
Abstract
Objective
For the majority of patients with lupus nephritis-related end-stage kidney disease (LN-ESKD), kidney transplant is associated with better outcomes than dialysis. Access to kidney transplant requires an initial referral to a transplant center and medical evaluation prior to waitlisting. The study’s objective was to examine access to these early steps in the kidney transplant process among patients with LN-ESKD.
Methods
Adults who began treatment for ESKD in the Southeast, Northeast, New York, or Ohio River Valley U.S. regions from 1/1/2012 to 12/31/2019, followed through 6/30/2021, were identified from the United States Renal Data System. Referral and evaluation start data were collected from 28 of 48 transplant centers across these regions. The exposure was primary cause of ESKD (LN-ESKD vs other-ESKD). The outcomes were referral and evaluation start at a transplant center. Cox models quantified the association between LN-ESKD (vs other-ESKD) and referral and evaluation start.
Results
Among 192,318 patients initiating treatment for ESKD, 0.4% had LN-ESKD. Over half (58%) of LN-ESKD patients were referred before study end, and among those referred, 66% started the evaluation. In adjusted analyses, patients with LN-ESKD were referred (HR: 1.09, 95% CI: 0.99, 1.19) and started the transplant evaluation (HR: 1.13, 95% CI: 1.00, 1.28) at a higher rate than patients with other-ESKD. Among referred patients with LN-ESKD, the median time from ESKD start to referral was 2.9 months (IQR: <1 to 11.7 months), which is similar to patients with other-ESKD (median 2.6 months, IQR: <1 to 8.8 months).
Conclusions
Among incident patients with ESKD, having a primary diagnosis of LN-ESKD versus other-ESKD is associated with higher rates of early transplant access outcomes. Despite this, patients with LN-ESKD (vs other-ESKD) are less likely to be preemptively referred (i.e., referred prior to ESKD start) for kidney transplant. While providers may no longer be delaying the early steps in the kidney transplantation process among this patient population, there is still room for improvement in the rates of preemptive referral. Access to kidney transplant referral prior to ESKD could result in increased transplant rates and better transplant outcomes for patients with LN-ESKD.
Introduction
The estimated risk of progressing to LN-associated end-stage kidney disease (LN-ESKD) within 5, 10, and 15 years following systemic lupus erythematosus (SLE) diagnosis is 11%, 17%, and 22%, respectively. 1 Despite improvements and advances in immunosuppressant therapies for patients with SLE, there has been no change in the progression to LN-ESKD since the 2000s 1 Once patients reach ESKD, there are only two primary treatment options to prolong life: dialysis and kidney transplantation.
In prior decades, rheumatologists 2 and nephrologists 3 favored a clinical approach of starting new patients with LN-ESKD on dialysis until the SLE became quiescent in the immunosuppressive state of ESKD out of concern for increased risk of recurrent LN post-transplant. 4 However, studies conducted more recently report that due to advancements in post-transplant immunosuppressive therapies, only 2.5%–10.5% of patients with LN-ESKD will experience recurrent LN post-transplant.5,6 Additionally, in a recent national study examining post-transplant outcomes among patients with LN-ESKD waitlisted for kidney transplant, authors reported a survival benefit associated with patients who received a kidney transplant compared to those that remained on the waitlist. 7 Finally, recommendations to intentionally delay kidney transplant are not standardized and are in direct contrast to literature for all-cause ESKD, which suggests a shorter time from ESKD diagnosis to kidney transplant leads to better post-transplant outcomes.8,9 A more recent study reported an association between longer wait times to transplant with equivalent or worse graft outcomes among a national cohort of LN-ESKD transplant recipients. 10
As evidenced by a large body of literature, there are longstanding inequities and barriers in access to each step in the kidney transplant process, including referral, start and completion of evaluation, and placement on the national waiting list.11–14 Data on the early steps in the kidney transplant process are lacking because patient referral for a kidney transplant and start of a medical evaluation at a transplant center are not captured in national surveillance data. A study examining variability in kidney transplant referral among incident adult patients with ESKD across dialysis facilities in the Southeastern U.S. reported that only 34% of patients were referred within 1 year of starting dialysis, and 48% of those referred patients started the transplant evaluation within 6 months of referral. 15 Previous studies of patients with LN-ESKD only included waitlisting, receipt of kidney transplant, and/or post-transplant outcomes as their primary endpoints, but this work does not provide insight into the larger groups of patients that do not make it to these downstream steps in the kidney transplant process. The purpose of this study was to examine how referral for kidney transplant and start of the evaluation at a transplant center among patients with LN-ESKD compared to patients with ESKD unrelated to LN.
Materials and methods
Data sources and study population
Patient data were obtained from the United States Renal Data System (USRDS), a publicly available national database that includes information on all treated patients with kidney failure in the United States. USRDS collects demographic, clinical, and socioeconomic data at the time of ESKD start (defined as the date of first ESKD service) using the Centers for Medicare & Medicaid Services (CMS) 2728 form. 16 Patient-level referral data from the novel Early Steps to Transplant Access Registry (E-STAR) were collected from 28 of 48 transplant centers across four regions in the U.S. (Southeast, Northeast, New York, and Ohio River Valley) and linked with USRDS data, as previously described. 15 Data on characteristics of patients’ 5-digit ZIP code were obtained from the 2017-2021 American Community Survey and linked to USRDS data by patient residential ZIP code.
