
Abstract
Background
Accurate assessment of disturbed consciousness level (DCL) is crucial for predicting acutely poisoned patients’ outcomes.
Aim
Development of a novel Poisoning Agitation-Sedation Score (PASS) to predict the need for endotracheal intubation (ETI) and mechanical ventilation (MV) in acutely poisoned patients with DCL. Validation of the proposed score on a new set of acutely poisoned patients with DCL.
Methods
This study was conducted on 187 acutely poisoned patients with DCL admitted to hospital from June 2020 to November 2021 (Derivation cohort). Patients' demographics, toxicological data, neurological examination, calculation of the Glasgow Coma Scale (GCS), Full Outline of Unresponsiveness (FOUR) score, Richmond Agitation–Sedation Scale (RASS), and outcomes were gathered for developing a new score. The proposed score was externally validated on 100 acutely poisoned patients with DCL (Validation cohort).
Results
The PASS assessing sedation consists of FOUR (reflexes and respiration) and GCS (motor) and provides a significantly excellent predictive power (AUC = 0.975) at a cutoff ≤9 with 100% sensitivity and 92.11% specificity for predicting the need for ETI and MV in sedated patients. Additionally, adding RASS (agitation) to the previous model exhibits significantly good predictive power (AUC = 0.893), 90.32% sensitivity, and 73.68% specificity at a cutoff ≤14 for predicting the need for ETI and MV in disturbed consciousness patients with agitation.
Conclusion
The proposed PASS could be an excellent, valid and feasible tool to predict the need for ETI and MV in acutely poisoned disturbed consciousness patients with or without agitation.
Introduction
Disturbed consciousness is a common major complaint in the emergency department. Many pathological etiologies of altered consciousness include sepsis, epilepsy, stroke, post-anoxic coma, organ failure, and metabolic disturbances. 1 Additionally, toxins can also cause altered consciousness, either directly through their action on the central nervous system or indirectly through inducing metabolic abnormalities (e.g., hypoglycemia or hyperammonemia caused by drug overdose). 2
Impaired consciousness has many nonspecific terms that are often misused, leading to miscommunications. It may range from drowsiness, somnolence, confusion, delirium, lethargy, obtundation, and stupor to deep coma. 3 Accordingly, scales have been designed to avoid subjective evaluations by quantitative consciousness assessment. 4 Furthermore, scoring systems facilitate communication among examiners for monitoring consciousness changes, rapid therapeutic decisions, and outcomes prediction. 5
Glasgow Coma Scale (GCS) has provided a practical tool for bedside assessment of consciousness level using the three components: verbal, motor, and eye response. 6 Yet, it has some limitations in evaluating the verbal response in aphasic, intubated patients and inconsistency of inter-observer reliability.7,8
Full Outline of Unresponsiveness (FOUR) score was developed to overcome the GCS confines with an accurate, comprehensive assessment of the patient’s neurological condition. 9 Additionally, it evaluates respiratory patterns and brainstem reflexes that GCS does not assess. 10 However, the FOUR score is more complicated, and its application remains quite difficult.. 11 Additionally, it can not be used to assess disturbed consciousness patients with agitations.
The Richmond Agitation-Sedation Scale (RASS) is a simple tool that assesses agitation and sedation. 12 It can evaluate agitation status in patients whose consciousness level assessment by traditional scales is relatively complex.13,14 Nevertheless, the RASS cannot evaluate consciousness in patients with visual or auditory impairments, as it relies on the presence of eye contact and vocal responses to verbal stimuli. 15
Altered consciousness patients are at high risk for mortality and various morbidities such as aspiration pneumonia, hypoxia, persistent cognitive impairment, need for mechanical ventilation (MV), intensive care unit (ICU) admission, and prolonged hospitalization period.16,17 Therefore, outcome prediction is a major concern for clinical toxicologists for early triaging of high-risk, acutely poisoned patients with disturbed consciousness, especially in developing countries with restricted hospital resources.18,19
Although various scoring systems and models are used in acutely poisoned patients with disturbed consciousness to predict the need for MV and ICU admission, their predictive accuracy is still questionable owing to their limitations and inadequate clinical validation. 20 – 23 As a result, the traditional prognostic scores are frequently inaccurate for determining prognosis in acutely poisoned patients with an unexpected course that is dependent on numerous variables.18,24
From this perspective, we aimed to develop and validate a novel Poisoning Agitation-Sedation Score (PASS) for predicting the need for endotracheal intubation (ETI) and mechanical ventilation (MV) in acutely poisoned patients with DCL.
Patients and methods
Study design and setting
This prospective cohort study was initially carried out on 187 acutely poisoned patients with disturbed consciousness who were admitted to Tanta University Poison Control Center (TUPCC) from the start of June 2020 till the end of November 2021 (the derivation cohort). Additionally, the novel proposed score for conscious assessment was validated on a new set of 100 disturbed conscious patients from the start of December 2021 to the end of May 2022 (the validation cohort).
