
Abstract
To evaluate the plasma levels and clearance of procalcitonin (PCTc) as prognostic biomarkers for patients with abdominal sepsis. A retrospective study of 103 patients with abdominal sepsis was conducted in our intensive care unit (ICU) from 2016 to 2018. Procalcitonin (PCT) plasma levels were measured at the time of diagnosis of abdominal sepsis and daily over the next 5 days. PCTc was calculated from day 3 to day 5. The prognostic accuracy of PCTc was expressed as the area under the receiver operating characteristic curve (AUROC). The Kaplan–Meier method was used to compare the survival curves by log-rank test. Logistic regression analysis was used to predict the 28-day mortality. The primary outcome was 28-day mortality since admission to ICU. Serum PCT levels from day 1 to day 5 did not differ significantly between survivors and non-survivors, while PCTc on day 5 was statistically significantly higher in survivors than that in non-survivors (86.4% vs 38.7%, P < 0.001). The cutoff value for PCTc-day 5 was 70%, with AUROC of 0.726, sensitivity of 64.6%, and specificity of 78.3%. The 28-day mortality was significantly lower among those with PCTc-day 5 >70% compared with those with PCTc-day 5 <70% (9.1% vs 38.3%, log-rank test, P < 0.001), and odds ratio (OR) was 0.16 (95% confidence interval (CI): 0.05–0.48, P < 0.001). The ability to decrease PCT by at least 70% on day 5 was an independent predictor of 28-day mortality after admission to ICU with moderate accuracy.
Introduction
Intra-abdominal infection and injury are common causes of sepsis in intensive care unit (ICU) patients and lead to high rates of mortality.1–3 Among critically ill patients, abdominal pathology leading to abdominal sepsis is common and carries a mortality rate of 30%–50%. 4 Early diagnosis and treatment of infection is associated with improved outcome and reduced mortality. 5 Although many different monitoring and scoring systems exist, daily clinical examination is the most reliable diagnostic tool in identifying patients with sepsis. 6 Tumor necrosis factor (TNF), interleukin 1 (IL-1), and interleukin 6 (IL-6) are valid and sensitive indicators; 7 however, they cannot be measured in a routine manner for diagnosis in the clinical settings. Procalcitonin (PCT) is a new indicator of bacterial infection and sepsis that can be routinely measured in clinical laboratory investigations. 8
PCT, a precursor of calcitonin consisting of 114–116 amino acids, is elevated in several systemic inflammatory conditions. 9 Most studies indicate that the ability of PCT to predict mortality is poor.7,10,11 As the half-life of PCT is only 24 h, theoretically, it is possible that the early kinetics of PCT may correlate with survival. Recently, several studies have suggested that PCT clearance was better than a single cutoff value to predict outcomes. Persistently high PCT levels demonstrated an association with significantly increased mortality in patients with sepsis.12,13 It is important to identify patients who are unresponsive to treatment after 24–48 h. 14 If patients are unresponsive to therapy and deteriorate rapidly, the treatment plan should be reassessed. 15
Intra-abdominal infections are the second most common cause of infectious mortality in ICUs. 16 Besides, robust data assessing the value of PCT for monitoring treatment response in abdominal sepsis are rare. 17 Therefore, we decided to assess the predictive value of PCT clearance in comparison with the PCT level in ICU patients with abdominal sepsis.
Materials and methods
Patient population
A sample size of 98 patients was needed to achieve the relevant anticipated area under the receiver operating characteristic curve (AUROC), that is, 0.7, at a significance level of 5%, power of study of 80%, precision of 10% on either side, and 20% dropout rate. A total of 103 patients in ICU at Renji Hospital were retrospectively studied from 2016 to 2018. This study was approved by the local ethics committee. Written informed consent was waived off by Institutional Ethics Committee due to the nature of a retrospective study.
Inclusion criteria include adult patients (above 18 years) who met the International Guidelines of the Surviving Sepsis Campaign. Patients with acute pancreatitis were excluded because PCT is increased in acute pancreatitis, regardless of the presence of an infectious complication.
In our ICU, the measurements of PCT levels were conducted upon ICU admission and for the next 5 days. The day of ICU admission was defined as day 0. Patients were followed up until day 28, and the primary outcome was the mortality related to abdominal sepsis at day 28. Results from patients who were discharged during this period were not analyzed.