To construct the incident study cohort, we included all patients who initiated treatment for ESKD between January 1, 2012 (Southeast region) or January 1, 2014 (Northeast, New York, and Ohio River Valley regions) and December 31, 2019, and followed through December 31, 2020 (N = 218,669). There were 192,318 patients with incident ESKD eligible for merging with E-STAR after excluding patients with a missing facility ID (N = 3671); patients who did not receive dialysis or a preemptive transplant as their first treatment (N = 21,222), and patients who were <18 years old (N = 1458) were further excluded (Figure 1). Data merge and cohort selection to examine the relationship between lupus nephritis-related end-stage kidney disease (versus end-stage kidney disease unrelated to lupus nephritis) and referral and evaluation start for kidney transplantation.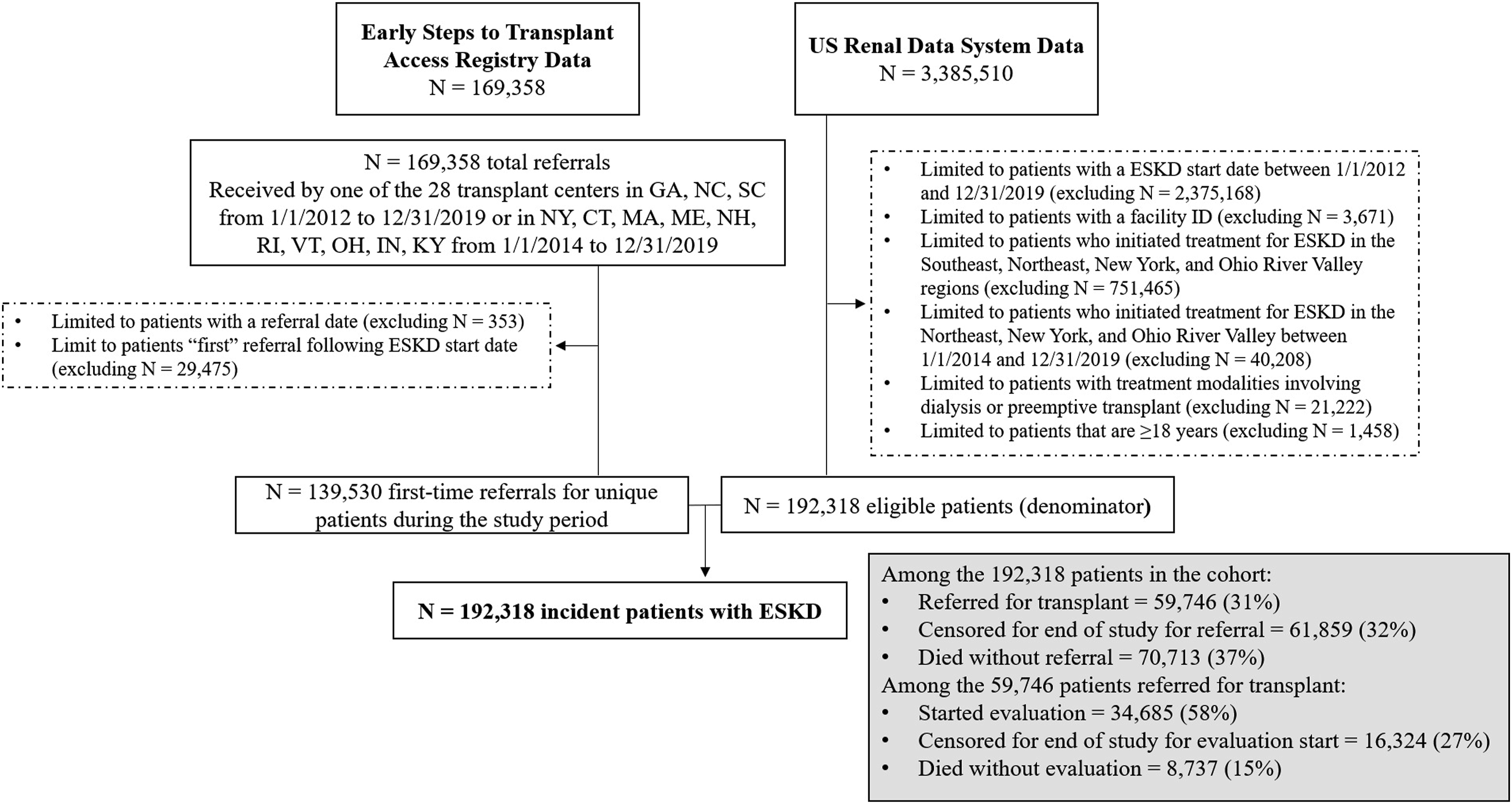
Outcome, exposure, and study variables
The primary outcome was time from ESKD start to referral for kidney transplantation. Referral to a transplant center was defined as the date in which a transplant center received a referral form for a patient (including referrals from dialysis facilities, chronic kidney disease clinics, and self-referrals). In the event that a patient was referred more than once during the study period, the patient’s first referral following ESKD start was used as the referral date. We examined evaluation start, which was defined as the date when a patient physically began a required component of the transplant evaluation, as a secondary outcome. Each transplant center defined what their center-specific classification of starting the evaluation was and this included the first visit to the transplant center or satellite clinic for a medical appointment, or attendance of a required transplant education course. Evaluation start was examined among all patients who were referred as a referral is required for patients to initiate the evaluation process.
The primary exposure was provider attributed primary cause of ESKD, as documented on the CMS-2728 form within the USRDS. The exposure was categorized as both a dichotomous [LN-ESKD (ICD-9/ICD-10 codes included 6954Z, 7100, 7011E, and 7100Z) versus other-ESKD: includes all other ICD-9/ICD-10 codes listed as assigned primary cause of kidney failure] and categorical (diabetes, hypertension, glomerulonephritis, LN, other cause, and unknown cause) variable.
