
Abstract
Background
A considerable portion of acutely intoxicated patients is presented with impaired consciousness. Early identification of those patients who require advanced medical care, such as mechanical ventilation (MV), can improve their prognosis.
Methods
This study included 330 acutely intoxicated patients who were presented with impaired consciousness and admitted to Tanta University Poison Control Center, Egypt, in the period from January 2021 to December 2023. Patients were enrolled in derivation (257 patients) and validation (73 patients) cohorts. Patients’ data were analyzed to develop and validate a predictive nomogram to determine the probability of MV need in acutely intoxicated patients.
Results
Significant predictors for MV need were mean arterial blood pressure (OR = 0.96, p = .014), PaO2 (OR = 0.96, p = .001), pH (OR = 0.00, p < . 001), and glucose/potassium ratio (OR = 1.59, p = .030). These four parameters were used to formulate a bedside nomogram. Receiver-operating characteristic (ROC) analysis for the proposed nomogram shows that area under the curve (AUC) = 95.7%, accuracy = 93.4%, sensitivity = 88.9%, and specificity = 95.1%. The internal validation for the developed nomogram was assessed using a bootstrapping method and calibration curve. Regarding external validation, AUCs for the developed nomogram probability was 96.5%, and for predicted probability using the developed nomogram was 97.8%.
Conclusion
The current study provides a validated nomogram that could be used as a reliable tool for the accurate prediction of MV need among acutely intoxicated patients with impaired consciousness. It could assist in the early identification of patients who will require MV, especially in low-income countries with limited resources.
Introduction
Acute poisoning stands behind high morbidities and mortalities across different societies worldwide. The higher percentages of poisoning-related fatalities were reported among low-income countries and attributed to the limited resources in healthcare institutes, along with the high prevalence of pesticides and household poisoning. 1
A disturbed level of consciousness is a commonly reported toxicological emergency. Notably, a wide range of poisons could result in disturbed sensorium either through direct inhibition of the central nervous system (CNS) or indirectly through impairing cerebral perfusion or inducing metabolic derangements. 2
In managing critical cases of poisoning, life-saving measures could involve mechanical ventilation (MV). It is essential to consider that adequate numbers of mechanical ventilators might be unavailable in low-income countries, particularly in rural areas with a high prevalence of lethal poisoning. Indeed, the timing of patients’ transfer to hospitals with available ventilators is a critical determinant of the patient outcome. Thus, utmost attention should be paid to the early identification of intoxicated patients who will require MV. In this context, different clinical scores were used as reliable predictive tools.3,4
Risk-prediction nomograms are applicable predictive models that guide medical decisions in clinical settings. Nomograms are essentially graphical calculators that display regression coefficients of multivariable regression models. They allow simple manual calculation of the probabilities of adverse events. The length of the scale on the nomogram is proportional to the importance of each variable in predicting the outcome, with longer scales indicating higher importance.5,6
Nomograms have been widely used in predicting the outcomes of managing pathological conditions.7–9 In recent years, nomograms have also been introduced to the field of clinical toxicology, specifically for predicting the outcomes in acutely intoxicated patients, such as mortality and ICU admission.10,11 Additionally, nomograms have been adopted to predict the prognosis of intoxication with particular poison categories, including pesticides,12,13 CNS xenobiotics, 14 antipsychotics,15,16 and cardiac glycosides. 17 The current study aimed to develop a predictive nomogram that utilizes easily accessible data to determine the probability of MV need among intoxicated patients with impaired consciousness.
Patients and methods
Study setting
The present study involved the electronic medical records of acutely intoxicated patients presented with impaired consciousness and admitted to Tanta University Poison Control Center (TUPCC) in the period from January 2021 to December 2023. This tertiary healthcare center serves Gharbia and other neighboring governates in and around the Delta region, one of Egypt’s most densely populated places. 18
Study design
This study was conducted on two cohorts: the retrospective derivation cohort and the prospective validation cohort. The nomogram derivation cohort included the medical records of acutely intoxicated patients who presented with impaired consciousness from January 2021 to June 2023, whereas the nomogram validation cohort enrolled patients who were admitted during the next 6 months from July to December 2023.
