
Abstract
Background:
Few studies have examined the relationship between heavy metal and serum cholesterol levels, and no recent study has examined this relationship in the US population.
Methods and Results:
A total of 19,591 individuals aged 0–80 years were included in the National Health and Nutrition Examination Survey 2009–2012; the current study was composed of survey participants for whom some or all low-density lipoprotein cholesterol (LDL-C), serum triglyceride, high-density lipoprotein cholesterol, total cholesterol, blood lead (Pb), total blood mercury (Hg), and blood cadmium (Cd) levels had been measured. Three tertiles (T1–T3) of heavy metals were used to explore dose–response association between heavy metal exposure and serum cholesterol level. Logistic regression was used to explore the relationship between tertiles of blood heavy metal levels and serum cholesterol levels after adjusting for age, sex, and socioeconomic status. We have shown that the groups with the highest levels of Pb, Hg, and Cd had a 56%, 73%, and 41% chance, respectively, of having a high total cholesterol level. In study subjects with the highest Pb levels, there was also a 22% chance of being in the group with the highest LDL-C level. An increase in total cholesterol and LDL-C levels was observed from the first to the third tertiles of the heavy metals studied.
Conclusion:
Increasing blood Pb, Hg, and Cd levels were associated with significantly increased odds of high total cholesterol after adjusting for age, sex, and socioeconomic status.
Introduction
Heavy metals are defined as metals with a density greater than 5 g/cm3. There are approximately 40 known heavy metals, including copper, Pb, zinc, and Cd. Heavy metals have the ability to interact with various enzymes and biomolecules and alter multiple physiological processes in the human body. 1
Cardiovascular diseases (CVDs), such as heart disease and stroke, are the leading cause of death in the United States, 2 and their prevalence in the developing world is increasing. One of the significant risk factors for CVD is hypercholesterolemia, a disorder characterized by the presence of high amounts of cholesterol in the blood. The implicating factors in the pathogenesis of this disorder include high serum low-density lipoprotein (LDL), total serum cholesterol levels, and low levels of high-density lipoprotein (HDL) in the blood. 3 The aim of this article was to identify any possible association and correlation between heavy metals in the blood and high cholesterol levels. Measurable quantities of heavy metals are found in the blood, and toxicological studies have found an association between heavy metals and cardiovascular mortality. 4 This study sought to explore any significant correlation between heavy metals in the blood 5 and a rise in serum cholesterol level.
Several studies have examined the relationship between serum levels of heavy metals and atherosclerosis. In vitro studies have shown that the formation of macrophage-derived lipid-laden cells can be promoted by copper 6 because copper was found to promote the oxidation of LDL. 7 In one study, a statistically significant association was found between high serum copper concentrations and atherosclerosis. Similarly, low serum zinc levels were associated with atherosclerosis. 7 Another study reported a significant positive correlation between elevated serum iron levels and atherosclerosis and atherosclerotic complications. 7 However, few studies have directly addressed the relationship between heavy metals and serum lipid levels. 8 A higher high-density lipoprotein cholesterol (HDL-C) level was found in African Americans receiving zinc supplementation than in those not receiving supplementation. 9 Another study did not find any association between serum zinc levels and serum lipid levels in elderly men. 10 Furthermore, an inverse relationship between serum copper and HDL-C levels was reported among middle-aged Chinese men. 11 Serum copper and zinc levels were found to be high in individuals with high LDL-C levels in Iran. 12 However, young individuals are not immune to this apparent trend, as a study conducted in Finland showed a positive correlation between serum zinc levels and total cholesterol, HDL and LDL levels in a 6- to 18-year-old population. 13 In the same study, an inverse association was found between serum copper and HDL-C levels. 13 A negative association between serum copper and total cholesterol levels among elderly individuals was reported in the United States. 14 The conflicting relationship between serum copper and HDL levels in reports from China 11 and Finland 13 should be carefully reviewed, and further study is required to address this conundrum.
Various heavy metals have been identified to be the direct or indirect causes of disease states, resulting from their undesirable effects on organs. Hooper et al. studied the effect of zinc levels on HDL-C in 1980 and found a reduction in HDL with a possible atherogenic effect. 15 Studies have implicated the toxicity of these metals, such as mercury (Hg) and cadmium (Cd), in the pathophysiology of hypertension, coronary heart disease, myocardial infarction (MI), cerebrovascular accidents, carotid artery disease, and renal dysfunction. 16 In addition, studies have indicated that these heavy metals, which are generally present in the body, may contribute to disease pathogenesis through the formation of free radicals with subsequent neurological deficits. 17 Notably, lipids have been implicated in the pathogenesis of many of these disease conditions.
However, despite the possible correlation between heavy metals and hyperlipidemia, few studies have assessed the relationship between heavy metals usually found in the blood and serum cholesterol levels and the propensity of heavy metals to increase serum cholesterol levels.
