
Abstract
Systemic lupus erythematosus (SLE) patients are at high risk of herpes zoster. Previously, we found increased immunoglobulin (Ig)G levels against varicella-zoster virus (VZV) in SLE patients compared to controls, while antibody levels against diphtheria and cellular immunity to VZV were decreased. We aimed to test our hypothesis that increased VZV-IgG levels in SLE result from subclinical VZV reactivations, caused by stress because of lupus disease activity or immunosuppressive drug use.
Methods
Antibody levels to VZV (IgG, IgA, IgM), total IgG and VZV-DNA were longitudinally determined in the serum of 34 SLE patients, using enzyme-linked immunosorbent assay and polymerase chain reaction. Clinical data were retrieved from medical records. Reactivation of VZV was defined as an at least fivefold rise in VZV-IgG or presence of VZV-IgM or VZV-DNA. Generalized estimating equations (GEE) were used to longitudinally analyse associations between antibody levels, lupus disease activity and medication use. Systemic Lupus Erythematosus Disease Activity Index, anti-double-stranded DNA and complement levels were used as indicators of lupus disease activity.
Results
A VZV reactivation was determined in 11 patients (33%). In at least five of them, herpes zoster was clinically overt. No association between SLE disease activity or medication use and VZV-specific antibody levels was found. There was a weak association between total IgG and VZV-IgG.
Conclusions
Our results indicate that increased VZV-IgG levels in SLE do not result from frequent subclinical VZV reactivations, and are not associated with lupus disease activity. Increased VZV-IgG can only partially be explained by hypergammaglobulinaemia.
Keywords
Introduction
Infectious diseases are an important cause of morbidity and mortality in patients with systemic lupus erythematosus (SLE), an autoimmune disease that is characterized by the presence of autoantibodies and recurrent disease flares. 1 Herpes zoster (HZ), characterized by severe pain and rash in a dermatomal distribution, is one of the infectious diseases frequently affecting SLE patients. The incidence of HZ is reported to be 5 to 16 times higher in SLE patients than in the general population, and is associated with the use of immunosuppressive medication.2–5
HZ is caused by reactivation of the varicella-zoster virus (VZV). After primary infection, known as varicella or chickenpox, VZV establishes latency in the sensory nerve ganglia.6–8 Since almost the entire population of temperate countries has experienced a primary VZV infection in childhood, almost the entire adult population is at risk of HZ, occurring when cellular immunity to VZV wanes. 9
Previously, we found increased VZV-specific antibody levels of the immunoglobulin (Ig) G class in SLE patients compared to age-matched healthy controls, while cellular immunity to VZV was found to be decreased. This phenomenon could not be explained by polyclonal hypergammaglobulinaemia alone, which is often observed in SLE, because for diphtheria lower antibody levels were found in SLE patients than in age-matched healthy controls. 10
Similar to VZV, increased antibody levels to other human herpes viruses, such as Epstein-Barr virus (EBV) and cytomegalovirus (CMV) have been described in SLE. 11 Antibody levels to several other infectious agents were shown not to differ or even be lower in SLE patients, compared to healthy controls. 12 Human herpes viruses, in particular EBV, have been implicated to play a role in the development and relapsing course of SLE. 13
Over the years, different research groups have suggested that reactivation of VZV without overt clinical manifestations may play a role in the increased VZV-IgG level in SLE patients.10,14,15 Indeed, it is known that a clinically evident reactivation of VZV, herpes zoster, leads to long-lasting increases in VZV-specific IgG levels.16,17 Subclinical reactivations of VZV have been described in immunocompromised patients 18 and are known to occur under stressful circumstances, even in otherwise healthy individuals.19,20
In the present study antibody levels to VZV and presence of VZV-DNA were determined longitudinally in a retrospective cohort of SLE patients. We expected to find frequent subclinical VZV reactivations in SLE patients, able to account for their increased VZV antibody levels. We hypothesized that VZV reactivations in SLE patients would be potentiated by stress because of SLE disease activity or immunosuppressive drug use, and aimed to investigate the association between VZV reactivation, VZV antibody levels, lupus disease activity and immunosuppressive drug use.
Materials and methods
Study population
Serum samples, present in our biobank, from randomly selected SLE patients were used. Patients could be included in the study when they fulfilled American College of Rheumatology (ACR) criteria for SLE 21 and had a minimum age of 18 years at time of first serum sample. At least five samples per patient had to be present, with a minimum of one year between first and last sample. The study has been carried out in accordance with the principles of the Declaration of Helsinki. Approval by the medical ethics committee of the University Medical Centre Groningen was obtained and all patients gave informed consent.