Sampling
Convenience sampling was adopted. The sample size was calculated using the Epi Info-7 program, 19 by adjusting power at 80%, confidence level 95%, and the incidence of MV need in self-poisoned patients was 11.2%. 20 The minimum estimated sample size was 153 patients. However, during the review of the available medical records in the study period, 104 patients met the inclusion criteria, and their medical records were enrolled in this study analysis to reach a sample of 257 patients, which increased the power of the study.
The following formula was used:
Where; • S = sample size for infinite population • Z = Z score (1.96) • P = population proportion (0.112) • M = Margin of error (0.05)
Inclusion criteria
The current study included all acutely intoxicated patients aged 18 and above of both genders who were admitted to TUPCC with impaired consciousness during the study period. Impaired consciousness was defined as GCS < 15. 21 Patients were included regardless of the manner of exposure. According to World Health Organization guidelines, diagnosing acute poisoning is based on a history of poison exposure or recognizing the drug(s), container(s), or characteristic toxicological manifestations by clinical examination. Also, the relevant investigations were conducted. 22
Exclusion criteria
Patients under 18 years or those with full consciousness levels (GCS = 15) were excluded. Moreover, patients who had concomitant head trauma or pathological conditions, such as neurological, cardiac, hepatic, or renal diseases, were excluded. In addition, the patients who received pre-hospital treatment or were discharged against medical advice were not included in the study. Also, cases with incomplete medical records were excluded as well. The recruitment process for patients enrolled in the present study is illustrated in Figure 1. Flowchart illustrating the recruitment process for patients enrolled in the present study.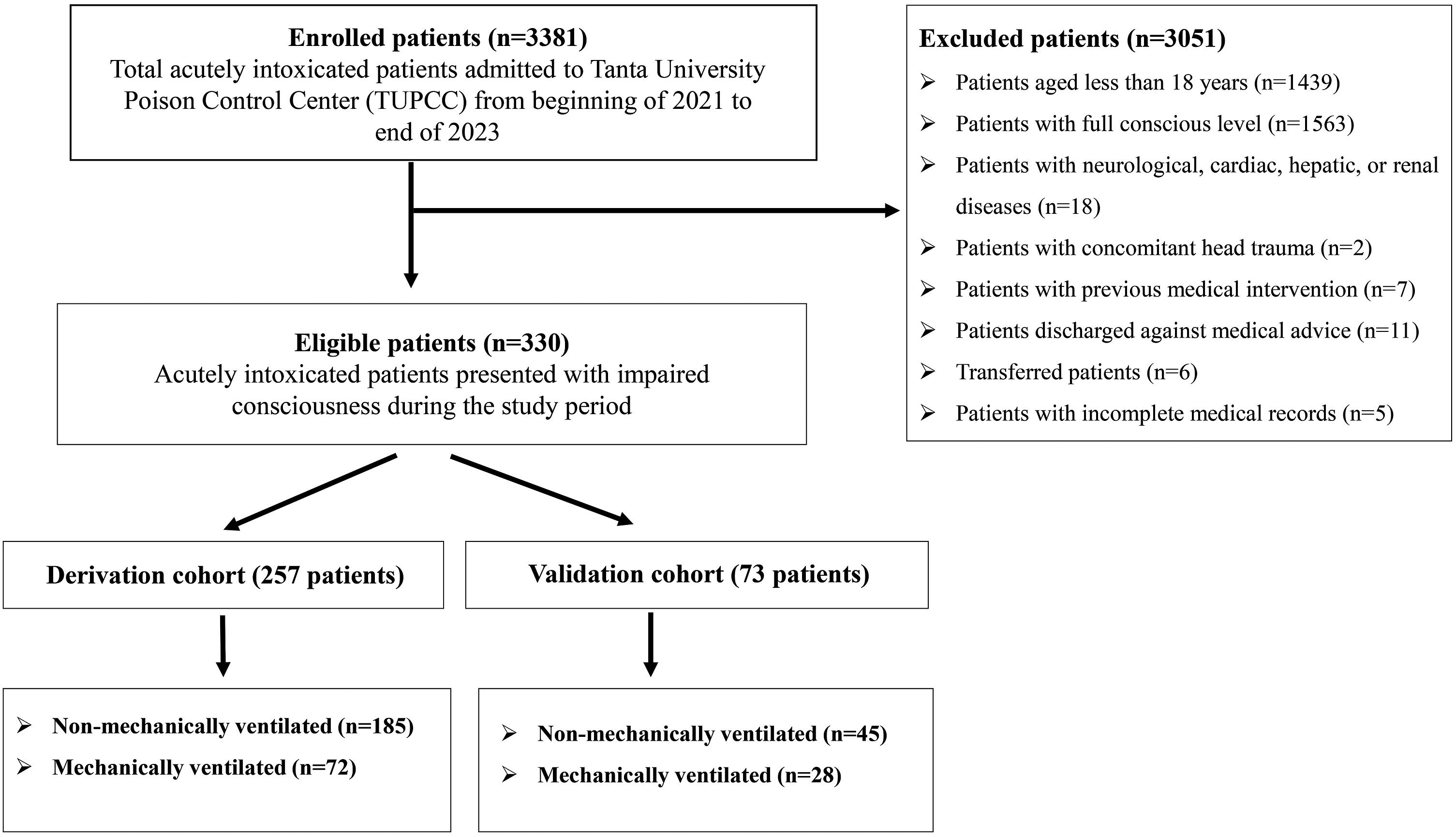
Ethical consideration
The present research was ethically approved by the Research Ethical Committee at the Faculty of Medicine, Tanta University (Approval number FWA00022834, IRB0010038/36264PR264/7/23). Based on the Declaration of Helsinki and its later amendment, written informed consent was taken from patients’ legal guardians in the validation cohort because these patients were incompetent due to their impaired consciousness. The authors strictly preserved the confidentiality of the personal data of the studied patients.
Data collection tool
Characteristics of the patients and clinical manifestations