Ethical considerations
This study was conducted following the approval of the medical research ethics committee of Tanta University Faculty of Medicine (33,809/5/20). Written informed consent was taken from patients’ legal guardians. The confidentiality of patients’ records was considered by keeping them anonymous.
Sample size
The sample size of the derivation cohort was calculated using G*Power version 3.1.9.4. (https://www.gpower.hhu.de/) based on the need for ETI and MV as the primary outcome. According to
Inclusion criteria
Figure 1 shows a flowchart of the eligibility criteria of patients included in our study. All admitted acutely poisoned patients with disturbed consciousness aged over 18 years (male or female) were included. The diagnosis was based on the history of any drug overdose or toxin exposure, characteristics of toxicological symptoms and signs, and available routine & toxicological investigations. Flow chart of the eligibility criteria of the studied patients.
Exclusion criteria
• Admitted patients more than 24 h after poisoning. • Patients with previous neurological diseases that affect consciousness level. • The presence of concomitant head trauma. • Patients with chronic illnesses such as liver, kidney, and heart diseases • Referred patients with previous medical intervention. • Patients with missing data.
Data collection tool for the derivation and validation cohort
Patient characteristics
Demographic data included age and sex. Toxicological data included poison name, exposure route, and poisoning mode. On admission, vital signs and neurological examinations were recorded.
Laboratory investigations on admission
Arterial blood gases, serum electrolyte levels, random blood sugar levels, liver enzymes, urea, serum creatinine, and complete blood count were done. Toxicological tests were performed, including a silver nitrate test to confirm phosphide exposure and serum pseudocholinesterase level to identify organophosphorus exposure. Qualitative urine screening was performed to detect cannabinoids, tramadol, opiates, benzodiazepines, and barbiturates using ACON® DOATM kits (one-step Drug of Abuse rapid test). 26
Scores calculation for the derivation cohort on admission
The GCS assesses patients according to three aspects of responsiveness (eye-opening, motor, and verbal responses.). It ranges from 3 (deep coma) to 15 (fully awake person). GCS grades are mild (13-14), moderate (9-12), and severe (less than 9).27,28
The FOUR score includes four components assessing neurological function: motor response, brainstem reflexes, eye response, and respiratory patterns. Each item is given a score ranging from 0 to 4. The total score ranges from 0 to 16. The lower score values indicated a lower level of consciousness. 9
The RASS is a 10-point scale ranging from −5 to +4. It has five levels of sedation ranging from 1 (drowsy) to −5 (unarousable), four levels of agitation that range from +1 (restless) to +4 (combative), and level 0 is “calm and alert”. 29
Patient outcomes and treatment
Patients were categorized according to the need for ETI and MV into patients who needed ETI and MV and did not. All patients were treated according to the TUPCC protocol that follows the • The patients in the present study were intubated and mechanically ventilated according to the following criteria reported by ➢ Respiratory insufficiency (respiratory rate < 8 or > 30 per minute, PO2 in blood gas < 55 mmHg, PCO 2 > 55 mmHg. ➢ Non-compensated acidosis-alkalosis. ➢ Upper and lower airway obstruction. ➢ Persistent hemodynamic instability. ➢ Excessive chest secretions with a high risk of aspiration.
Statistical methods
All data were analyzed by the Statistical Package for the Social Sciences (SPSS) version 26 (IBM Corp., Armonk, NY, USA). Categorical variables were summarized as frequencies and percentages. Comparison of the categorical variables was performed by the Independent Chi-Square or Fisher’s Exact tests as appropriate. Numerical variables were checked for distribution by the Shapiro-Wilk test, skewness, and kurtosis and presented with median and interquartile range (25th–75th percentile). The difference between the two groups and the associations between the components of the scores were performed by the Mann-Whitney U test. Consequently, two multivariable stepwise logistic regression analyses were performed to develop PASS for predicting the need for ETI and MV. The first was the model that involved disturbed consciousness patients without agitation (n = 113); the entered components in the regression analysis were eye & motor components of GCS, all components of FOUR, and RASS sedation. The second was the model for predicting the need for ETI and MV in disturbed consciousness patients with agitation (n = 74) that involved eye ‘& motor components of GCS, all components of FOUR score, and RASS (agitation).
The model’s performance was evaluated by the concordance (C) index as a discrimination measurement tool. The C index measures how well the model discriminates between patients who needed and did not need ETI and MV and can be viewed as the extension of the area under the receiver operating characteristics (ROC) curve. It varies theoretically between 0.5 and 1.0, with a value of 1.0 indicating perfect discrimination. p value <.05 was considered statistically significant. These two prognostic models were externally validated in a cohort of 100 patients. The ROC curve assessed the performance of the proposed score to predict the need for ETI and MV in the validation cohort. The area under the curve (AUC) is graded as follows: 0.6–0.7 = poor, 0.7–0.8 = fair, 0.8–0.9 = good, and 0.9–1 = excellent or perfect discrimination.