We sought to discover any direct association between the levels of heavy metals and cholesterol in the blood. The hypothesis of this study was that increasing levels of blood cholesterol may be a direct result of heavy metals present in the blood and that the probability of high blood cholesterol increases after the level of heavy metals has exceeded a particular threshold. Previous studies have noted an association between increased serum levels of heavy metals with cardiovascular-related mortality. However, these studies lacked detail concerning the primary consequential effect of heavy metals, which increased mortality. We hypothesized that high cholesterol is one such consequential effect.
Methods
Data sources
The National Health and Nutrition Examination Survey (NHANES) is a nationally representative, cross-sectional survey that includes noninstitutionalized civilian populations of the United States. The NHANES began in the early 1960s; however, the survey has been conducted continuously since 1999, and the data are made available to the public in 2-year cycles. The NHANES is conducted by the National Center for Health Statistics (NCHS) and Centers for Disease Control and Prevention. 18
This analysis was conducted using NHANES 2009–2011 data based on NCHS recommendations. 19 The information was collected using multistage, stratified sampling of selected counties, blocks, households, and persons within households. The study protocol for the NHANES 2009–2010 and NHANES 2011–2012 data cycles was approved by the NCHS Institutional Review Board (protocol #2005-06 and protocol #2011-17, respectively). 20
Study population
A total of 19,591 individuals 0–80 years of age were surveyed from 2009 to 2012, and the study participants included individuals for whom some or all LDL-C, serum triglyceride, HDL-C, total cholesterol, blood Pb, and total blood Hg levels were available. We excluded samples with nonpositive weighting.
Measurements of heavy metal exposure
Serum Hg, Pb, and Cd concentrations were measured using inductively coupled plasma mass spectrometry (ICP-MS). This multielement analytical technique is based on quadrupole ICP-MS technology. Plasma is created by coupling radiofrequency power into a flowing argon stream seeded with electrons. The predominant species in the plasma are positive argon ions and electrons. Dilute whole blood samples are converted into an aerosol using a nebulizer inserted within a spray chamber and then through the central channel of the plasma, where they experience temperatures of 6000–8000 K. This thermal energy atomizes and ionizes the samples. The sample ions, along with the argon ions, enter the mass spectrometer through an interface that separates the ICP, which operates at atmospheric pressure (approximately 760 torr), from the mass spectrometer, which operates at approximately 10–5 torr. The mass spectrometer permits the detection of ions at each mass-to-charge ratio in rapid sequence, allowing the individual isotopes of an element to be determined. Once inside the mass spectrometer, the ions pass through the ion optics and then the mass-analyzing quadrupole before being detected as they strike the surface of the detector. The ion optics focus the ion beam using an electrical field.
Electrical signals resulting from detection of the ions are processed into digital information that is used to indicate the intensity of the ions and subsequently the concentration of the element. In this method, blood samples were diluted with 18 Mohm water and a diluent containing 1% v/v tetramethylammonium hydroxide, 0.05% disodium ethylenediaminetetraacetate, 5% ethyl alcohol, and 0.05% Triton X-100; gold was added to reduce intrinsic Hg memory effects, rhodium was added for the internal standardization of Cd, and bismuth was added for the internal standardization of Hg and Pb. The samples were prepared with a ratio of sample:water:diluent of 1:1:48. Cd and Hg were measured in micrograms per liter, and Pb was measured in micrograms per deciliter. 21
In this study, we categorized the participants into three tertiles (T1–T3) depending on heavy metal levels in increasing the order from the first to the third tertile.
Outcome measurements
Following overnight fasting for at least 9 h, venous blood samples were collected from the participants, processed, stored (frozen at −20°C), and analyzed at the Fairview Medical Center Laboratory at the University of Minnesota, Minneapolis, USA. Serum cholesterol and triglyceride levels were measured using a Roche Modular P Chemistry Analyzer (USA). 22,23 Abnormal blood lipid levels or dyslipidemia were defined as blood lipid levels outside the optimal triglyceride (<150 mg/dl), LDL-C (<100 mg/dl), HDL-C (≥60 mg/dl), and total cholesterol (<200 mg/dl) ranges. 24
Covariates
Age (years), sex (male/female), ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, other), and educational status (less than a high school education, a high school education, beyond a high school education), which correlates with socioeconomic status, were considered covariates in this study. Information on these covariates was obtained using questionnaires completed at the time of the surveys.
Statistical analysis
All statistical analyses were performed with SAS software (version 9.4, SAS Institute Inc., Cary, North Carolina, USA) using survey procedures accounting for the weighting and nesting of variables in a multistage clustered, probability sampling design and nonresponse. Weights for the combined NHANES 2009–2010 and NHANES 2011–2012 data cycles were obtained based on the NHANES guidelines. 18 The weight used in the analysis was calculated by multiplying each observation weight by 0.5 to account for the use of multiyear analysis.