Definition of VZV reactivation
In line with the definition of Ljungman et al., 18 a subclinical reactivation was defined as an at least fivefold increase in VZV-specific IgG antibody level or the occurrence of specific IgM (unless explained by presence of rheumatoid factor) without clinical signs of varicella or zoster. Moreover, we added the occurrence of VZV-DNA in serum to the existing definition. The definition of a clinical reactivation was the same as that of a subclinical one, but in the presence of clinical symptoms of herpes zoster. As VZV-specific IgA has been suggested to have some value in the diagnosis of herpes zoster, 16 we also analysed the course of antibodies of this isotype, but did not include it in the definition of a VZV reactivation.
VZV-specific antibody levels
For determining VZV-specific IgG, IgA and IgM levels, an in-house glycoprotein enzyme-linked immunosorbent assay (ELISA) was performed, which was validated previously. 10 VZV-purified glycoproteins (EastCoast Bio, North Berwick, ME, USA) were used as antigen, and pooled human serum with known levels of anti-glycoprotein VZV was used as standard. Threshold for positivity was set at 100 mIU/ml for VZV-specific IgG levels, at 50 U/ml for VZV-specific IgA levels and at 15 U/ml for VZV-specific IgM levels, according to recommendations of a commercial kit used for validating the in-house ELISAs (Institut Virion\Serion).
Detection of VZV-DNA
DNA was extracted from whole blood samples by the MagnaPure 96 system, using the MagnaPure 96 DNA and viral DNA small volume kit (Roche Applied Bioscience, Mannheim, Germany) according to the manufacturer’s instructions. Detection of VZV-DNA was performed using a previously described protocol. 22
Total IgG antibody levels
Total IgG antibody levels were determined using a commercial kit (Thermo Fisher Scientific, Waltham, MA, USA), following the manufacturer’s instructions.
Symptoms of herpes zoster
Medical records from included patients were checked for a history of herpes zoster during the follow-up period and at least two years before the first sample, when possible.
Statistics
Generalized estimating equations (GEE) were used to explore parameters associated with antibody levels over time. The exchangeable correlation matrix was used to take into account the within-patient correlations. In case residuals were non-normally distributed, the dependent variable was log-transformed before being entered into the analysis. Tested parameters included disease activity and immunosuppressive medication use over time. Systemic Lupus Erythematosus Disease Activity Index (SLEDAI, continuous and ≥ 5 for active disease), anti-double-stranded DNA (anti-dsDNA) and complement levels (C3, C4) were used as indicators of lupus disease activity. Medication use was tested overall (use of any immunosuppressive drugs) and for different drugs separately when used by at least five patients. Lastly, longitudinal associations between VZV-IgG and total IgG were investigated.
To be able to compare results from this study with results from studies using a cross-sectional sample, statistical analyses were also conducted when including the first available patient samples only. Associations between antibody levels (VZV-specific IgG and IgA, and total IgG), patient characteristics, medication use and disease activity parameters were explored by determining Spearman’s correlations coefficients in case of continuous variables and using the Mann–Whitney U test to compare differences between groups.
Statistical analysis was performed using IBM SPSS Statistics 23 (SPSS, Chicago, IL, USA). Figures were created using GraphPad Prism 5.0 (GraphPad Software, La Jolla, CA, USA). P values ≤ 0.05 were considered significant.
Results
Patient characteristics
Patient characteristics
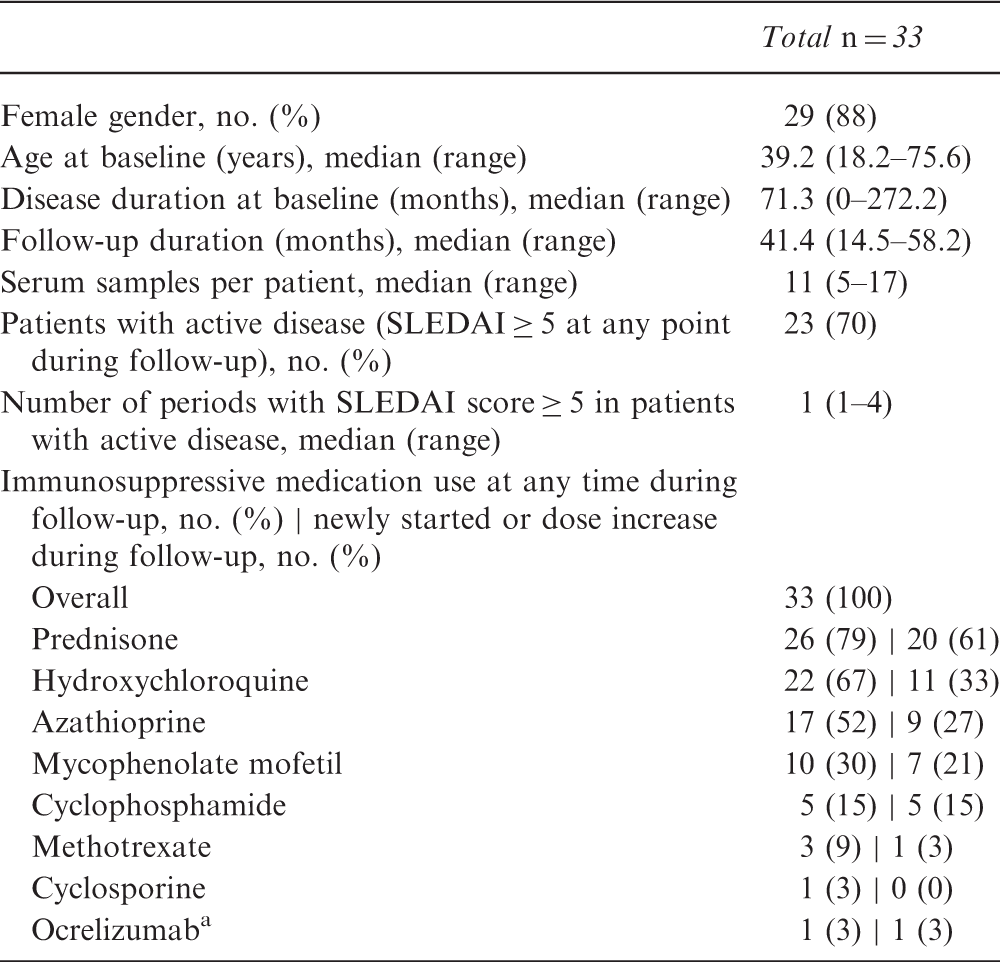
Used in a study setting.