The collected data included the patient’s demographics, toxicological history, and the time between exposure to the poison and receiving medical care in the poison center. Moreover, the patient’s symptoms and signs upon admission were reported.
Furthermore, the values of the vital signs on admission were extracted from the patient’s records and assessed according to their reference ranges. 23 Additionally, the values of the Glasgow Coma Scale (GCS) 24 and the Poison Severity Score (PSS)25,26 were extracted as assessed and reported by the treating physician in each patient’s medical file. Besides, any abnormal electrocardiography (ECG) findings, length of hospital stay, and occurrence of in-hospital mortality were reported.
Laboratory investigations
The first values of routine laboratory investigations for the enrolled patients were extracted, including measured arterial blood gases, random blood glucose levels, serum electrolytes, Glucose/Potassium (Glu/K) ratio, liver transaminases, serum urea, serum creatinine, and complete blood count (CBC).
Outcome (Mechanical ventilation)
The patients in every cohort were categorized according to MV need. MV was initiated when patients have one or more of the following indications: airway protection for patients with impaired consciousness, presence of hypoxemic or hypercapnic respiratory failure, and hemodynamic instability, in which MV can decrease the oxygen burden of breathing.20,27,28
Data analysis
The collected data was fed to R statistical software version 4.2.2, “Innocent and Trusting.” Normality assumptions were checked using the Shapiro–Wilk test. Descriptive analyses were conducted between mechanically ventilated and non-mechanically ventilated patients using a two-sample t-test or Wilcoxon rank sum test for continuous variables and a Chi-squared or Fisher’s exact test for categorical ones. p value < .05 was considered statistically significant. The power analysis was done via the “pwr” and “lsr” packages in R Language for Statistical Computing version 4.2.2.
Development and validation of the nomogram
A univariate binomial logistic regression model was performed using the patients’ data in the derivation cohort to investigate the potential risk factors associated with the MV need. Then, a multivariate logistic regression model was done for all significant variables in the baseline statistics after excluding the following: • Systolic and diastolic blood pressures to avoid multicollinearity with mean arterial blood pressure (MAP). • Random blood glucose and serum potassium levels to avoid multicollinearity with Glu/K ratio. • Oxygen saturation to avoid multicollinearity with PaO2. • PSS to avoid multicollinearity with other predictors.
