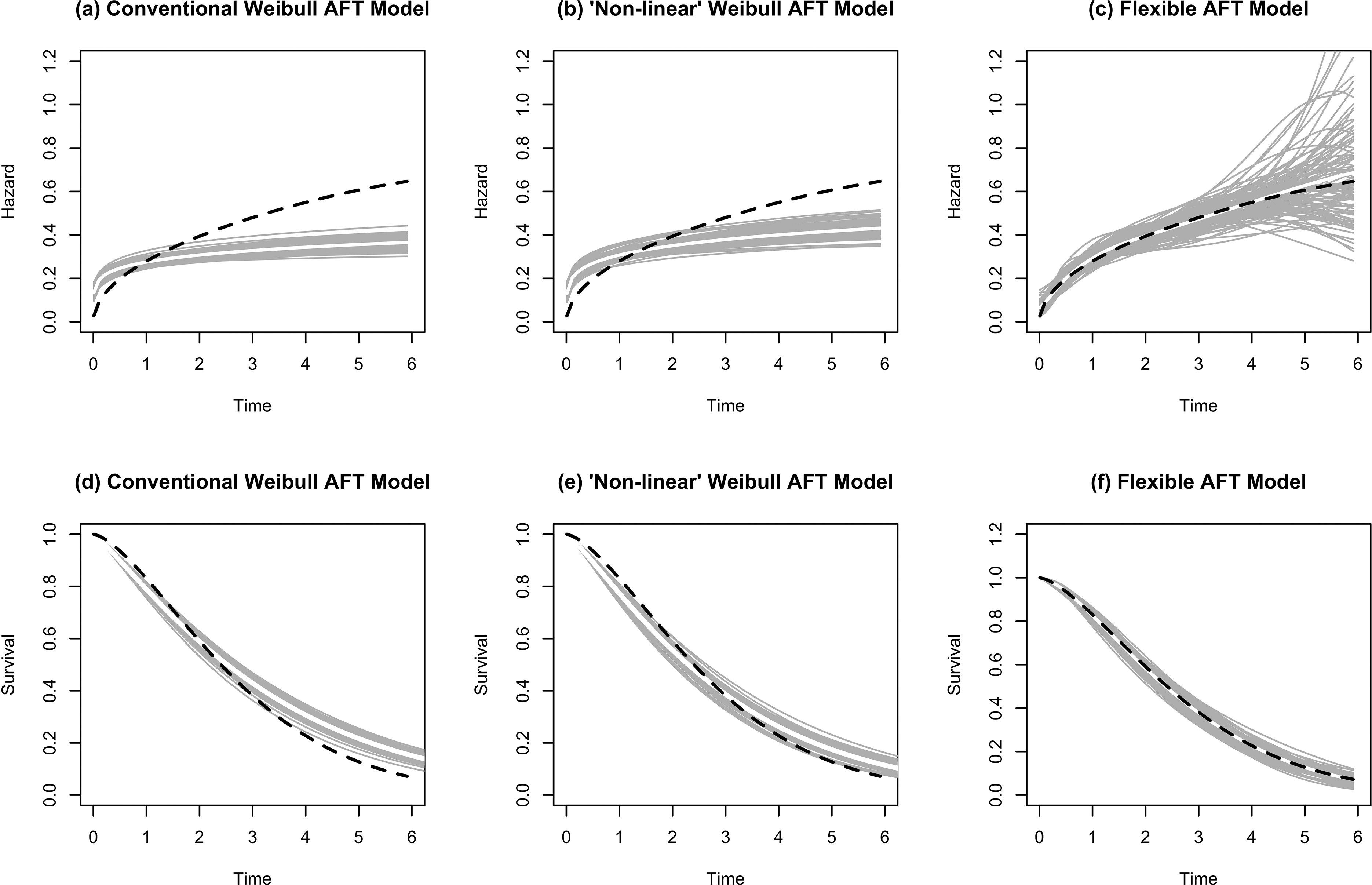
Estimated baseline hazard functions (the first row) and survival curves (the second row) by the three alternative models using 100 samples in simulation scenario 1. The gray curves are the individual estimates from 100 samples, and the pointwise mean is shown by the white curve. The black dashed curve represents the true baseline hazard and survival functions.
