
Abstract
Data about etiologic and demographic characteristics of acute poisoning in adults in Qatar are lacking. This prospective observational study was undertaken to analyze characteristics and possible determinants of acute poisoning in adults in Qatar. During 2010, 18,073 patients attended the emergency department of Hamad General Hospital, a teaching hospital in Qatar. Out of them, 599 (3.3%) patients were diagnosed as “poisoning case” with either chemical or pharmaceutical substances. The prevalence rate of poisoning incidence was 35.3/100,000 population. Seven patients died, corresponding with a case-fatality rate of 0.39/1000. The majority were male (65%) and the mean age was 34 years. The poisons involved were mainly chemicals (61.6%) and pharmaceuticals (38.4%). Female, mainly single, suffered more intentional poisoning compared to male. Of the patients aged 60 years and above (7.2%), the majority (95.3%) suffered unintentional poisoning with pharmaceuticals; 56% with warfarin, 12% with digoxin and 7% with insulin. Multivariate analysis shows that female gender, single status, younger than 35 years of age, being poisoned by pharmaceutical products, and the need for hospitalization are significant determinants for acute intentional poisoning after adjusting all other possible covariates. The findings of this study can be used to establish awareness and prophylactic campaigns in Qatar.
Introduction
Poisoning is a substantial global public health concern. According to data from the World Health Organization (WHO), an estimated 346,000 people died worldwide in 2004 due to unintentional poisoning. Out of those, 91% occurred in low- and middle-income countries. 1 Moreover, acute poisoning is one of the most common causes of admission to emergency rooms in many countries. 2
The extent of this problem, the situation of exposure and the types of poison involved vary from one country to another. This variation depends on the level of industrialization and urbanization, the type of agricultural activities and the availability of medical facilities in each particular country. 3 In addition, these differences may be attributed to the socioeconomic and cultural factors among diverse ethnic groups who immigrate to different countries. 4
The increased tendency to use synthetic chemicals, therapeutic and over-the-counter (OTC) drugs is the major etiological factor for both unintentional and suicidal acute poisoning and has resulted in a significant rise in the number of patients admitted to the hospital because of overdose. 5
Reports from several Middle Eastern countries (Saudi Arabia, 6 Bahrain, 7 Oman, 3,8 Iran, 9 Palestine 10 and Turkey 2,11 ) show that acute poisoning in adolescents and adults is an important clinical emergency and contributor to morbidity and mortality in this part of the world.
More than two decades ago, Dawod et al. reported about the unintentional poisoning of children in Qatar. 12 However, acute poisoning in adults has not been extensively studied yet.
Therefore, this study was undertaken to analyze the characteristics and find possible determinants of acute poisoning in adults admitted to the Accident and Emergency Department (ED) in a teaching hospital in Qatar. This would allow establishing a baseline epidemiological database for poisoning hazards as well as identifying high-risk patients and organizing preventive campaigns.
Methods
This prospective observational study evaluates adolescents (14 years and older) and adults with the diagnosis of acute poisoning (drug overdose or chemical poisoning) admitted to the ED in Hamad General Hospital (HGH) from January 1, 2010 to December 31, 2010. HGH is a tertiary care teaching hospital with a capacity of 600 beds and is a member of Hamad Medical Corporation (HMC), the premier nonprofit health care provider in the State of Qatar.
The State of Qatar is located at the western coast of the Arabian Gulf on a 160-km-long peninsula with a total area of 11,493 km2. In April 2010, the Qatar Statistics Authority estimated the total population to be 1,699,435 individuals of which 75.6% were males and 24.4% females and 47% of the total population were living in the capital Doha. 13
Data collected included patient’s age, gender, ethnicity, marital status, admission date and time, location, poison’s nature and quantity (if applicable), route of administration, clinical assessment about the intentional or self-poisoning ideation, management and possible therapeutic interventions, length of stay (in ED, hospital ward and intensive care unit; ICU) and possible morbidity and mortality due to the intoxication. Patients with adverse drug reactions, food poisoning or poisoned by venomous animals were excluded from this study.
Poisoning agents were categorized as either chemicals or pharmaceuticals. Chemicals include household products, pesticides, alcohols, hydrocarbons and gases. Pharmaceuticals include OTC items and therapeutic (prescribed) medications. Exposure to a poisoning substance was classified as intentional or unintentional. Intentional poisoning includes any deliberate self-harm or suicide attempt by taking any substance that is known to be toxic in nature or a large amount of medication that exceeds the normal therapeutic dose. Clinical assessment and history taking, in addition to medical notes, were deployed to reassess the patients’ intention. The length of stay was classified as “normal” (2 days or less) and “prolonged” (3 days or more).