The remaining significant predictors for MV need were used to develop the multivariate model, a Kattan-style nomogram. 6 The developed nomogram was internally validated by bootstrapping method (1000 bootstrap replicates) to calculate bias-corrected and accelerated confidence intervals (BCa 95% CI) as an average of the coefficients (β) differences. 29 A receiver-operating characteristic (ROC) analysis was conducted to test the predictive accuracy of the developed nomogram and validate its performance internally on the derivation cohort. In addition, the area under the curve (AUC) was carried out using optimism-adjusted discrimination and calibration by the Hosmer and Lemeshow goodness of fit test.
External validation was performed using a validation cohort via ROC analysis to ascertain the generalizability of the developed nomogram. In addition, ROC analyses were conducted for each predictor included in the corresponding logistic regression model developed in both the derivation and validation cohorts to be compared with the AUCs of the predicted probability of the developed nomogram in both cohorts.
Interpretation of the nomogram
The nomogram contains four types of scales. The first scale is a points scale, followed by one scale for every individual predictor, followed by a total points scale, and finally, there is the need for an MV probability scale. Four steps should be carried out to detect the need for MV probability: First, the patient’s actual value for every predictor is marked on its specific scale. Second, imaginary perpendicular lines are drawn from the marks on the particular predictor scales upwards to the point scale with the marking of the corresponding points. Third, the sum of the marked points for every predictor is calculated, and then a mark is made opposite to the total sum value on the total points scale. Finally, an imaginary perpendicular line is drawn downwards from the previous mark on the total points scale to the probability scale, indicating the patient’s need for MV probability. 11
Results
The current study included 330 acutely intoxicated patients with impaired consciousness who were enrolled in both derivation (257 patients) and validation (73 patients) cohorts, as illustrated in Figure 1. Among the derivation cohort, 72 patients (28%) required MV, while 28 (38.4%) required MV in the validation cohort.
Comparative analysis for baseline demographics, toxicological history, presenting manifestations, hospitalization period and in-hospital mortality regarding the need for mechanical ventilation among derivation and validation cohorts.

*: Significance at p < .05.
Data are represented as median (IQR, interquartile range), mean (SD, standard deviation) or numbers (n; percent); P 1 : for derivation cohort; P 2 : for validation cohort; P 3 : for derivation versus validation cohorts.
Oral intake of the poison was the mainstay route of exposure in the great majority (89.5%) of the derivation cohort. However, inhalation and injection of poisons were significantly more prevalent among mechanically ventilated patients (p < .001). Considering the manner of exposure, poisoning with suicidal intent represented 86.4% of the cohort. Drug overdose was reported among 23.6% of mechanically ventilated patients and only 4.3% of non-mechanically ventilated patients (p < .001). There were significant variations between mechanically ventilated and non-mechanically ventilated patients regarding neurological, respiratory and gastrointestinal manifestations (p < .05). The overall mortality proportion in the derivation cohort was 14%, and most of the mortalities (94.4%) were among mechanically ventilated patients.
Comparative analysis for vital signs, patients’ scoring and ECG findings regarding the need for mechanical ventilation among derivation and validation cohorts.

*: Significance at p < .05.
Data are represented as median (IQR, interquartile range), mean (SD, standard deviation) or numbers (n; percent); GCS: Glasgow Coma Scale; PSS: Poisoning Severity Score; ECG: Electrocardiogram; P 1 : for derivation cohort; P 2 : for validation cohort; P 3 : for derivation versus validation cohorts.
Comparative analysis for laboratory investigations regarding the need for mechanical ventilation among derivation and validation cohorts.

*: Significance at p < .05.
Data are represented as median (IQR, interquartile range), mean (SD, standard deviation) or numbers (n; percent); PaO2: Partial arterial oxygen pressure; PaCO2: Partial arterial carbon dioxide pressure; HCO3: Bicarbonate; AST: Aspartate aminotransferase; ALT: Alanine aminotransferase; Glu/K ratio: Glucose/Potassium ratio; P 1 : for derivation cohort; P 2 : for validation cohort; P 3 : for derivation versus validation cohorts.