Patient-level characteristics were obtained from USRDS at the time of ESKD start. Demographics included age, sex, race, and ethnicity. Clinical characteristics included receipt of nephrology care prior to ESKD start (yes, no, unknown), documentation that the patient was informed of kidney transplant as a treatment option, initial dialysis modality, comorbidities (body mass index ≥35 kg/m2, congestive heart failure, atherosclerotic heart disease, cardiovascular disease, peripheral vascular disease, chronic obstructive pulmonary disease, and active malignancy), lifestyle behaviors (tobacco use and alcohol dependence), and year of incident ESKD. Patient’s primary source of health insurance at ESKD start was categorized as Medicaid, Medicare, employer group coverage, other coverage, or no coverage. U.S. region of treatment was categorized as Southeast, Northeast, New York, and Ohio River Valley. At the neighborhood ZIP code level, socioeconomic indicators included the percentage of residents living in a ZIP code where ≥20% of residents live below the federal poverty line, percentage of Black residents, percentage of Hispanic residents, and percentage of residents with a high school degree.
Statistical analysis
We examined characteristics of our study population overall, by primary cause of ESKD, and by referral and evaluation start status. A small number of patients were missing at least one covariate (N = 5,777, 3%); thus, we conducted a complete case analysis. The proportional hazards (PH) assumption was tested for all outcomes using log-log survival curves and found no gross violation. Crude and multivariable cause-specific Cox models were used to quantify the association between LN-ESKD (vs other-ESKD and diabetes, hypertension, glomerulonephritis, other cause, and unknown cause) and time to referral or evaluation start for kidney transplantation. Patients were censored for death or end of follow-up period (December 31, 2020 for referral and June 30, 2021 for evaluation start). Patients with negative follow-up time from ESKD start to referral (preemptively referred) and/or referral to evaluation start were assigned a follow-up time of 1 day for both referral and evaluation start. Patients treated at the same dialysis facility may have similar referral and evaluation start access. Therefore, robust sandwich variance estimators were used to account for potential clustering of the outcome within dialysis facilities. Multivariable models were adjusted for demographic, clinical, and socioeconomic characteristics. Variables with known associations between primary cause of ESKD and early access to kidney transplantation were included in the multivariable models. The final multivariable models for referral were adjusted for categorical age, sex assigned at birth, race, ethnicity, body mass index ≥35 kg/m2, cardiovascular disease, initial treatment modality, primary source of health insurance at ESKD start, access to nephrology care prior to ESKD start, incident year of ESKD, and U.S. region of treatment for ESKD. The evaluation start model was adjusted for the same variables as the referral model with the addition of congestive heart failure. Finally, age stratified (age dichotomized as <50 and ≥50 years) models were also fit for the referral outcome, given the difference in median age between patients with LN-ESKD and other-ESKD.
In a subanalysis, descriptive statistics were performed to describe baseline characteristics of patients with LN-ESKD who were preemptively referred for kidney transplant. A patient was considered to have a preemptive referral if the date of the first referral occurred prior to the patient’s ESKD start date.
Sensitivity analyses
Several sensitivity analyses were conducted for the outcome of referral. Patients >80 years of age with ESKD rarely receive a kidney transplant due to age restrictions outlined by transplant center eligibility criteria and are thus, very unlikely to be referred for kidney transplant. We performed the same Cox PH models excluding patients >80 years from the dataset, and excluding patients who were referred, waitlisted, or transplanted prior to starting dialysis because the events occurred prior to the follow-up period.
All analyses were done using SAS version 9.4 (SAS Institute, Cary, NC). The Emory University IRB approved this study (IRB00113572) and waived the requirement for written informed consent.
Results
Baseline characteristics by primary cause of ESKD
Characteristics of adult ESKD patients who initiated treatment for ESKD in the Southeast, New York, Northeast, and Ohio River Valley regions in the United States at time of ESKD start, 2012–2019 (Southeast) and 2014–2019 (New York, Northeast, and Ohio River Valley), overall and by provider attributed primary cause of ESKD (N = 192,318).