The study was approved by the institution’s medical research committee (Protocol # 10016/10).
Statistical analysis
Data were analyzed using the statistical package for the social sciences version 18.0. Descriptive statistics such as mean, SD and range for interval data, frequency and percentage of categorical variables were used to summarize baseline demographic and clinical data. Mean differences between two independent groups were assessed using unpaired t test. Association between two or more categorical variables was assessed using appropriate (χ 2) test. For small cell frequency (expected cell frequency less than 5), the (χ 2) test with continuity correction factor or Fisher’s exact test was used. Normality test was examined through the Shapiro–Wilk test. For non-normal data, differences between two independent groups were tested using the Mann–Whitney U test. A p value equal or less than 0.05 (two-tailed) was considered as statistically significant.
Prevalence rate was used as the morbidity frequency measure by comparing the number of intoxicated patients with the total number of population and is expressed as the number of cases per 100,000 people. Fatality rate was used as mortality frequency measure and it is the proportional result of known cases that died over the total admissions due to intoxication.
Univariate and multivariate binary logistic regression analyses were used to determine the relationship strength between the dependent variable (intentional intoxication) and several possible independent variables and covariates. The independent variables considered in the logistic regression analyses are gender, marital status, age, toxic substance, the need for ward admission, prolonged hospital stay and the need for ICU admission. Following the results of univariate logistic regression analysis, a p value equal or less than 0.1 was considered clinically significant for the predictor to be included in the multivariate logistic regression analysis. Results for each predictor variable in the univariate and multivariate logistic regression analyses are expressed as unadjusted and adjusted odds ratio (OR) along with their corresponding 95% confidence interval (CI).
Results
