
Abstract
Objectives
To determine if serologic phenotypes could be identified in systemic lupus erythematosus patients developing interstitial lung disease (ILD) and/or myositis.
Methods
Adult SLE patients (without myositis/ILD at baseline) had annual assessments and serum sampling between 2000 and 2017. New-onset ILD was identified using the SDI pulmonary fibrosis item. New-onset myositis was identified using the SLICC Damage Index muscle atrophy/weakness item, the SLEDAI-2K item for myositis, and annual creatinine kinase testing. Chart review confirmed ILD/myositis cases and randomly sampled SLE patients from baseline formed our sub-cohort (N = 72). Cases and sub-cohort were compared regarding myositis-related biomarkers at baseline and at a randomly selected follow-up between baseline and end of observation (date of ILD/myositis diagnosis or Dec. 31, 2017). Descriptive analyses and hazards ratios (HRs) were generated for ILD/myositis incidence, focusing on baseline serology and adjusting for sex, race/ethnicity, age at SLE diagnosis, and SLE duration.
Results
Fourteen SLE patients developed ILD (N = 9), myositis (N = 3), and/or both (N = 2). Thirteen of those (92.9%) developing ILD/myositis had at least one biomarker at baseline, versus 47 (65.3%) SLE patients who never developed myositis/ILD. The most common biomarkers in myositis/ILD were KL-6, anti-Ro52, and anti-Ku. Baseline biomarkers tended to remain positive in follow-up. In multivariate Cox regressions, SLE patients had higher risk of developing myositis/ILD with elevated baseline KL-6 (adjusted hazard ratio 3.66; 95% confidence interval 1.01, 13.3). When updating biomarkers over time, we also saw correlations between anti-Smith and ILD/myositis.
Conclusions
Baseline myositis-related biomarkers were highly associated with ILD/myositis incidence. This is the first identification of biomarker phenotypes with ILD/myositis risk in SLE.
Introduction
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease associated with many different comorbidities, including interstitial lung disease (ILD) and inflammatory myositis. Although pulmonary involvement (including pleuritis) can affect up to 50% of SLE patients, 1 ILD is less common.2,3 Similarly, inflammatory myositis is reported in less than 10% of SLE patients.4–7 Although ILD and myositis are not considered common in SLE, they are associated with poor outcomes, including organ damage, disability, and death, as well as high healthcare use.3,6,8,9
To date, no biomarkers have been identified as predictors of the development of ILD/myositis in adult SLE. Our goal was to fill this gap.
Materials and method
Population
The McGill University Health Centre (MUHC) SLE clinic cohort enrolls patients meeting the 1997 American College of Rheumatology criteria. 10 For the current study, we identified all patients with a study visit between January 2000 to December 2017, with no prior history of ILD or myositis (N = 551). Baseline visit was the first visit, or enrollment date into cohort, after January 1, 2000. Patients were evaluated annually until the end of observation period (either the date of myositis/ILD diagnosis, or December 31, 2017).
A case-cohort analysis was performed in these SLE patients. Cases were all patients who developed myositis and/or ILD on follow-up. Cases were compared with a randomly selected sub-cohort (N = 72) from all the eligible SLE MUHC cohort (i.e. those who were free of ILD/myositis as of Jan 1, 2000). This sub-cohort provided controls for all risk-sets at each time-point that a case occurred, which was defined as the index time for each case-control set. Approval for our study was obtained from the research ethics board of MUHC’s Research Institute. Written informed consent was obtained from all participants.
Demographic and clinical data
Patients in the SLE MUHC cohort undergo annual study visits, where information is collected on medication exposures, disease activity, and other demographic and clinical data. Demographic variables evaluated as potential covariates of interest included sex, age at SLE diagnosis, race/ethnicity (White vs all others), SLE duration at first assessment, and smoking status at baseline.
The presence of potential myositis was screened for using the Systemic Lupus International Collaborating Clinics (SLICC) ACR Damage Index,11 SDI item for muscle weakness or atrophy, the SLE Disease Activity Index-2K 12 item for the variable myositis, and elevated annual serum creatinine kinase (CK) levels. Patients positive for any of these variables then had myositis confirmed through chart review (requiring supportive findings on muscle biopsies, muscle magnetic resonance imaging, electromyography, and/or neurologic consultation).
