
Abstract
Objectives
To identify the predictive factors of first hospitalization and associated variables to the main causes of hospitalizations in lupus patients from a Latin American cohort.
Methods
The first hospitalization after entry into the cohort during these patients’ follow-up due to either lupus disease activity and/or infection was examined. Clinical and therapeutic variables were those occurring prior to the first hospitalization. Descriptive statistical tests, multivariable logistic, and Cox regression models were performed.
Results
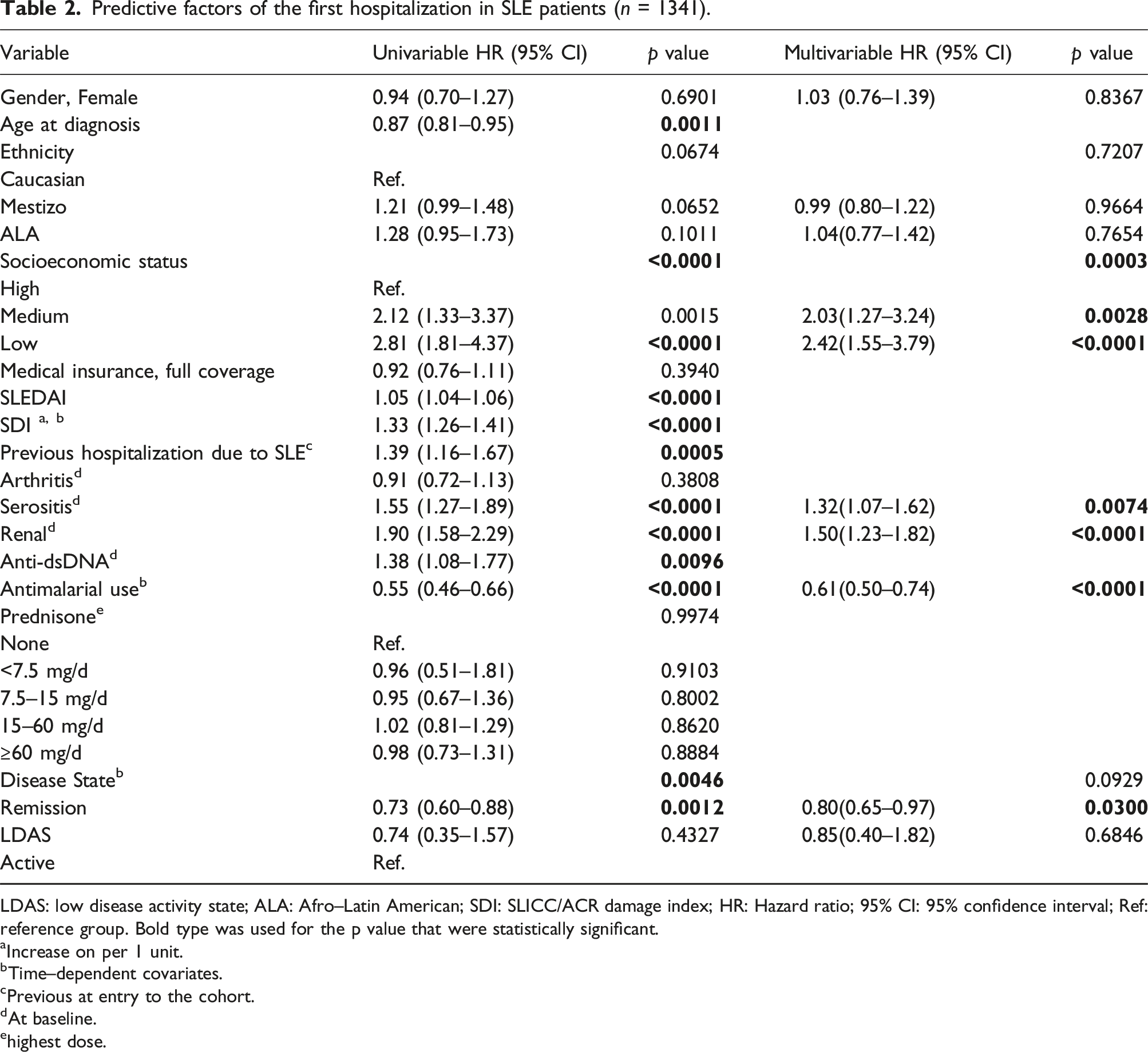
1341 individuals were included in this analysis; 1200 (89.5%) were women. Their median and interquartile range (IQR) age at diagnosis were 27 (20–37) years and their median and IQR follow up time were 27.5 (4.7–62.2) months. A total of 456 (34.0%) patients were hospitalized; 344 (75.4%), 85 (18.6%) and 27 (5.9%) for disease activity, infections, or both, respectively. The predictors of the first hospitalization regardless of its cause were: medium (HR 2.03(1.27–3.24); p = 0.0028) and low (HR 2.42(1.55–3.79); p < 0.0001) socioeconomic status, serosal (HR 1.32(1.07–1.62); p = 0.0074) and renal (HR 1.50(1.23–1.82); p < 0.0001) involvement. Antimalarial (AM) use (HR 0.61(0.50–0.74); p < 0.0001) and achieving remission (HR 0.80(0.65–0.97); p = 0.0300) were negative predictors.