A total of 18,073 patients received medical care from the ED at HGH during 2010. Out of them, 599 (3.3%) adult patients were diagnosed as acute poisoning with either chemical or pharmaceutical substances. A total of 93 patients (15.5%) required admission, out of which 35 (5.8%) were admitted to ICU. The remaining506 patients (84.5%) were treated and discharged from the emergency. The admission rate due to poisoning (prevalence rate) was 35.3/100,000 population. The total fatal poisoning was seven cases, which accounts for a case-fatality rate of 0.39/1000 admissions.
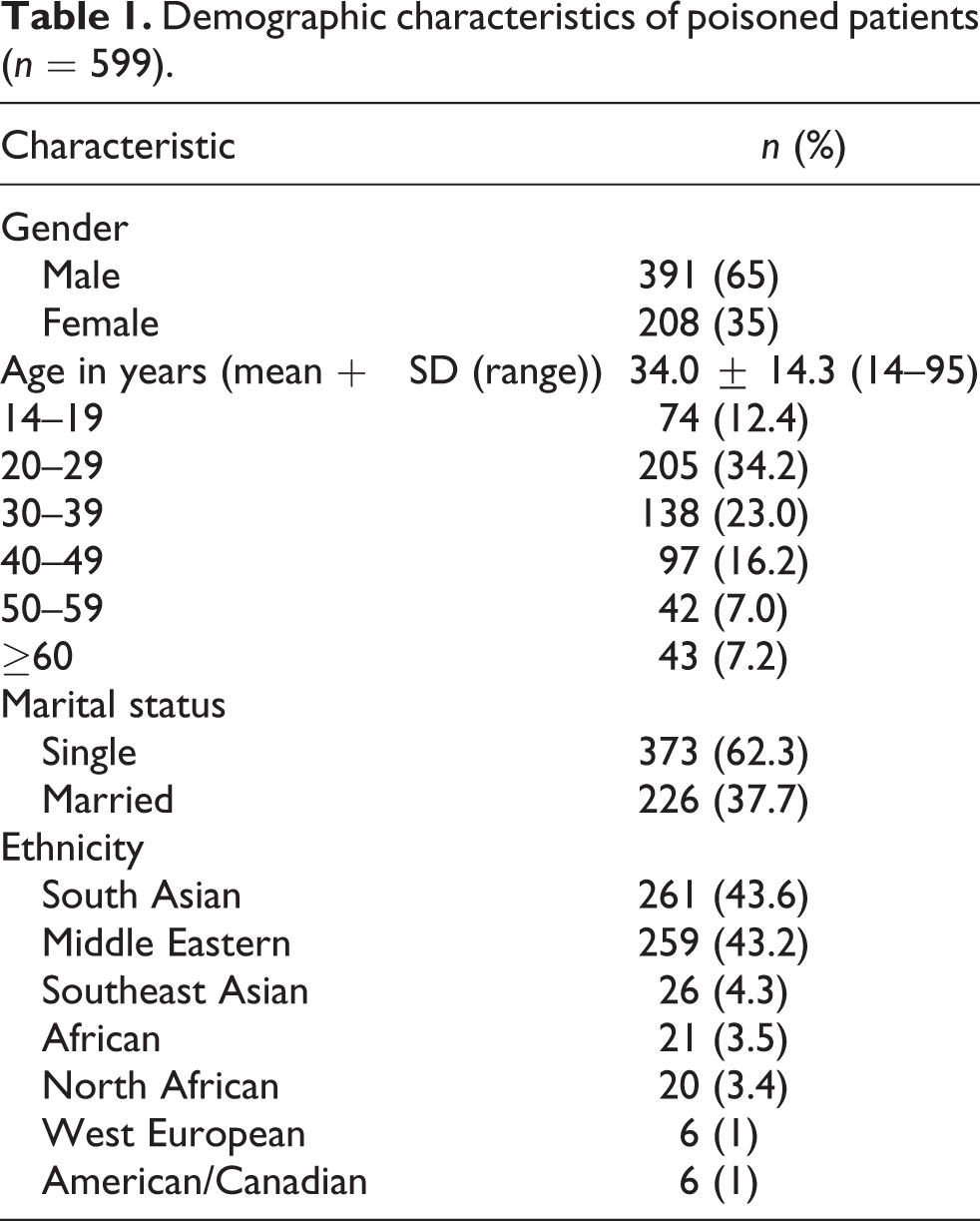
Demographic details and characteristics of the population study are summarized in Table 1. Male patients were the majority (65%) with the male to female ratio being 1.9:1. The mean age was 34 years (±14.3, range 14–95 years) and most patients were single (62.3%). Patients were mostly from South Asia and the Middle East. The age distribution in relation to intentional and unintentional poisoning is shown in Figure 1. Intentional poisoning tends to decrease as the age increases. Most cases of intentional poisoning occur in patients between 14 and 19 years of age, while most cases of unintentional poisoning occur between the age of 25 and 29 years.

Age distribution of patients presenting with intentional and unintentional poisoning (n = 599).
Demographic characteristics of poisoned patients (n = 599).
Details about poisonous substance and its burden are presented in Table 2. The poisonous substances used were mainly chemicals (61.6%). Total patient days in hospital due to intoxication incidence were 1375 days. Most of the cases (81.1%) were managed by close medical observation and supportive treatment. Patients that reported to the ED within 2 h of orally ingested poisons were primarily treated by gastric lavage followed by activated charcoal. Specific antidotes were given according to the intoxication type, such as N-acetylcysteine for paracetamol, vitamin K for warfarin, dextrose for hypoglycemic agents and flumazenil for benzodiazepines. About 59.3% of the patients were admitted during summer and autumn. The main location of poisoning exposure was in residential areas (52.3%).
Characteristics of the poisons and its burden (n = 599).

The route of exposure and substances involved in chemical poisoning are summarized in Table 3. Patients intoxicated with chemicals were most frequently affected by alcohols (64.2%) followed by “disinfectant and detergents” (15.2%), mainly sodium hypochlorite “Chlorox®” (80.4%) and hydrocarbons (7%). Blood level detection of these chemicals was feasible in 67.2% of the patients.
Details about patients with acute chemical poisoning (n = 369).
