
Abstract
Objectives
Systemic lupus erythematosus (SLE) is associated with high levels of workplace disability and unemployment. The objective of this study was to understand the reasons for this and to describe the barriers and facilitators of employment identified by people with SLE to develop appropriate solutions. Unemployment, as well as unsuitable work, has adverse health outcomes.
Methods
Adults with SLE completed a UK-specific online survey, through the LUPUS UK website, designed to find out more about the difficulties and successes that people with SLE have in maintaining employment. The survey was predominantly qualitative, to understand participants’ employment experiences to generate possible solutions.
Results
Three hundred and ninety-three people gave detailed responses to the survey within eight weeks. Every respondent reported a detrimental effect of SLE on their ability to work: 40.45% had left employment because of it. The themes of concern to respondents were unambiguous: (i) the difficulties of working (and career damage) with SLE, (ii) fear and anxiety overshadowing work/family life, (iii) the greater potential to remain in some employment or stay in full employment when modifications of work pattern and support from management and colleagues were available. SLE-related fatigue, its invisibility and fluctuating nature were felt to be the main barriers to maintaining employment. Numerous respondents could work only part-time and anxiety was high regarding their future ability to continue working. Many had taken substantial pay reductions and refused offered promotions to preserve their health. Distress due to loss of work and the benefits it brings were reported by every respondent who had left work.
Conclusion
SLE presents specific difficulties for maintaining employment – fatigue, fluctuation and invisibility – not addressed by current anti-discrimination legislation or currently available ‘reasonable adjustments’. This study demonstrates that (i) employment is an important area of concern for people with SLE, (ii) SLE has significant detrimental effects on individuals’ ability to participate and progress in employment, (iii) legislators and employers need information about SLE as invisibility and fluctuation cause hidden problems, and (iv) more data is needed to inform workplace adjustments if individual distress and societal loss of skills are to be addressed.
Introduction
Systemic lupus erythematosus (SLE or lupus) is a chronic, multisystem autoimmune disease, which is currently incurable. It fluctuates with flares, relapses and remissions throughout life. There are a broad range of presentations, clinical trajectories and severity between individuals. It is more common in women (incidence ratio 9:1 female to male) and in those of Asian or African ethnicity. 1 Its onset is most commonly in youth or middle-age, although presentation in older age groups is possible. Advances in clinical care enable most people with SLE, without major organ involvement, to live a relatively normal lifespan, but intrusive symptoms (particularly fatigue and cognitive dysfunction) often have a profound effect on quality of life. The physical and psychological features of SLE are well characterized in the medical literature.1,2 The psychosocial impacts of the illness are now being documented.2–5
A recurrent theme in the existing literature is the detrimental effect of SLE on individuals’ ability to work with higher levels of (i) disability, (ii) absenteeism and (iii) increased levels of ill-health retirement.4–9 Kent et al. 4 concluded, from their online survey of 121 people, that SLE ‘has a considerable impact on patients’… physical, social and economic wellbeing’. Reduced levels of participation in employment were highlighted as was the need for ‘improved support and information for employers of patients’. Drenkard et al. 6 concluded, from their cohort study in a population from southeast USA, that ‘the risk of unemployment in SLE is almost 4-fold higher than the general population. SLE imposes a substantial toll on individuals and society’. For those in work, they noted that ‘fatigue had the greatest impact on WPI (work productivity impairment)’. The impact of fatigue on WPI was also strongly highlighted in Gordon et al.’s 7 online survey of European patients with lupus, which summarized its findings as ‘the substantial burden of systemic lupus erythematosus on the productivity and careers of patients’. 7 These important studies quantified the profound effects of SLE on individuals’ ability to participate in employment.
It is also established that ‘employment is one of the most important aspects of psychosocial functioning. It not only provides earnings and social status, but also imparts a sense of self-worth and the opportunity to socialize with peers and to create social networks, 10 and that being excluded from work has detrimental effects on individual’s health’.
This concise report presents key findings from an online survey developed to add to the existing literature4–8 to identify the employment challenges that people with SLE experience (using a qualitative methodology) with the possibility of developing strategies to overcome them.