We report baseline characteristics using means for continuous variables and percentages for categorical variables, and where applicable, we report the 95% confidence interval of the means and percentages. In comparing the characteristics across levels of heavy metal exposure, we used a t-test or analysis of variance for continuous variables and the χ 2 test for categorical variables.
To test associations between variables, we used multivariate regression models with age, sex, and socioeconomic status as covariates, and associations are reported in terms of odds ratios. The PROC SURVEYLOGISTIC procedure, in which we modeled the outcome as categorical, was used for logistic regression, and the PROC SURVEYREG procedure, in which we modeled the outcome as a continuous variable to compare means across different tertiles of heavy metal levels, was used for linear regression. For logistic regression, we used the cutoff stated above to categorize serum lipid levels as high and normal. Then, in the model, we used the new variable of high or normal serum cholesterol as the dependent variable and the heavy metal tertiles T1–T3 as independent variables while correcting for age, sex, and socioeconomic status. Three tertiles (T1–T3) of heavy metals were used to study whether there was a dose–response association between heavy metal exposure and serum cholesterol level.
We excluded missing observations from the analysis.
All of the reported analyses were two-tailed, and statistical significance was indicated by p < 0.05.
Results
The baseline characteristics of all the participants are shown in Table 1. Of the study participants, 50.27% (95% confidence interval (CI) 50.23–51.93) were female and 49.73% (95% CI: 48.07–49.73) were male. The mean age of the subjects was 36.93 years (95% CI 36.03–37.83). Non-Hispanic Whites accounted for 63.75% (95% CI 58.38–69.12), non-Hispanic Blacks accounted for 12.24% (95% CI 9.63–14.85), Hispanics accounted for 10.10% (95% CI 6.93–13.27), and others accounted for 13.90% (95% CI 13.12–22.46) of the study subjects. Approximately 46.92% (n = 3499) of the participants were educated beyond high school.
Baseline characteristics of the study population (n = 19,591) 0–80 years of age in the 2009–2012 National Health and Nutrition Examination Survey.
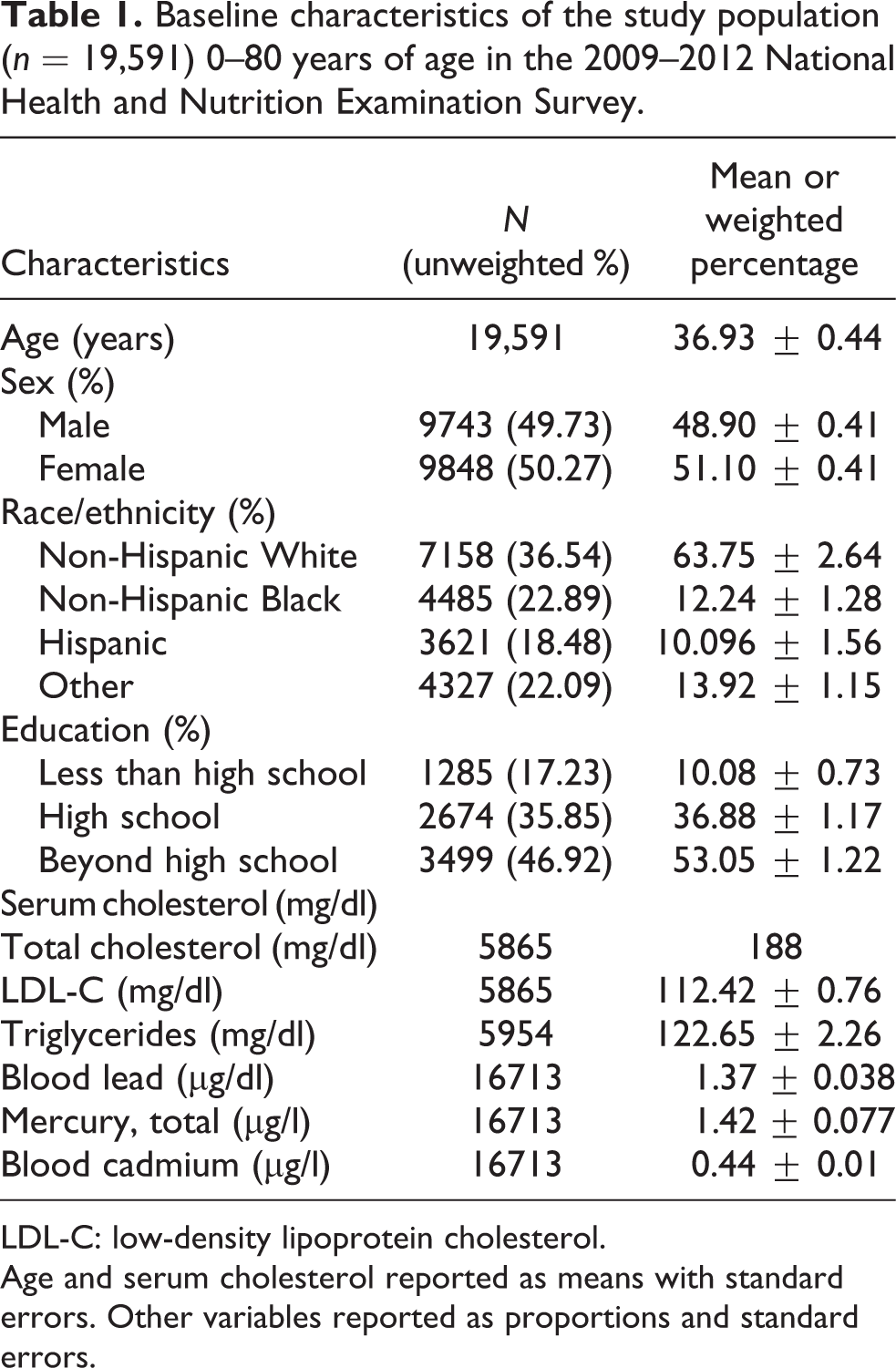
LDL-C: low-density lipoprotein cholesterol.
