
Abstract
Delta neutrophil index (DNI), which reflects the fraction of immature granulocytes, is used to detect infection and sepsis from noninfectious conditions, but few studies have evaluated in the early stage of acute poisoning. This retrospective observational study was performed on acute poisoning patients who visited to the emergency department (ED) and were consecutively admitted in intensive care units over 18-month period. The serial DNI, conventional inflammatory biomarkers, and culture results were obtained in the ED and after admission. The outcomes were the identification of sepsis, bacteremia, and 30-day mortality. Of 166 patients (mean age, 56.0 years) in this cohort, 59 (35.5%) had sepsis and 29 (17.5%) had bacteremia. Initial and peak DNI fractions 24 h after ED admission were strong independent predictors of sepsis development. Analysis of the area under the curve according to multiple receiver operating characteristics showed that DNI had a higher capability to predict sepsis than other parameters (0.815 for DNI, 0.700 for procalcitonin, 0.681 for C-reactive protein, and 0.741 for white blood cell). Using multivariable logistic regression analysis, it was found that DNI was an independent predictor of sepsis (95% confidence interval (CI) of odds: 1.03–1.18) and bacteremia (95% CI: 1.01–1.14). Therefore, initial and serial measurement of DNI may serve as useful risk predictor for development of sepsis or bacteremia in acute poisoning.
Introduction
Infection remains the leading cause of death among critically ill patients with acute poisoning. To reduce the mortality rates, early diagnosis of serious complications, adequate monitoring, and prompt treatment are required. 1,2 The type of infection that co-occurs with poisoning generally includes aspiration pneumonia, pancreatitis, gastrointestinal sepsis, and urinary tract infection. 3 The current guidelines for sepsis management emphasize early initiation of fluid resuscitation and appropriate antimicrobial therapy to improve patient outcomes and to reduce sepsis-induced mortality. 4,5 Immediate diagnosis of sepsis and identification of infection focus are important to provide the appropriate antibiotic treatment.
However, distinguishing between infection and noninfectious systemic inflammatory response syndrome (SIRS) is often difficult and presents a dilemma in poisoning due to toxin-induced febrile conditions and toxidrome. 6 Fever without bacterial infection can develop in acute poisoning owing to direct toxin effects (e.g. from anticholinergics and sympathomimetic agents), antidote-related adverse reactions (e.g. from atropine), withdrawal symptoms (e.g. from alcohol and benzodiazepine), neuroleptic malignant syndrome, and serotonin syndrome. With certain toxins, infectious parameters increase atypically, making it difficult to differentiate infection from other etiologies during the early stages of poisoning. 2,3,7 In the previous reports of the Toxicology Investigators Consortium Case Registry, drug-induced malignant hyperthermia (>40.5°C) was observed in 0.6% of all cases of acute poisoning. 3
Infection is commonly defined and graded by several parameters, such as increased white blood cell (WBC) count and elevated acute-phase infection markers like procalcitonin and C-reactive protein (CRP). 8 Procalcitonin is a potential diagnostic and prognostic biomarker of bacterial infection and sepsis, and it was recently described as a standard indicator of sepsis during treatment. 9 –11 Moreover, some studies also reported nonspecific increases in procalcitonin levels in response to certain drug actions. 12,13 Recent studies that investigated the infection status in patients with SIRS attempted to predict survival using the intensive care infection score, 14,15 neutrophil-to-lymphocyte ratio, 16 and delta neutrophil index (DNI), which are all indicators of the neutrophil left shift that occurs during bacterial infection and sepsis. 17 –20 The DNI is the immature granulocyte fraction provided by a blood cell analyzer; it is determined by subtracting the fraction of mature polymorphonuclear leukocytes from the sum of myeloperoxidase-reactive cells and reflects the number of immature neutrophils as a blood biomarker. This index is calculated by differentiating two granulocyte measurements; one measured using the cytochemical myeloperoxidase reaction and the other by the nuclear lobularity channel. 17 DNI strongly correlates with manual immature granulocyte count, and has been studied by several researchers as an adjunctive marker in infectious and inflammatory reactions. However, data on the clinical efficacy of neutrophil-related parameters for diagnosing sepsis in patients with acute poisoning are limited.