Diagnosis of abdominal sepsis and septic shock
Abdominal sepsis was defined as an increase in the Sequential (Sepsis-related) Organ Failure Assessment (SOFA) score of 2 points or more, which caused by presumed or confirmed infection (Sepsis-3). 18 Septic shock was defined as evidence of infection and a systemic response to infection, in addition to a systolic blood pressure of <90 mmHg despite adequate fluid replacement, and a need for at least 1-h administration of vasopressors, according to the Surviving Sepsis Campaign (SSC) International Guidelines. 19
PCT measurement
PCT levels were assessed by electrochemiluminescence method with analyzer (Cobas e411; Roche Diagnostics GmbH, Mannheim, Germany) by original reagents. Calibration solution, reagents, and quality control materials were provided by Roche. The clearance of procalcitonin (PCTc) from day 3 to day 5 was calculated using the following formula: PCTcday 3–5 = [(PCT0 – PCTday 3–5)/PCT0] × 100%.
Data collection
The collected data included demographic data, site of infection, type of causative microorganism(s), results of blood cultures taken in the first hour, the Acute Physiology and Chronic Health Evaluation II (APACHE II) score and Sequential Organ Failure Assessment (SOFA) score on admission, PCT level on admission and the following 5 days, use of mechanical ventilation and vasopressors, and length of stay in ICU. The primary outcome was 28-day mortality. Patients were divided into two groups: survivors and non-survivors.
Statistical analysis
Continuous data are expressed as mean ± standard deviation for normally distributed data, and median with interquartile range (IQR) for non-normally distributed data. The chi-square test or the Fisher’s exact test was used to compare categorical variables. A comparison of continuous variables that did not follow normal distribution test was done using the Mann–Whitney U-test. The prognostic accuracy of PCTc was expressed as the AUROC. The optimal cutoff values were obtained using Youden’s Index. The Kaplan–Meier method was used to compare the survival curves by log-rank test. Logistic regression analysis was used to predict the 28-day mortality. P < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS for Windows (version 19.0; SPSS Inc., Chicago, IL, USA).
Results
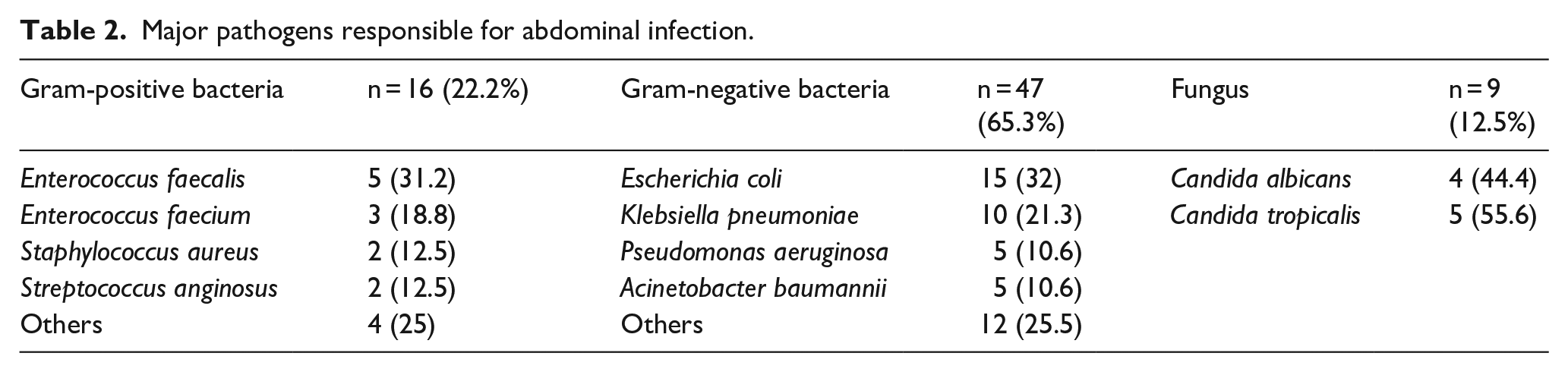
In our study, 195 patients who met the inclusion criteria were initially enrolled, with 92 excluded because of hospital discharge, missing initial blood samples or information regarding the primary outcome (Figure 1). A total of 103 patients were finally eligible for the study analyses. The demographics of the included patients are presented in Table 1. The mean age was 67.9 ± 14.2 years with 64.4% male and 35.6% female patients. The mean APACHE II score was 24.9 ± 7.3, and the mean SOFA score was 10.2 ± 3.6. Fifty patients (48.5%) required mechanical ventilation and 65 patients (63.1%) required vasopressor therapy within the first 24 h of their ICU stay. A positive blood culture was found in 26.2% of patients. The median length of ICU stay was 6 days (IQR: 3–15) and 66 patients exhibited septic shock (Table 1). Both APACHE II and SOFA scores were higher in the non-survivors; however, neither score showed a significant difference between the two groups. Besides, serum PCT levels on days 0–5 did not have significant difference between survivors and non-survivors. Factors that showed a significant difference between survivors and non-survivors just included receiving mechanical ventilation (P = 0.01). Pathogens responsible for abdominal infection were shown in Table 2. Gram-negative bacteria were the major pathogens, which accounted for 65.3%.