Age and serum cholesterol reported as means with standard errors. Other variables reported as proportions and standard errors.
The mean Pb level was 1.37 µg/dl (95% CI 0.04–1.29). The mean levels of Pb in the first, second, and third tertiles were 0.53 µg/dl (95% CI 0.52–0.54), 1.04 µg/dl (95% CI 1.03–1.05), and 2.61 µg/dl (95% CI 2.43–2.78), respectively. The mean Hg level was 1.42 µg/l (95% CI 1.26–1.58); in the first, second, and third tertiles, the mean Hg levels were 0.26 µg/l (95% CI 0.25–0.27), 0.68 µg/l (95% CI 0.67–0.69), and 3.03 µg/l (95% CI 2.76–3.29), respectively. The mean Cd level was 0.44 µg/l (95% CI 0.42–0.45). The mean levels of Cd in the first, second, and third tertiles were 0.13 µg/dl (95% CI 0.12–0.13), 0.24 µg/l (95% CI 0.23–0.26), and 0.89 µg/l (95% CI 0.84–0.93), respectively.
The mean total cholesterol level was 188.90 mg/dl (95% CI 187.43–190.36). The mean LDL-C level was 112.18 (95% CI 110.74–113.63). The mean triglyceride level was 124 mg/dl (95% CI 119.16–129.06).
The relationships between various participant characteristics across tertiles classified by total serum Hg and Pb levels and blood Cd levels are presented in Tables 2 to 4, respectively. The mean differences are reported in Table 5. There was no statistically significant difference in sex of the participants across the three tertiles with different total Hg levels. Individuals in T3 were more likely to have higher absolute total serum cholesterol (p < 0.0001) and LDL-C (p < 0.0001) levels than individuals in T2 who had higher total serum cholesterol and LDL-C levels than individuals in T1.
Characteristics of participants by tertiles based on total mercury level.

LDL-C: low-density lipoprotein cholesterol.
T1–T3 represent tertiles based on levels of the heavy metals studied.
Characteristics of participants in tertiles based on lead levels.

LDL-C: low-density lipoprotein cholesterol.
Characteristics of participants in tertiles based on cadmium levels.

LDL-C: low-density lipoprotein cholesterol.
Mean differences in serum cholesterol and triglyceride levels.a

Tchol: total cholesterol; LDL: low-density lipoprotein; TGL: triglyceride.
a Units are in mg/dl.
Individuals classified in tertile T3 based on Pb levels were more likely than those in tertiles T1 and T2 to be in the 20–39 years (T3 > T1 > T2, p = 0.0086), 40–59 years (T3 > T1 > T2, p < 0.0001), and more than 60 years (T3 > T1 > T2, p = 0.0005) age groups. There was a statistically significant difference in the gender of participants across the three tertiles classified by blood Pb levels. Individuals in T3 were more likely to have high total serum cholesterol (p < 0.0001), LDL-C (p < 0.0001), and triglyceride (p < 0.0001) levels than individuals in T2, who had higher levels of those parameters than individuals in T1.
Individuals classified in tertile T3 based on Cd levels more likely than individuals in tertiles T1 and T2 to be in the <20 years (T3 > T1 > T2, p < 0.0001), 40–59 years (T3 > T1 > T2, p < 0.0001), and more than 60 years (T3 > T1 > T2, p < 0.0001) of age groups. There was a statistically significant difference in the gender of the participants across the three tertiles classified by blood Pb levels. Individuals in T3 were more likely to have high total serum cholesterol (p < 0.0001), LDL-C (p = 0.0013), and triglyceride (P = 0.0340) levels than individuals in T2 who had higher levels of those parameters than individuals in T1.