Conclusions
The first hospitalization was associated with worse socioeconomic status and serosal and renal involvement. Conversely, AM use and achieving remission were associated with a lower risk of hospitalizations.
Introduction
Systemic lupus erythematosus (SLE) is a chronic multisystemic disease that has diverse clinical manifestations. Although the survival rate of patients with SLE has improved since the 1950s due to advances in diagnosis and therapy, morbidity-mortality remain high compared with that of the general population.1–3
SLE patients experience frequent hospitalizations associated with several factors, including disease activity, infections, adverse drug reactions, and comorbidities. Hospitalizations not only reflect the severity of the disease, but also limit the patient’s social and economic activities, contributing to further reduce the patients’ health-related quality of life (HRQoL).4–7
The positive impact of achieving remission or Low Disease Activity State (LDAS) in lupus patients has been studied previously. The Grupo Latinoamericano de Estudio del Lupus (GLADEL) cohort,8,9 the Lupus in Minority populations, Nature versus nurture (LUMINA) 10 and the Hopkins Lupus cohorts 11 have shown that patients who achieve remission during their disease course accrue less damage.
The relationship between achieving remission or LDAS and hospitalizations has been described by Reátegui-Sokolova et al 4 in the Almenara Lupus Cohort (a Peruvian prevalent lupus cohort), resulting in a diminished hospitalization rate.
The aim of this study is to identify the predictive and associated factors of first hospitalization and the main causes of hospitalizations in lupus patients from a Latin American (LA) cohort.
Methods
GLADEL is an observational, multiethnic, longitudinal inception cohort study started in 1997 and constituted by patients from 34 centers from nine Latin American countries under local institutional review boards’ regulations and the Declaration of Helsinki’s guidelines. 12 The first patients were enrolled in October 1997; to insure their recent disease onset they could only had been included if the diagnosis of SLE had been made after 1 January 1996, either by a rheumatologist or by a qualified internist with experience in SLE. Fulfillment of 4 1982 ACR 13 SLE criteria at the time of enrollment was not mandatory; nevertheless, 95.9% of the patients met ≥4 criteria during the follow-up period. Patients included in this cohort had to have a disease duration ≤24 months.
The first hospitalization after entry into the cohort during these patients’ follow-up due to either SLE disease activity and/or infection was examined; other causes, which constituted less than 1% of them, were not included in this analysis.
Socioeconomic demographic variables included are age at SLE diagnosis, gender, ethnicity [Caucasian, Mestizo, and African Latin American (ALA)], residence (rural vs urban), time to diagnosis (the time elapsing from when a patient met the first ACR criterion to SLE diagnosis), socioeconomic status (SES) (by the Graffar’s method), medical insurance (full vs partial/no coverage), and years of education.
The variables included were: previous hospitalizations for SLE (before entry into the cohort), cumulative ACR and non-ACR clinical manifestations, immunological variables, disease activity [SLE Disease Activity Index (SLEDAI)] 14 and damage accrual [Systemic Lupus International Collaborating Clinics/American College of Rheumatology (SLICC/ACR) Damage Index (SDI)] at the baseline visit (1 year after entry into the cohort) and at the last visit. 15
Renal involvement was defined as the presence of any of the following: persistent proteinuria greater than 0.5 g/day on two or more occasions or red or cellular casts or histologically (renal biopsy compatible with LN histopathology classes II, III, IV, V according to the WHO). Neurologic involvement was defined as the presence of any of the following: headache, seizures, longitudinal and transverse myelitis, peripheral neuropathy, optic neuritis, cranial nerve involvement, stroke or psychosis.