SLEDAI: Systemic Lupus Erythematosus Disease Activity Index.
Longitudinal measurement of total IgG antibodies and VZV-specific antibodies
There was considerable variation in levels of VZV-specific IgG and total IgG between patients. Twenty-eight of 33 patients exceeded the normal upper limit of 16.0 g/l of total IgG at one or multiple times during follow-up. A total of 17 (52%) SLE patients had positive VZV-specific IgA levels (≥50 U/ml) at one or multiple time points during follow-up (data not shown). In two (6%) patients, levels of VZV-specific IgM above the threshold for positivity (15 U/ml) were found that could not be explained by presence of rheumatoid factor (data not shown).
Reactivations of VZV
Summary of findings in patients with a VZV-reactivation
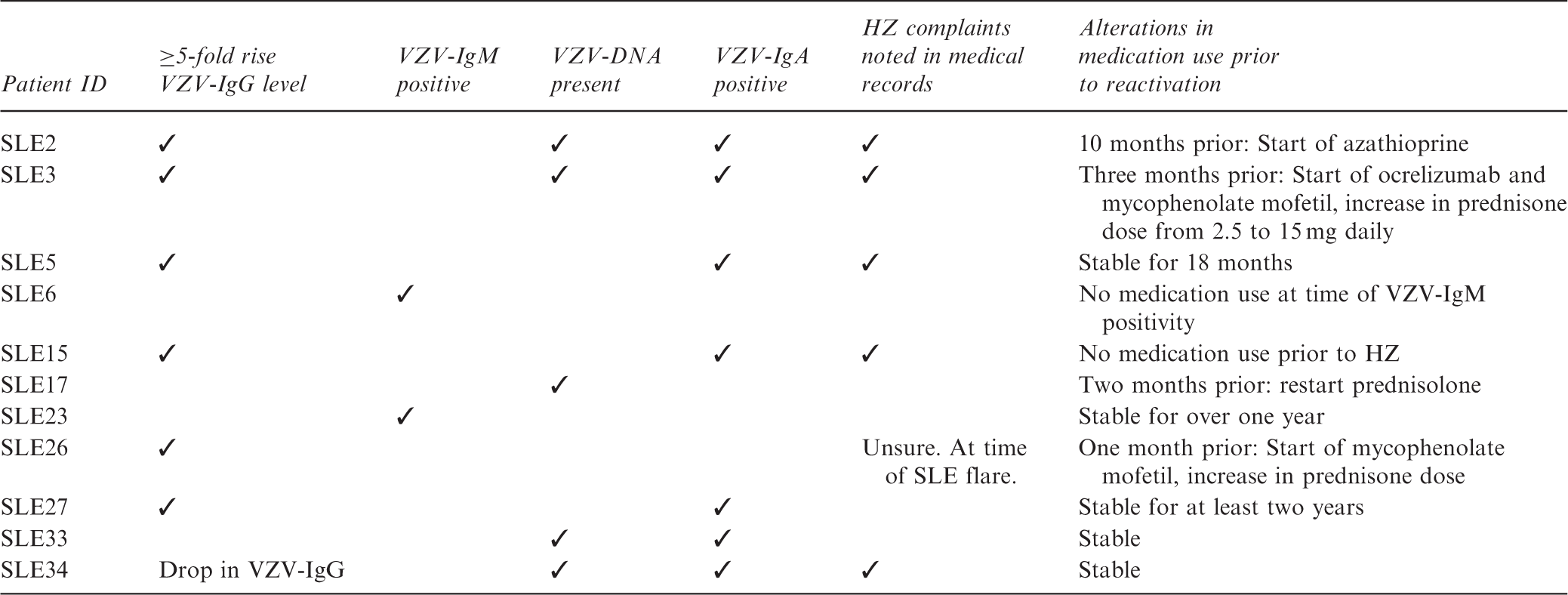
ID: identification; VZV: varicella-zoster virus; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; HZ: herpes zoster; IgG: immunoglobulin G.