Time-dependent time ratios
Figure 4 shows the estimated adjusted time-dependent time ratios (gray curves), reconstructed using methods of the section “Reconstructing time-dependent time ratios,” in scenario 1 for selected contrasts (see figure legend for details), against the true time ratios (black dashed curves). The shapes of the reconstructed time-dependent time ratios for
Comparison of goodness of fit
Table 1 shows that, as expected, when true time ratios were time-varying for some covariates, the proposed flexible model (5) yielded better fit to data than the more constrained AFT models (i) and (ii) (mean Akaike information criterion (AIC) differences of 44–125 points). In contrast, in additional simulations with data generated from the conventional AFT model (1), with constant time ratios and linear effects, our flexible model (5) yielded AIC worse by, on average, 10–13 points than the two simpler AFT models (Appendix A4.7 in Supplementary material), which correctly suggested the lack of systematic TD and NL effects. These results confirm the usefulness of goodness-of-fit comparisons for “model diagnostics.” 37
Comparison of mean Akaike information criterion (AIC) in simulation studies from three alternative models.

AFT: accelerated failure time.
Real-life application
Data source
We applied the model (5) to a real-life study to re-assess the role of important prognostic factors for 3-month all-cause mortality after septic shock.38,39 Time zero corresponded to initiation of vasopressors in response to septic shock, and patients alive at 90 days after the septic shock were censored. 39 Details on baseline covariates, measured at admission, were reported elsewhere.38,39 Our analyses included 858 patients who had appropriate antibiotics therapy and complete covariate data. There were 433 (50.5%) deaths during the 1478 patient months of follow-up (median duration: 63.5 days).
Flexible AFT analyses
We assessed five important baseline prognostic factors, selected a priori, based on the literature 38 : age, and Sepsis-related Organ Failure Assessment (SOFA) score, with higher scores indicating a worse organ dysfunction, and three binary variables: immune suppression (yes vs. no), infection site (urinary tract vs. other), and Knaus score of activity limitations (normal or moderate vs. severe or bedridden). 38 Three additional binary covariates were considered for inclusion if they improved the model's fit to data: presence of the germ, infection type (community-acquired vs. nosocomial) and cirrhosis status.
Appendix A5.1 in Supplementary material describes the 3-stage procedure used to select specific TD and/or NL effects, and the additional covariates, into the final multivariable model (5). The pointwise 95% confidence bands for the baseline hazard, and the selected TD and NL functions, were estimated based on 300 bootstrap resamples.
Alternative models
We estimated three additional models, with the same covariates, as selected into our final flexible model (5): (i) the “conventional” Weibull AFT model, with constant time ratios and linear effects of continuous covariates, (ii) the “nonlinear” Weibull AFT model that allowed for NL effects (see the section “Results of primary simulations” for details), and (iii) the extension of constant/linear AFT model (i) which modeled baseline hazard in (2) with splines, to avoid distributional assumptions. 17 Notice that models (i)–(iii) could not accommodate potential TD effects and only model (ii) allowed for NL effects.
Results
The spline-based estimate in Figure 5(a) shows that the baseline all-cause mortality hazard decreases monotonically with time since septic shock. For each prognostic factor (row), Table 2 compares the effects estimated with the four AFT models (columns). (Table A5.1.1 in Supplementary material shows details of model selection). For variables for which no TD effects were selected, all four models estimate similar constant-over-time time ratios, with longer survival associated with absence of immunosuppression, urinary infections and less severe Knauss scores.