Results
Patients characteristics in the derivation and validation cohort.
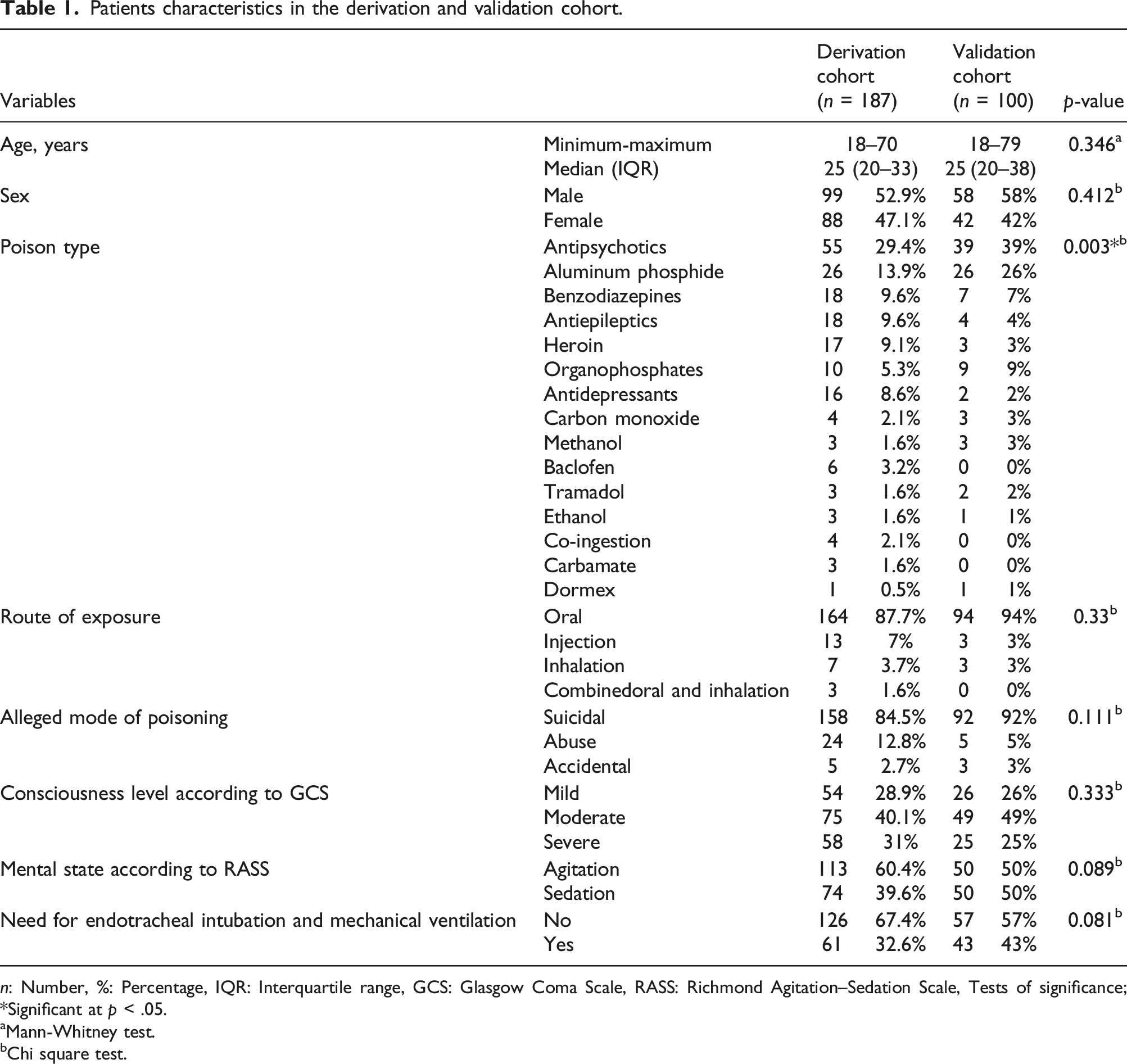
n: Number, %: Percentage, IQR: Interquartile range, GCS: Glasgow Coma Scale, RASS: Richmond Agitation–Sedation Scale, Tests of significance; *Significant at p < .05.
aMann-Whitney test.
bChi square test.
Comparison between patients in the derivation cohort who needed endotracheal intubation and mechanical ventilation and those who did not need as regards the GCS, FOUR, and RASS scores components.