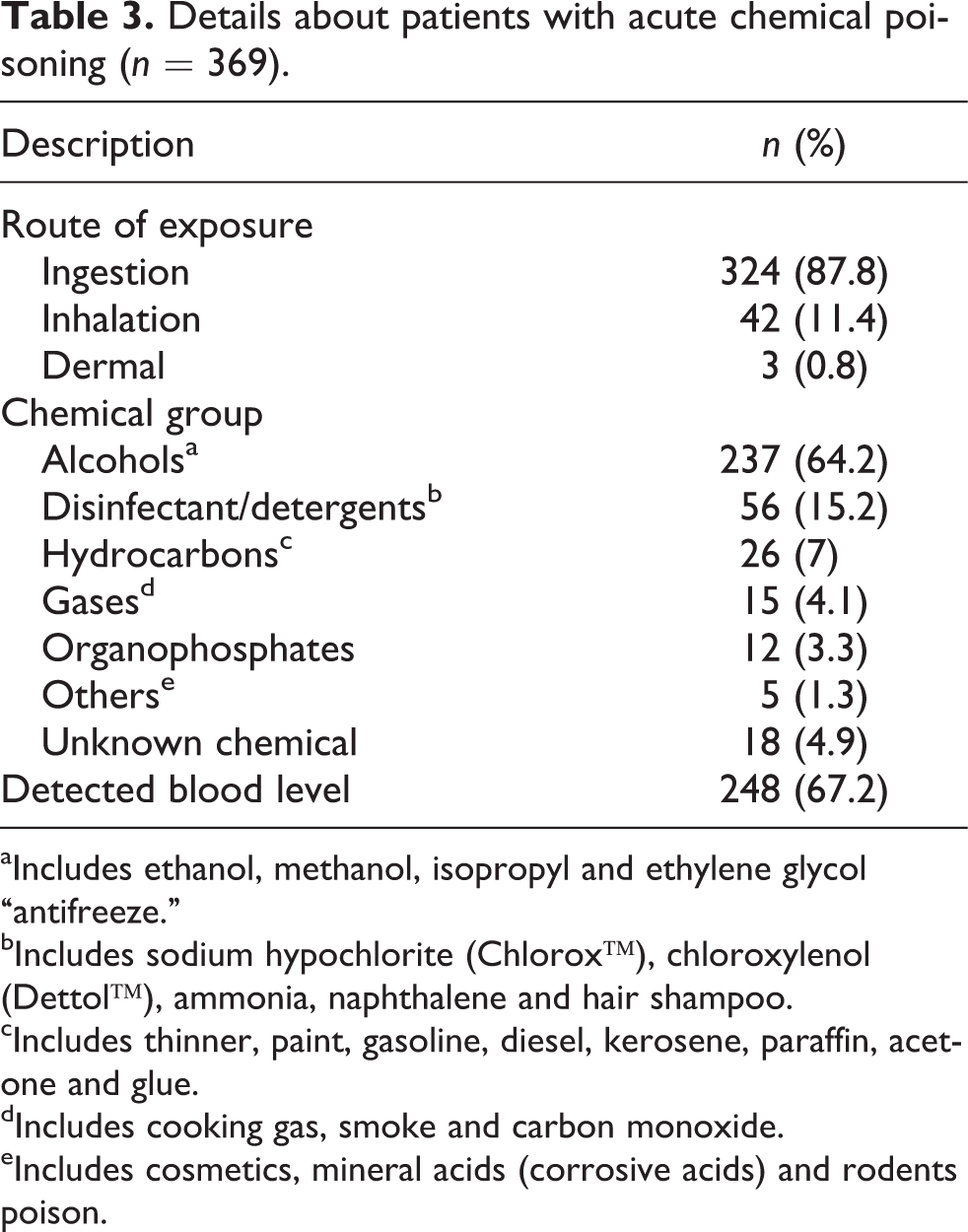
aIncludes ethanol, methanol, isopropyl and ethylene glycol “antifreeze.”
bIncludes sodium hypochlorite (Chlorox™), chloroxylenol (Dettol™), ammonia, naphthalene and hair shampoo.
cIncludes thinner, paint, gasoline, diesel, kerosene, paraffin, acetone and glue.
dIncludes cooking gas, smoke and carbon monoxide.
eIncludes cosmetics, mineral acids (corrosive acids) and rodents poison.
Details about the patients with acute pharmaceutical intoxication are summarized in Table 4. Most poisoning cases with these agents resulted from oral intake (97%), of which 50.4% involved OTC items while 42.6% were prescribed medications. The major pharmaceutical group involved was analgesics (46.1%), mainly paracetamol (87.7%) followed by anticoagulants (12.6%) and antiepileptics (8.7%). Around 70% of the pharmaceutical poisoning cases were confirmed by blood levels. A total of 70 patients (11.7%) were poisoned with high-alert medications, as defined by the Institution for Safe Medication Practice. 14
Details about patients with acute pharmaceutical poisoning (n = 230).

aHigh-alert medications.
bIncludes anticholinergic, antihistamines, muscle relaxants, selective serotonin reuptake inhibitors, antihypertensives, methylxanthines, hormones and cough remedies.
In Table 5, a comparison between patient’s characteristics and the type of exposure (chemical versus pharmaceutical) is provided. The majority of male patients were poisoned with chemicals while most of the female patients suffered poisoning with pharmaceuticals (p < 0.001). The average age was similar in both groups. Intentional poisoning was observed more frequently with pharmaceuticals than with chemicals (p < 0.001). Patients with pharmaceutical poisoning needed more medical care and admission for at least 2 days (24.8%) compared with the patients who suffered chemical poisoning (9.8%; p < 0.001). Seven patients (1.17%) died as a consequence of the intoxication: four cases because of chemical exposure (two cases by alcohols, one case by disinfectant and one case by gas) and three cases because of pharmaceutical exposure (two cases by warfarin and one case by paracetamol).
Comparison between patient’s characteristics for patients exposed to chemical and pharmaceutical poisoning.