Methods
This was a cross-sectional, online, study of patients aged ≥18 years, resident in the UK, with a self-reported diagnosis of SLE. The questionnaire was designed with the input of a leader of a local lupus group, using her experience of supporting members. A small within-group review of the questionnaire was undertaken. It was posted on LUPUS UK’s website, after a ‘priming’ article in the LUPUS UK member’s magazine, using the Bristol Online Software. It was available from 2 September–31 October 2017. All responses were anonymous. Ethical approval was obtained from the Faculty of Health Sciences, University of Hull.
The survey consisted of 22 questions: nine collected demographic data, including one on drug therapy, to gauge diagnosis. Fifteen were stem questions where a quantitative response was required with an opportunity for free text statements. Ten stem questions related to employment, two to the benefits system.
A range of demographic data was collected, including occupation and employment status. Participants were asked about the level of understanding shown by their managers and colleagues about their illness and its day-to-day fluctuations, and to quantify (on numerical rating scales) the psychological distress associated with (i) loss of income resulting from SLE, (ii) the proportion of income loss due to SLE, (iii) the degree of fear that participants experienced about being unable to sustain future employment, and (iv) any stress associated with claiming benefits.
The descriptive statistics summarized respondent characteristics and frequency of responses. A thematic analysis of free text comments was conducted independently by all authors, then compared, agreed upon and summarized.