In three patients (SLE3, SLE17 and SLE26) VZV reactivation was closely related to a change in medication (Table 2).
Supplementary figures of antibody levels, presence of VZV-DNA and anti-dsDNA (as a measure of lupus disease activity) for all patients with a VZV reactivation are available online.
Increases in VZV-specific IgG antibody level
Six patients had a ≥ 5-fold rise in VZV-specific IgG level (Table 2). Total IgG levels were stable at the time of VZV-specific IgG increases, indicating that large increases in VZV-specific IgG levels were not a consequence of increases in total IgG levels (data not shown).
In four of six patients with a VZV-IgG increase, clinical complaints matching herpes zoster were evident when reviewing medical records. For a fifth patient (SLE26), the VZV-IgG increases occurred during a severe SLE flare including skin manifestations and herpes zoster-like complaints could not be distinguished with certainty from the medical records retrospectively.
Figure 1 shows the last sample before a ≥ 5-fold VZV-specific IgG increase and course thereafter. Interestingly, VZV-specific IgG levels remained at increased levels for a long time and had not returned to original level after one year.
Last sample before ≥ 5-fold rise and the varicella-zoster virus (VZV)-specific immunoglobulin G (IgG) course thereafter in five systemic lupus erythematosus (SLE) patients, presented on a log-scale. Because the VZV-IgG rise in patient SLE5 occurred in the last sample, this patient is not included in the graph.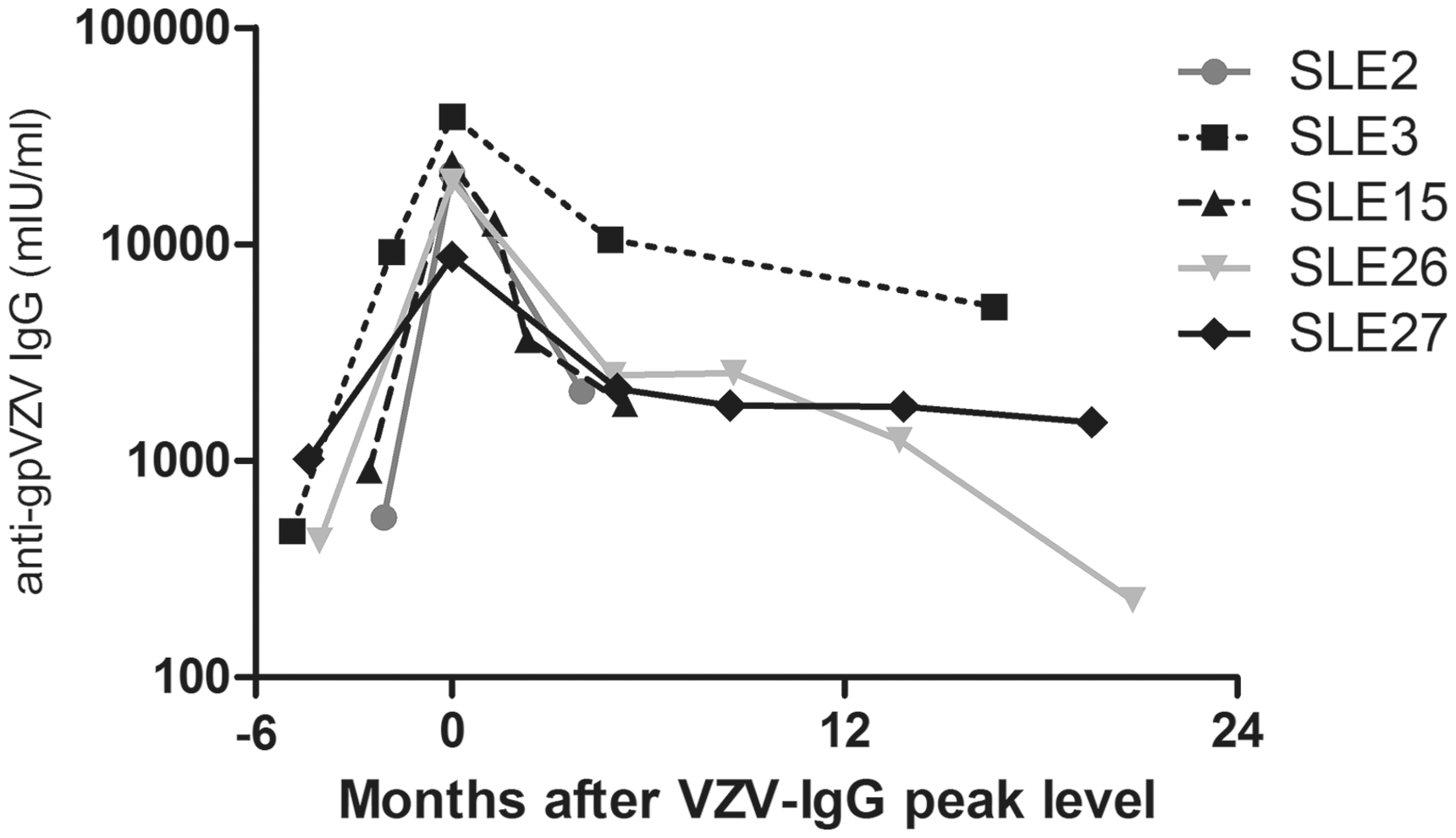
Presence of VZV-DNA in serum
VZV-DNA was detected in the serum of five patients. In two of those patients (SLE2 and SLE3) a ≥ 5-fold VZV-specific IgG level increase also was seen and they had clinically evident herpes zoster. In another patient (SLE34) a drop of VZV-specific IgG was seen at the time of VZV-DNA presence.