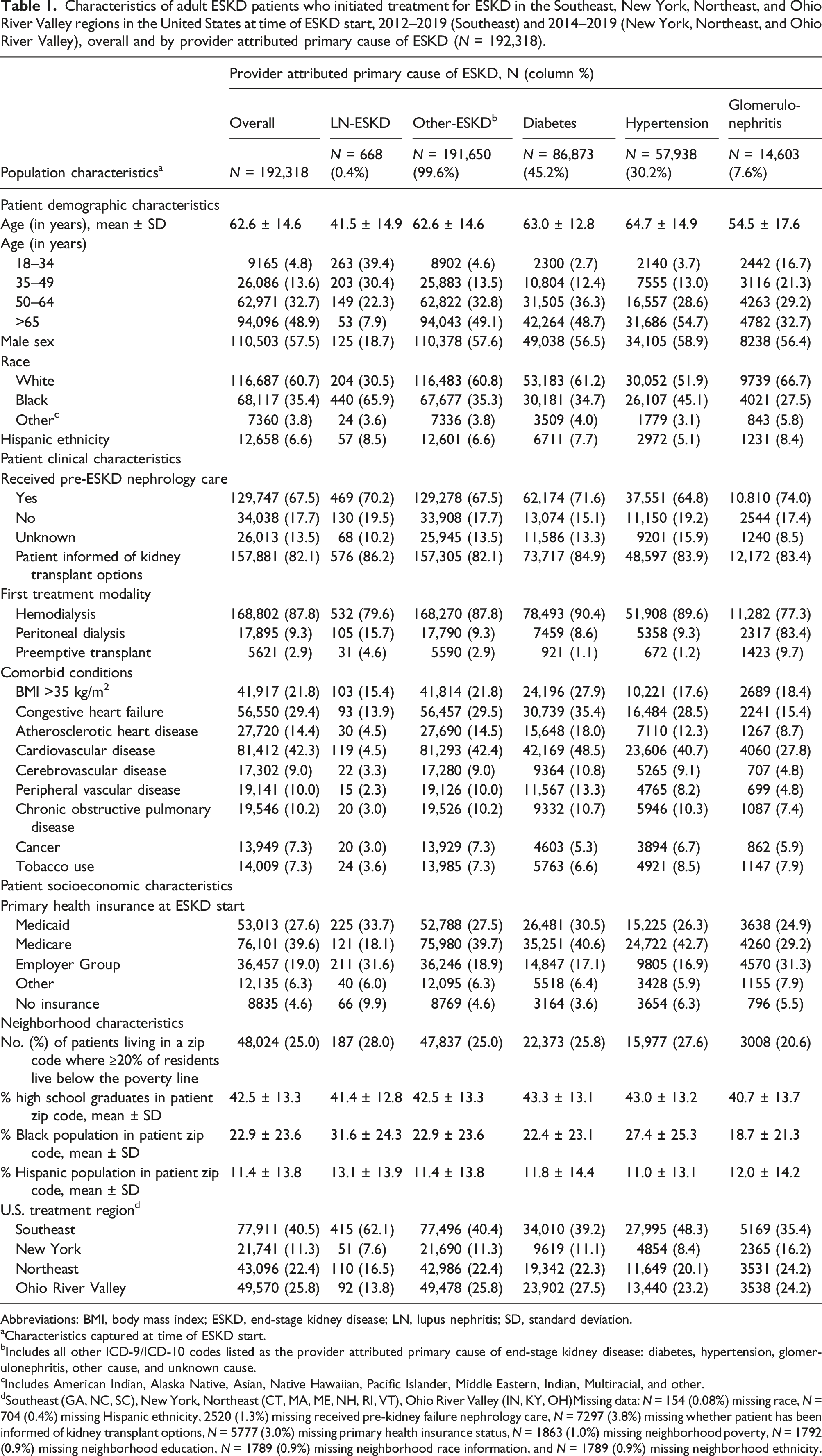
Abbreviations: BMI, body mass index; ESKD, end-stage kidney disease; LN, lupus nephritis; SD, standard deviation.
aCharacteristics captured at time of ESKD start.
bIncludes all other ICD-9/ICD-10 codes listed as the provider attributed primary cause of end-stage kidney disease: diabetes, hypertension, glomerulonephritis, other cause, and unknown cause.
cIncludes American Indian, Alaska Native, Asian, Native Hawaiian, Pacific Islander, Middle Eastern, Indian, Multiracial, and other.
dSoutheast (GA, NC, SC), New York, Northeast (CT, MA, ME, NH, RI, VT), Ohio River Valley (IN, KY, OH)Missing data: N = 154 (0.08%) missing race, N = 704 (0.4%) missing Hispanic ethnicity, 2520 (1.3%) missing received pre-kidney failure nephrology care, N = 7297 (3.8%) missing whether patient has been informed of kidney transplant options, N = 5777 (3.0%) missing primary health insurance status, N = 1863 (1.0%) missing neighborhood poverty, N = 1792 (0.9%) missing neighborhood education, N = 1789 (0.9%) missing neighborhood race information, and N = 1789 (0.9%) missing neighborhood ethnicity.
Primary cause of ESKD and referral for a kidney transplant
A total of 59,746 (31%) were referred for transplant during the study period, including 58% of patients with LN-ESKD and 31% of patients with other-ESKD. Among those referred, the median time from ESKD start to referral was 2.6 months (IQR: <1 month–8.8 months), with a longer median time to referral for patients with LN-ESKD (median: 2.9 months, IQR: <1 month–11.7 months) versus patients with other-ESKD (median 2.6 months, IQR: <1 month–8.8 months). A total of 70,713 (37%) patients died during the follow-up period for referral, with a smaller proportion of patients with LN-ESKD (18%) dying compared to patients with other-ESKD (37%) (Supplemental Table 1). Reflective of the demographics of the underlying SLE patient population, referred patients with LN-ESKD were on average younger (39 vs 55 years) than patients with other-ESKD, and more likely to be female (82% vs 60%), Black (76% vs 47%), and Hispanic (7% vs 5%). Referred patients with LN-ESKD were less likely to have each of the eight assessed comorbidities but were more likely to have Medicaid as their primary health insurance (35% vs 26%) and live in a high poverty neighborhood (32% vs 26%) (Supplemental Table 2).
Cause-specific modeling results for the association of provider attributed primary cause of ESKD with time to referral for kidney transplant in 29 transplant centers among incident ESKD patients treated across 13 states in the Northeast, Southeast, and Ohio River Valley regions of the United States: 2014–2018, followed through 2020 (N = 192,318).