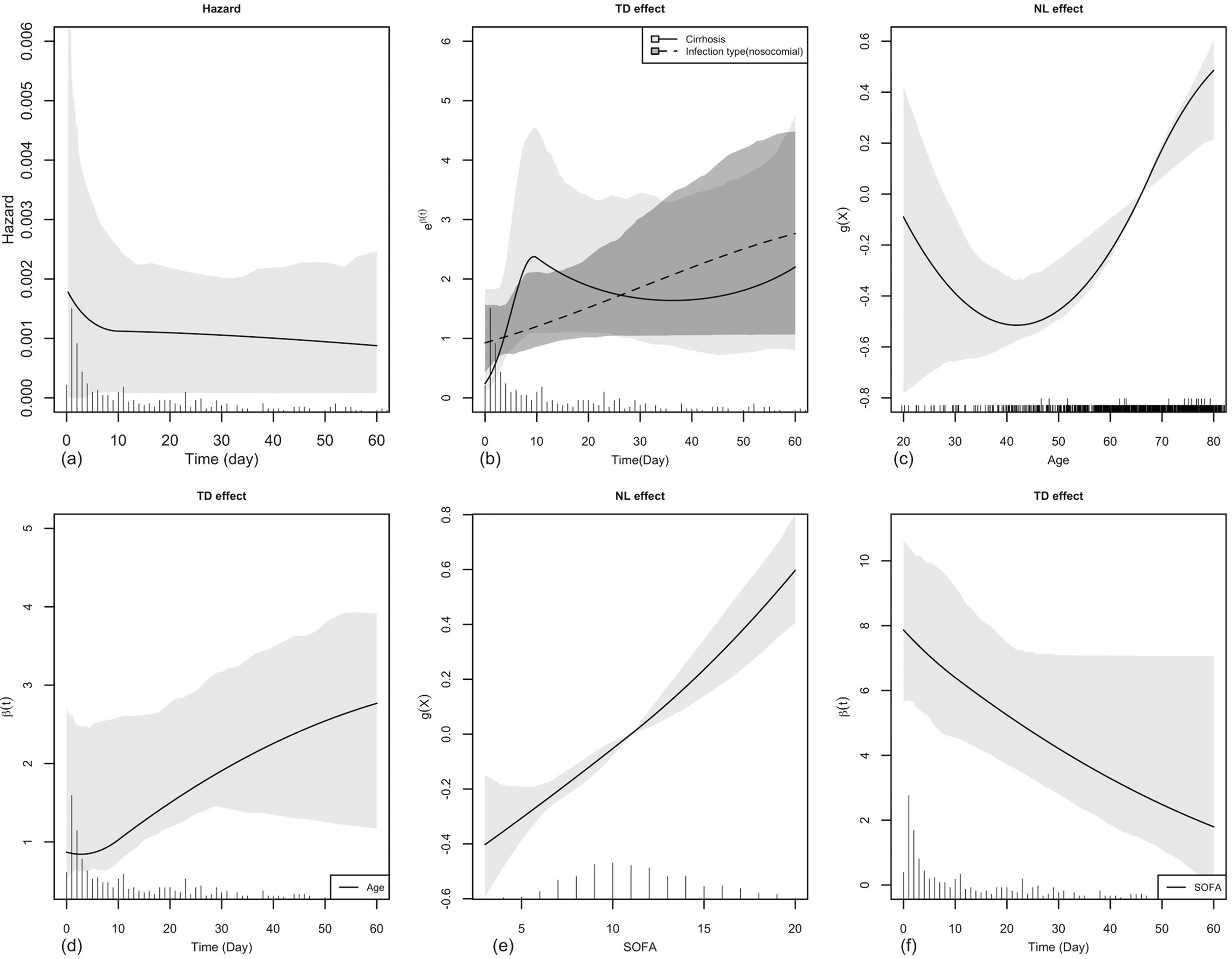
Results of the flexible AFT model in study on mortality after septic shock. (a) Baseline hazard function (for individuals with all binary covariates equal 0, age equals to the minimal age of 20 years, and SOFA score equals to the minimal value of 3); (b) TD effects of the cirrhosis status and nosocomial infection; (c) NL effect of age relative to the mean age of 66 years; (d) TD effect of age; (e) NL effect of SOFA score relative to the mean score of 11; and (f) TD effect of SOFA score. Estimates are represented by the black curve, and the shaded gray areas correspond to the 95% pointwise confidence bands, based on 300 bootstrap resamples. The NL effects are constrained to equal 0 at the reference value corresponding to the mean covariate value, and thus the estimates at the reference value show no variation. The empirical distributions of the observed event times (panels a, b, d, f), age (panel c), and SOFA score (panel e) are shown by rug plots at the bottoms of the respective graphs.