ED = Accident and Emergency Department; ICU = intensive care unit; SD = standard deviation.
The comparison between patient’s characteristics related to intentional and unintentional acute poisoning is given in Table 6. Female patients suffered more intentional poisoning compared to male (p < 0.001), while older patients (60 years and older) suffered more from unintentional poisoning than younger patients (p < 0.001). The majority of intentional poisoning occurred in the patient’s residence (p < 0.001) with 26.8% of them requiring hospitalization compared to 11.5% in the case of unintentional poisoning (p < 0.001). Intentional poisoning required prolonged hospital stay (more than 2 days), which is significantly more than unintentional poisoning (p < 0.001).
Comparison between patient’s characteristics regarding intentional and unintentional poisoning.

ED = Accident and Emergency Department; ICU = intensive care unit; SD = standard deviation.
A subanalysis of 43 elderly patients (60 years and older) is presented in Table 7. The mean age was 68.4 years and almost all (95.3%) suffered unintentional poisoning mainly with pharmaceutical substances (83.7%): warfarin (55.8%) followed by digoxin (11.6%) and insulin (7%). Two patients died because of accidental warfarin intake.
Characteristics of patients of 60 years and older with acute poisoning (n = 43).
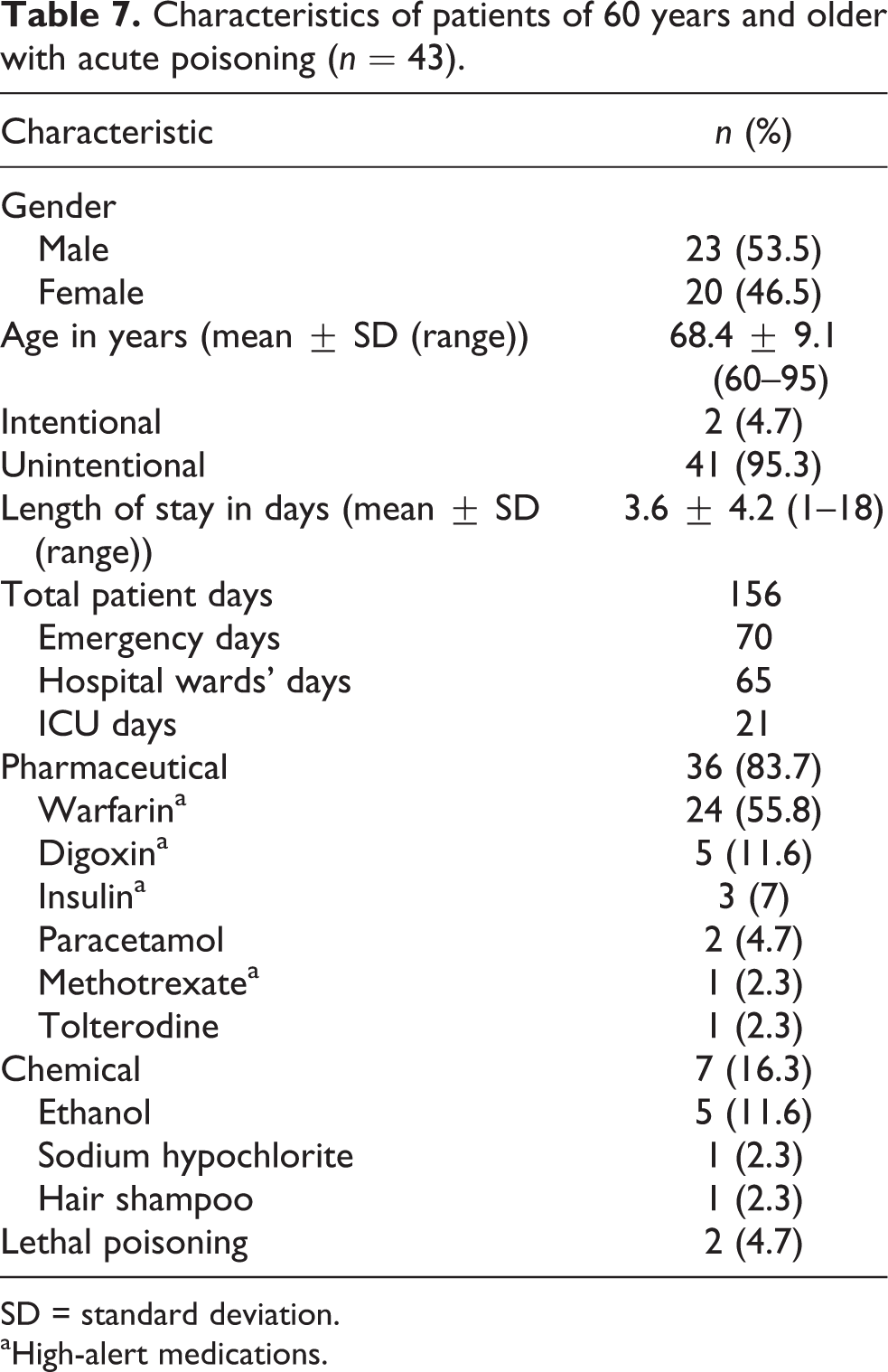
SD = standard deviation. aHigh-alert medications.