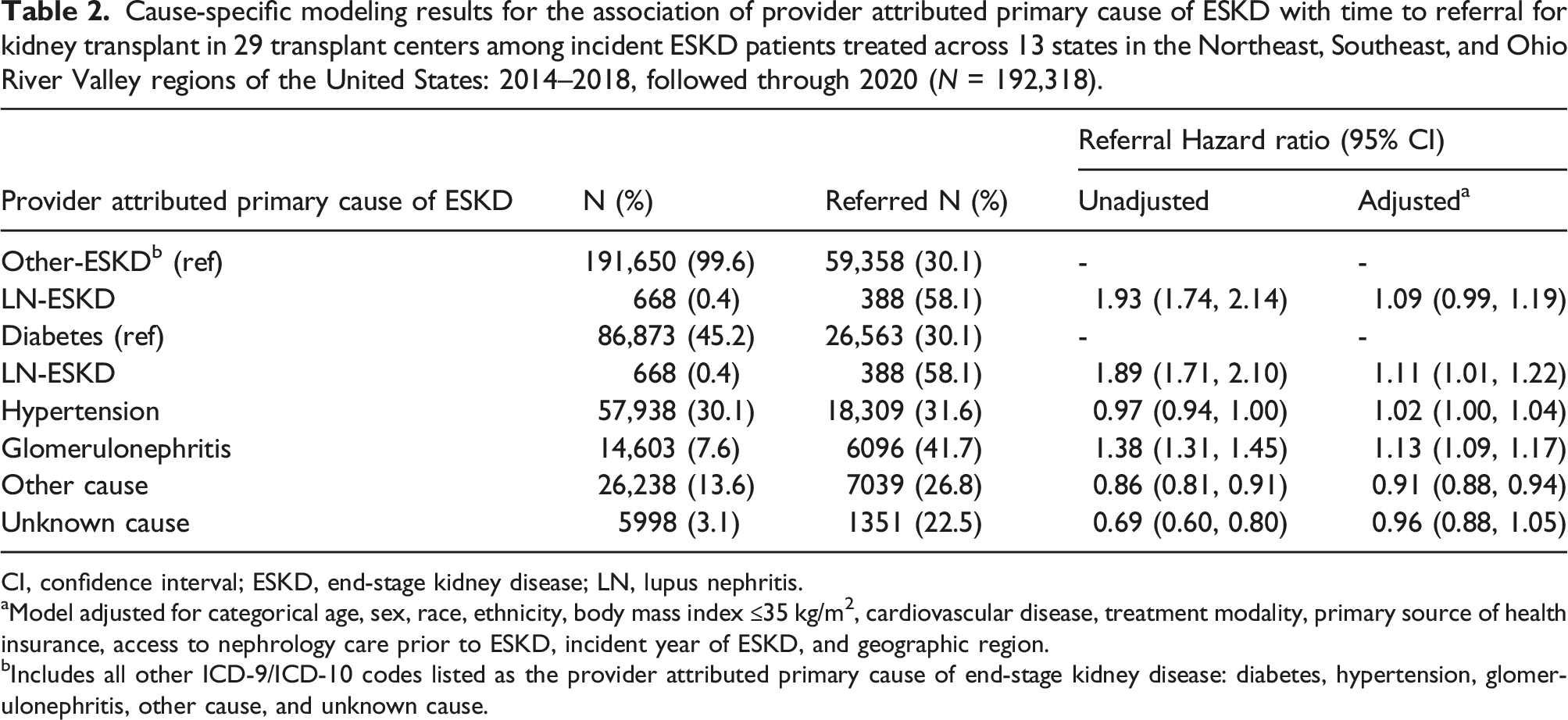
CI, confidence interval; ESKD, end-stage kidney disease; LN, lupus nephritis.
aModel adjusted for categorical age, sex, race, ethnicity, body mass index ≤35 kg/m2, cardiovascular disease, treatment modality, primary source of health insurance, access to nephrology care prior to ESKD, incident year of ESKD, and geographic region.
bIncludes all other ICD-9/ICD-10 codes listed as the provider attributed primary cause of end-stage kidney disease: diabetes, hypertension, glomerulonephritis, other cause, and unknown cause.
Cause-specific modeling results stratified by age for the association of provider attributed primary cause of ESKD with time to referral for kidney transplant in 29 transplant centers among incident ESKD patients treated across 13 states in the Northeast, Southeast, and Ohio River Valley regions of the United States: 2014–2018, followed through 2020 (N = 192,318).