Demographic and clinical characteristics of the studied population.
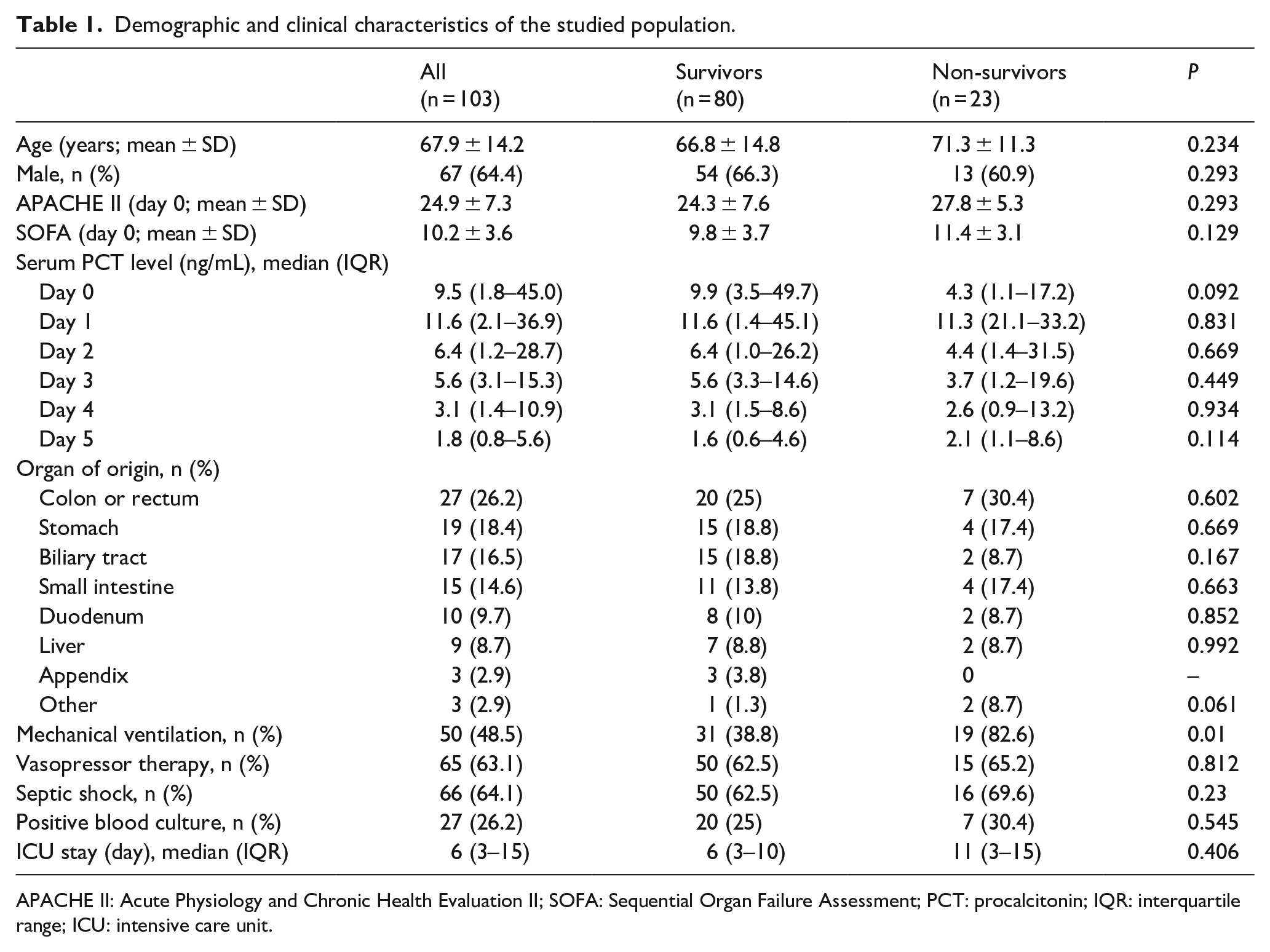
APACHE II: Acute Physiology and Chronic Health Evaluation II; SOFA: Sequential Organ Failure Assessment; PCT: procalcitonin; IQR: interquartile range; ICU: intensive care unit.