Presence of VZV-specific IgM antibodies
In two patients positive VZV-specific IgM levels were found. Patient SLE23 had a very high VZV-specific IgM value of 479 U/ml at one time point, rapidly decreasing at succeeding time points. Patient SLE6 had positive but decreasing VZV-specific IgM levels at the start of follow-up that lasted for over one year. At the same time VZV-specific IgG levels gradually decreased. No clinical signs of a VZV reactivation were present in these patients.
Presence of VZV-specific IgA antibodies
Levels of VZV-IgA above the threshold for positivity were found in 17 patients. The five patients with clinically evident herpes zoster all were VZV-IgA positive at that time. A rise in VZV-IgG usually co-occurred with a rise in VZV-IgA.
Longitudinal analysis of VZV-specific antibody levels
VZV-IgG levels were stable following SLE disease flare (including 11 patients with a minimum difference in SLEDAI of four points between intervals) (Figure 2).
Stable course of varicella-zoster virus (VZV)-immunoglobulin G (IgG) surrounding systemic lupus erythematosus (SLE) disease flare in 11 patients with a minimum difference in Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) of four points between intervals.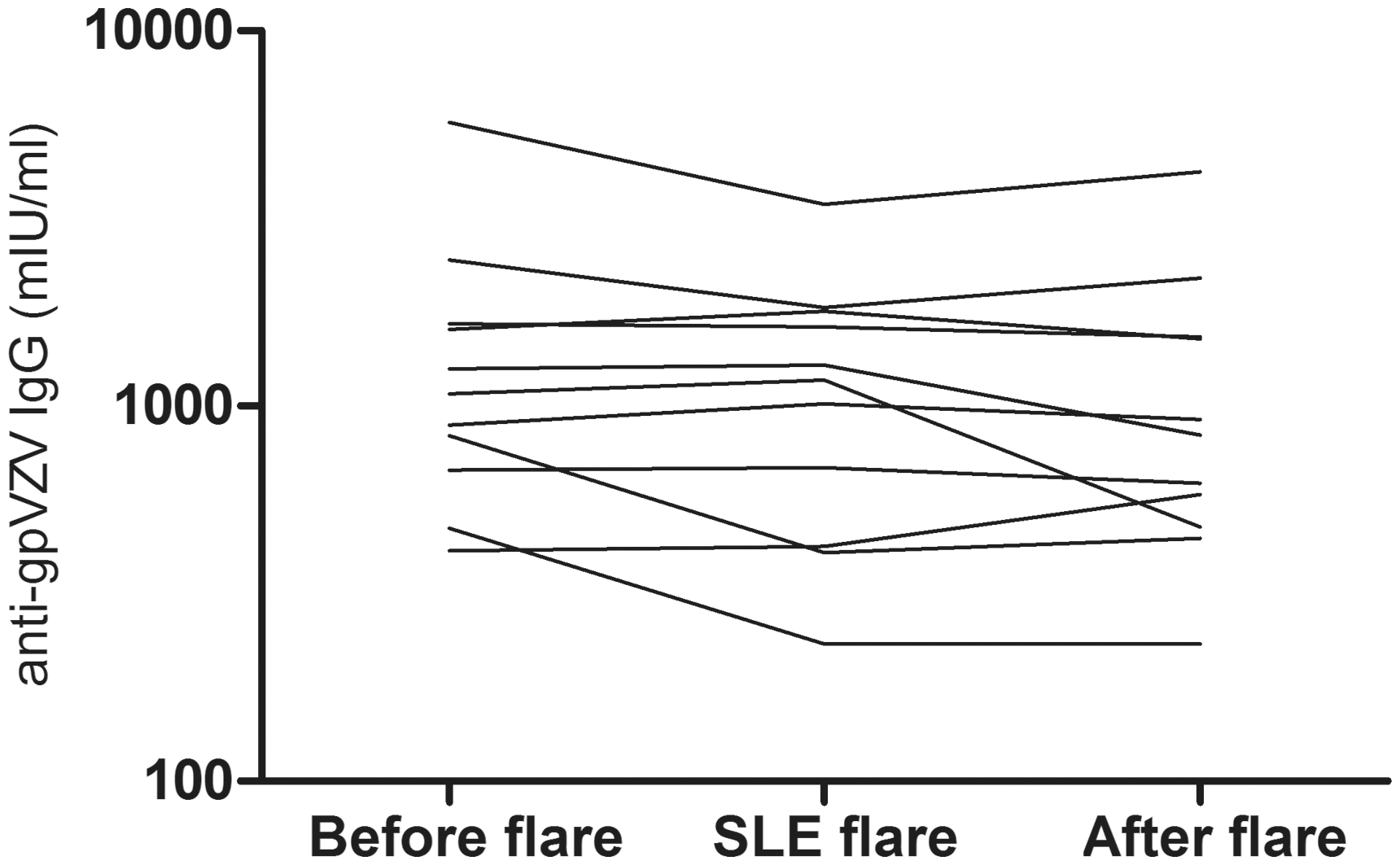
GEE analysis exploring the relationship of disease activity and medication use with VZV-IgG levels (log-transformed) over time in all patients and in patients without ≥ 5-fold rise in VZV-IgG
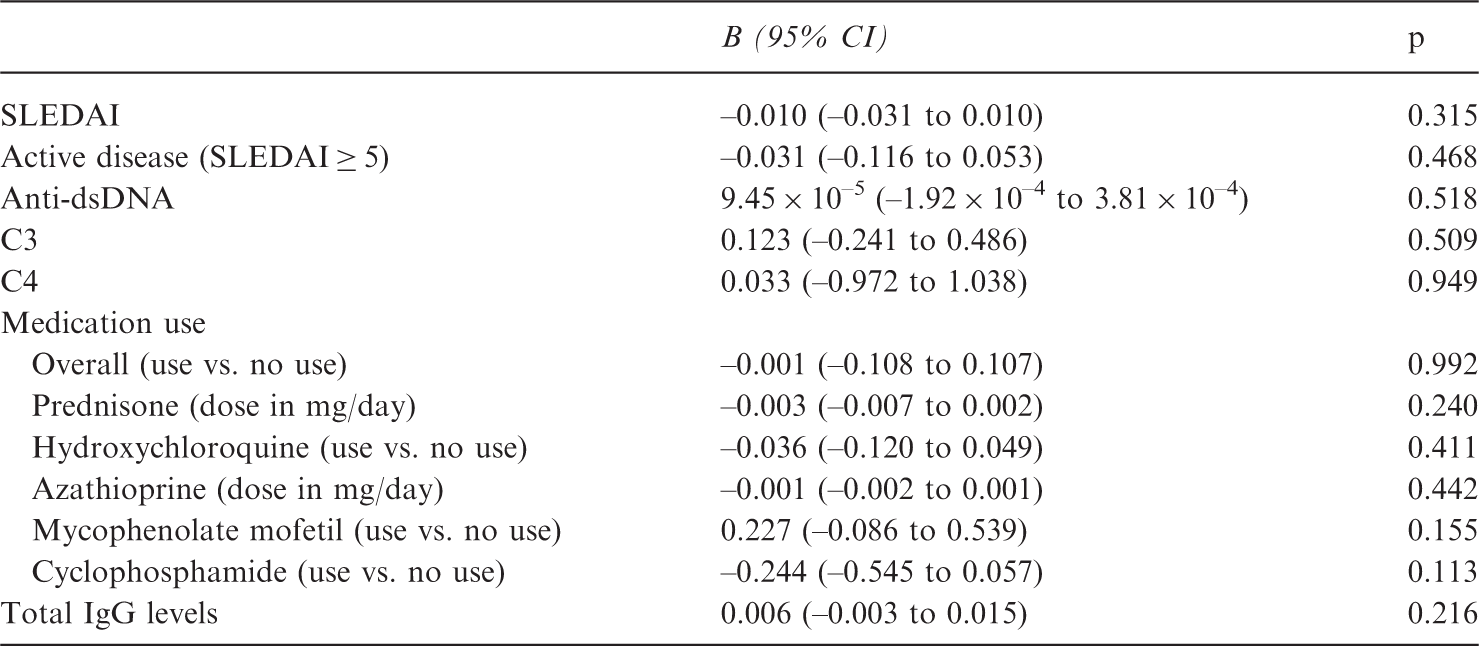
GEE: generalized estimating equations; CI: confidence interval; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; C3: complement 3; C4: complement 4; dsDNA: double-stranded DNA; IgG: immunoglobulin G; VZV: varicella-zoster virus.