The adjusted odds ratios of total cholesterol levels in tertiles of individuals based on heavy metal levels from two logistic regression models are presented in Tables 6 to 8. After adjustments for age, sex, and socioeconomic status, the odds of having high cholesterol were 1.3 times higher in the second tertile classified by Pb level (odds ratio (OR) 1.23, 95% CI 1.15–1.44) and 1.4 times higher in the second tertile classified by Pb level (OR 1.43, 95% CI 1.26–1.62) than that in the reference group T1. The odds of having high total cholesterol levels were 1.51 times higher in the second tertile classified by Hg level than in the first tertile (OR 1.51, 95% CI 1.37–1.68). Additionally, the odds of having high total cholesterol levels were 1.7 times higher in the third tertile based on Hg level than in the first tertile (OR 1.72, 95% CI 1.50–1.97). A positive association was also found for Cd; the odds of having high total cholesterol levels were 1.4 times higher in the second tertile than in the first tertile (OR 1.41, 95% CI 1.20–1.65), and the odds of having high cholesterol levels were 1.46 times higher in the third tertile than in the first tertile (OR 1.46, 95% CI 1.22–1.75).
Association between heavy metal and total cholesterol levels after adjusting for age, race, sex, and SES.a
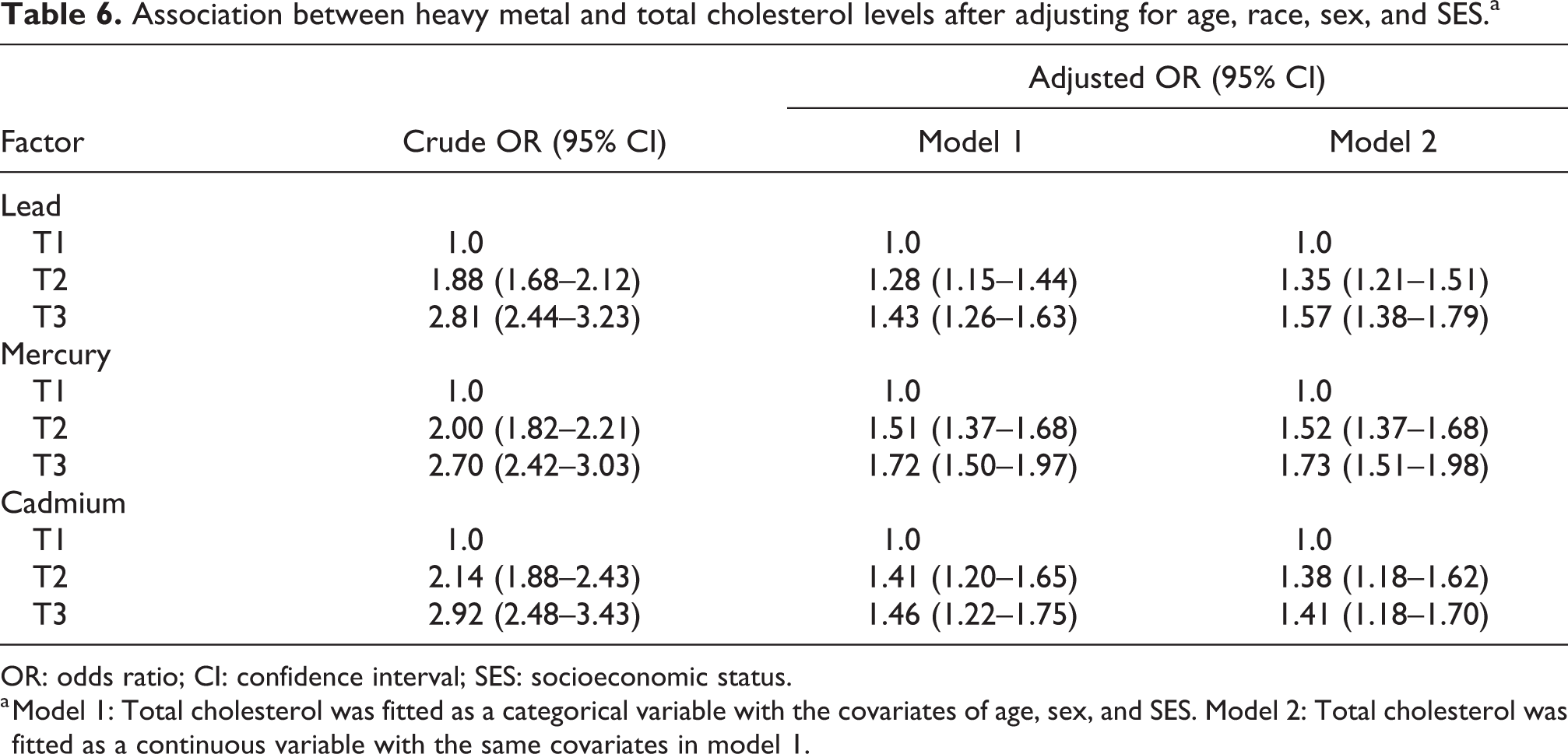
OR: odds ratio; CI: confidence interval; SES: socioeconomic status.
a Model 1: Total cholesterol was fitted as a categorical variable with the covariates of age, sex, and SES. Model 2: Total cholesterol was fitted as a continuous variable with the same covariates in model 1.