The estimated event time ratios and AIC values from alternative models in study on mortality after septic shock.
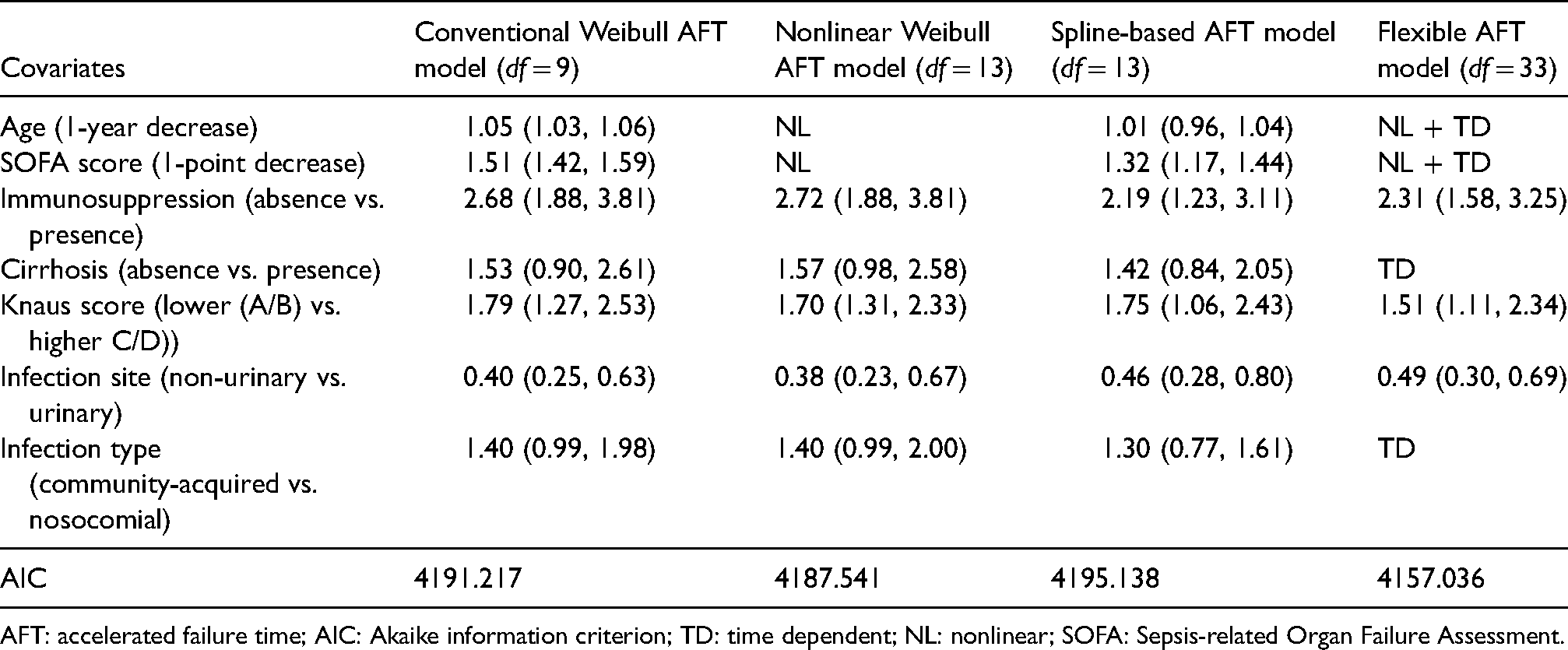
AFT: accelerated failure time; AIC: Akaike information criterion; TD: time dependent; NL: nonlinear; SOFA: Sepsis-related Organ Failure Assessment.