The aim of this study was to evaluate the efficacy of inflammatory biomarkers as early predictors of sepsis in acute poisoning patients visiting the emergency department (ED) and to compare reliability of DNI with that of conventional markers of infection, including procalcitonin, WBC count, and CRP, in patients with acute poisoning.
Materials and methods
Study design and patients
This retrospective observational study was performed on adults >18 years of age with acute poisoning, and approved by the institutional review board (KNUH 2018-09-017, 2019-05-32). Patients with acute poisoning who presented to the ED of a level 1 regional emergency medical center (a 960-bed tertiary hospital) from July 2016 to December 2017 were initially reviewed. It can provide chemical detoxification and critical antidotes based on stocks from the Korean Ministry of Health and Welfare. Serious poisoned patients were treated directly by emergency physicians and admitted to the 20-bed emergency intensive care unit (eICU) or the general ward. The exclusion criteria were (1) a medical history of abnormal hematological findings or leukemia, (2) malignancy, (3) admitted at ED 24 h after exposure to poisonous substances, (4) observation period ending within 48 h after admission, and (5) measurements of infection-related biomarkers unavailable for ≤1 h and/or 24 h (Figure 1).

Flowchart of patient enrollment and clinical outcomes.
Data collection
Clinical and toxicological variables relevant to the study included age, gender, initial vital signs at ED, poison-related data, radiologic results, and sputum/urine/blood culture results. Infectious biomarkers including WBC count, procalcitonin levels, CRP levels, and serum DNI fractions obtained in the ED and intensive care units were investigated. 21 To assess DNI, we used the same type of automatic hematology analyzer (ADVIA 120/2120; Siemens, Tarrytown, New York, USA) used for the analysis of complete blood cell count (CBC). 5,17
Definition and outcomes
SIRS was defined based on two or more of the following conditions: (1) body temperature >38°C or <36°C; (2) heart rate >90 beats/min; (3) respiratory rate >20 breaths/min or PaCO2 <32 mmHg; and (4) WBC >12,000 cells/mm3 or <4000 cells/mm3 or >10% immature (band) forms. 4 Sepsis was defined as activation of the inflammatory process due to infection within SIRS and was based on clinical assessments and cultures. 18 Thereafter, radiologic findings (chest radiography and computerized tomography) were reviewed and the infection focus (e.g. lungs or abdomen) was confirmed.
Study endpoints
The primary endpoints were sepsis and non-sepsis conditions. Secondary endpoints were septic shock, bacteremia, and in-hospital mortality.
Statistical analysis
Continuous variables were expressed as the median (interquartile range). Categorical variables were reported as the number of occurrences and frequency. Univariate χ2 tests and the Mann–Whitney test were used to compare categorical and continuous variables, respectively. Logistic regression analysis was used to identify the factor to predict the sepsis and bacteremia, and the results are expressed as odds ratio with 95% confidence interval (CI). We selected all demographic and laboratory variables with a p value <0.05 from univariate analysis, and then clarified the independent prognostic factors to the prediction of septic conditions in the early stage of poisoning using multivariable logistic regression analysis with an enter method in one single step. Considering time to event data, we performed the Kaplan–Meier survival analysis to obtain a promising prediction of 30-day mortality according to DNI elevation.
In addition, we calculated a linear mixed model with repeated-measures covariance within patients to determine the significance of the differences between the groups during the observational times. The model included two fixed effects: the determination of clinical outcomes (prediction of sepsis and bacteremia) and the serial measured time effect (initial DNI, at 24 h, 48 h, and at 72 h). To compare the predictions for the development of sepsis, areas under the receiver operator characteristic (ROC) curves were used to determine the optimal cutoffs of DNI, procalcitonin, erythrocyte sedimentation rate (ESR), CRP level, and WBC counts. p Values less than 0.05 were considered statistically significant, and all statistical analyses were performed using SPSS Statistics version 25 (IBM Corp., Armonk, New York, USA) and MedCalc (MedCalc Software, Mariakerke, Belgium).