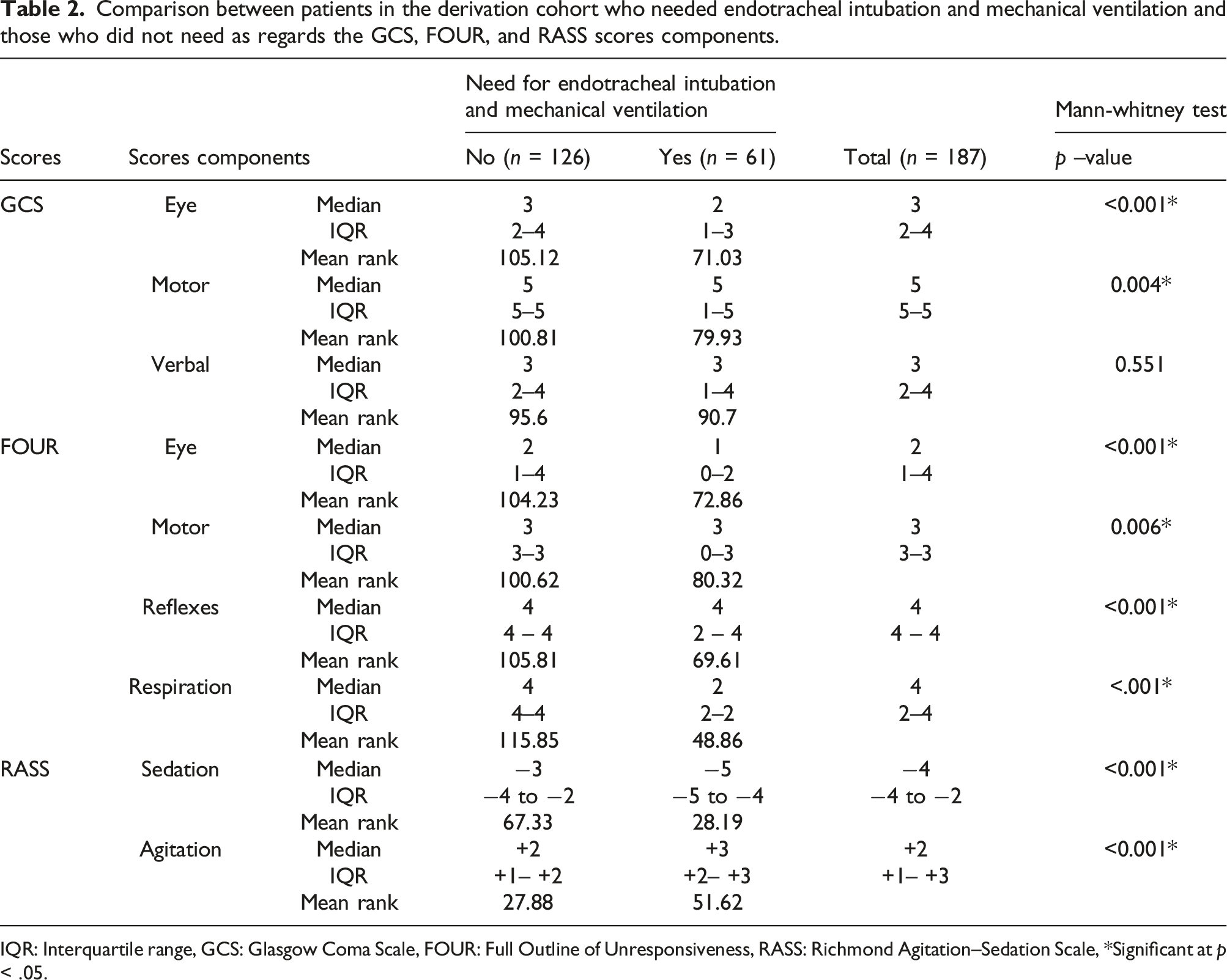
IQR: Interquartile range, GCS: Glasgow Coma Scale, FOUR: Full Outline of Unresponsiveness, RASS: Richmond Agitation–Sedation Scale, *Significant at p < .05.
Diagnostic performance of the GCS, FOUR, and RASS scores components for predicting the need for endotracheal intubation and mechanical ventilation in the derivation cohort.

%: percentage AUC: area under the curve, CI: Confidence interval, GCS: Glasgow Coma Scale, FOUR: Full Outline of Unresponsiveness, RASS: Richmond Agitation–Sedation Scale, *Significant at p < .05.