Therapeutic variables included are glucocorticoid and antimalarial (AM) use. Clinical and therapeutic variables were those occurring at baseline, prior to the first hospitalization.
Based on the definitions of remission in SLE (DORIS) framework, 16 remission on treatment was defined as a SLEDAI (excluding serology) of 0, prednisone ≤5 mg/day and maintenance treatment with immunosuppressants. 8 LDAS was defined as a SLEDAI ≤4 with no SLEDAI scores for renal, central nervous system, serositis, vasculitis, and constitutional components, no increase in any SLEDAI component since the previous visit, and prednisone dose ≤7.5 mg/day. Immunosuppressants at maintenance doses were allowed for LDAS and AM were allowed in both groups.
Statistical analyses
Patient characteristics were compared between the two groups: hospitalizations versus no hospitalizations due to SLE (activity, infections or both). Categorical variables were examined by the Chi-square test and continuous variables by the Kruskal–Wallis test; categorical variables are presented as frequencies and percentages while continuous variables are presented as medians and their interquartile ranges (IQRs).
Univariable and multivariable Cox regression models were used to study time to first hospitalization regardless of its cause. Univariable and multivariable logistic regression analysis were used to study the associated factors of hospitalization due to disease activity and infections but hospitalizations due to both were excluded. Disease activity state, SDI and AM use were evaluated as