Results
Study population
Figure 1 presents the enrollment and clinical outcome data of patients with acute poisoning. In 166 patients (median age, 56.0 years) with acute poisoning, pesticides (n = 58, 34.9%) were the most common poisonous substances, followed by antipsychotics and sedatives (n = 55, 33.1%), antidepressants (n = 12, 7.2%), and cardiovascular agents (n = 11, 6.6%). The clinical progress of patients after their admission was as follows: 24 patients (14.5%) received mechanical ventilator treatment, 26 (15.7%) were administered with inotropes for shock treatment, 67 (40.4%) developed fever during hospitalization, and 41 (24.7%) developed a complication of septic shock. In addition, 22 patients (13.3%) died in the hospital. The overall intoxication characteristics of the cohort are shown in Tables 1 and 2.
Clinical characteristics and intoxication-related data of the study cohort.

Clinical characteristics of the study patients according to the development of sepsis.a
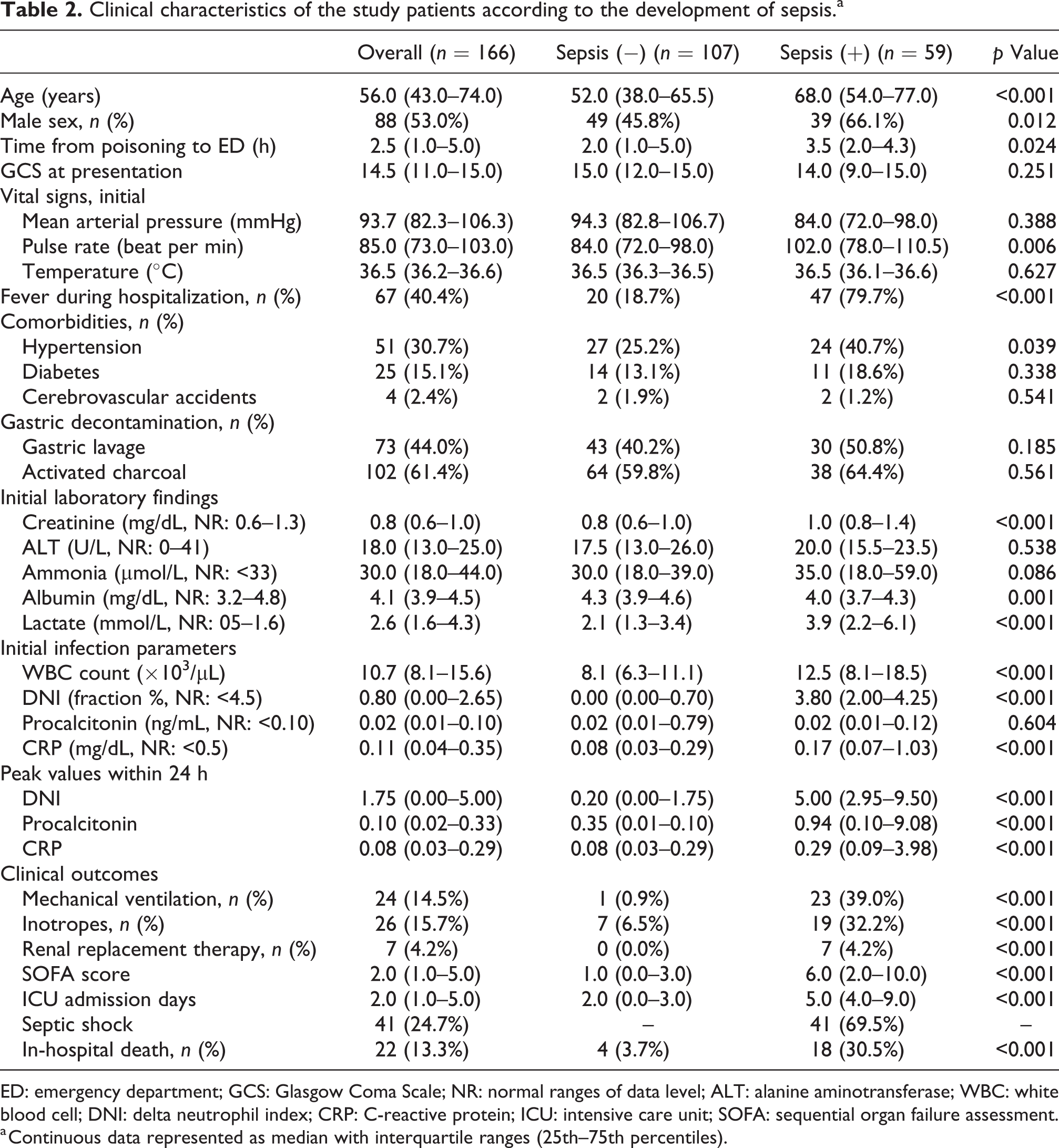
ED: emergency department; GCS: Glasgow Coma Scale; NR: normal ranges of data level; ALT: alanine aminotransferase; WBC: white blood cell; DNI: delta neutrophil index; CRP: C-reactive protein; ICU: intensive care unit; SOFA: sequential organ failure assessment.
a Continuous data represented as median with interquartile ranges (25th–75th percentiles).