Results
The survey generated a swift, substantial response (393 replies in eight weeks, 200 within the first 48 hours), indicating the importance of the issues to patients. A hundred per cent of participants used the free text option to give detailed information.
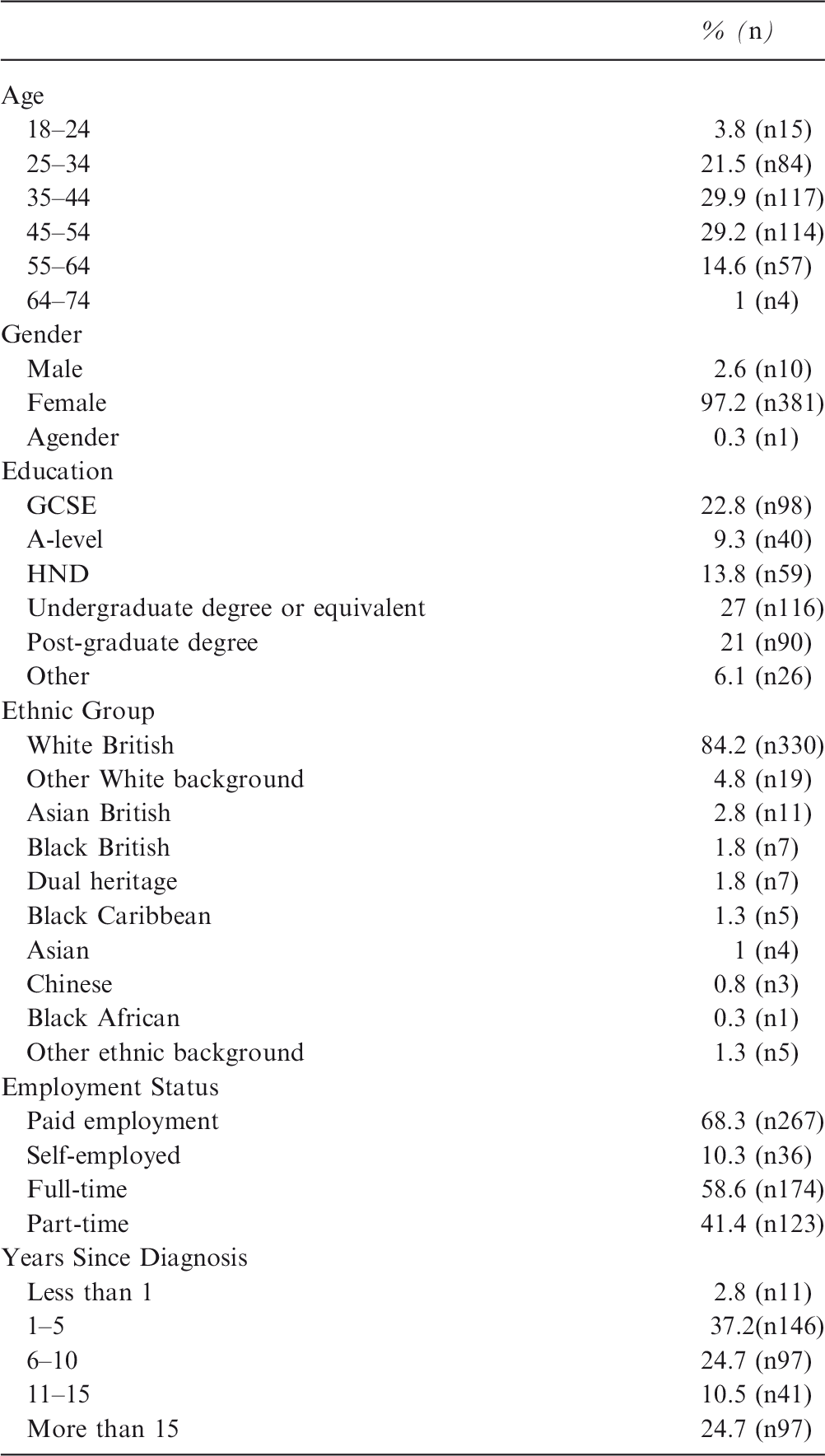
Respondents’ ages ranged from 18–74, with 60% aged between 35 and 54; the sample was 97% female, a significant number were highly educated, (48% had a first or post-graduate degree), and 84% were White British. There was a broad geographic spread of respondents across the UK. Thirty-seven per cent of respondents reported that they had had SLE for 1–5 years, 25% reported that they had been diagnosed for over 15 years. Ninety-three per cent of respondents were taking SLE medication.
Respondents were employed in a wide range of occupations including, managerial, academic, professional, technical, administrative and sales. A number were employed in the NHS. No one was employed in occupations that relied exclusively upon the use of manual labour (however, it is recognized that any occupation might involve varying degrees of physical activity). This finding corresponds closely with the qualifications data. All reported a detrimental impact of lupus on their careers, variously citing (i) a reduction in the number of hours they were able to work and/or (ii) its negative impact on their promotion prospects, and/or (iii) their ambitions. Some 40.45% of the total sample had left their employment due to lupus; of these, 27% were retired on medical grounds, 36.5% resigned, 25.8% were dismissed on capability grounds and 10.7% chose to retire.