Univariate binary logistic regression results (presented in Table 8) showed that age, gender, marital status, substance, hospital admission and prolonged hospital stay were significantly associated with and had significant impact on acute intentional poisoning.
Univariate logistic regression analysis (n = 599).a
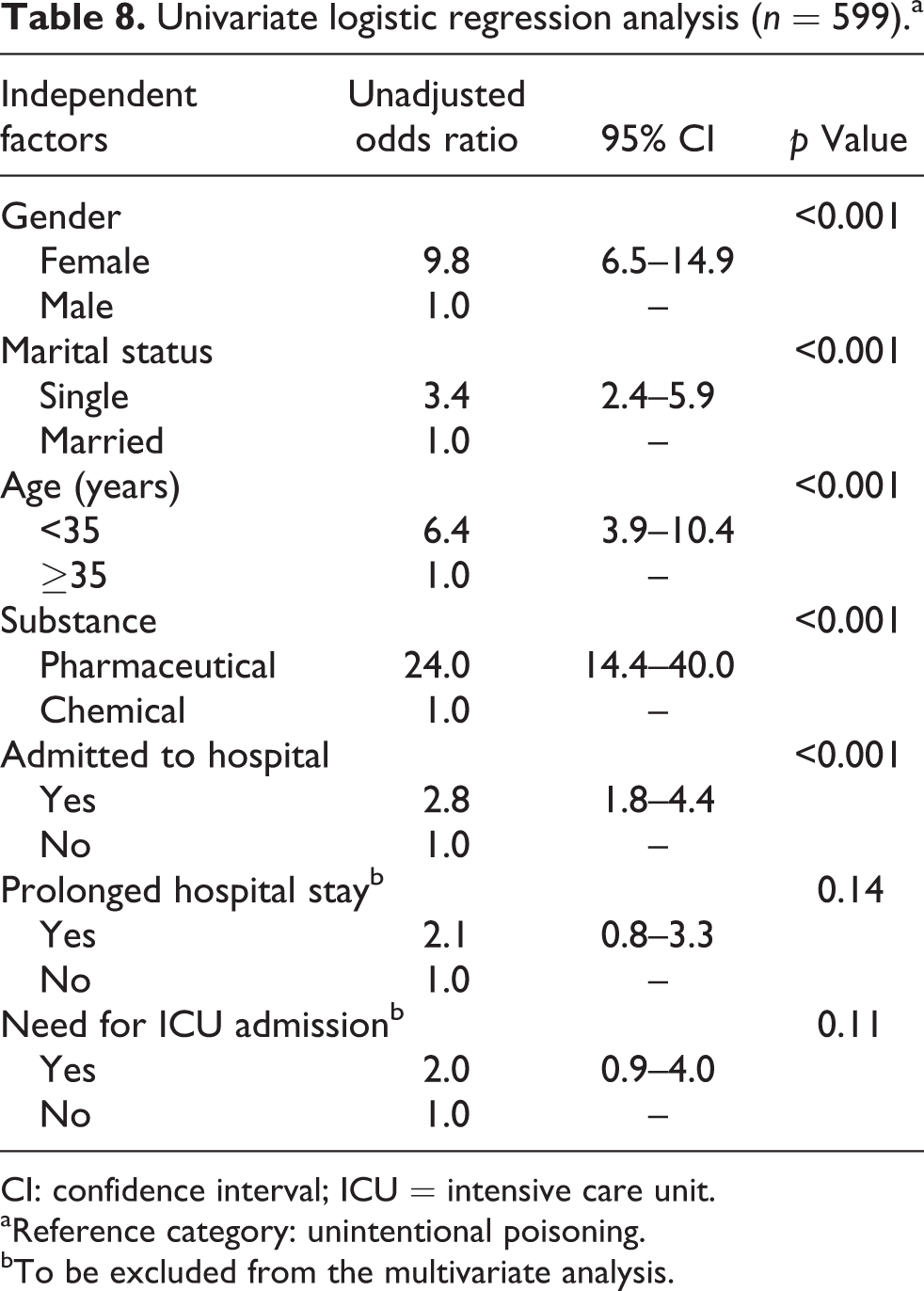
CI: confidence interval; ICU = intensive care unit.
aReference category: unintentional poisoning.
bTo be excluded from the multivariate analysis.