Association between heavy metals and other factors with LDL-C after adjusting for age, sex, and SES.
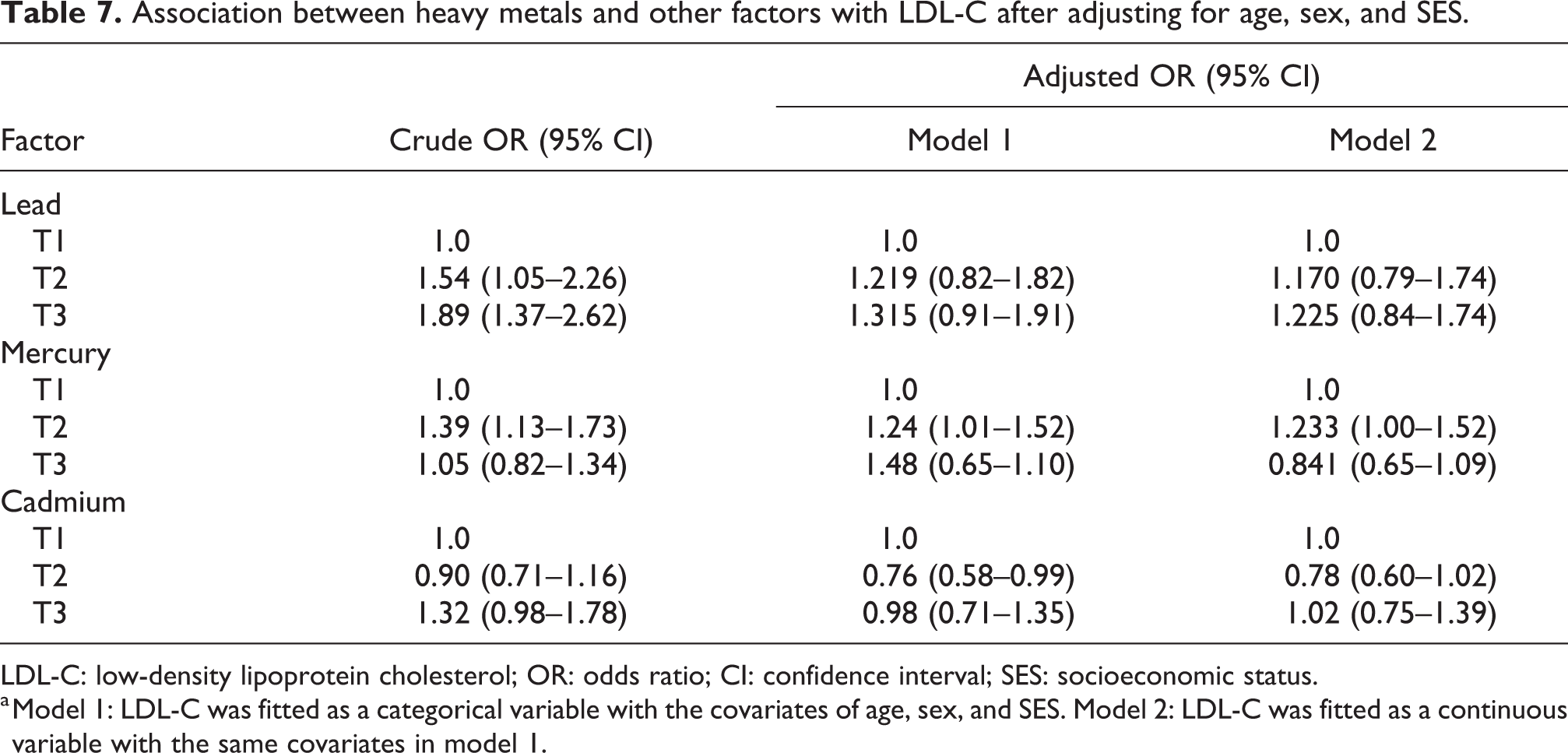
LDL-C: low-density lipoprotein cholesterol; OR: odds ratio; CI: confidence interval; SES: socioeconomic status.
a Model 1: LDL-C was fitted as a categorical variable with the covariates of age, sex, and SES. Model 2: LDL-C was fitted as a continuous variable with the same covariates in model 1.