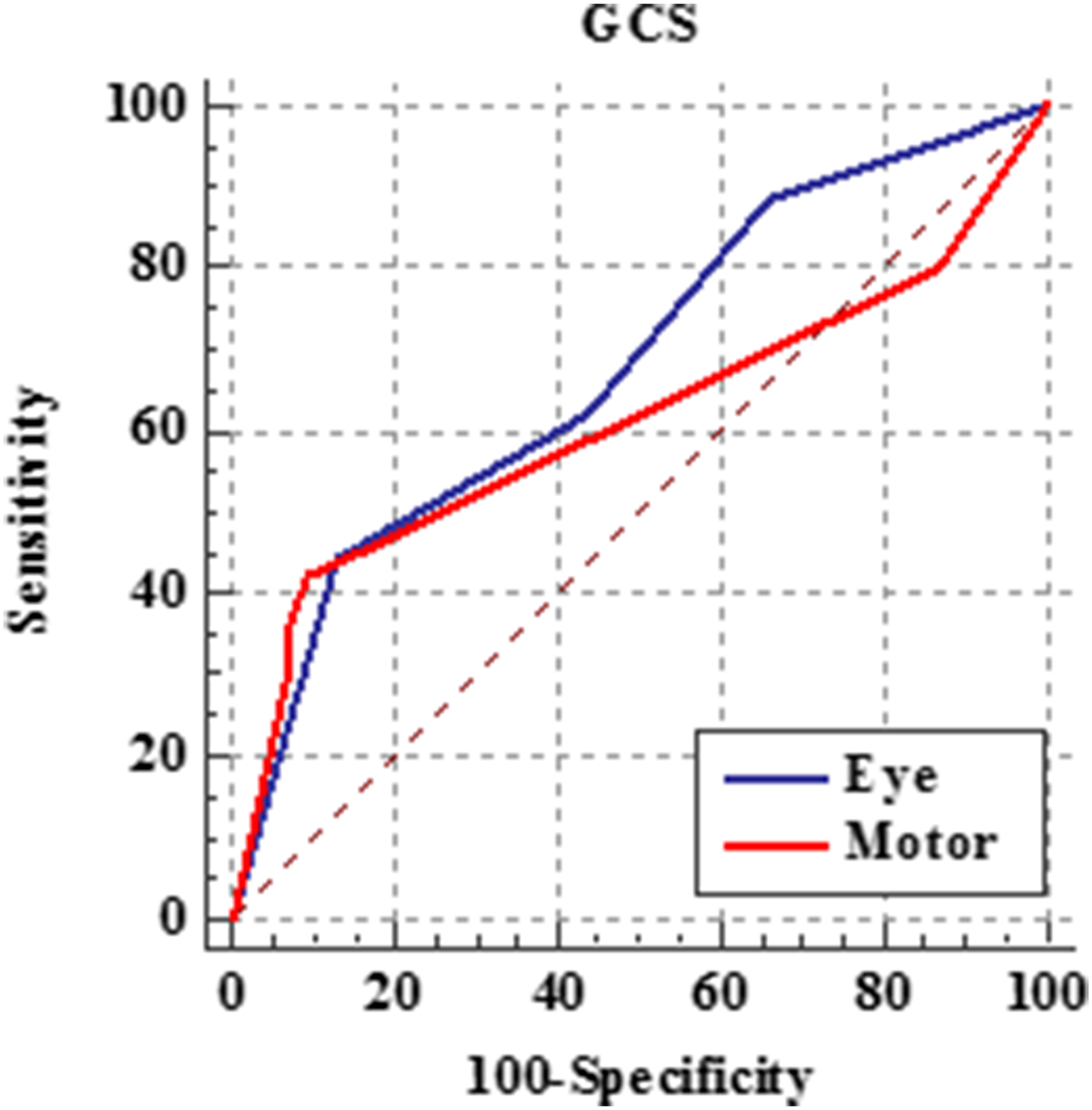
ROC curves of eye and motor component of GCS for predicting the need for endotracheal intubation and mechanical ventilation in the derivation cohort.

ROC curves of FOUR score components for predicting the need for endotracheal intubation and mechanical ventilation in the derivation cohort.

ROC curve of RASS (sedation) for predicting the need for endotracheal intubation and mechanical ventilation in the derivation cohort.