In our clinic, patients undergo CXR and pulmonary function tests (PFT) if they have persistent cough or SOB. We subsequently order high-resolution CT chest in persistently symptomatic patients despite normal CXR. There is no CXR or PFT screening of asymptomatic patients. The SDI is scored every year at the annual exam and if there was pulmonary fibrosis/ILD detected on pulmonary imaging or clinic notes, it was scored on the SDI. Chart review was then performed to confirm evidence of pulmonary fibrosis with either respirology consult, CT chest, or lung biopsy.
Laboratory testing for ILD/myositis-related biomarkers
All ILD/myositis-related biomarkers were assessed at baseline (first visit as of Jan. 2000 or enrollment visit if later than this date) and one randomly selected follow-up between baseline and end of observation (date of myositis/ILD diagnosis or Dec. 31, 2017). Line immunoassay (LIA: Euroimmun AG, Luebeck, Germany) detected autoantibodies to Mi2α, Mi2β, melanoma differentiation-associated gene 5 (MDA5), nuclear matrix protein-2 (NXP2), transcriptional intermediary factor 1γ (TIF1γ), PM/Scl-75, PM/Scl-100, Ku, signal recognition particle (SRP), Jo‐1, EJ, OJ, PL7, PL-12, Ro52, hydroxymethylglutaryl CoA reductase (HMGCR), cytosolic 5′-nucleotidase 1A (NT5C1A)/Mup44, centromere antigens (CENP) -B, topoisomerase 1 (Scl70), RNA polymerase III (RNAP), and Th/To (hPOP1). Addressable laser bead immunoassays were used to detect antibodies to telomeric repeat binding factor −1 (TERF-1), and Krebs von den Lungen-6 (KL-6) levels were determined by ELISA (R&D Systems).
Biomarkers detected by LIA were semi-quantitatively measured for signal intensity (SI) on the air-dried strips using a flatbed scanner and proprietary software (EUROArray Scanner, Euroimmun AG). Results were interpreted as: negative (≤10 SI), weak positive (11–29 SI), medium positive (30–89 SI), and high positive (>90S SI). Anti–TERF-1 and KL-6 were interpreted to be positive if greater than 500 U/mL which was based on 2 standard deviations above the mean value for adult healthy controls.
Statistical analysis
Cases and the sub-cohort were compared regarding baseline descriptive statistics for demographic and clinical variables. Differences in proportions between groups were analyzed using the Newcombe–Wilson score method. The Wilcoxon test was used to determine confidence intervals (CIs) for the continuous variables of age at SLE diagnosis and SLE duration at first assessment. Since antibody positivity may be correlated (with each other and/or with other model covariates), we examined correlation coefficients to detect any possible collinearity in the model. Multicollinearity arises in a regression model when some or all of model covariates are correlated with each other; this can cause imprecision, and make it difficult or impossible to interpret the parameter estimates from the model.
We used Cox proportional hazards regression, modified as per Prentice for case-cohort designs 13 to generate hazard ratios with 95% CIs for the variables of interest. Our multivariate models adjusted for sex, race/ethnicity, age at SLE onset, SLE duration at baseline, and, given our previously published paper linking anti-Smith antibodies with myositis in SLE, 4 we also included this variable.
Results
Patient characteristics
The median and interquartile range (IQR) of SLE duration at baseline was 1.8 (0.38, 5.6) years. Fourteen of 551 SLE (2.5%) patients with a study visit from January 2000 to December 2017 developed myositis and/or ILD (9 ILD, 3 myositis, 2 ILD associated with myositis). Of the 14 myositis and/or ILD SLE cases, 12 (85.7%) were female.