time-dependent covariates. Potential confounders of hospitalization included sociodemographic factors and the baseline SDI; previous hospitalizations (before entry into the cohort) and AM use and were examined at the same visit as disease activity state. A multivariable model was built by selecting covariates using a backward elimination procedure. A probability value less than 0.05 was considered significant. Statistical analyses were performed using SAS software, version 9.1.3 (SAS Institute, Cary, NC, USA).
Results
A total of 1480 patients were included in the GLADEL cohort; 1341 individuals with sufficient data on the variables of interest were included in this analysis; of them, 1200 (89.5%) were women. Their median and interquartile range (IQR) age at diagnosis were 27 (20–37) years and their median and IQR follow up time were 27.5 (4.7–62.2) months. A total of 456 (34.0%) patients were hospitalized; 344 (75.4%), 85 (18.6%) and 27 (5.9%) for disease activity, infections, or both, respectively, as depicted in Figure 1. The most common infection sites that led to hospitalizations were respiratory and cutaneous. Reasons for the first hospitalization.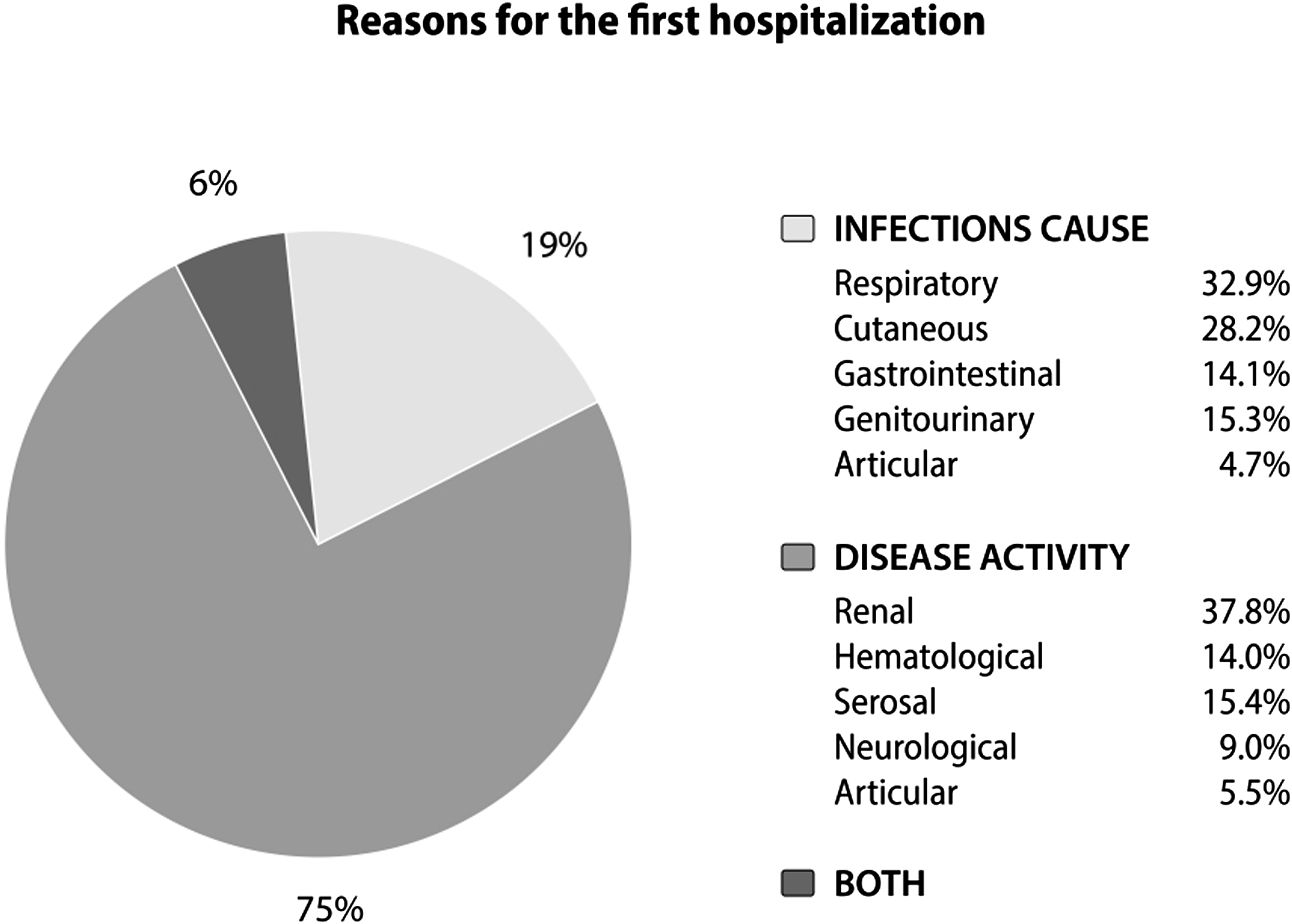
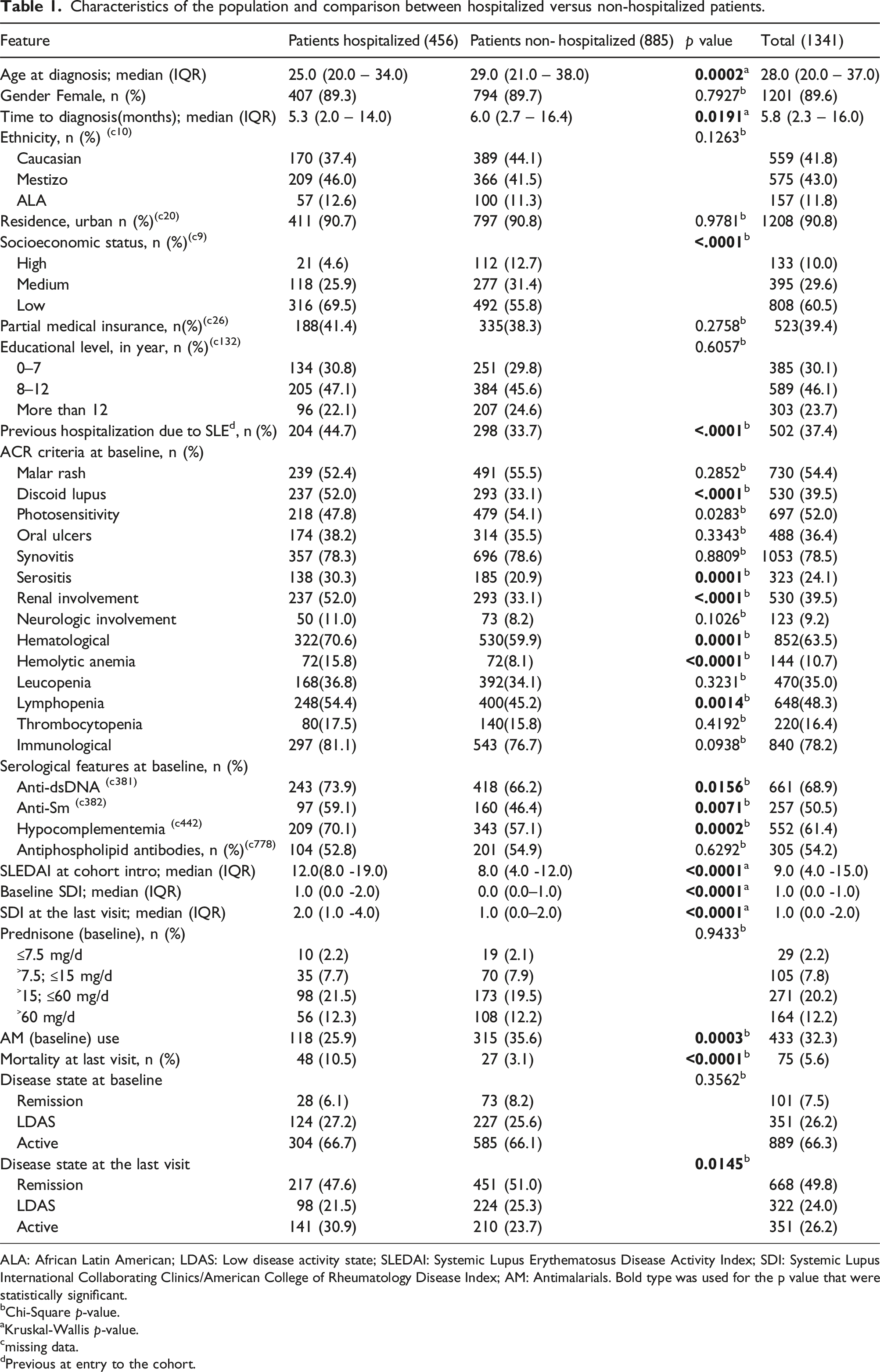
Characteristics of the population and comparison between hospitalized versus non-hospitalized patients.
ALA: African Latin American; LDAS: Low disease activity state; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; SDI: Systemic Lupus International Collaborating Clinics/American College of Rheumatology Disease Index; AM: Antimalarials. Bold type was used for the p value that were statistically significant.