Demographic data of sample surveyed
The main themes identified from free text data were:
The difficulties of working (and the reality of career damage) with a fluctuating condition such as SLE; Fear and anxiety overshadowing work and family life; The potential to remain in some or full-time employment when modifications of work pattern and support from management and colleagues were available.
Theme 1: the difficulties of working (and the reality of career damage) with SLE
Themes 1 and 2
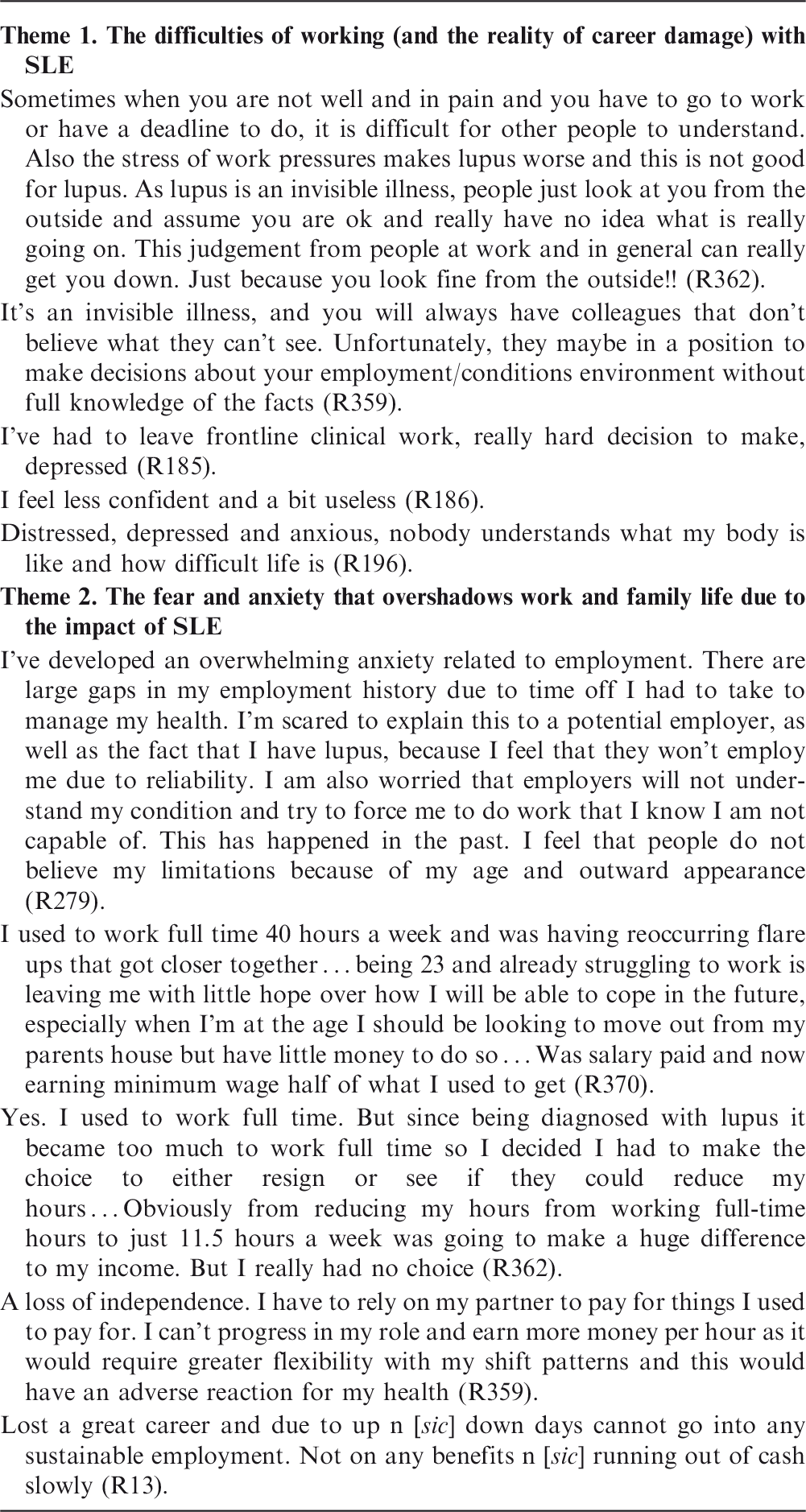
Theme 2: the fear and anxiety that overshadows work and family life due to the impact of SLE
Participants were asked to rate the severity of their worry regarding maintaining employment in the future. On a scale from 0–10, where 0 indicated ‘low or no worry’ and 10 denoted ‘significant worry’, 68% (n = 255) scored 8 or above, with 47.2% of the total number of respondents indicating 10 (see Box 1).
These concerns were linked to (i) individuals’ future prospects of continuing to earn enough to live on, (ii) uncertainty regarding future health and (iii) fear of reliance on benefits.
Where individuals had stopped work, they were concerned about the possibility of relying solely on another person’s income. Two examples of respondents' (R) comments are given below My husband and I are completely reliant on the money he makes so I worry if something happens to that, what will we do? (R391). I am lucky my husband works to cover our expenses but if something happens to him we couldn’t manage (R102).