Tables 1–3 illustrate no statistical differences between derivation and validation cohorts concerning age, gender, residence, route and manner of exposure, delay time, and hospitalization period. Moreover, the patient’s vital signs, scoring (GCS and PSS), and ECG findings on admission have no significant variations between the studied cohorts. Most laboratory investigations showed no significant variations between derivation and validation cohorts (p > .05).
Univariate and multivariate logistic regression models to investigate potential risk factors for mechanical ventilation among the derivation cohort.

*: Significance at p < .05.
CI: confidence interval; OR: odds ratio; PaCO2: Partial arterial carbon dioxide pressure; HCO3: Bicarbonate; Glu/K ratio: Glucose/Potassium ratio.
Figure 2 illustrates that the baseline comparative analysis between derivation and validation cohorts had non-statistically significant differences regarding MAP, PaO2, pH, and Glu/K ratio. These parameters were used to develop a bedside on-admission nomogram predicting the need for MV among acutely intoxicated patients with impaired consciousness (Figure 3(a)). An actual patient’s data was used to demonstrate how to estimate the patient’s probability of needing MV through the proposed nomogram (Figure 3(b)). The developed nomogram cut-off point = 0.332, equivalent to 98 total points, exhibited the highest AUC (95.7%) than the predictors from the logistic regression model individually (Table 5). Comparative analysis of the four nomogram predictors (MAP, PaO2, pH, and Glu/K ratio) between derivation and validation cohorts. (a) Risk prediction nomogram for the need for mechanical ventilation among acutely intoxicated patients with impaired consciousness (derivation cohort). (b) Using the developed nomogram to predict the probability of requiring mechanical ventilation in an acutely intoxicated patient with impaired consciousness. His on-admission parameters included MAP = 60 mmHg, PaO2 = 85 mmHg, pH = 7.3, and Glu/K ratio = 4.1. The probability was estimated as follows: MAP of 60 mmHg corresponds to 22.5 points, PaO2 of 85 mmHg corresponds to 40 points, pH of 7.3 corresponds to 30 points, and Glu/K ratio of 4.1 corresponds to 20 points. The sum of these patient points is 22.5 + 40 + 30 + 20 = 112.5 points, which means 75% associated risk of need for mechanical ventilation. ROC analysis for the need for mechanical ventilation prediction nomogram and variables from logistic regression model in derivation cohort. *: Significance at p < .05. AUC: Area under the ROC Curve; CI: confidence interval; PPV: positive predictive value; NPV: negative predictive value; MAP: Mean arterial blood pressure; PaO2: Partial arterial oxygen pressure; Glu/K ratio: Glucose/Potassium ratio.


Multivariate logistic regression model for developing a nomogram predicting the need for mechanical ventilation among the derivation cohort.

*: Significance at p < .05.
OR: odds ratio; CI: confidence interval; BCa: bias corrected accelerated; AUC: Area under the ROC Curve; MAP: Mean arterial blood pressure; PaO2: Partial arterial oxygen pressure; Glu/K ratio: Glucose/Potassium ratio.

Calibration curve evaluating the accuracy of the developed nomogram in predicting the need for mechanical ventilation.