Females were significantly more likely to have intentional poisoning compared with males (unadjusted OR = 9.8, 95% CI = 6.5–14.9). Also, singles were significantly more likely to have intentional poisoning compared with the married people (unadjusted OR = 3.4, 95% CI = 2.4–5.9). Odds of acute intentional poisoning were 6.4 times higher among the patients younger than 35 years (unadjusted OR = 6.4, 95% CI = 3.9–10.4). Odds of acute intentional poisoning were 24 times higher among the patients who ingested pharmaceutical substances compared with the patients who ingested chemical substances (unadjusted OR = 24.0, 95% CI = 14.4–40.0). Patients admitted to the hospital (medical or ICU) were significantly more likely to have intentional poisoning as compared with the patients not requiring admission (unadjusted OR = 2.8, 95% CI = 1.8–4.4). The insignificant results with two predictors, prolonged hospital stay and the need for ICU admission, under the univariate analysis were excluded from the multivariate analysis.
Multivariate analysis (Table 9) shows that female gender (adjusted OR = 3.0, p < 0.001), single (adjusted OR = 4.0, p = 0.005), younger than 35 years of age (adjusted OR = 3.5, p = 0.010), being poisoned by pharmaceutical products (adjusted OR = 18.8, p < 0.001) and the need for hospitalization (adjusted OR = 3.7, p < 0.001) are significant determinants for acute intentional poisoning after adjusting for all other possible covariates.
Multivariate logistic regression analysis of significant predictors for acute intentional poisoning among the studied patients (n = 599).

CI: confidence interval.
Discussion
This study deals with a very important medical and community risk issue in Qatar. It allows defining the etiological and demographical characteristics of acute adult poisoning-related ED visits and related complications.
Our rate of admission for poisoning (prevalence rate) was 35.3/100,000 population. This is substantially lower than the neighboring country Bahrain (105/100,000 population 7 ) and similar to Malaysia (31.79/100,000 population 15 ). The poisoning admission rate in our institution was 3.3%, which is higher compared with the reports from other centers and countries (Istanbul 2.4% 2 and Adana 1.6% 11 (both in Turkey), Oman 0.18%, 8 Malaysia 0.43% 15 and Palestine 1.5% 10 ). This proves a heavy burden of acute poisoning in our setting.
The case-fatality rate however was 0.39/1000 admissions (corresponding with 1.2%), which is higher compared to the findings of one study (Istanbul (Turkey) 0.7% 2 ) and lower compared to the findings of other studies (Tehran (Iran) 1.3%, 9 Malaysia 3.6%, 15 Pakistan 2.5%, 16 India 4%, 17 and Taiwan (elderly patients) 9.6% 18 ). Our low-fatality rate may be explained by the fact that most commonly ingested agents were mostly nonlethal drugs and the prompt access to medical support. The high mortality observed in other studies was attributed to a delay in admission to the hospital, improper management of the poisoned patient, lack of information regarding the poison agent and its antidote. 19
Most cases of intentional poisoning occur in youngsters between 14 and 19 years. We noticed that intentional poisoning tends to decrease as the age increases, which is in parallel with other studies. 2,9,19 Probing the problem of intentional intoxication could be an effective measure for prevention. Al-Ansari et al. reported that 13% of young poison victims had visited mental health facilities in the preceding week of the poisoning incidence and 18% in the previous month. 7 Therefore, an important prevention step, especially for patients with mental problems, depression and even for any unsuccessful or potential suicide person, is to recommend psychiatric care and provide the necessary support. 9
The majority of alcohol intoxication (55.3%) was mainly seen in South Asian labors. This is mainly a homemade drink to which alcohols such as cheap perfumes and antiseptic alcohols are added. Alcohol intoxication was found to be common in these countries. 18,19 This suggests that habits and norms of different ethnic variations are transferable and can affect the host country. Ethnic variation was also found to affect the choice of suicide and self-harm from toxic substances. These differences may be attributed to the socioeconomic and cultural factors among the ethnic groups. 4
Our study found that poisoning due to household cleaning agents, especially sodium hypochlorite, posed a significant cause for admission to the hospital. This finding is similar to the findings from studies in Turkey. 2,11
While in our study, chemical and pharmaceuticals were equally contributing to mortality, other studies revealed that chemical poisoning exposures were associated with increased mortality. 4 These cases do not include intoxicated patients that died before their arrival to the hospital, which could explain the equality. The mortality depends also on the type of agent, route and duration of exposure, and the access to proper management. On the other hand, drug overdoses were associated with increased morbidity including intensive care treatment and longer hospital stay. 4
Analgesics are listed third among the top 25 substances most frequently involved in poisoning of adults above 19 years of age in the United States. 20 In Qatar, similar to the United States, paracetamol-containing products can be purchased from any kind of store without restriction on the number of tablets. This very likely explains why this drug is found to be the commonest pharmaceutical agent ingested in the cases of intentional self-harm.