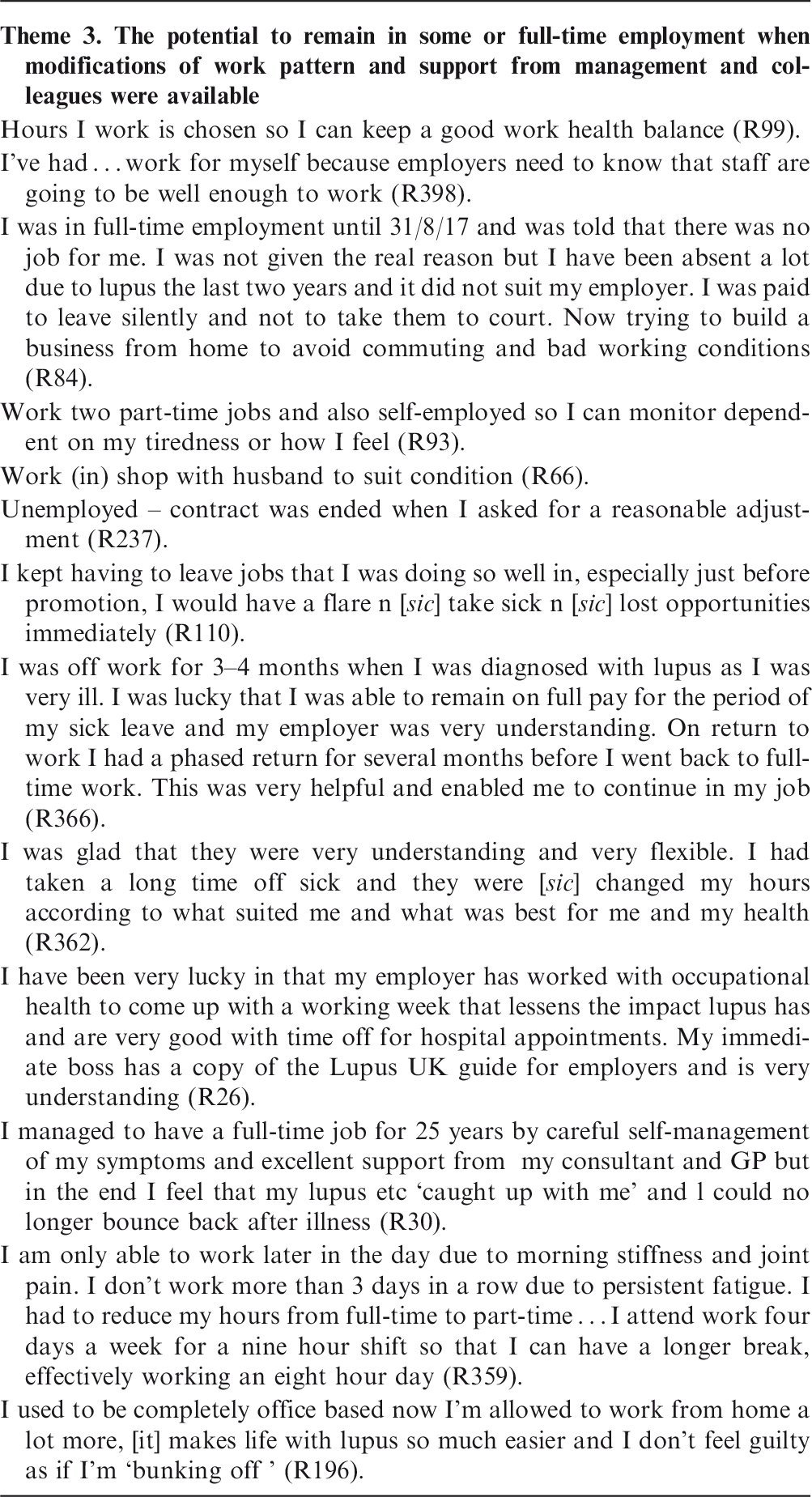
Theme 3: the potential to remain in employment when modifications of work pattern and support from management and colleagues were available
Theme 3
Patients identified the following strategies that supported remaining in paid work:
Understanding from managers; Appreciation from colleagues that the symptoms of SLE can fluctuate; Flexibility in working hours and patterns; Belief in the reality of the illness and its impact. Because I have a very senior position I'm in a good place to access support and adaptations. But it is really hard to admit I need help due to attitudes to hidden disabilities (R138). I have more flexibility to work on different days and times depending on how I feel. Less stressful than feeling pressured to go in when unwell (R 229).
Discussion
This study describes the challenges faced by people with SLE in maintaining employment. It is now well established that SLE causes impaired productivity at work, reduced levels of employment and increased levels of medical retirement.4–11 Neuropsychiatric lupus and arthritis are particularly associated with the need to leave employment.9,11,12 All these cause substantial distress to individuals, significant loss of individual income and societal costs owing to benefits and early pension payments. SLE is a hidden cause of years of working lives curtailed or lost, with damaging effects on workplace skills, experience and diversity. 9
Importantly, this study identified three characteristics of the illness that contribute to the impact on employment: (i) the unpredictability of SLE, making provision of a consistent contribution to work problematic, (ii) its invisibility – militating against colleagues and managers believing in the reality of the disease and (iii) SLE-related fatigue – the distinction between tiredness that results from a busy schedule and the crushing fatigue that is unresponsive to rest – associated with lupus seems hard for others to appreciate.