Association between heavy metal levels and other factors with triglyceride levels after adjusting for age, sex, and SES.a
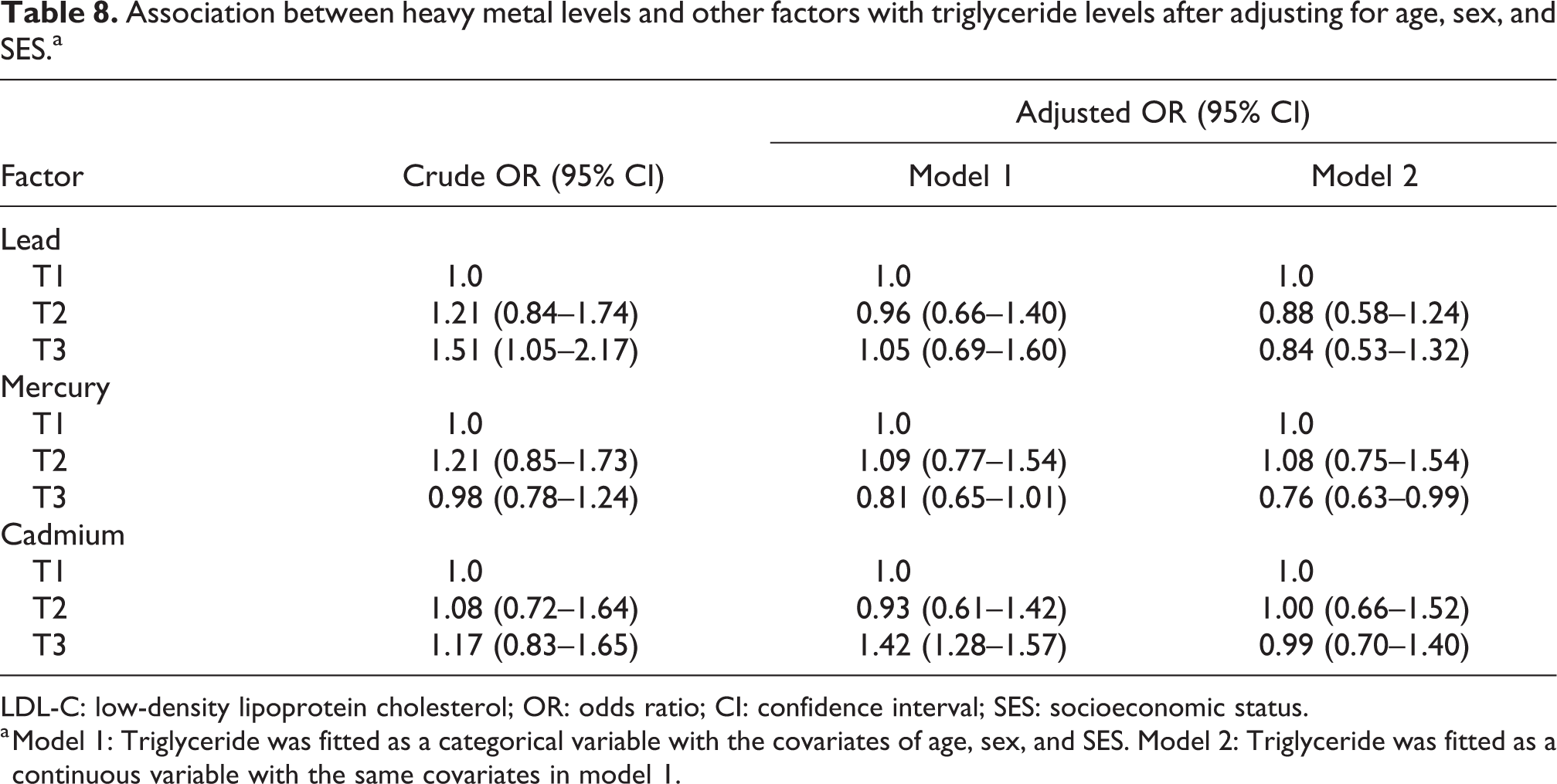
LDL-C: low-density lipoprotein cholesterol; OR: odds ratio; CI: confidence interval; SES: socioeconomic status.
a Model 1: Triglyceride was fitted as a categorical variable with the covariates of age, sex, and SES. Model 2: Triglyceride was fitted as a continuous variable with the same covariates in model 1.
The odds of having high LDL-C levels were higher in the second tertile classified by Pb levels than in the first tertile, but this difference was not statistically significant (OR 1.22, 95 CI 0.82–1.82). The odds of having high LDL-C levels were higher in the third tertile classified by Pb levels than in the first tertile, but this was also not statistically significant (OR 1.32, 95% CI 0.91–1.91). The odds of having high LDL-C levels were 1.24 times higher in the second tertile classified by Hg levels than in the first tertile (95% CI: 1.01–1.52), and the odds of having high LDL-C levels were 1.48 times higher in the third tertile than in the first tertile (95% CI 0.66–1.10). There was no statistically significant effect of Pb levels on cholesterol levels.