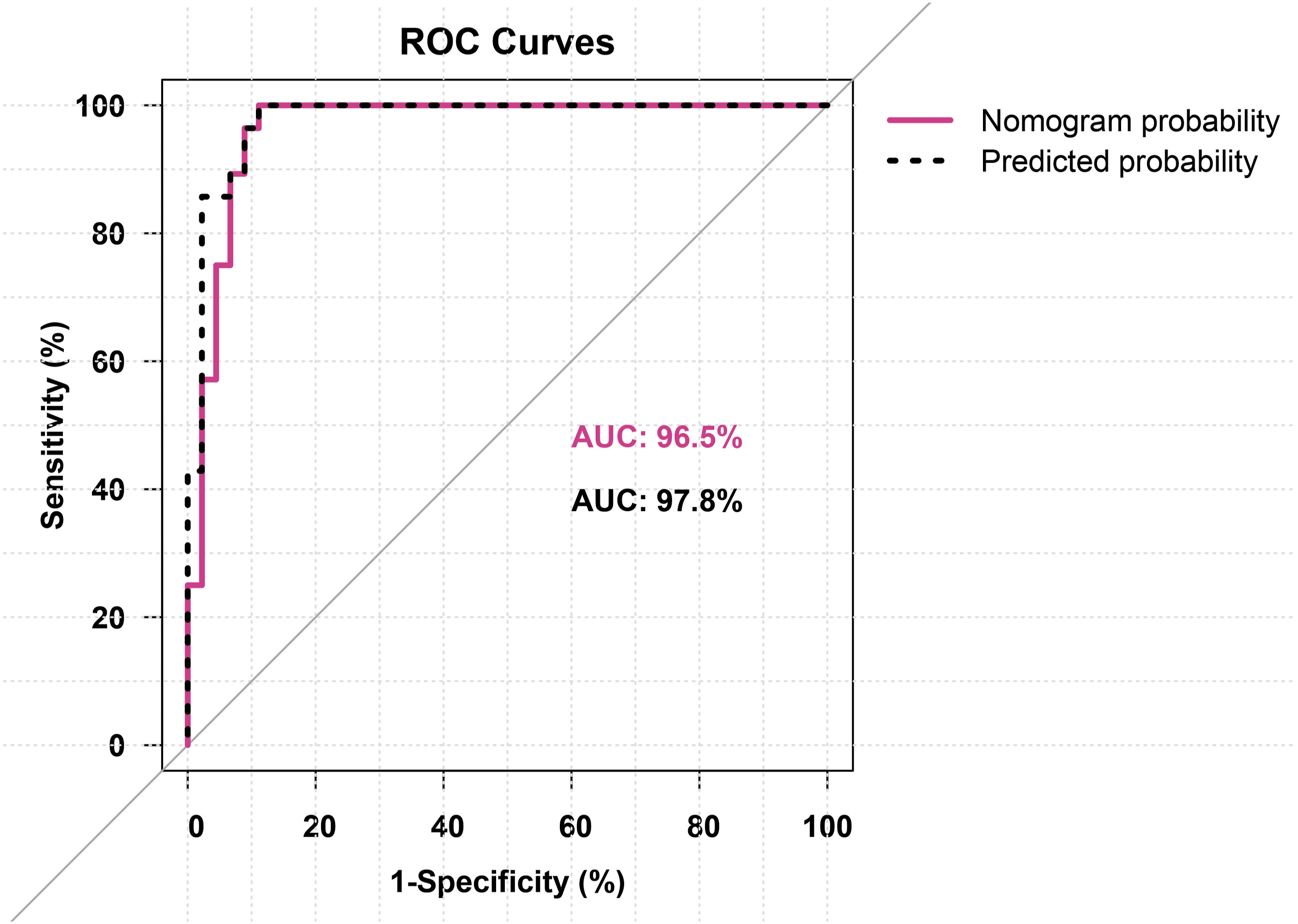
Figure 5 shows the external validation of the developed nomogram by comparing its predictive ability with that of the validation cohort and derivation cohort. The cutoff point of the developed nomogram predictive ability on the validation cohort = 0.146, equivalent to 90 total points exhibiting the highest AUC (96.5%) than the predictors from the corresponding logistic regression model developed in the validation cohort individually (with maximum AUC = 94.3%) as shown in Table 7. Moreover, Figure 6 illustrates the discriminatory power of the developed nomogram probability to predict the need for MV in the validation cohort and the predicted probability using the developed logistic regression model. The AUC for the developed nomogram probability was 96.5% with a 95% CI of 92.5–100 (p < .001). While the AUC of the predicted probability using the developed model was 97.8% with a 95% CI of 94.9–100 (p < .001). ROC curves for the developed nomogram in derivation and validation cohorts. ROC analysis for the developed nomogram and variables from logistic regression model in validation cohort. *: Significance at p < .05. AUC: Area under the ROC Curve; CI: confidence interval; PPV: positive predictive value; NPV: negative predictive value; MAP: Mean arterial blood pressure; PaO2: Partial arterial oxygen pressure; Glu/K ratio: Glucose/Potassium ratio. ROC curves validate the discriminatory power of the developed nomogram, which predicts the need for mechanical ventilation in the validation cohort.