Descriptive statistics for SLE patients and differences between groups
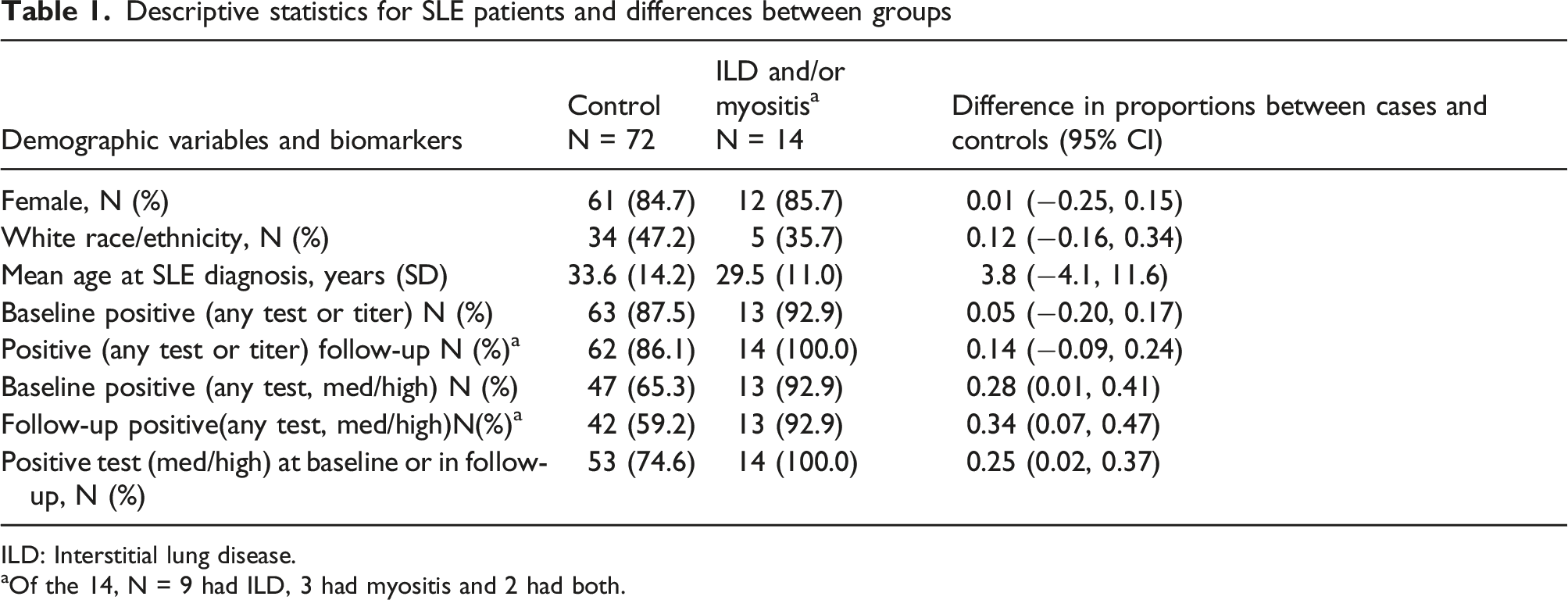
ILD: Interstitial lung disease.
aOf the 14, N = 9 had ILD, 3 had myositis and 2 had both.
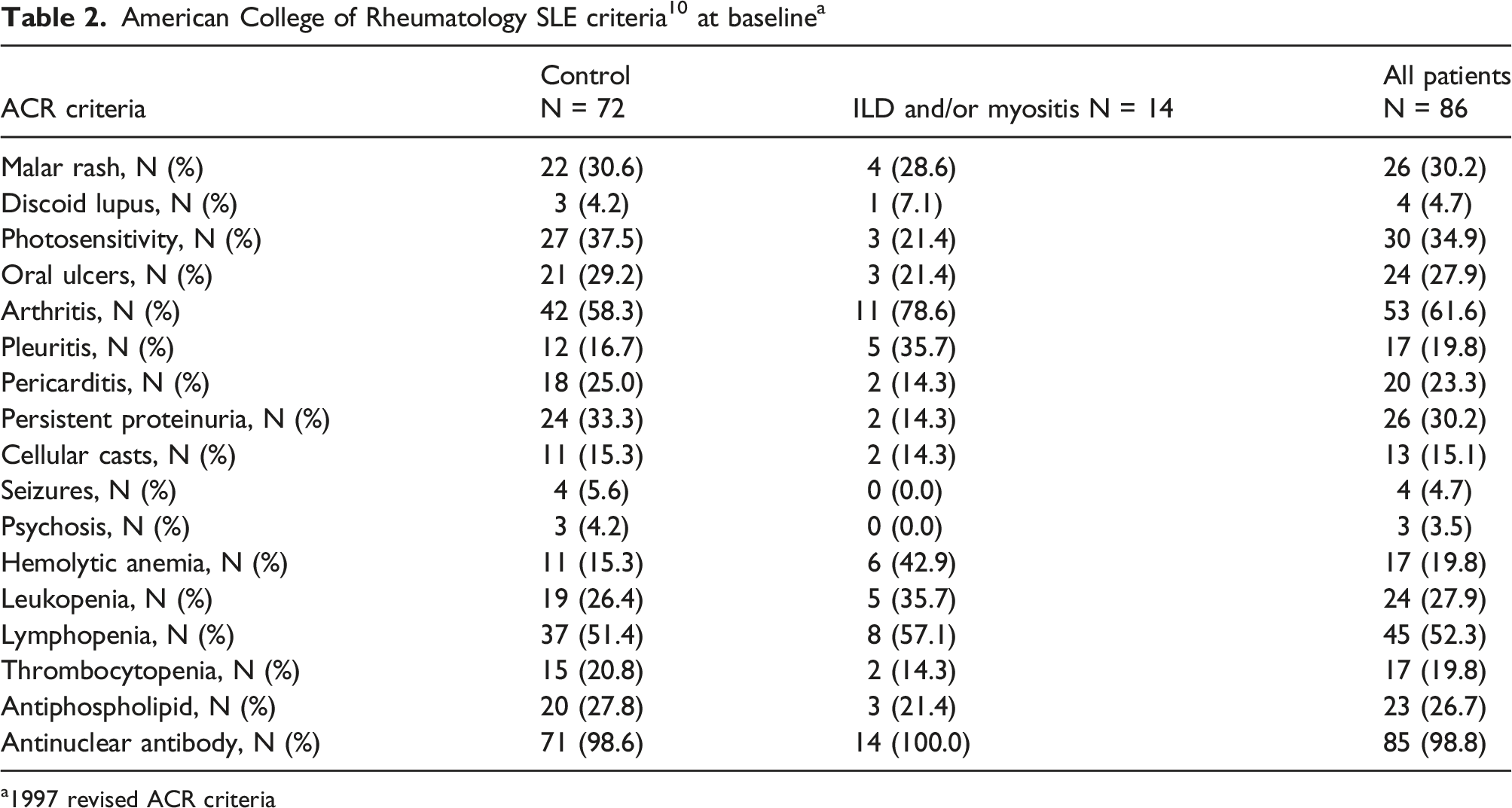
a1997 revised ACR criteria
Baseline and follow-up biomarkers in SLE-ILD/myositis cases versus controls
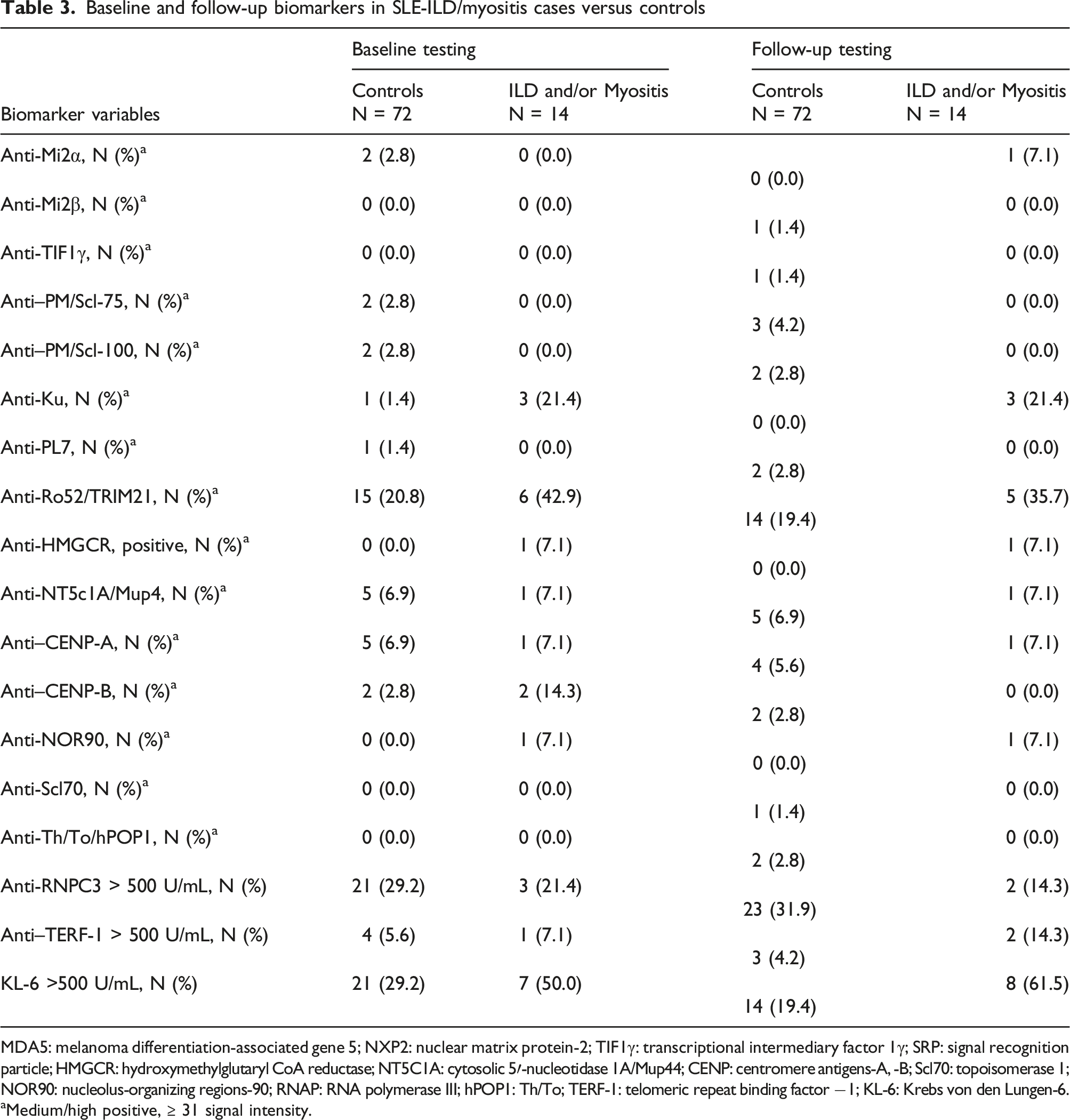