Significant but very weak associations were revealed between VZV-specific IgA levels and anti-dsDNA levels or VZV-specific IgG levels using GEE (data not shown).
Parameters associated with total IgG levels over time
GEE analysis of variables of influence on total IgG levels was performed as a large variation was observed in total IgG levels between patients and also within patients over time, and a weak association between VZV-IgG and total IgG levels seemed to be present. This analysis revealed that overall medication use was inversely associated with total IgG levels. A negative association was shown for the use of prednisone, mycophenolate mofetil and cyclophosphamide.
GEE analysis exploring the relationship of disease activity and medication use with total IgG levels in all patients
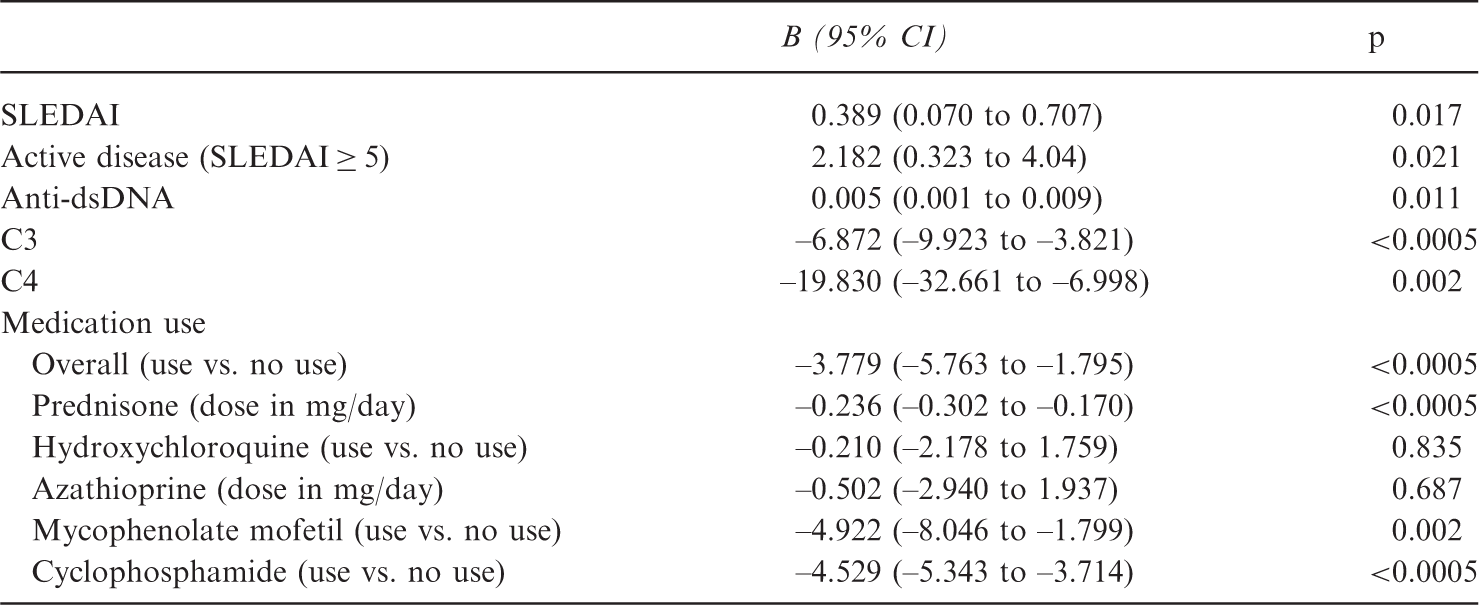
GEE: generalized estimating equations; C3: complement 3; C4: complement 4; CI: confidence interval; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; dsDNA: double-stranded DNA; IgG: immunoglobulin G. Significant associations are presented in bold.
Cross-sectional analysis using first available samples
To be able to compare our results with previous studies that used a cross-sectional approach, we analysed the first included samples per patient in a cross-sectional manner. In this analysis, a significant correlation between VZV-specific IgG and IgA levels was found (rho = 0.404), but not between VZV-IgG and total IgG. Another significant but inverse correlation was determined between VZV-specific IgG levels and C4 levels (rho = –0.360). No significant correlations between other parameters and VZV-IgG levels were found. For VZV-IgA levels, no significant correlations were noted with parameters other than VZV-IgG. Significant negative correlations were demonstrated between total IgG levels and prednisone dose (rho = –0.612) and C3 levels (rho = –0.459).
Discussion
The present study was initiated to clarify the cause of the elevated VZV-specific IgG levels in SLE patients. During longitudinal observation, in which 33 VZV-seropositive SLE patients were followed for a median duration of 41.4 months, one substantial (≥5 fold) VZV-IgG increase was observed without clinical symptoms of herpes zoster. It therefore seems unlikely that subclinical VZV reactivations play an important causative role in the origin of increased VZV-IgG levels in SLE. Furthermore, longitudinal analysis using GEE did not reveal an association between lupus disease activity or medication use and VZV-specific antibody levels.