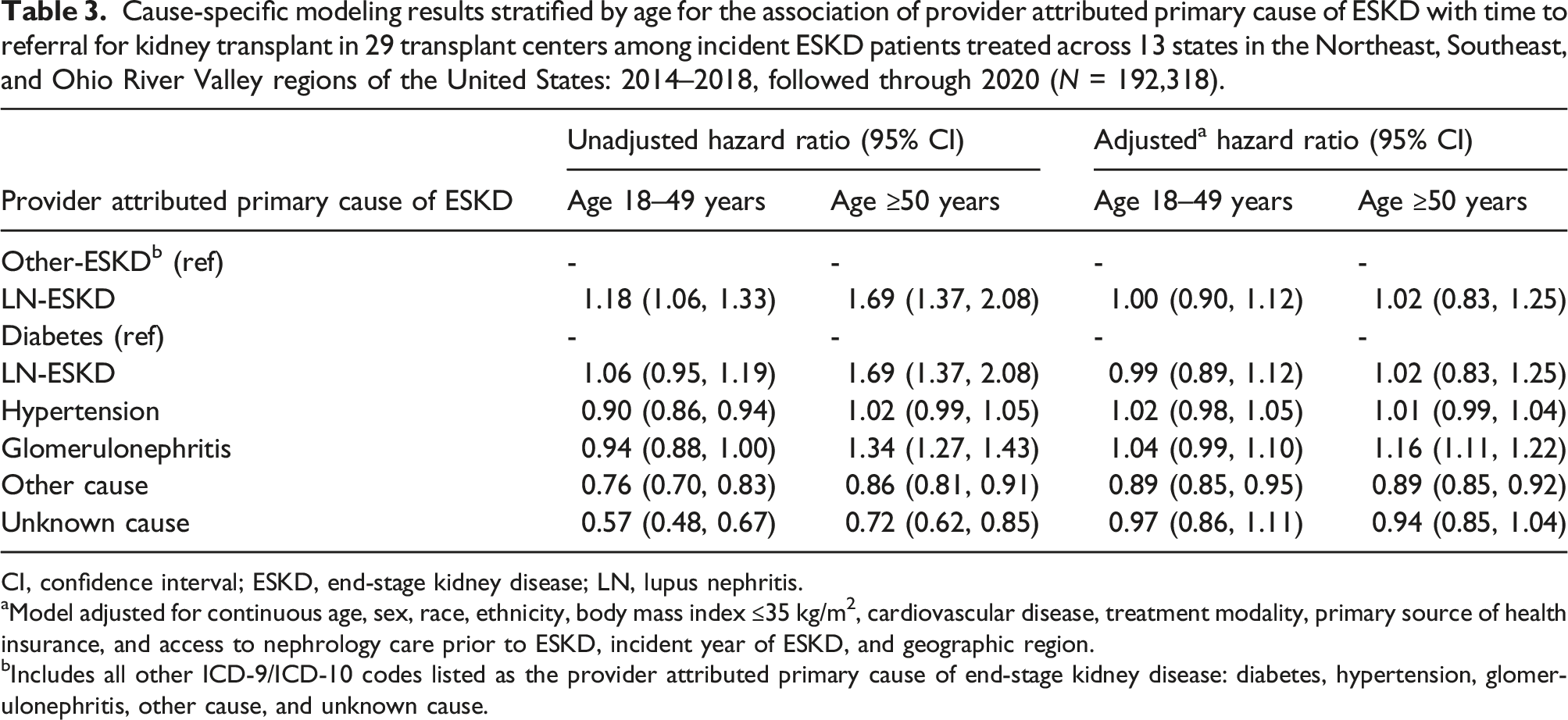
CI, confidence interval; ESKD, end-stage kidney disease; LN, lupus nephritis.
aModel adjusted for continuous age, sex, race, ethnicity, body mass index ≤35 kg/m2, cardiovascular disease, treatment modality, primary source of health insurance, and access to nephrology care prior to ESKD, incident year of ESKD, and geographic region.
bIncludes all other ICD-9/ICD-10 codes listed as the provider attributed primary cause of end-stage kidney disease: diabetes, hypertension, glomerulonephritis, other cause, and unknown cause.
In a subanalysis, we descriptively compared the characteristics of patients with LN-ESKD who were preemptively referred for kidney transplant with patients with LN-ESKD who were referred after starting dialysis. Among the N = 388 patients with LN-ESKD who were referred for kidney transplant, 23% (N = 90) were preemptively referred, with an older mean age of 43 years (SD: 14.5) compared to 37 years (SD: 12.8) among patients with LN-ESKD referred after starting dialysis. Similar to patients with LN-ESKD referred after starting dialysis, preemptively referred patients with LN-ESKD were majority female (84%) and Black (84%). Preemptively referred patients with LN-ESKD differed from patients with LN-ESKD referred after starting dialysis in that almost all of the patients were seen by a nephrologist prior to an ESKD diagnosis (89% vs 64%) and no more than 13% of patients were diagnosed with any of the examined comorbidities, including cardiovascular disease and peripheral vascular disease. Almost half of the preemptively referred patients had employer group health insurance (47% vs 39%) and resided in lower-poverty neighborhoods (78% vs 63%) compared to patients who were not preemptively referred.
Primary cause of ESKD and evaluation start at a transplant center
Cause-specific modeling results for the association of provider attributed primary cause of ESKD with time to evaluation start in 29 transplant centers among incident ESKD patients referred for kidney transplant across 13 states in the Northeast, Southeast, and Ohio River Valley regions of the United States: 2014–2018, followed through 2020 (N = 59,746).