MDA5: melanoma differentiation-associated gene 5; NXP2: nuclear matrix protein-2; TIF1γ: transcriptional intermediary factor 1γ; SRP: signal recognition particle; HMGCR: hydroxymethylglutaryl CoA reductase; NT5C1A: cytosolic 5′-nucleotidase 1A/Mup44; CENP: centromere antigens-A, -B; Scl70: topoisomerase 1; NOR90: nucleolus-organizing regions-90; RNAP: RNA polymerase III; hPOP1: Th/To; TERF-1: telomeric repeat binding factor −1; KL-6: Krebs von den Lungen-6.
aMedium/high positive, ≥ 31 signal intensity.
Biomarkers/antibodies at baseline versus follow-up
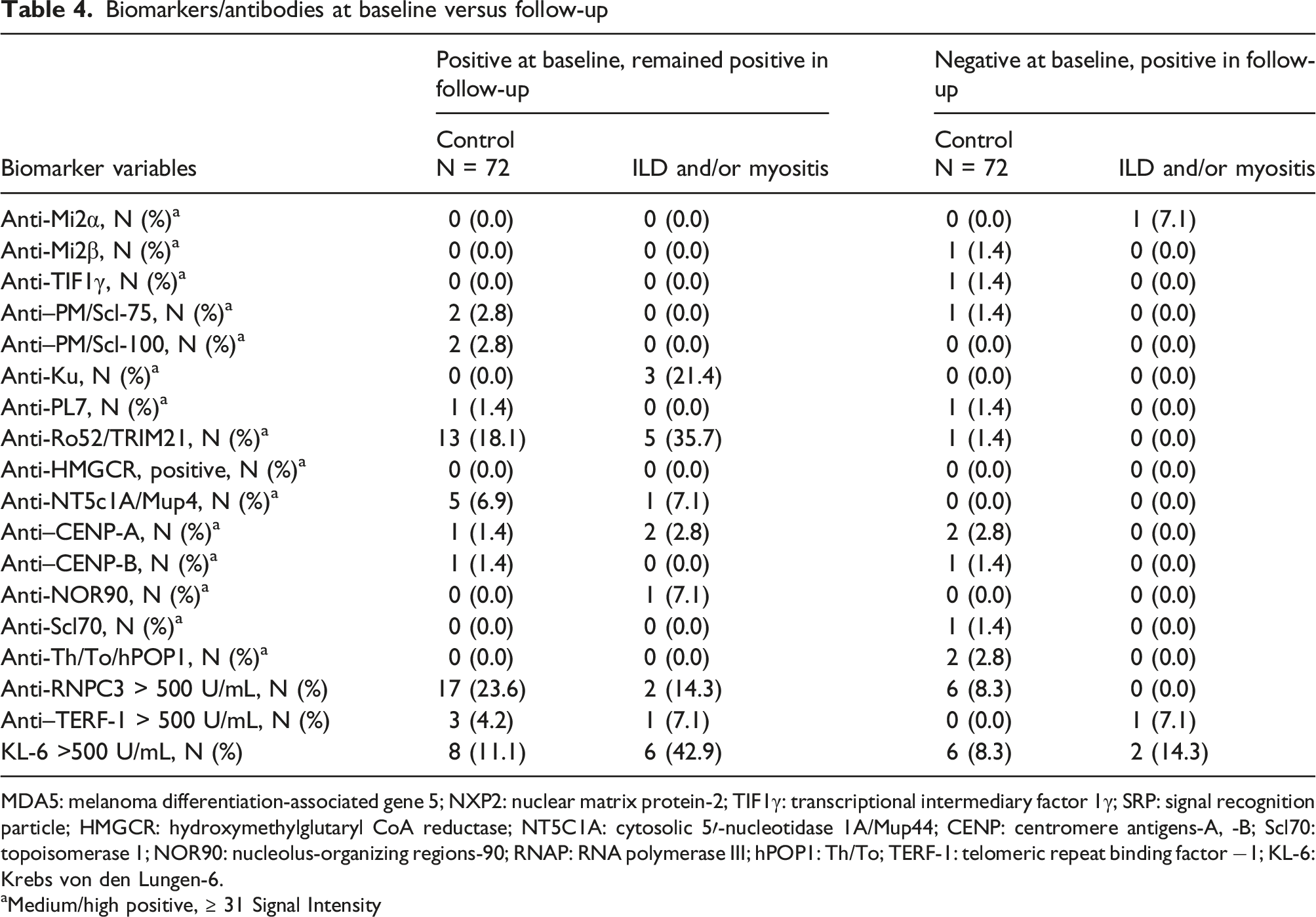
MDA5: melanoma differentiation-associated gene 5; NXP2: nuclear matrix protein-2; TIF1γ: transcriptional intermediary factor 1γ; SRP: signal recognition particle; HMGCR: hydroxymethylglutaryl CoA reductase; NT5C1A: cytosolic 5′-nucleotidase 1A/Mup44; CENP: centromere