Sepsis, septic shock, and bacteremia
Of the 166 patients with acute poisoning in the ICU, 59 (35.5%) were in the sepsis group. There were no significant differences in the initial mean arterial pressure, body temperature, and Glasgow Coma Scale score between the sepsis and non-sepsis groups. There were, however, significant differences in age, sex, interval to hospital admission after poisoning, pulse rates, number of patients with hypertension, the sequential organ failure assessment scoring, and use of inotropes (Table 2). Additionally, mechanical ventilator use, renal replacement therapy, and in-hospital mortality were significantly higher in the sepsis group. Other characteristics of the sepsis and non-sepsis groups are shown in Table 2. A comparison of the peak values of the infection parameters observed in the two groups at different time points showed that the level of DNI sharply increased from the initial value measured at the time of hospital admission to the maximum value measured within 24 h of admission (Table 2 and Figure 2(a)).
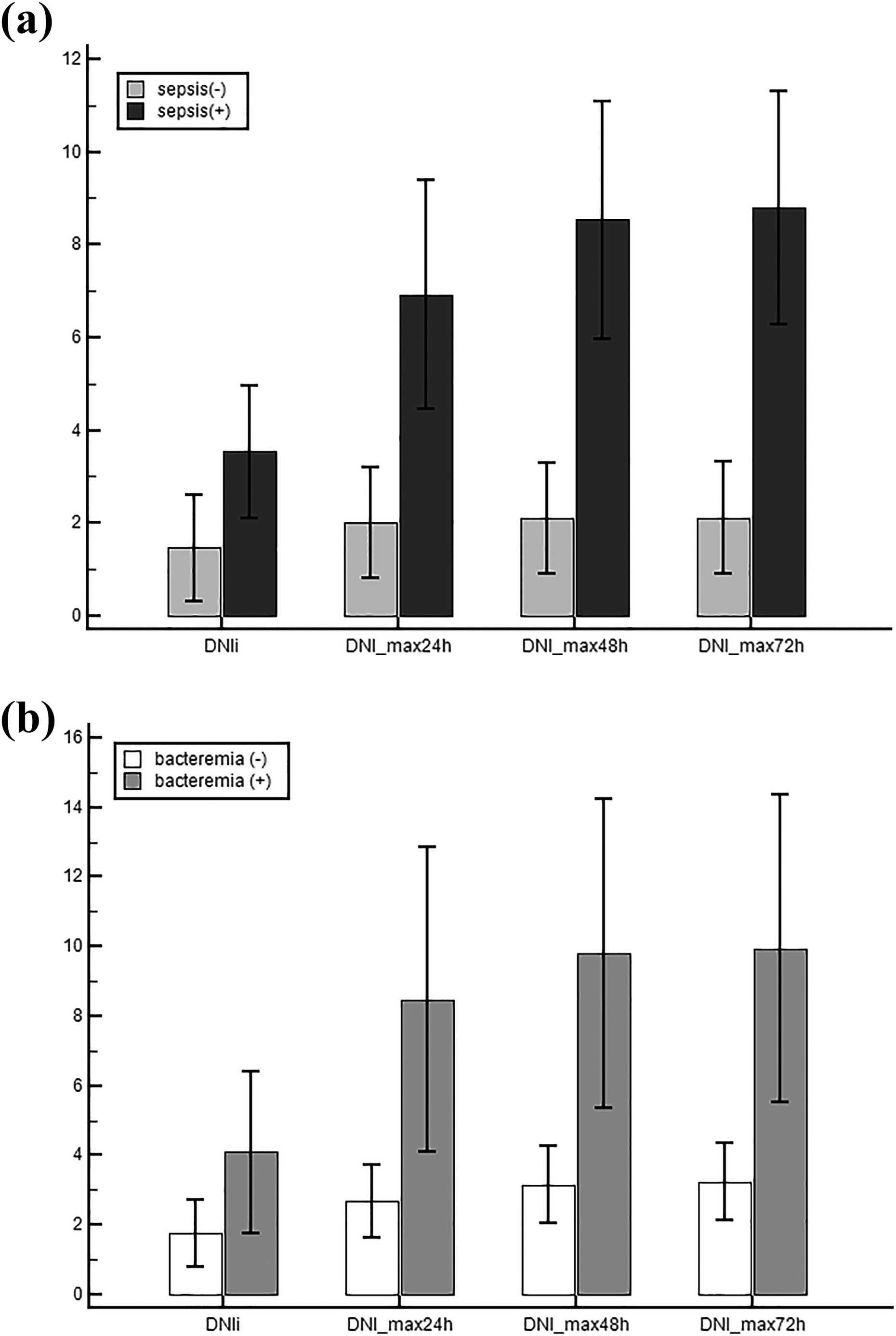
Linear mixed model of the DNI in the significant differences between groups over time according to the development of (a) sepsis and (b) bacteremia. These levels were measured at 0, 1, 2, and 3 days for the sepsis and non-sepsis groups (a). DNI values were already elevated at initial time and within 24 h after ED admission. Marked elevations of DNI fractions were similarly observed in the bacteremia group (b) at the same time points. DNI: delta neutrophil index; ED: emergency department.
In this cohort, 41 (24.7%) had septic shock and 29 (17.5%) had bacteremia. The linear mixed model revealed significant differences in DNI values between patients grouped according to the development of sepsis and bacteremia (all group × time interaction, p < 0.001) from ED admission to 72 h (Figure 2(a) and (b)). The Kaplan–Meier survival analysis demonstrated that elevation of DNI fractions within 24 h of ED admission was strong predictor of 30-day mortality (p < 0.001, Figure 3). The elevation of the DNI fraction was significantly associated with an increased 30-day mortality risk in adult patients with acute poisoning.