Poisoning with benzodiazepines was low in our setting. This might be attributed to the restricted availability (hospital only) and the fact that this group of drugs is governed by the local regulations under the psychotropic substance act (i.e. similar to narcotic drugs). In other countries, however, benzodiazepine was found to be one of the most frequently used substances involved in poisoning with pharmaceuticals. 2,9,16 – 18
Several factors can contribute to the wide difference in poisoning pattern such as climate (for carbon monoxide poisoning), cultural (traditional remedies versus medical advice and products) 8 and ethnic variations. 4 In addition, a different prescribing practice between physicians, the type of medications involved and their availability can vary from one country to another. 8 In Qatar, health care is highly subsidized in all governmental hospitals. Medication is free for nationals and at a much reduced cost for residents. This leads to accumulation of medications and might increase the risk of drug poisoning. This issue should be addressed in future prevention programs.
Seasonal differences were observed in the number of poisoned patients consulting our ED with most victims being seen in summer and autumn. This seasonal variation was also seen in studies from Turkey and India. 11,18 Patients with psychotic disorders, depression and anxiety seem to opt for drug overdosages during summer. 11
In elderly, medications were responsible for the majority of unintentional poisoning. This finding was similar to other studies. 18,21,22 Patients aged 65 years or older were at higher risk of developing toxicity from warfarin, digoxin and insulin according to a national surveillance from the United States. 21 These three medications caused nearly one-third of adverse drug events treated in the ED and up to 41.5% of estimated hospitalizations. 21 Another study from Pakistan showed that digoxin, warfarin and immunosuppressants were mostly involved in unintentional overdose. 16 These findings are in line with our findings. Elderly patients receiving warfarin therapy should be given special attention by the health care providers. Their understanding about warfarin and how to respond upon missing a dose or bleeding incidence is difficult to assess. 23 Moreover, elderly patients are likely to be prescribed a higher number of drugs. Furthermore, the narrow therapeutic window of these medications combined with the possible accumulation linked to chronic intake increases the risk of unintentional toxicity. This in addition to age-related physiological changes might increase unintentional overdosages. Physicians can decrease the chance of drug overdose by simplifying the prescription and by avoiding long-term prescription especially for the elderly. 18 Any future prevention effort should certainly focus on this vulnerable population. 21,22
In conclusion, multivariate regression analysis revealed that female gender is a significant determinant for acute intentional poisoning unlike other study. 6 Other determinants such as marital status (single), younger than 35 years of age, being poisoned by pharmaceutical products and the need for hospitalization are also associated with acute intentional poisoning. These results are useful to highlight intentional poisoning in our setting and to define the risk groups for future preventive measures.
We recommend raising public awareness by setting up campaigns about the potential toxic materials in the region, hazardous household products and medications. This approach has a proven record in reducing acute poisoning. 6,10,19 In addition, providing training programs to health care workers about the most likely poisons involved, the populations at risk and the overall management are likely to improve the outcome. Finally, proper data collection in all health care centers throughout the country will be an important key to get a complete insight into the poisoning pattern in the State of Qatar.
Limitations
This study was done at the ED of a tertiary, teaching hospital. Therefore, it will not provide the overall poisoning pattern of the country. Very severe cases that might have died before reaching the hospital have not been included neither the probably less severe cases seeking help at primary and secondary health care centers.
Despite these limitations, these data provide very important information about the characteristics and determinants of poisoning in adolescents and adults in the State of Qatar. Further prospective, comprehensive and multicenter-based studies in all age groups are necessary to provide a more complete picture.
Footnotes
Acknowledgment
The authors would like to thank Dr Prem Chandra, Clinical Scientist in Biostatistics, Medical Research Centre in Hamad Medical Corporation for his assistance and review of statistics used in this study. The authors would also like to express their sincerest thanks to all physicians, pharmacists and nurses in the Accident and Emergency Department as well as all other health care providers of Hamad General Hospital for their outstanding commitment toward patient care and for their valuable help in facilitating this study.
Conflicts of interest
The authors declared no conflicts of interest.
Funding
This work was supported by the Medical Research Center of Hamad Medical Corporation (grant number 10016/10).