In three patients we found a subclinical reactivation (one positive VZV-IgM, two presence of VZV-DNA) while VZV-IgG remained stable. Substantial increases in VZV-specific IgG level were shown in six patients, almost all coinciding with clinical symptoms matching herpes zoster, as assessed retrospectively by reviewing medical records. The increased VZV-IgG levels were shown to be long lasting, with high levels even after a year of follow-up. Also, in healthy individuals VZV-specific IgG is known to remain increased for months and even one year after herpes zoster.16,17
Medication use was found not to be associated with VZV-specific IgG levels over time, but was clearly shown to be negatively associated with total IgG levels. Although in three patients a close temporal relationship was seen between the start of a new drug and a VZV-reactivation, numbers are too low to draw firm conclusions.
When patients with a large increase in VZV-specific IgG values were excluded from the analysis, a weak association between VZV-specific IgG and total IgG levels was revealed that was not found in the cross-sectional analysis. This suggests that there can be some influence of general increased B-cell activity on the height of VZV-IgG values, but that this association is insufficient to completely explain the increased height of VZV-specific IgG values in SLE patients.
Our findings add valuable information to the debate on the role of human herpes viruses in the development and relapsing course of SLE. EBV especially has been implicated to be involved. 13 Increased antibody levels and impaired cellular immunity to EBV in SLE patients.23,24 were found, similar to our previous findings for VZV. 10 The elevated level of antibodies directed against lytic cycle antigens and an elevated level of EBV-DNA are suggested to indicate frequent EBV reactivations, and to contribute to the occurrence of SLE disease flares. 23 However, there is no direct evidence of this proposed link. The lack of an association between SLE disease activity and VZV reactivations in our study suggests that there is no etiologic role of VZV reactivations in the relapsing disease course of SLE. Further research is needed to investigate whether this also holds true for other human herpes viruses.
Although herpes zoster is usually diagnosed based on clinical symptoms, the diagnosis can be challenging, when rash is absent (e.g. zoster sine herpete, VZV encephalitis). Elevated levels of VZV-specific IgA have been proposed to be of some diagnostic value in these cases.16,25 VZV-specific IgA positivity was found in 17 out of 33 SLE patients at one or multiple time points during follow-up in our study, while only five patients were found to have clinically evident herpes zoster. The value of VZV-IgA in diagnosing herpes zoster therefore is questionable in SLE patients. VZV-specific IgM was shown to lack sensitivity when assessing its value in the diagnosis of herpes zoster in SLE patients.
This study has some limitations. Most important, because of the retrospective study design, clinical data regarding herpes zoster complaints could be missing from hospital medical records, as herpes zoster infections do not necessarily come to the attention of the treating specialist. Also, the study population consisted of patients with established disease, which made it impossible to study possible alterations in VZV-specific humoral immunity earlier in the disease course. Furthermore, the definition of a subclinical reactivation is arbitrary and intervals between measurements were not standardized. We believe we have used a broad definition, based on the study by Ljungman et al., 18 including ≥ 5-fold VZV-IgG increases, positivity of IgM and the addition of VZV-DNA.
A strength of the study is the use of GEE analysis in looking for associations between VZV antibody levels, disease activity and medication use. The GEE analysis was independent from the arbitrary definition of subclinical reactivation and this type of analysis is suitable for analyses of data with non-standardized intervals.
Concluding, our study results do not support the hypothesis that the increased VZV-specific antibody levels in SLE patients are caused by subclinical VZV reactivations or are related to SLE disease activity or medication use during established disease. Although generally increased B-cell activity seems to influence the height of VZV-IgG values, this association is insufficient to completely explain the increased height of VZV-specific IgG values. Our findings might suggest an origin earlier in the disease process. Despite the limitation of a retrospective design, this study adds to the understanding of the humoral response to VZV in this patient group at increased risk of herpes zoster.
Supplemental Material
Supplementary Figures -Supplemental material for Longitudinal analysis of varicella-zoster virus-specific antibodies in systemic lupus erythematosus: No association with subclinical viral reactivations or lupus disease activity
Supplemental material, Supplementary Figures for Longitudinal analysis of varicella-zoster virus-specific antibodies in systemic lupus erythematosus: No association with subclinical viral reactivations or lupus disease activity by C Rondaan, C C van Leer, S van Assen, H Bootsma, K de Leeuw, S Arends, N A Bos and J Westra in Lupus
Footnotes
Acknowledgements
The authors thank Alicia Borneman and Elisabeth Eelsing for their assistance in performing ELISAs, and Dr Fiona Maas for her help with GEE analyses.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the J.K. de Cock Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.