As SLE primarily affects young women, and may be active over many decades, the potential impact on an individual’s educational prospects, employment opportunities and personal development is profound.4–6 It may interrupt the attainment of educational milestones and entry into employment, negatively shaping an individual’s destiny over the course of their working life. The resulting reduction in quality of life, psychological status and income from being unable to participate fully in employment will affect individuals’ physical and psychological health adversely. 14 As SLE is incurable, workplaces need to adapt to accommodate people with an illness that fluctuates over years with potential accumulating morbidity from both the illness and its treatment. Current employment legislation does not specifically highlight the need for support for fluctuating, incurable conditions and awareness seems low. Good practice is reliant on local imaginative adaptations and informed occupational health services. A recent Arthritis and Musculoskeletal Alliance 15 report on employment is a promising development, but makes no mention of the three cardinal features of SLE identified by the respondents that make work difficult: invisibility, fluctuation and fatigue. It also makes no specific recommendations about how work patterns may be modified to accommodate people with these conditions. Another advisory paper and report from the Trades Union Congress16,17 dealt with invisibility but not fluctuation. Employment support needs to be fitted to the disability or long-term condition; a prosthetic limb would not help a blind person, nor a hearing aid someone with an amputation. No specific research data has been developed to guide occupational health and employers for the key disabling aspects of lupus, although excellent general ideas are available from, for example, LUPUS UK.18.
In addition, the context of the workplace for those with hidden disabilities and fluctuating conditions, where no quantifiable tests such as dyslexia severity or decibels of hearing loss are available. This needs consideration where disbelief and scepticism, as reported by our respondents and other reports, can be demeaning16,17.
Many previous papers describe the social ‘burdens’ that lupus imposes, often emphasizing societal costs.4–7. Some of this financial loss for the individual and society may well be avoidable if more sophisticated ideas on employment support were available. The burdens that society imposes on people with SLE, reducing their chances of remaining in work, also need consideration, as do the possible societal gains of improved support. Our findings go some way to explaining why unemployment rates are so high in lupus.The results also demonstrate a high level of anxiety in respondents currently in work, because they feel that their future ability to work is threatened by the disease.
The barriers to employment for people living with a fluctuating condition were considered by Steadman et al. 19 Their report made a number of recommendations on recognizing and adapting the work environment and patterns of employment for people with these types of illnesses, which cover a wide range of physical and mental conditions. However, no research data that was specific to lupus was cited in that report. Our study highlights how, when the fluctuating nature of lupus and its specific symptoms are recognized by management and colleagues, and flexible work patterns are developed to accommodate these, there is a much higher chance of continuing employment. Research on specific adaptations for working with lupus would be helpful, including the organization of teamwork, so that others do not feel their workload is unfair. An understanding of the impact of fatigue on the ability to retrain as well as maintain current employment would also be useful.
Although it is considered a relatively rare disease, the number of working days lost from SLE is relatively high. One person not completing higher education or managing to stay in employment may lose 50 or more years of working life. As such, the personal and societal toll will be very high. It is clearly in society’s interests to keep people in education and employment as long as possible, or at least combine welfare benefits with part-time work where needed.
Appropriate employment, that is, work that enables an individual to function in a way consistent with their physical and mental capabilities, can be seen as an intervention that supports health and wellbeing.12,14 This is increasingly recognized by governments who realize that if they do not retain people with long-term conditions (LTCs) in work they will have to support them on benefits. 20 Conversely, work has the potential to damage health if it consistently imposes demands that an individual cannot meet. This is both physically and psychologically stressful, creating a psychological double-bind by locking individuals into cycles of failure as well as unmanageable physical burdens.
Successive UK governments have, nonetheless, pledged (i) to increase the proportion of people with LTCs in work, (ii) to ensure that workplaces adjust the environment and the systems of work to make it possible for those with serious disability to continue employment, (iii) to provide financial support if people are unable to work, and (iv) to always make work pay. However, the White Paper (2017) 20 makes no specific mention of adaptations for fluctuating conditions, nor the idea of part-time work in combination with benefits for those unable to sustain full-time employment. Without considering fluctuating conditions separately, progress seems unlikely.