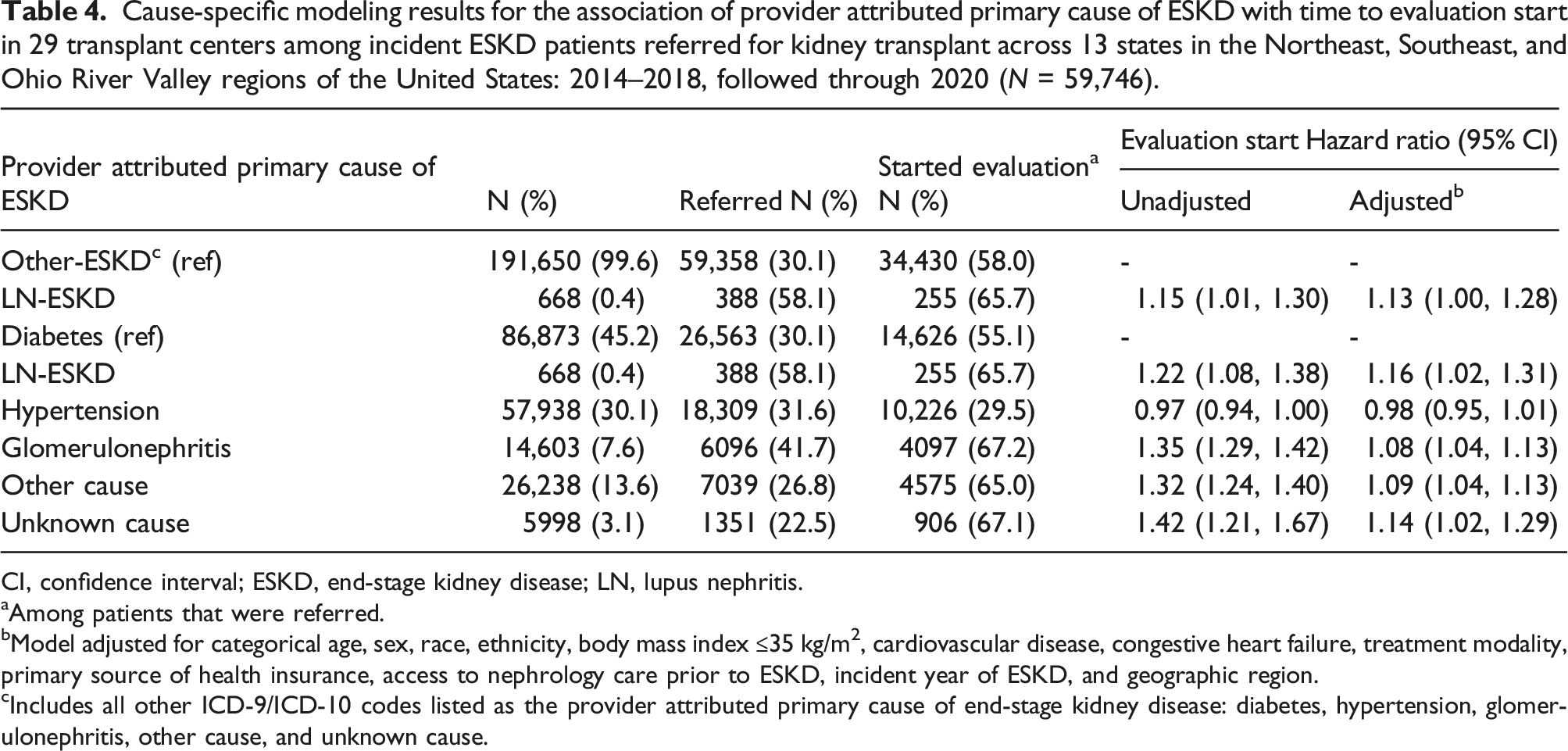
CI, confidence interval; ESKD, end-stage kidney disease; LN, lupus nephritis.
aAmong patients that were referred.
bModel adjusted for categorical age, sex, race, ethnicity, body mass index ≤35 kg/m2, cardiovascular disease, congestive heart failure, treatment modality, primary source of health insurance, access to nephrology care prior to ESKD, incident year of ESKD, and geographic region.
cIncludes all other ICD-9/ICD-10 codes listed as the provider attributed primary cause of end-stage kidney disease: diabetes, hypertension, glomerulonephritis, other cause, and unknown cause.
Discussion
Among adult patients with ESKD treated across the Southeastern, Northeastern, New York, and Ohio River Valley regions of the U.S., over half of patients with LN-ESKD were referred for kidney transplant, and, among those referred, two-thirds started the medical evaluation during the up to 8-year study period. Patients with LN-ESKD were referred to a transplant center for a medical evaluation at a higher rate compared to patients with ESKD unrelated to LN, with the exception of patients with glomerulonephritis. This association is likely driven by the younger age of the LN-ESKD patient population, as the association between LN-ESKD (vs other-ESKD) was attenuated in age stratified analyses among patients 18–49 years and ≥50 years. Among referred patients, patients with LN-ESKD were also evaluated at a transplant center at a higher rate compared to patients with ESKD unrelated to LN.
Prior to this study, access to kidney transplant among patients with LN-ESKD was only measured by outcomes downstream in the kidney transplant process, including waitlisting and receipt of a kidney transplant, which excludes the large pool of patients that experienced barriers in accessing these later steps. Early access to kidney transplantation is critically important to evaluate among all patients with ESKD but is especially relevant to patients with LN-ESKD due to prior clinical guidelines suggesting an intentional delay in pursuing kidney transplant. Historically, when patients with LN approached ESKD, the trend was for rheumatologists 2 and nephrologists 3 to start patients on hemodialysis and suspend kidney transplant in allowance for the quiescence of the underlying autoimmune processes of SLE and LN. However, recent studies demonstrated a lower risk of graft failure following recurrent LN5,6,10 secondary to advancements in immunosuppressive therapies5,6 and a lower risk of premature mortality among patients with LN-ESKD spending less time on dialysis prior to kidney transplant.7,17,18 With kidney transplant now being a well-established treatment option for patients with LN-ESKD, it is vital that a concerted effort is put forth in understanding at what point in the disease process is this younger patient population initiating first steps to transplant.
In our study population, we found that over half of patients with LN-ESKD are being referred for kidney transplant, and the likelihood of referral is comparable, specifically among patients ages 18–49 years, to patients with other causes of ESKD. There are two primary reasons why patients with LN-ESKD may be referred similarly to patients with other causes of ESKD <50 years old. Most importantly, patients with LN-ESKD are a much younger patient population compared to the general ESKD patient population, with younger patients generally deemed more appropriate candidates for kidney transplant. Additionally, patients with LN-ESKD are seen by multiple specialists due to their underlying lupus disease. Therefore, patients with LN-ESKD may have more interactions with the healthcare system, which could lead to more frequent discussions about kidney transplant as a treatment option.