The last column of Table 2 indicates which TD and/or NL effects were selected into our final flexible model (5). TD estimates in Figure 5(b) show how the strength of the effects of infection type and cirrhosis on the hazard vary over the first 60 days after the septic shock. The association of nosocomial infection with higher mortality becomes stronger with longer follow-up (dashed curve), whereas the impact of cirrhosis increases rapidly during the first 10 days and then stabilizes (solid curve). Table A5.1.2 in Supplementary material shows the resulting time ratio estimates. Both TD effects substantially improve the model's deviance (3-df likelihood ratio test (LRT) statistics of 8.93 and 22.24, respectively), implying also rejection of the H0 of no association with survival. 40 In contrast, all simpler models (i)–(iii), that did not allow for TD effects, suggested constant-over-time effects of both factors were marginally nonsignificant (Table 2) and under-estimated their long-term impact, relative to our TD time ratio estimates in Table A5.1.2.
Our final flexible model (5) included also NL and TD effects for age and the SOFA score (last column of Table 2). The nonmonotone J-shaped NL effect of age (Figure 5(c)) suggests mortality is lowest at about 45 years and increases for both younger and older patients. The TD effect for age in Figure 5(d) indicates that this impact becomes stronger over time. In contrast, the NL effect of SOFA is weak (Figure 5(e)) and adding the NL term improves only marginally the deviance (4-df LRT = 9.256, p = 0.055). While this association weakens over time, a higher SOFA at the time of septic shock is associated with a risk increase even two months later when the 95% pointwise confidence interval still excludes 0 (Figure 5(f)). (Figure A5.2.1 in Supplementary material shows NL effects of age and SOFA estimated, based on our model (5), at different follow-up times, and Figure A5.2.2 in Supplementary material shows their NL effects estimated by the “nonlinear” Weibull model (ii).)
The proposed flexible extension of the AFT model (5) improved AIC by at least 30 points relative to simpler models (i)–(iii) (bottom of Table 2), highlighting the importance of accounting for the effects NL and/or TD effects. (The Cox–Snell residual plots are shown in Figure A5.2.3 in Supplementary material).
Discussion
To the best of our knowledge, the proposed model (5) is the first flexible extension of the AFT model that simultaneously incorporates both the TD effects and NL effects of continuous variables on the logarithm of hazard function, along with TD effects for categorical variables. The NL and TD effects, and the baseline hazard, are modeled using low-dimension unpenalized regression B-splines. The NL estimate describes how the hazard varies with an increasing value of a continuous covariate, whereas the TD estimate informs how the strength of the covariate effect changes during the follow-up.
In multivariable simulations, the proposed spline-based estimates of the NL and TD effects were reasonably unbiased, and the methods of the section “Reconstructing time-dependent time ratios” permit reconstructing time-dependent time ratios for arbitrary contrasts in the covariate values. Furthermore, the survival curves, conditional on multiple covariates with possibly complex effects, are accurately estimated. In contrast, simulations in Appendix A4.5 in Supplementary material demonstrate that ignoring an important NL effect may bias survival curve estimates. This was expected, given similar simulation results obtained within the PH modeling framework 34 confirm that mis-specified models yield biased estimates. Here, we note that in most of our simulations the data-generating mechanisms were structurally compatible with our proposed flexible model (5). This helped assess the accuracy of the NL and TD estimates under a correctly specified model, but future research should investigate more complex situations where the selection of TD/NL effects relies on data-dependent criteria. However, in additional simulations in Appendix A2 in Supplementary material, even if the data-generating mechanism avoided any explicit specification of time-dependent effects on the hazard, i.e. did not favor our model (5), it still allowed an accurate reconstruction of group-specific survival functions, providing some further reassurance regarding its usefulness.
The analyses of mortality after septic shock illustrate how our flexible NL/TD estimates may provide new insights into the role of different prognostic factors. For age, the NL estimate suggests a nonmonotone effect on the hazard, whereas the TD estimate indicates that its strength increases over time, possibly because mortality soon after a septic shock depends mostly on the indicators of the severity of the patient's initial condition (especially SOFA and Knaus scores) rather than on age. In contrast, among those who survive this critical early period, older patients are more likely to die. Furthermore, TD estimates for both nosocomial infection and cirrhosis suggest statistically significant increases in their impact with longer time since the septic shock (Figure 5(b)). In contrast, all simpler AFT models, constrained to constant-over-time event time ratios, did not yield evidence of systematic associations of either factor with survival.