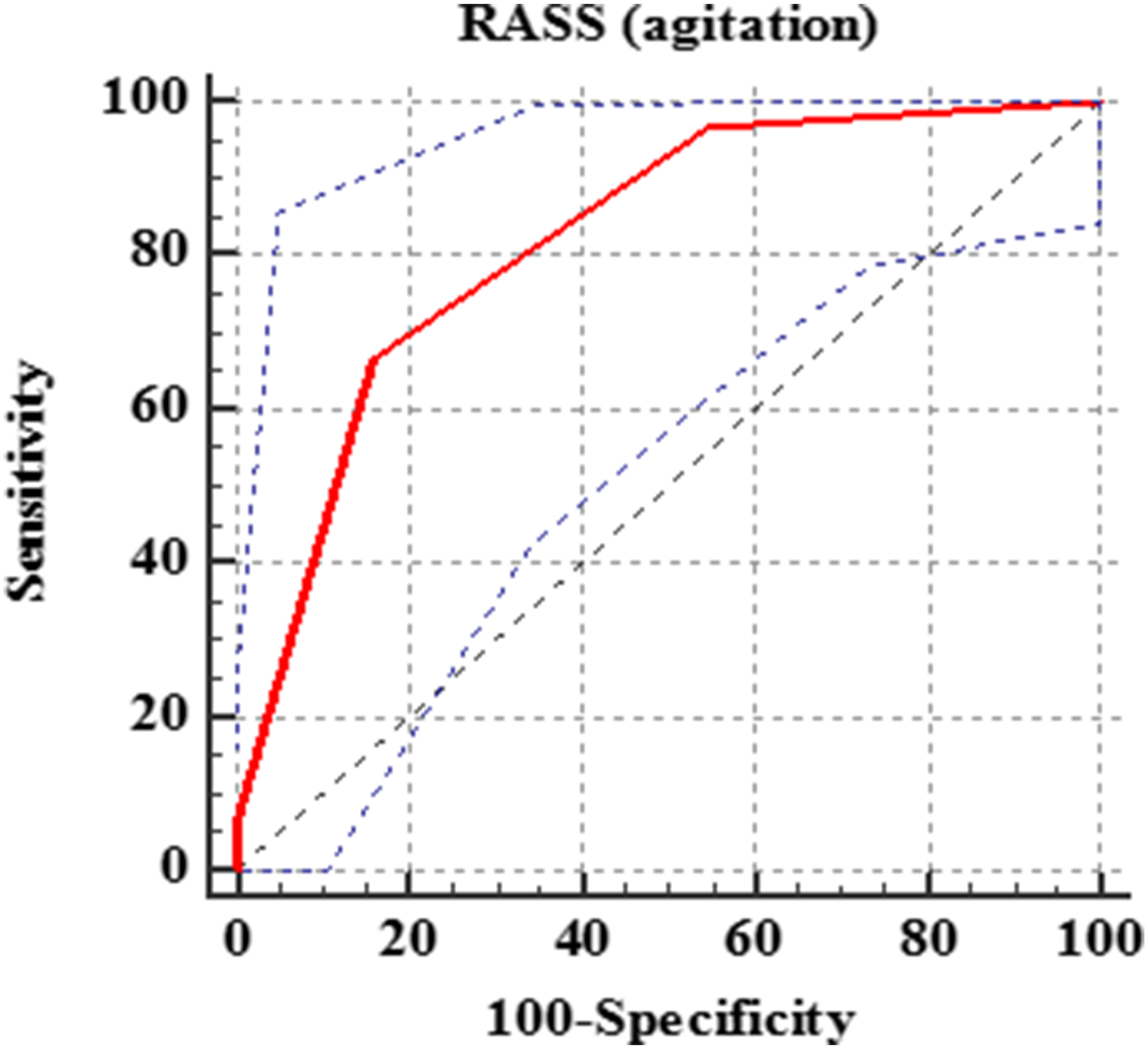
ROC curve of RASS (agitation) for predicting the need for endotracheal intubation and mechanical ventilation in the derivation cohort.
To develop a PASS for predicting the need for ETI and MV, the studied patients in the derivation cohort were categorized according to the presence or absence of agitation into two categories: patients without agitation (113) and patients with agitation (74). Consequently, significant variables were entered in multivariable stepwise logistic regression analysis.
Multivariable logistic regression analysis (stepwise) prognostic model for predicting the need for endotracheal intubation and mechanical ventilation in disturbed consciousness patients with or without agitation.

AOR: Adjusted odds ratio, %: percentage, AUC: area under the curve CI: Confidence interval, GCS: Glasgow Coma Scale, FOUR: Full Outline of Unresponsiveness, RASS: Richmond Agitation–Sedation Scale, *Significant at p < .05.
Components of the proposed Poisoning Agitation-Sedation Score (PASS) for predicting the need for endotracheal intubation and mechanical ventilation in acutely poisoned patients with disturbed consciousness with or without agitation.

Performance of GCS, FOUR, RASS, and PASS scores in predicting the need for endotracheal intubation and mechanical ventilation in the validation cohort.

%: Percentage AUC: Area under the curve, CI: Confidence interval, GCS: Glasgow Coma Scale, FOUR: Full Outline of Unresponsiveness, RASS: Richmond Agitation–Sedation Scale, PASS: Poisoning Agitation-Sedation Score, ROC: receiver operating characteristics, *Significant at p < .05.