Survival curves according to DNI levels as a predictor of 30-day mortality. The elevation of the DNI fraction was significantly associated with an increased 30-day mortality risk in adult patients with acute poisoning. DNI: delta neutrophil index.
In multiple regression analysis, age and DNI were significantly associated with predictors of sepsis and septic shock. Conversely, ESR, CRP, and procalcitonin were not significant predictors (Table 3). For predicting bacteremia, on multivariable logistic regression analysis, CRP and DNI were identified as the significant predictors (Table 4).
Multivariable analyses for prediction of sepsis and septic shock.a

CI: confidence interval; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; PCT: procalcitonin; DNI: delta neutrophil index.
a Values shown are odds ratios (95% CI).
b Statistically logistic regression analysis was performed using the Enter method.
Univariate and multivariable analyses for prediction of bacteremia.a

CI: confidence interval; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; PCT: procalcitonin; DNI: delta neutrophil index.
a Values shown are odds ratios (95% CI).
b Statistically logistic regression analysis was performed using the Enter method.
Comparison of DNI and conventional infection parameters for predicting sepsis
To predict the development of sepsis, comparisons of the ROC curves show that the area under the curve (AUC) for the peak DNI 24 h after ED admission was significantly superior to those of other parameters (peak procalcitonin, CRP, ESR, and WBC count at the same time, Figure 4). In relation to the prediction of sepsis, the sensitivity and specificity of DNI were 76.3% and 81.3% (AUC: 0.809; cutoff: 2.1%) and 40.7% and 94.4% (in point of upper normal range, cutoff value 4.5%), respectively.