bChi-Square p-value.
aKruskal-Wallis p-value.
cmissing data.
dPrevious at entry to the cohort.
In relation to the clinical variables, the presence of discoid lupus (52.0% vs 33.1%; p < 0.0001), serosal (30.3% vs 20.9; p = 0.0001), renal (52.0% vs 33.1%; p < 0.0001), hematological (70.6% vs 59.9%; p = 0.0001) and serological involvement (70.1% vs 57.1%; p = 0.0002) were more frequent at baseline in the hospitalized versus the non-hospitalized patients. Hospitalized patients also had a higher baseline SLEDAI (12.0 vs 8.0; p < 0.0001), as well as a higher SDI at baseline (1.0 vs 0.0; p < 0.0001) and at the end of follow-up (2.0 vs 1.0; p < 0.0001); they also experienced a higher mortality (10.5% vs 3.1; p < 0.0001) and a lower AM use before the baseline visit (25.9% vs 35.6%; p = 0.0003) compared with non-hospitalized patients. In the same way, these patients had reached remission (47.6% vs 51.0; p = 0.0145) and LDAS (21.5 vs 25.3; p = 0.0145) less frequently at the end of the follow-up period than the non-hospitalized patients.
Predictive factors of the first hospitalization in SLE patients (n = 1341).
LDAS: low disease activity state; ALA: Afro–Latin American; SDI: SLICC/ACR damage index; HR: Hazard ratio; 95% CI: 95% confidence interval; Ref: reference group. Bold type was used for the p value that were statistically significant.
aIncrease on per 1 unit.
bTime–dependent covariates.
cPrevious at entry to the cohort.
dAt baseline.
ehighest dose.