antigens-A, -B; Scl70: topoisomerase 1; NOR90: nucleolus-organizing regions-90; RNAP: RNA polymerase III; hPOP1: Th/To; TERF-1: telomeric repeat binding factor −1; KL-6: Krebs von den Lungen-6.
aMedium/high positive, ≥ 31 Signal Intensity
Case-cohort analyses
Hazard ratios (HR) for baseline characteristics of SLE patients with and without ILD/myositis
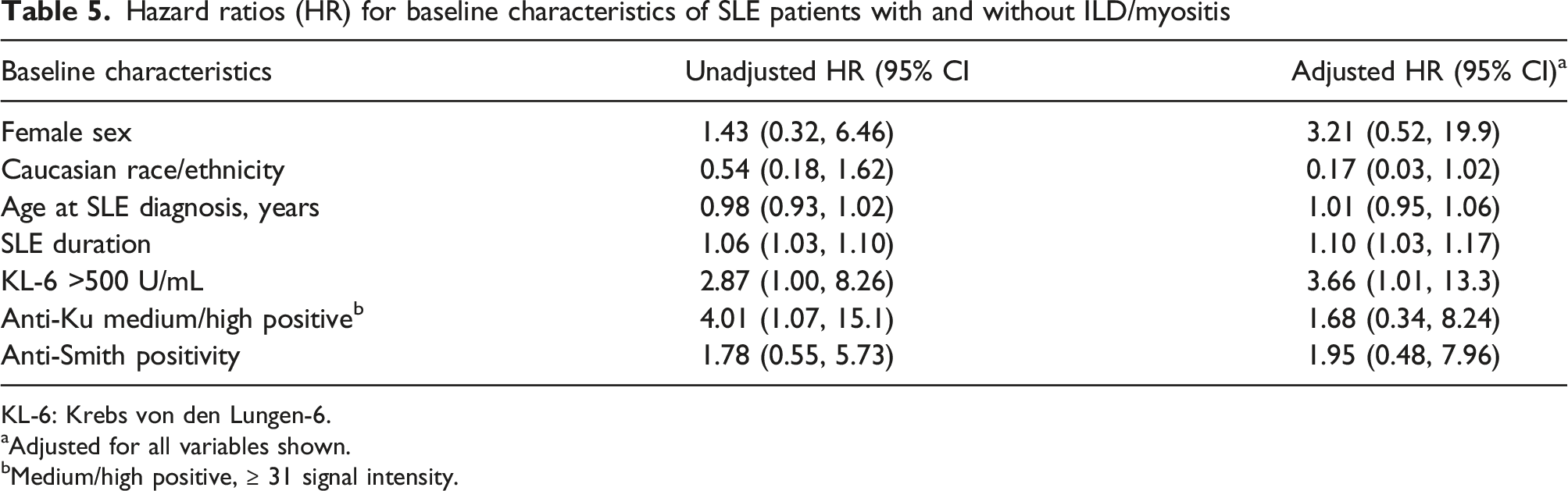
KL-6: Krebs von den Lungen-6.