Some of the initiatives available for other disease groups may also give ideas for how employment levels and quality of life may be improved for those living with lupus. There are proactive evidence-based strategies for ‘survivorship’ in illnesses like cancer (often now a chronic, symptomatic condition where fatigue is prominent), designed to keep people engaged in the community and in employment.21, 22 No such investment has been made in helping patients with lupus, which predominantly affects young and middle-aged people. Panopolis et al. 10 and Yelin et al. 12 suggest that specific training schedules used in cases of traumatic head injury and mental illness could help people with lupus and neuropsychiatric lupus (NPL) to improve their work performance. Canham 24 has designed and tested an online training schedule for employers of people affected by bipolar disorder, another fluctuating, invisible condition. Employee passports have been tried in some organizations to highlight individuals’ specific needs and limitations at work. 19 We suggest that employment level or the ability to participate in a chosen role should routinely become outcome measures in lupus studies assessing quality of life.
Strengths and limitations of the study
The strengths of our study include the unequivocal consistency of concerns expressed by participants of themes with a high proportion of the sample in work and speaking from contemporary experience. Limitations include the high proportion of White British respondents, few men, the need for digital literacy to complete the survey and the lack of diversity in the levels of education. SLE was a self-reported diagnosis, which may be seen as a limitation, however, 93% of the sample were on at least one anti-SLE drug, (24.75% were taking two or more). Selection bias is inevitable, but the rapid, voluntary participation in the survey confirms the importance of the issues to people with SLE. Future work involving purposive sampling would enable between-group differences to be investigated. This was an explorative, qualitative study to report patient experience and generate hypotheses.
Our findings build and extend those of previous investigations on employment in relation to lupus4–11 and echo Kent et al’s. 4 call ‘for improved information and support for employers of those with SLE’ as well as early intervention to keep people with lupus in education and employment. Supporting individuals to combine some work with benefits may enable people to increase their work, income and tax receipts at a point when their condition allows, but receive the necessary financial support when it does not. Current approaches seem predicated on a binary condition of health and a constant, quantifiable level of disability, which can be overcome with a piece of equipment or simple change in a work schedule.
Conclusions
This data provides further confirmation that SLE is associated with (i) a reduction in working hours and income,3–11 (ii) changes in working patterns, (iii) changes in career path potential25,26 and (iv) high levels of fear and anxiety in patients related to SLE and employment.14,15
Our data indicate that a lack of employment causes mental distress and individuals wanting to stay in work in the best health possible. Employment is increasingly recognized as a health intervention: the health of individuals with lupus is worsened by uninformed employment practices. Consequently, society experiences a loss of working years, skills, expertise and diversity. The data suggest that there are ways in which this could be mitigated by changes in equality legislation and employment practices. Research is needed to understand the specific changes, including individual training for employers, employees, and occupational health professionals that may prove helpful. 24 Another area of interest is considering how those with SLE could make informed employment decisions, finding a work environment or being retrained for work that is likely to support their health, taking SLE into account. 24 Increased awareness of the disease and its impact are needed at the highest levels of government and wider society before this is likely. More data is needed to inform this process. If the Department for Work and Pensions/Department of Health and Social Care intend ‘to transform employment prospects for … those with long-term health conditions’ in order to overcome ‘a wide range of barriers and historic injustices’, 20 these barriers need to be better understood and the specific problems of those with SLE (and diseases like it) explored, documented and solutions generated. Examples of good practice urgently need wide dissemination to help retain people in employment, and part-time attendance at school and university needs to be supported, not penalized. Our survey suggests this is possible and that the beneficial impacts on the health of those with SLE and wider society could be significant.
Footnotes
Acknowledgements
We would like to acknowledge the early support of the remarkable Shelagh Cheesman, former leader of Cambridge Lupus group, who died in March 2018. We would like to thank all our anonymous participants and all other correspondents who sent separate messages of support. We are very grateful to Paul Howard, deputy CEO of LUPUS UK, who hosted the survey on the LUPUS UK website and publicized it. We would like to thank Professor Debbie Cohen for information about other initiatives being considered for supporting employment in those with relapsing and remitting disorders.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.