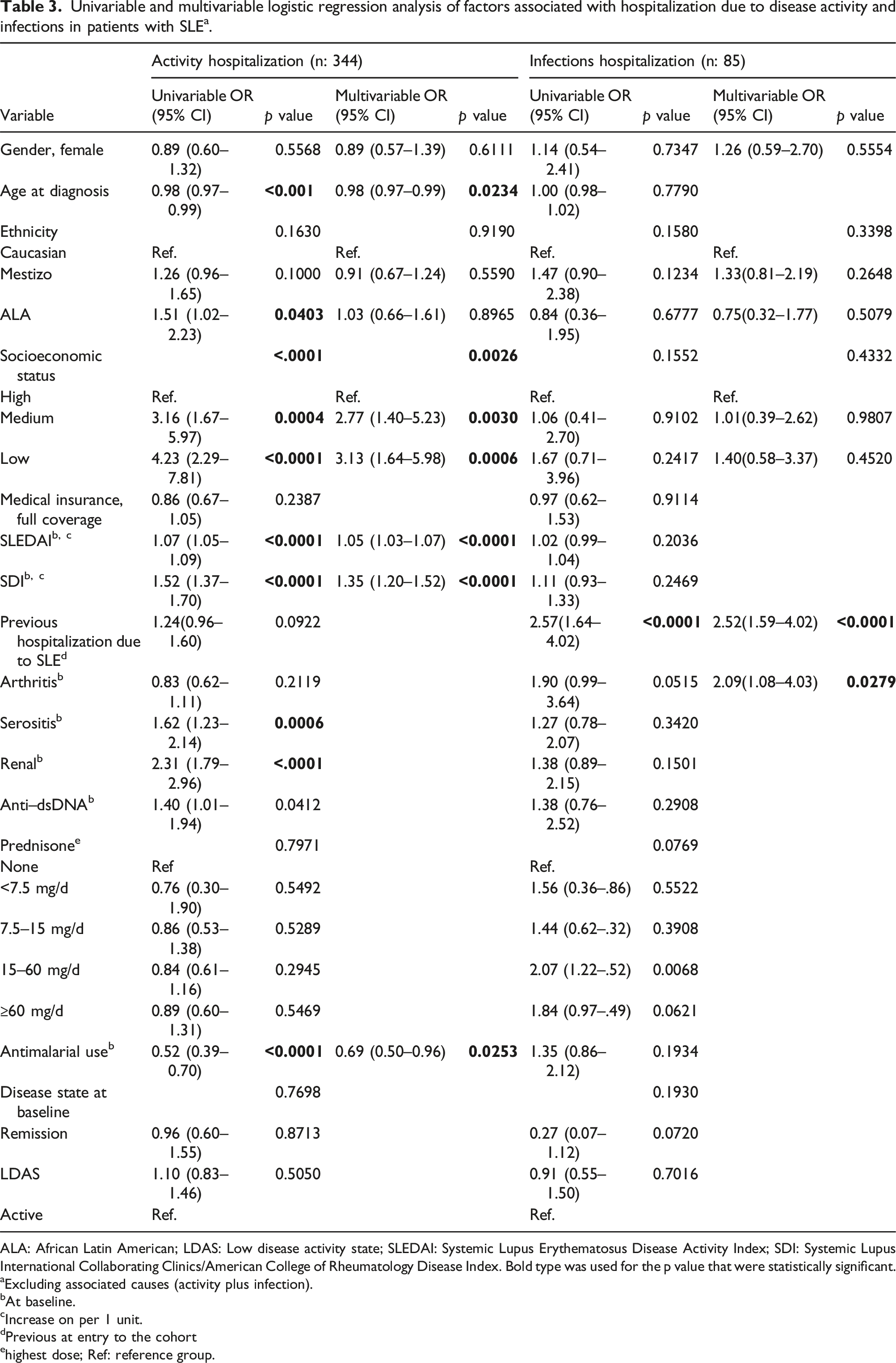
Univariable and multivariable logistic regression analysis of factors associated with hospitalization due to disease activity and infections in patients with SLE a .
ALA: African Latin American; LDAS: Low disease activity state; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; SDI: Systemic Lupus International Collaborating Clinics/American College of Rheumatology Disease Index. Bold type was used for the p value that were statistically significant.
aExcluding associated causes (activity plus infection).
bAt baseline.
cIncrease on per 1 unit.
dPrevious at entry to the cohort
ehighest dose; Ref: reference group.
In terms of infections, the variables associated with the first hospitalization that maintained statistical significance in the multivariable analysis were: previous hospitalizations (before entry into the cohort) due to SLE (OR 2.52(1.59–4.02); p < 0.0001) and the presence of arthritis at baseline (OR 2.09(1.08–4.03); p = 0.0279).