aAdjusted for all variables shown.
bMedium/high positive, ≥ 31 signal intensity.
Hazard ratios (HRs) for ILD/myositis in SLE, biomarkers ever positive (baseline and/or follow-up)
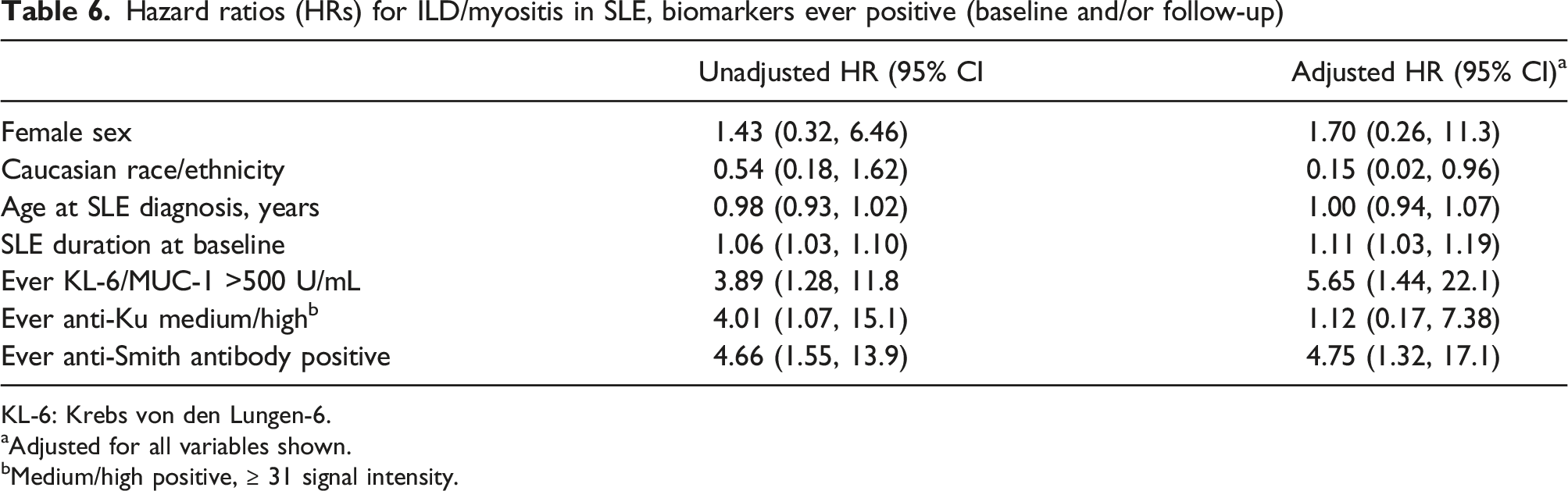
KL-6: Krebs von den Lungen-6.
aAdjusted for all variables shown.
bMedium/high positive, ≥ 31 signal intensity.
Discussion
In this SLE cohort, we identified that elevated KL-6 at baseline was highly associated with the development of ILD/myositis. Ours is the first study to identify a baseline biomarker phenotype of SLE patients most at risk for ILD/myositis.