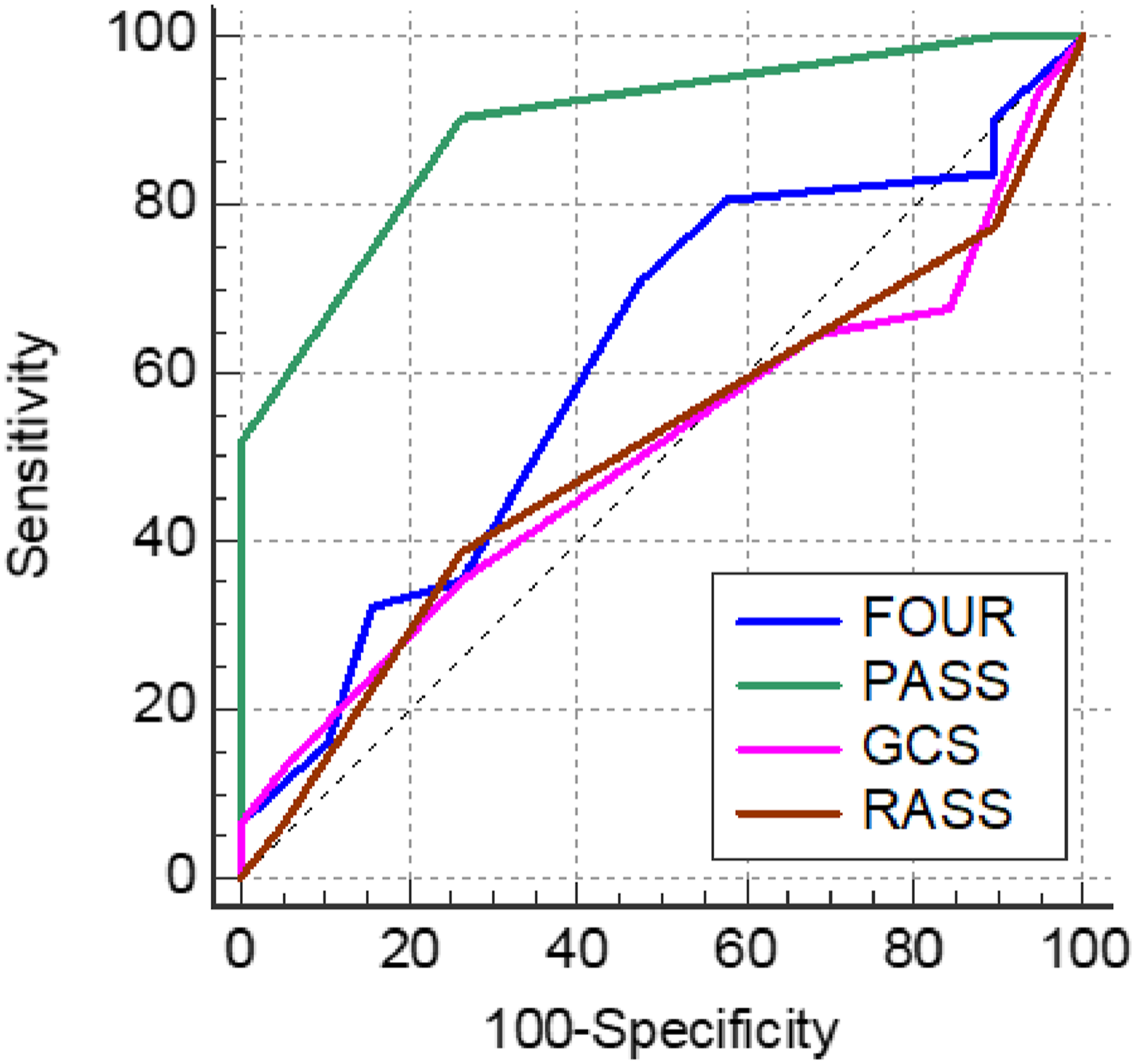
ROC curves of GCS, FOUR, RASS, and PASS (sedation) for predicting the need for endotracheal intubation and mechanical ventilation in the validation cohort.
ROC curves of GCS, FOUR, RASS, and PASS (agitation) for predicting the need for endotracheal intubation and mechanical ventilation in the validation cohort.
Discussion
The decision for ETI and MV is challenging, especially in high-risk, acutely poisoned patients with disturbed consciousness. 36 Additionally, there is an urgent need to develop a practical score accurately assessing the level of consciousness in disturbed conscious patients to improve healthcare professionals' communication and patient outcomes.
The current study revealed that the median age of the studied patients in both groups was 25 years, with male predominance (52.9% and 58%) in the derivation and validation cohorts, respectively. Similarly,
The most frequently involved poisons in both groups of the present study were antipsychotics, followed by aluminum phosphide administrated for suicidal intention. Similarly,
Regarding GCS assessment, the highest percentage of patients presented with moderate GCS (40.1% and 49%) in both the derivation and validation cohorts, respectively. However,
The current study revealed that 32.6% of patients in the derivation cohort needed ETI and MV compared to 43% of patients in the validation cohort. Near similar results
Comparison between the components of GCS, FOUR, and RASS scores regarding predicting the need for ETI and MV in the derivation cohort revealed that both eye (≤1) and motor (≤3) components of GCS were significantly valid in predicting the need for ETI and MV with poor prediction power (AUC = 0.682 and 0.612, respectively). On the contrary,
Concerning the FOUR score, the respiration component had a good prediction power (AUC = 0.858, at a cutoff of ≤2) for the likelihood of ETI and MV requirements. Alternatively, eye, motor, and reflex components were significantly valid in predicting the need for ETI and MV with poor discriminatory power (AUC = 0.668, 0.609, and 0.694, respectively).