Post-hoc power analysis
In the derivation cohort, the study investigated the risk factors associated with needing MV in acutely intoxicated patients with impaired consciousness. Considering the MAP, PaO2, pH, and Glu/K ratio were the significant nomogram risk factors, the pooled effect sizes (Cohen’s d) between the two study groups were 1.31, 1.44, 1.84, and 0.92, respectively, for the above predictors that considered very large ones. So, the detected post-hoc power (1-β) for a sample size (257 patients) at a 5% level of significance is approximately = 1 using any of the mentioned nomogram predictors.
In the validation cohort, the pooled effect sizes (Cohen’s d) were 1.28, 1.9, 1.82, and 0.98, respectively, considered very large too and the detected post-hoc power (1-β) for a sample size (73 patients) at 5% level of significance approximately = 1 using any of the mentioned nomogram predictors indicating sufficient power in both derivation and validation cohorts and therefore proving adequate sample sizes.
Discussion
Improving the outcome of intoxicated patients includes early identification of patients who are most likely to deteriorate and require advanced medical care. Thus, applying predictive models allows the immediate transfer of high-risk, poisoned patients to healthcare institutes with adequate facilities, including mechanical ventilators.3,4
Noteworthy, a considerable portion of poisoned patients are presented with impaired sensorium, as various poisons could diminish the level of consciousness. 2 In such cases, the patients might not be able to mention the name of the poison, and they could not express their complaints if their condition worsens. Thus, it is valuable to adopt a universal predictive model that could be applied to any intoxicated patient presented with disturbed consciousness, regardless of the causative poison.
Nomograms are regression models that yield a single numerical approximation for the patient’s condition. They represent simple and quick tools over the conventional clinical scores to identify high-risk patients.10,11 Thus, the current study proposed a risk-prediction nomogram to early identify intoxicated patients with a high probability of needing MV. The adopted model was subjected to internal and external validation to ensure its reliability and reproducibility.
This research started with an enrolment of 257 acutely intoxicated patients with disturbed sensorium that considered derivation cohort. A considerable portion (28%) of these patients were mechanically ventilated. Similarly, an Egyptian study conducted by El-Sarnagawy and Hafez mentioned that 23% of intoxicated patients required MV. 3 Also, in Taiwan, Shen et al. stated that 23.4% of intoxicated patients included in their study required MV. 30 On the other hand, Günaydın et al. reported that only 1.1% of intoxicated patients in Turkey were mechanically ventilated 31 ; such variation in the results could be attributed to differences in poisoning patterns among countries.
The current study showed that a significantly higher number of mechanically ventilated patients were from rural areas. This could be explained by the high prevalence of poisoning with highly toxic pesticides, including aluminum phosphide and cholinesterase enzyme inhibitors, in agricultural towns.32,33
Antipsychotics were the commonest poison categories that induced a disturbed level of consciousness. It is noteworthy that several recent studies pointed to the high incidence of antipsychotic poisoning in Egypt, which complies with the current research.16,34–36 Nevertheless, aluminum phosphide was the most common poison that mandated MV among exposed patients. Indeed, aluminum phosphide is a highly toxic metal phosphide with high mortalities that necessitates advanced life-supportive measures, including MV, as reported in the literature.37–42 Opioids were the second most common poison that induced severe toxicity and necessitated MV. It is worth mentioning that opioid compounds are commonly abused substances in Egypt, including heroin, tramadol, and Strox.43,44 These substances are often smoked, inhaled, or injected, which explains why inhalational and parenteral poisoning was significantly prevailing among mechanically ventilated patients.
Among the derivation cohort, logistic regression analysis was conducted to unveil the risk factors for MV need among intoxicated patients with disturbed sensorium. Then, a predictive nomogram was formulated using four parameters: MAP, PaO2, pH, and Glu/K ratio. These four parameters were selected statistically because of their high discriminative powers. In addition, including these four parameters in a single regression model increases the discriminative power to 95.7%. Also, the quantitative nature of these four laboratory parameters eliminated any potential subjectivity.
From a clinical point of view, MAP, PaO2, pH, and Glu/K ratio values are always convenient as these parameters are routinely measured for all poisoned cases on admission, even in small healthcare facilities. In addition, using a nomogram that considers the patients' hemodynamic stability, acid-base status, and metabolic homeostasis is clinically justifiable.