KL-6 antigen is produced by alveolar pneumocytes and bronchiolar epithelial cells.14–16 Serum levels rise due to increased permeability of epithelial and vascular cells in the presence of damage, fibrosis, and regeneration/proliferation of pneumocytes.14–16 A handful of studies have suggested KL-6 as a potential biomarker for prevalent ILD in systemic juvenile idiopathic arthritis, juvenile SLE, and juvenile dermatomyositis.14–18 It has even been proposed to have a role in the pathophysiology of ILD, acting as a chemoattractant for fibroblasts. 14
KL-6 has been found to negatively correlate with pulmonary function and positively correlate with extensive radiographic pulmonary fibrosis in systemic sclerosis, as well as a possible correlation with mortality. KL-6 has previously been considered as a possible biomarker for ILD in pediatric-onset connective tissue disease. 18
In our study, of the SLE patients who had elevated baseline KL-6 level, four went on to develop ILD at follow-up, two went on to develop myositis, and one developed both myositis and ILD. High KL-6 levels in SLE patients with myositis, even in the absence of a clinical ILD diagnosis, have not been previously published, to our knowledge. Despite the average follow-up of 9.2 years in our study, it is possible that these patients may develop ILD later in their disease course, especially given the suspicion expressed in the literature that it is a slowly progressive manifestation that presents in long-standing SLE.1,3,19 Whether KL-6 could help to identify pre-clinical ILD within SLE requires additional investigation.
Elevated anti-Ro52 antibody level was also associated with the development of ILD/myositis in our SLE patients, but given its collinearity with other antibodies, we were unable to include it in the hazard ratio analysis. Ro52/TRIM21 is a common autoantibody target in systemic autoimmune rheumatic diseases, and has distinct clinical functional properties from Ro60, although previously commonly classified together.20–22 It has a cited prevalence of 70%–90% in primary Sjogren’s syndrome 40%–70% in SLE, 20%–68% in DM, and 15%–30% in scleroderma.21,22
Anti-Ro52 is also associated with ILD, and in some cases even rapidly progressive ILD 23 resistant to immunosuppressive therapies, 24 and a poor prognosis in idiopathic inflammatory myopathies. 25 Anti-Ro52 often co-exists with other autoantibodies and some studies suggest that isolated anti-Ro52 may indicate an idiopathic inflammatory myopathy. 22 Thus, it is perhaps not unexpected that we found co-linearity of anti-Ro52 with other autoantibodies in our study, and it is high prevalence in our SLE-ILD/myositis patients further highlights the significance this autoantibody may have in this overlap syndrome.
Anti-Ku antibody is an antinuclear autoantibody that has been identified in several connective tissue diseases such as SLE and scleroderma, and is more common in African American versus Caucasian SLE populations. 26 Anti-Ku in SLE was previously reported to be associated with prevalent ILD, inflammatory myopathy, arthralgia, and Raynaud’s phenomenon,26–30 further suggesting that SLE patients who developed myositis and/or ILD represent a specific phenotype within the broad spectrum of SLE.
Our previous publication identified the presence of anti-Smith antibody as a risk factor to developing myositis in a cohort of SLE patients, 4 and an association between ILD/myositis was evident in the adjusted analyses that updated biomarkers over time (Table 6).
Strengths of the study include its prospective nature as it measured incident myositis and ILD cases, rather than prevalence. Potential limitations include the relatively low number of events of ILD and myositis. Since screening for myositis and ILD (using SDI, SLEDAI-2K, and CK) was performed annually, it is possible that cases of myositis and/or ILD were missed. However, the low number of events is consistent with other published studies in myositis and ILD.8,9,31 Although a case-cohort analysis remains an alternative cohort-based design, meaning that data is collected prospectively, the analyses have a retrospective nature which is a potential limitation.
In conclusion, SLE patients were more likely to develop ILD and/or myositis if they had elevated baseline myositis-related biomarkers, particularly KL-6. When updating biomarkers over time, we also saw correlations between anti-Smith and ILD/myositis. To our knowledge, we are the first to identify a biomarker phenotype in adult SLE patients most at risk of developing new-onset ILD and/or myositis.
Footnotes
Acknowledgment
The authors acknowledge the laboratory assistance of Haiyan Hou and Meifeng Zhang, University of Calgary.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the McGill University Health Center Lupus Clinic research activities are funded by the Singer Family Fund for Lupus Research.