Our patients who required ETI and MV, had a significantly lower median RASS (sedation) than those who did not need (−5 vs −3, respectively). In line with that,
Few studies compared scoring systems for predicting the need for ETI and MV in acutely poisoned patients with drug overdose, pesticides, tricyclic antidepressants (TCAs), carbon monoxide (CO), and clozapine.23–52 However, previously compared scores cannot be applied to all poisoned patients with disturbed consciousness. Additionally, they cannot assess the risk of agitated patients needing ETI and MV.
From this perspective, we proposed a novel PASS to predict the need for ETI and MV in all acutely poisoned patients with disturbed consciousness, either with or without agitation. The PASS assessing sedation consists of three variables (reflexes & respiration components of FOUR and motor component of GCS). Meanwhile, PASS assessing agitation includes adding RASS (agitation) to the previous score to predict the need for ETI and MV in acutely poisoned patients with disturbed consciousness with agitation. The accuracy proposed PASS was externally validated on a new set of 100 patients (the validation cohort). The PASS assessing sedation in disturbed consciousness patients without agitation had a significantly excellent predictive power (AUC = 0.975) at a cut off ≤9 with 100% sensitivity, 92.11% specificity, and total accuracy of 96% for predicting the need for ETI and MV. Additionally, the PASS assessing agitations in disturbed consciousness patients with the agitation was significantly valid in predicting the need for ETI and MV with good prediction power (AUC = 0.893), 90.32% sensitivity, and 73.68% specificity at a cutoff of ≤14. 53 – 55
The PASS score has advantages over the conventional scores, making it more suitable for predicting the need for ETI and MV as it assesses the breathing pattern, which is essential for predicting the need for assisted ventilation in disturbed-conscious patients. Additionally, the respiratory component of FOUR enables clinicians to assess the breathing patterns of apneic and irregular breathing patients. Moreover, the brain stem component provides valuable information about brain stem affection.56,57 Additionally, the motor component is the most reliable component of GCS for predicting outcomes as it has a good inter-observer agreement and can be easily assessed, even in intubated, inebriated, or sedated patients, as well as, it is the most affected component in severely injured patients. 58 – 60 Furthermore, adding RASS agitation to the PASS model allows for better evaluation of disturbed consciousness patients with agitation.
Strength and limitation
The proposed PASS score has many potential implications in clinical practice due to its validity and easy applicability for rapid neurological assessment, especially in settings with limited resources. Although the PASS score was externally validated, the studied patients were relatively small as it is a single-center study, which may not represent all poisoned patients.
Conclusion and recommendations
From the existing data, the proposed PASS is a simple clinical valid score providing an excellent discrimination power for predicting the need for ETI and MV in acutely poisoned disturbed consciousness patients with or without agitation. Accordingly, applying on-admission PASS assessment in toxicological centers may improve the patient's outcomes with reasonable healthcare resource utilization.
Further studies should be implemented on a wide scale with a larger sample of patients to assess the PASS's discriminatory ability for evaluating potential outcomes. Similarly, exploring the PASS applicability in various clinical settings or populations is essential to generalize its utilization. Additionally, investigating the long-term outcomes of patients assessed with PASS is recommended to endorse its validity and relevance. Furthermore, combining PASS with other clinical or laboratory markers is suggested to enhance its objectivity and predictive accuracy.
Supplemental Material
Supplemental Material - Development and validation of a novel poisoning agitation-sedation score for predicting the need for endotracheal intubation and mechanical ventilation in acutely poisoned patients with disturbed consciousness
Supplemental Material for Development and validation of a novel poisoning agitation-sedation score for predicting the need for endotracheal intubation and mechanical ventilation in acutely poisoned patients with disturbed consciousness by Soha A. Abd Elghany, Heba I. Lashin, Ghada N. El-Sarnagawy, Merfat M. Oreby, and Eman Soliman in Human & Experimental Toxicology.
Footnotes
Acknowledgments
The authors extend their appreciation to Tanat University Poison Control Center (TUPCC) for facilitating data collection.
Author contributions
Soha A. Abd Elghany contributed to the study conception, data collection, methodology, analysis, interpretation, and manuscript writing.; Heba I. Lashin contributed to the study conception, data collection, methodology, analysis, interpretation, and manuscript writing; Ghada N. El-Sarnagawy: contributed to the study conception, data collection, methodology, analysis, interpretation, and manuscript writing; Merfat M. Oreby; contributed to the study conception, data collection, methodology, analysis, interpretation, and manuscript writing; Eman Soliman; contributed to the study conception, data collection, methodology, analysis, interpretation, and manuscript writing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon reasonable request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.