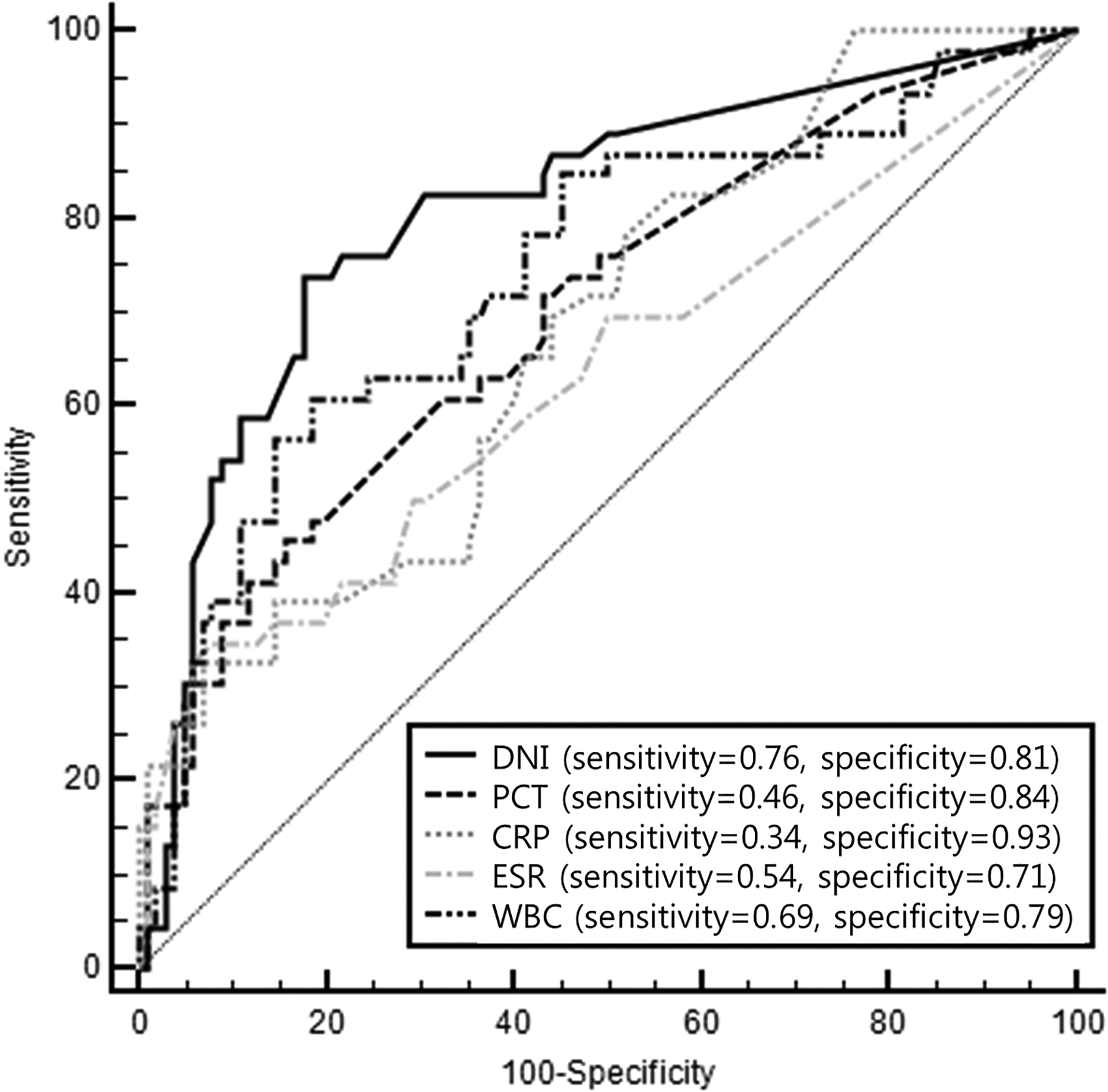
The ROC curves for the predictability of DNI and inflammatory biomarkers at 24 h after ED admission for predicting sepsis in acute poisoning patients. The ROC curves showed the optimal sensitivity and specificity for prediction of sepsis. On comparing peak DNI and other parameters, the areas under the curves for indicators were 0.815 for DNI, 0.700 for PCT, 0.681 for CRP, 0.632 for ESR, and 0.741 for WBC count. Associated cutoff criteria were defined as values corresponding to the maximal Youden’s index. DNI: delta neutrophil index; ED: emergency department; ROC: receiver operator characteristic curves; PCT: procalcitonin; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; WBC: white blood cell.
Discussion
Although this study is retrospective, we found that compared to other infection parameters, DNI levels across several time points showed the highest predictive capability for sepsis in critically ill patients with acute poisoning in this study. In particular, DNI differentiated sepsis from non-sepsis groups sooner and more efficiently. Serial DNI measurement is helpful in the treatment of acute poisoning by distinguishing between fever caused by infection versus noninfectious conditions (e.g. toxidrome or withdrawal).