Discussion
This study describes the causes of the first hospitalization in lupus patients, their associated factors and highlights the importance of achieving remission as well as of AM use as being protective factors of the first hospitalization.
In relation to the causes, disease activity was the most frequent cause followed by infections, as has been described in several studies.1,2,17–20 The active organs that required hospitalizations were renal, followed by hematological and serosal involvements; these finding are similar to those from other studies, particularly in terms of renal involvement,7,8,17,18 but differ from the Hopkins Lupus Cohort data, where neurological involvement was the most frequent cause of hospitalization. 20 This difference could be due to limitations in determining SLE as the cause of the neurological manifestations in these patients. On the other hand, and in concordance with other studies,1,2,17,18,21 the most common infection sites that led to hospitalizations were respiratory and cutaneous.
Hospitalized patients had a shorter time to diagnosis, were younger, and had a lower SES. These sociodemographic variables have already been described in the GLADEL cohort as factors of a worse disease course.12,22–26 In relation to the clinical variables, hospitalized patients presented a higher frequency of renal, serological and serosal involvement, higher SLEDAI and SDI at baseline and at the end of the follow-up which is similar to other studies.19,20,23 They use, however, less AM. The beneficial effect of AM has been extensively studied and GLADEL27–31 has demonstrated the impact of AM use on different outcomes, such as the onset of renal compromise and associated accrual damage.
In relation to the disease state, hospitalized patients were less likely to have achieved LDAS and remission at the end of follow-up. The treat-to-target (T2T) strategy for SLE has been proposed by experts to optimize the outcomes of these patients, such as damage accumulation, survival and use of health resources. Previous studies have shown that achieving remission or LDAS is associated with lower rates of damage accrual and of mortality.4,10,11
Factors associated with the first hospitalization due to activity were lower SES, SLEDAI, and SDI at baseline. In the same way, the Lupus Canadian cohort and the Hopkins Lupus Cohort suggested hospitalizations were associated with disease activity and comorbidities, among other variables.19,20
This study, as well as several other publications, highlight that AM use reduces the risk of hospitalizations.6,17 This effect of AM adds to others such as reducing disease activity, preventing lupus flares, lowering damage accrual, and improving survival. Despite the low percentage of AM use in this study, its benefits were demonstrated.
The most relevant risk factor for the first hospitalization due to infections was a history of previous hospitalizations for lupus before cohort entry. This may be associated with the use of a more aggressive treatment, with the consequent occurrence of an infection secondary to immunosuppression.
In the multivariable Cox regression analysis, independent predictors of the first hospitalization regardless of the cause were: lower SES, renal and serosal involvement. Conversely, AM use and having reached remission prior to the hospitalization were protective factors.4,6,17 These observations are relevant to the management of patients with lupus; that despite presenting an unfavorable socioeconomic condition and a severe disease, AM use and the attempt made by physicians to achieve remission will have a favorable impact in the prognosis of our patients.
This study has strengths and limitations. Within the first, it is a Latin American multicenter study that reflects the different factors involved in the hospitalizations of our patients. GLADEL represents a diverse patient population from various countries and ethnicities, providing a good representation of SLE patients, the natural history of the disease, treatment burden, and use of medical resource utilization (including hospitalizations) in the real life. The main limitations were some missing data, not having precise data about the hospitalizations, as well as the fact, that the therapeutic strategies used do not reflect current practices, in which T2T is prioritized; a mean follow-up time of only 5 years is also highlighted.
In conclusion, the first hospitalization in LA patients with diagnosis of lupus were associated with socioeconomic disadvantages and renal and serosal involvement. Conversely, reaching remission and AM use are goals that must be prioritized. Likewise, new studies are necessary since the introduction of new therapies for lupus and the changes in the paradigms in the management of these patients.
Footnotes
Acknowledgements
To members of Grupo Latino Americano De Estudio del Lupus (GLADEL), Study Group of PANLAR, for their participation.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AO, US, EA and FZ are Janssen Pharmaceutical Companies employees.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript received financial support for their publication from Janssen Pharmaceutical Companies.
Contributorship
All of the listed authors have contributed to collecting data and reviewing the manuscript.
Ethical statement
ORCID iDs
Data availability statement
To be considered upon request.