Additional practical advantages of our flexible multivariable model (5), that extends the AFT model to account for NL and/or TD effects of the covariates on the hazard, may include also improving both (i) the model's fit to data (Section “Results”) and (ii) accuracy of prediction for individual patients. Regarding (ii), in simulations our flexible model (5) yielded practically unbiased estimates of survival functions, conditional on different covariate vectors, whereas simpler AFT models constrained by the conventional assumptions of either constant time ratios or linearity, yielded markedly biased estimates of survival probability, for selected covariate patterns (Figure 3 and Figures A2.1 and A4.5). Thus, our proposed flexible model (5) may be of interest, both for etiology and prediction, especially in multivariable analyses, where some covariates act consistently with the AFT assumption but other may violate the constant time ratio assumption. Finally, because AFT estimates are not affected by noncollapsibility,5,6 in some applications flexible time-varying AFT models, such as our model (5) or the Crowther et al.'s model, 16 may help explore the reasons for TD effects identified through flexible extensions of the PH model. Indeed, if for covariate X one finds decreasing-over-time effects in terms of both event time ratios and hazard ratios, then it is less likely that the latter finding reflects just an omitted “susceptibility” or frailty.7,41,42
To facilitate interpretation of the time-dependent covariate effects estimated through our model (5), section “Reconstructing time-dependent time ratios” describes how to reconstruct the corresponding time-dependent event time ratios. The time-dependent time ratio, for a given contrast in the covariate value (e.g.
Several flexible methods were proposed to estimate time-dependent hazard ratios in the extended Cox model.20,24,28,40,43 In contrast, to date, discussion of TD covariate effects in the context of AFT modeling, i.e. time-dependent time ratios, has received relatively little attention and, to the best of our knowledge, is limited to the general idea expressed by Cox and Oakes,
18
an extended linear hazard model by Elsayed et al.,
33
and the recent arxiv manuscript by Crowther et al.,
16
discussed later in this section. (Indeed, published flexible AFT partial linear models relax the linearity constraint, but impose the constant time ratio assumption30–32). One reason may be related to a complex relationship of time-dependent time ratio with the inverse survival function, as outlined in section “Reconstructing time-dependent time ratios.” In the PH framework, the time-dependent hazard ratio for a given covariate at time t is independent of the baseline hazard, or other covariates. In contrast, in the AFT framework, assessing the time-dependent time ratio for covariate
Therefore, to facilitate separating possibly TD covariate effects from the baseline hazard, and to avoid difficulties in modeling survival and/or density functions,
20
we have implemented our model (5) as a flexible extension of the hazard-based formulation of the AFT model (2), rather than of the “classic” event time-based AFT model (1). Specifically, we replaced the constant
Our proposed methods have some limitations. First, when analyzing the simulated data, we have a priori decided to estimate all potential NL and TD effects, regardless of which effects were present in the “true” data-generating model. We were encouraged to observe that for covariates without true TD or NL effects, most of the TD estimates were approximately constant-in-time and the NL estimates approximated well a straight line (Figures 1(e) and 2(d)). Thus, over-fit bias, a common concern for flexible modeling,23,36,45 was not a major issue in our simulations, with about 250 uncensored events and three covariates. Additional simulations, with different event frequency and more covariates, may be, however, necessary to further explore this issue.
Furthermore, due to the complexity of the likelihood function and the iterative ACE procedure, the computation time can be long, especially for large datasets where several TD and/or NL effects need to be estimated. For example, the average run time across the 100 simulations for scenario 1 in the section “Simulation studies” with N = 1000 and 80% event rate was 1.5 h on computers with Ubuntu operating system with 3.20 GHz Intel Core i7-8700 CPU and 16 GB memory. For the septic shock application, it took 6.7 h to run the final model, with 7 covariates, 33 df's and N = 858, on a Mac computer with 2.7 GHz Intel Core i5 CPU and 8 GB memory. Yet, despite the computational burden, we were able to run multivariable simulations and estimate TD and/or NL effects of 3 covariates. With rapid improvement of the computational power, future real-life analyses of a single, even large, multivariable datasets will become increasingly efficient.