Additionally, as presented in Table 7, in the first model, there was no statistically significant effect of Cd on LDL-C levels. In the second model, the odds of having high LDL-C levels were significantly higher in the second tertile classified by Cd level than in the first (OR 1.23, 95% CI 1.00–1.52).
The odds of having high triglyceride levels were lower in the second tertile classified by pb level than in the first tertile (OR 0.96, 95% CI 0.66–1.40) but higher in the third tertile than in the first tertile (OR 1.05, 95% CI 0.69–1.60). There was no statistically significant effect of Hg and Cd levels on serum triglyceride levels.
As presented in Table 7, after adjustments for age and sex, the ORs (95% CI) of high triglyceride levels were not significantly different for individuals in T2 and T3 classified by Pb, Hg, and Cd levels compared to those in T1.
After adjustments for age and sex, the odds ratios (95% CI) of high triglyceride levels were not significantly different for individuals in T2 or T3 classified by Pb, Hg, and Cd levels, as presented in Table 8.
Discussion
Our study sought to gain a better understanding of the association between heavy metals (Pb, Hg, and Cd) and serum cholesterol levels. Very few studies on this association are available.
Our analysis demonstrated a 56% chance of high total cholesterol levels in the group with the highest level of Pb, a 73% chance of high total cholesterol levels in the group with the highest level of Hg, and a 41% chance of a high level of total cholesterol in the group with the highest level of Cd. For the study subjects with the highest levels of Pb, there was also a 22% chance of being in the group with the highest levels of LDL-C. There was an increase in the levels of total cholesterol and LDL-C in the third tertile classified by heavy metal levels compared to the first tertile, as presented in Tables 2 to 4. These findings are significant due to the implication of these heavy metals and the increased risk of CVD, which is a possible mechanism of action. 25 In a previous study, Hg diminished cardiovascular protection due to fish consumption. This study reported a monotonic increase in MI with an Hg toenail content of 0.25 µg/g. 26 A study conducted in North Korea demonstrated a positive association between Cd levels and ischemic heart disease; this association was also mentioned in a systematic review. 27,28
A proposed mechanism by which serum cholesterol is raised in the presence of Pb in the blood is through the effect of Pb on hepatic cholesterol metabolism, resulting in an increase in serum cholesterol levels. This finding could be due to the suppression of cytochrome p450, which is essential for lipid metabolism, or the induction of lanosterol alpha-demethylase, which is vital for cholesterol biosynthesis. 29 Pb-mediated hypercholesterolemia involves the activation of cholesterol synthesis enzymes, such as 3-hydroxyl-3-methylglutaryl-CoA reductase, farnesyl diphosphate synthase, and squalene synthase and the direct suppression of catabolic enzymes such as 7 alpha-hydroxylase. 29 This finding is very important, as exposure to Pb may be an essential factor in statin resistance. Additionally, Hg has the ability to increase LDL oxidation and plasma oxidized LDL, making LDL metabolism difficult and causing its subsequent accumulation. 4 In animal studies, Cd has been associated with increased serum triglyceride and total cholesterol levels. This association was attributed to a decrease in lipoprotein lipase activity. 30 As explained, we have a plausible physiological explanation for our findings.
In a cross-sectional study that measured occupational exposure to Pb, the group exposed to Pb had a higher level of total cholesterol than the control group. 31 Another study showed a positive association between Hg exposure, total cholesterol, and LDL-C levels. 32
As expected, our study is not without limitations. Like any other cross-sectional study, it focused more on prevalence rather than incidence. It is also challenging to predict whether the outcome predates exposure, or vice versa, as the timing of the outcome and exposure is unknown. We also did not have information on medications taken by the study participants. We attempted to reduce the effects of confounders by correcting some of these factors. For example, although we corrected for socioeconomic status, other factors, such as poverty, could have accounted for raised cholesterol levels in participants with an increased level of heavy metals.
Conclusion
In toxicological studies, heavy metals are found in measurable quantities in the blood. These metals have been implicated in the in vivo formation of free radicals and macrophage-derived lipid-laden cells, which promote the oxidation of LDL with atherosclerosis and atherosclerotic sequelae. Few studies have directly addressed the relationship between heavy metals and serum lipid levels. As shown in our study, elevated cholesterol has a significant relationship with incremental levels of heavy metals. This relationship could have grave cardiovascular consequences for those exposed, including individuals in situations such as the Flint water crisis, residents of “locked in” hurricane zones without access to potable water and those that follow practices leading to increased exposure to Hg, such as the ritual use of Hg in some parts of the world. More studies are needed to validate these findings in other individuals, and routine screening for these toxic metals should be considered to further mitigate the risk of atherosclerotic CVDs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.