We also observed that, similar to patients with other-ESKD, referred patients with LN-ESKD are, on average, referred just under 3 months after ESKD start. It is difficult to ascertain whether clinical characteristics specific to patients with LN-ESKD contributed to a provider’s decision to refer as we did not have access to data on patient lupus disease activity pre-ESKD or within the first year of being on dialysis. However, there does not appear to be a difference in timing of referral following ESKD start between patients with LN-ESKD and patients with ESKD unrelated to LN. Our findings suggest that providers may no longer be unnecessarily delaying the transplantation process in this patient population for 1–2 years, but there may be room for improvement with respect to preemptive referral. In our study, 23% of patients with LN-ESKD were preemptively referred for kidney transplant compared to 29% of patients with ESKD unrelated to LN. There is no prior work examining preemptive referral among patients with LN-ESKD, but a previous study found that only 9% of transplants among patients with LN-ESKD are preemptive, 19 while close to 20% of transplants among patients with ESKD from other causes are preemptive. 16 Additionally, in a study among patients referred for kidney transplant in the U.S. state of Georgia, 20% were preemptively referred, and Black patients were less likely to be preemptively referred than white patients. 20 With data from other studies suggesting better post-transplant outcomes among patients with LN-ESKD receiving a preemptive and early kidney transplant, it is critical that we strive to focus efforts in improving the rates of preemptive referral among patients with LN-ESKD.
Our study also found that two-thirds of referred patients with LN-ESKD started the evaluation at a transplant center, which is comparable to a multistate study of patients with ESKD in the U.S. Southeast, where 48% of referred patients with ESKD started the evalution. 15 There is a growing body of literature examining the non-medical barriers associated with starting the transplant evaluation, with public or no health insurance21–23 and inadequate kidney transplant knowledge22,24–26 being associated with lower chance of medical evaluation. In this study, a higher proportion of patients with LN-ESKD had employer group health insurance and were more likely to be informed of kidney transplant as a treatment option compared to patients with other primary causes of ESKD. However, upon adjusting for these socioeconomic characteristics when examining access to evaluation start among referred patients, there was little change in the association. This suggests that the patient characteristics, specifically age, contributing to the differences in referral between patients with LN-ESKD and other-ESKD may not be the same for starting the evaluation.
Limitations
The findings from this study must be interpreted in the context of its limitations. First, we do not have early transplant access data for all 48 transplant centers across the four regions in this study. Researchers associated with E-STAR were unable to collect complete referral and evaluation start data from 20 of the 48 transplant centers as of 2022, although data collection will continue annually and more centers are expected to be added in future rounds of data collection. Second, we did not have access to more granular data on patient-level factors such as lupus disease activity and immunosuppressive medication use, biomarkers of nutritional status at time of ESKD start, which may have introduced confounding by indication. Moreover, patients’ lupus disease activity may change during the time spanning ESKD diagnosis and could lead to delay in referral and start of an evaluation for kidney transplant. Finally, without access to medical records and kidney biopsy reports for the patients included in our study, we relied on the CMS-2728 form to appropriately classify whether a patient’s primary cause of ESKD is attributable to LN, which may have led to some misclassification of the exposure. However, using American College of Rheumatology criteria as the gold standard, a 2017 validation study found that SLE diagnosis in the USRDS with good sensitivity (79%), and excellent specificity (99.9%), positive predictive value (93%), and negative predictive value (97%), reducing concern for differential misclassification of the exposure. 27
Conclusions
Our study found that a large proportion of patients with LN-ESKD are being referred and evaluated for kidney transplant, suggesting that providers may not be unnecessarily delaying transplantation in this patient population, which could lead to more transplantations and better transplant outcomes. We also observed that patients with LN-ESKD are being referred and starting the evaluation as or more often than patients with ESKD unrelated to LN. Yet, patients with LN-ESKD are being referred less often prior to dialysis start (preemptively referred) compared to patients with other-ESKD. These results are encouraging, and providers should continue their current referral practices among patients with LN-ESKD. However, a rheumatologist should put forth a more concerted effort to ensure that patients with LN are referred prior to developing ESKD, by providing earlier referrals to nephrology, directly referring patients for transplant, or encouraging self-referral. Earlier referral could lead to more opportunities for living donor kidney transplants and better post-transplant outcomes among those with LN-ESKD, such as improved patient survival and lower risk of graft failure. Patients with LN-ESKD are a unique subset of the general ESKD population given their younger age and prolonged use of immunosuppression due to their underlying disease. It is critical that clinicians and researchers in the field of ESKD continue to make every effort to increase survival and quality of life for this patient population by pursuing transplant early in the kidney disease course.
Supplemental Material
Supplemental Material - Referral and evaluation for kidney transplantation among patients with lupus nephritis-related end-stage kidney disease
Supplemental Material for Referral and evaluation for kidney transplantation among patients with lupus nephritis-related end-stage kidney disease by Laura McPherson, Laura C Plantinga, Penelope P Howards, Michael Kramer, Stephen O Pastan, and Rachel E Patzer in Lupus
Footnotes
Acknowledgments
The authors’ work was supported by the National Institute on Minority Health and Health Disparities (NIMHD) through grant U01MD010611 and the National Institute of Diabetes and Digestive and Kidney Diseases through grant R01DK122701 and F31DK135379-01. The data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy or interpretation of the U.S. government.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (F31DK135379-01), National Institute of Diabetes and Digestive and Kidney Diseases (R01DK122701), National Institute on Minority Health and Health Disparities (U01MD010611).
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.