Further work is needed to systematically compare the proposed flexible NL/TD extension of the AFT model (5) with the PH Cox model, and its flexible extensions. Our simulations were designed to evaluate the performance of the proposed model under the AFT framework, therefore the data were generated accordingly. However, in many real-life applications, the “true” data-generating model may be more consistent with the PH model, implying violation of the constant time ratio assumption underlying the conventional AFT model, which may lead to biased estimates, unless the baseline hazard is exponential or Weibull. In such situations, by allowing the time ratios to vary during the follow-up, our proposed flexible model (5) with TD effects may still reasonably capture the relationships between the covariates and the hazard, but will require more parameters than the PH model, with a single hazard ratio for each covariate. A reverse situation will occur if the (unknown) data structure is more consistent with the AFT model. Therefore, further simulations comparing the PH and AFT models, and their flexible extensions, under a broader range of assumptions concerning “true” data-generating mechanisms, are necessary. Furthermore, in complex real-life studies with multiple covariates, neither the PH nor the AFT assumption may be fully satisfied for all covariates. Then implementing alternative modeling strategies and using goodness-of-fit criteria, supplemented by residual diagnostics, may help choose the final model, or alternative models, but further simulations are necessary to systematically evaluate such diagnostic tools. Finally, because our main focus was on accurate modeling of covariate effects within the AFT framework, we have not considered complex event time distributions. This limitation should be overcome in future simulations, even if our recent work suggests that flexible spline-based modeling of the baseline hazard ensures accurate estimation of constant-over-time covariate effects, i.e. constant acceleration factors, under the conventional AFT model (1), regardless of the “true” (unknown) shape of the hazard. 17
Our flexible TD/NL model (5) can be considered an alternative for the flexible parametric AFT model proposed by Crowther et al. 16 The two models allow for assumption-free modeling of both the event times distribution and time-varying covariate effects, in multivariable analyses, but use different mathematical formulations and estimation procedures. Crowther et al. rely on an elegant full maximum likelihood estimation approach, with user-friendly implementation in R and STATA, which facilitates variance estimation and, for a binary exposure in univariate setting, estimates directly interpretable time-varying acceleration factor. 16 Our model (5) allows more flexibility in accounting for possibly NL effects of continuous covariates and is more directly adaptable to modeling possibly time-dependent covariate effects on the hazard in multivariable analyses. In the general case, both models require additional calculations to estimate time-varying event time ratios for specific contrasts in the values of a particular covariate, and in the section “Reconstructing time-dependent time ratios,” we describe the procedures applicable to our model (5), in univariate or multivariable analyses. Future simulation studies and real-life applications should help systematically compare these two flexible extensions of the AFT model with respect to accuracy of both estimation and inference about time-varying acceleration factors, and computational efficiency. Other outstanding analytical challenges, that need to be addressed in future research on both models, include developing and validating criteria and methods to assist in multivariable model building.
Overall, in simulations involving multivariable analyses, our proposed flexible extension of the AFT model yielded reasonably accurate estimates of complex covariate effects on the hazards and allowed unbiased estimation of individual survival curves, conditional on these effects. The model can be implemented using our R programs, available at GitHub (https://github.com/MenglanPang/Flexible-AFT-Model). Furthermore, our septic shock application suggests that the proposed flexible extension of the AFT model may offer new insights into the role of prognostic factors in clinical studies. Still, further comprehensive simulations and multivariable empirical analyses will be necessary to systematically compare our estimates with those offered by alternative flexible extensions of either the PH model or the AFT model, including the elegant flexible parametric AFT model recently proposed by Crowther et al. 16 We also hope that our work may encourage more widespread use of AFT modeling in time-to-event analyses and stimulate further methodological research in this area.
Footnotes
Acknowledgements
The authors thank Dr Marie-Eve Beauchamp for her valuable comments on the R program.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: RWP holds the Albert Boehringer I Chair in Pharmacoepidemiology. MA and RWP are members of the Research Institute of the McGill University Health Centre, which is supported by core funds from Fonds de Recherche du Quebec-Sante (FRQS). MP was supported by doctoral training award from FRQS. TS was supported through funding from the Canada Research Chair in Biostatistical Methods for Primary Health Care Research (Tier II). This research was partly supported by the NSERC grants of MA and RWP.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.