Major pathogens responsible for abdominal infection.

Flowchart of the study process.
As regards PCT clearance, it was significantly higher in survivors group than in non-survivors group on day 5 (P < 0.001) (Table 3). The AUROC was 0.726 (95% confidence interval (CI): 0.61–0.84) for PCTc-day 5. According to the Youden’s index, the cutoff value for PCTc-day 5 was 70%, with sensitivity of 64.6% and specificity of 78.3%. The 28-day mortality was significantly lower among those with PCTc-day 5 >70% compared with those with PCTc-day 5 <70% (9.1% vs 38.3%, log-rank test, P < 0.001) (Figure 2). The univariate logistic regression showed that the odds ratio (OR) of PCTc-day 5 >70% to predict 28-day mortality was 0.16 (95% CI: 0.05–0.48, P < 0.001).
Clearance of procalcitonin from day 3 to day 5 in survivors and non-survivors.

PCT: procalcitonin.

The Kaplan–Meier 28-day survival analysis comparing PCTc-day 5 >70% and PCTc-day 5 <70%.
Discussion
Sepsis is the leading cause of death among critically ill patients. Intra-abdominal infection is associated with significantly increased morbidity and mortality. Nearly 25% of severe sepsis or septic shock is due to intra-abdominal infection. In this retrospective observational study, we found that PCTc-day 5 could be a predictor of the prognosis in patients with abdominal sepsis, while isolated determinations of serum PCT levels showed no correlation with prognosis.
Recently, the discriminatory and prognostic significance of PCT clearance has gained interest in clinical research. Suberviola et al. 20 found that in 88 patients admitted to a general ICU with septic shock, the mortality rate in patients with increased PCT clearance in the first 72 h after ICU admission was lower than in patients with reduced clearance (15.4% vs 58.8%, P < 0.01). Ruiz-Rodriguez et al. 13 reported a significant increase in PCT clearance after 24, 48, and 72 h of treatment in survivors and a reduction in non-survivors. As regards abdominal sepsis, our study tried to focus on PCT clearance from day 3 to day 5 with all patients diagnosed with sepsis or septic shock caused by intra-abdominal infection. We found that PCT clearance on day 5 had significant difference between survivors and non-survivors. However, isolated serum PCT levels from day 0 to day 5 did not differ significantly between survivors and non-survivors group. Our results showed that the cutoff value for PCTc-day 5 to predict 28-day mortality was 70% with OR of 0.16 (95% CI: 0.05–0.48, P < 0.001). In addition, patients with PTCc-day 5 >70% had significantly lower 28-day mortality than those with PTCc-day 5 <70%. Schuetz et al. 21 indicated that ability to decrease PCT by more than 80% is a significant independent predictor of 28-day mortality. Huang et al. 12 also reported that patients with increased PCTc-day 5 of more than 80% may have lower 28-day mortality rate compared with those below 44%. Ryu et al. 22 found that a cutoff value of 78% of PCTc could be used to stratify patients, and 28-day mortality was significantly lower among those with high levels of PCTc. However, in this study, the AUROC of PCTc-day 5 to predict 28-day mortality was 0.726. Therefore, it just had moderate accuracy.
Our study has some limitations. First, it is a single-center retrospective observational study. Our results needed to be confirmed by large multicenter studies. Second, we did not collect information about antibiotic therapy to the pathogen and its appropriateness. Third, time zero was difficult to define because of the retrospective nature of study. Last but not least, we did not compare PCT clearance with other indicators, such as C-reactive protein (CRP) clearance or SOFA changes, which could be investigated in the future study.
Conclusion
The prognosis of patients with abdominal sepsis may be associated with PCTc. The ability to decrease PCT by at least 70% on day 5 was an independent predictor of 28-day mortality after admission to ICU with moderate accuracy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by 2018 Shanghai “Rising Stars of Medical Talent” Youth Development Program (SHWSRS (2019)-72).