Mean arterial blood pressure indicates hemodynamic instability, and hypotension is frequently reported among patients with impaired consciousness. 21 Also, unresponsive hypotensive shock is one of the indicators of MV need. 28 In concordance with the current results, Elgazzar et al. included blood pressure to formulate predictive nomograms for ICU admission of acutely intoxicated patients. 10
In addition, PaO2 and pH denote the acid-base status of the acutely poisoned patients. Severe hypoxia and respiratory acidosis are among the indications of MV need. 45 Therefore, these two parameters were included in a nomogram as their early changes on admission could be alarming signs of respiratory function deterioration.
Regarding the Glu/k ratio, there is an inverse relationship between blood glucose and potassium levels. Hyperglycemia promotes the intracellular shifting of potassium and hypokalemia. Subsequently, literature pointed to the Glu/k ratio as a reliable predictor of adverse outcomes of various toxicities that comply with the current results. Demirtaş et al. proved that the Glu/k ratio could predict delayed neurological sequelae following carbon monoxide poisoning. 46 In 2022, Sharif et al. used this ratio to predict intermediate syndrome following exposure to cholinesterase inhibitor pesticides. 33 Also, a recent study applied this ratio to predict the occurrence of life-threatening events among patients poisoned with methylxanthines. 47
Validation is essential to verify the reliability and reproducibility of risk-prediction models. 48 Thus, the proposed nomogram was subjected to internal and external validation. The internal validation was verified using the bootstrapping method, and the calibration curve illustrated that the adopted nomogram’s performance was accepted. The external validation of the developed nomogram performance was tested using the validation cohort. ROC analysis revealed that the AUC of the nomogram was 96.5%, close to that of the developed nomogram (95.7%), which denoted the developed nomogram’s validity. Also, the four predictors included in the derivation nomogram were used to formulate another regression model using a validation cohort. The predicted probability was 97.8%, confirming the predictive power of the four parameters encompassing the nomogram. In addition, post-hoc power analysis revealed large pooled effect sizes of nomogram risk factors and proved sufficient statistical power in derivation and validation cohorts.
Because of the importance of predicting MV need in poisoned patients, El-Sarnagawy and Hafez compared the accuracy of the GCS, rapid acute physiology score (RAPS), acute physiology and chronic health evaluation (APACHE II), and rapid emergency medicine score (REMS) to predict the need of acutely intoxicated patients for MV. 3 Also, Abd Elghany et al. developed and validated the Poisoning Agitation-Sedation Score (PASS) to predict the need for MV among poisoned patients with disturbed sensorium. 4
The current study provided a validated nomogram that could be applied to acutely intoxicated patients with impaired consciousness to predict their need for MV early. In the context of MV-related issues, Shen et al. 30 predicted the duration of MV in patients with carbon monoxide poisoning using a regression model. In addition, Assaf et al. 49 predicted weaning from MV in acutely intoxicated patients in Egypt.
The main limitation of the present work is being a uni-centered study, as both derivation and validation cohorts were recruited from TUPCC. Thus, we recommended future studies that enroll patients from multiple poison centers, particularly for external validation cohorts. In addition, the inclusion of patients intoxicated with different poison categories is an inherited limitation either in the current study or other studies that predicted adverse outcomes of acute poisonings, such as MV need,3,4 and mortality.50,51 The presence of significant differences in some individual parameters between derivation and validation cohorts was another inevitable limitation either in the current study or in other studies with similar designs.32,52 Yet, the implementation of appropriate statistical analyses ensures results reliability.
Conclusion
The current study provided a validated nomogram that predicts the need for MV among acutely intoxicated patients with impaired consciousness. It is valuable to adopt a model that could be applied to poisoned patients with disturbed consciousness, regardless of the causative poisons, as these patients often could not provide medical history or express their complaints. MAP, PaO2, pH, and Glu/K ratio were the four parameters constituting the nomogram, which are convenient and objective.
Footnotes
Acknowledgments
The authors thank Tanta University Poison Control Centre (TUPCC) for facilitating data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon reasonable request from the corresponding author.