While patients with acute poisoning often develop fever, 3 it is difficult to ascertain if the fever is caused by infection or a toxin. Distinguishing between these etiologies is important because infection requires prompt administration of antibiotics, whereas toxin-induced fever does not. The confirmation of infection can be determined through radiologic imaging and bacterial culture. However, these procedures cannot be performed routinely as they are costly and time-consuming.
In the present study, fever was observed in 67 patients during hospitalization (20 due to noninfectious causes). Various factors have been suggested to be fast and accurate predictors of infection, including the highly sensitive procalcitonin. However, procalcitonin testing is relatively expensive, and results require a relatively longer time to obtain. DNI reflects the fraction of circulating immature granulocytes, and it is elevated during sepsis. Therefore, several investigators have studied the capability of DNI to reliably predict the development of infection and sepsis. The DNI used in this study was based on the number of polymorphonuclear neutrophils obtained from the combined value of neutrophils and eosinophils that are automatically measured using the ADVIA 2120. Results are obtained simultaneously with leukocyte differential counts as a part of CBC count and therefore do not require additional time or cost. 17,20,22 WBC and neutrophil counts, which are measured together with DNI during CBC tests, are also easily obtainable indicators of infection. However, in terms of WBC count, both leukocytosis and leukopenia may occur during infection, which may lead to bidirectional changes (increases and decreases) in baseline data points; this can obfuscate the interpretation of these data. Therefore, a greater emphasis should be placed on immune dysfunction (i.e. neutrophil paralysis and immaturity) than on abnormal counts. 5 Furthermore, while the level of CRP shows a rapid increase within 6 h post-insult, its peak is relatively late (36–50 h). And it is nonspecific because it is also elevated in cancer and other conditions. 23 Collectively, our results indicate that DNI is a faster and more accurate indicator of infection and sepsis in critically ill patients with poisoning, thus avoiding the need for additional medical expenses.
It has been reported that serum DNI is useful for diagnosing sepsis in ICUs. For example, Park et al. 18 showed a correlation between DNI and severity of sepsis in patients in ICUs. Moreover, Zanaty et al. 24 found that DNI could be a more robust diagnostic and predictive indicator of the severity of sepsis or septic shock than lactate clearance. In contrast to the abovementioned studies, the current study was conducted in patients with acute poisoning and covered multiple time points to observe the infection-related parameters over time and compare their capability to predict sepsis at these time points.
One major finding in the current study was that DNI was more predictive of sepsis than other infectious indicators, and showed high reliability within 24 h of patients’ hospital admission. The sensitivity and specificity of DNI reached 76.3% and 81.3%, respectively, by day 1, whereas procalcitonin showed lower levels of accuracy during the same time. Following inflammation, serum DNI reportedly rises within 1 h and then decreases just as rapidly. DNI characteristically shows an increase for a maximum of 12 h before the occurrence of circulatory failure, and its half-life or response time is 3–6 h, whereas that of procalcitonin is 24–30 h. In our study, the DNI cutoff value for indicating the presence of accompanying sepsis in patients with acute poisoning was 2.1%. This was similar to the cutoff value of 2.7% obtained in a study of patients with Still’s disease and 1.8% in severe acute pancreatitis. 25,26 The DNI cutoff values in other similar studies of SIRS, sepsis, and severe sepsis were also approximately 2–7%. 18,19,27 Further studies need extended adjustment of cutoff points in various septic conditions or acute kidney injuries according to the commodities and emergent conditions.
This study had several limitations. First, patients were assigned to the study groups based on results of positive radiology or bacterial cultures, which may have led to underestimation of the number of patients with infection. Second, it also seems that the WBC count was a major confounding factor in defining infection, which explains the higher discriminative ability of DNI measurements. Further studies performed in larger patient cohorts should integrate those conditions to better understand their effects on DNI levels under sepsis.
Conclusion
In acute poisoning patients who presented to the ED, initial and serial measurement of DNI fractions may serve as useful risk predictor for development of sepsis or bacteremia. In patients who exhibit drug-induced toxidrome or withdrawal syndromes that are similar to sepsis, time series DNI values should be determined to detect underlying infections at the sites of poisoning to allow rapid intervention and reduce mortality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.