
Abstract
Background:
Limited information exists about epidemiology and management of mushroom poisoning. We analyzed and described epidemiology, clinical presentation, and clinical course of mushroom-poisoned patients admitted to emergency departments (EDs) of the Province of Parma, Italy.
Methods:
Data from the database of mycological service were matched with clinical information retrieved from hospitals’ database, from January 1, 1996 to December 31, 2016.
Results:
Mycologist consultation was obtained in 379/443 identified mushroom poisonings. A remarkable seasonality was found, with significant peak in autumn. Thanks to the collaboration, the implicated species could be identified in 397 cases (89.6%); 108 cases (24.4%) were due to edible mushrooms, Boletus edulis being the most represented (63 cases). Overall, 408 (92%) cases presented with gastrointestinal toxicity. Twenty cases of amatoxin poisoning were recorded (11 Amanita phalloides and 9 Lepiota brunneoincarnata). One liver transplantation was needed. We observed 13 cases of cholinergic toxicity and 2 cases of hallucinogenic toxicity. Finally, 46 cases were due to “mixed” toxicities, and a total of 69 needed hospitalization.
Conclusions:
Early identification and management of potentially life-threatening cases is challenging in the ED, so that a mycologist service on call is highly advisable, especially during periods characterized by the highest incidence of poisoning.
Introduction
The term “mushroom” is generally referred to the fleshy, spore-bearing fruiting body of higher fungi, typically growing above soil, that is their food source. The underground and vegetative part of a fungus is known as “mycelium” and consists of a mass (often several times heavier than the mushroom itself) of branching, thread-like hyphae.
The first written record about mushroom poisoning is included in an epigram of the Greek poet Euripides (fifth century BC), commemorating the death of a woman and her three children, all deceased during the same day after mushroom ingestion. 1 Some centuries later, the famous Latin philosopher Lucius Annaeus Seneca (4 BC to 65 AD) stated that “Fungus, qualiscumque sit, semper malignus est,” that is, every kind of mushroom is poisonous. 2 Despite this, mushrooms have been actively harvested and consumed for centuries, all around the world.
Worldwide, there are at least 5000 well-classified mushrooms species, up to 100 of which are known to be poisonous to humans, whereas only 200–300 have been clearly established to be safely edible. 3 The number of mushroom species in Europe is thought to be around 2000. 4 –6 Less than 100 of these European species are known to be poisonous, 35 of which containing amatoxins. 5 –8
Although mushrooms are ubiquitous and widely appreciated as foods, wild mushroom intoxication is a relatively infrequent cause of emergency department (ED) visit in European countries. 9 The actual yearly incidence is not completely defined, since it is highly dependent on local ecology and gastronomic traditions, but is believed to be somehow underdiagnosed or underreported. 10 Based on a Swiss Poison Center database, it has been reported that the incidence of mushroom intoxication may approximate 5 cases per 100,000 inhabitants per year, representing only 1.1–1.6% of all poisoning cases recorded in the Swiss Poisons Information Center. 9,11 During the year 2014, over 4500 harvests have been controlled by the Swiss Mushroom Control Association (Schweizerische Vereinigung Amtlicher Pilzkontrollorgane: VAPKO), concluding that up to 37% contained inedible mushrooms and 12% contained poisonous species, accounting for 49% of the entire sample. 12 It is also well established that mushroom poisoning may sometimes occur with ingestion of edible mushrooms, which have been improperly collected, transported, stored, and cooked. 13
The toxicity profile of most mushroom species has not been investigated so far. 5,6 A kaleidoscope of clinical syndromes, however, may be attributable to mushrooms consumption, mostly depending on the species, but with meaningful differences within the same genus (e.g. Amanita phalloides, potentially lethal; Amanita muscaria, toxic but not lethal; and Amanita cesarea, one of the best edible mushrooms worldwide, are comprised within the genus Amanita). 14 –16 Gastrointestinal symptoms are present in most cases of poisoning but are highly nonspecific and potentially mask more serious toxicity. 16 It has been for long acknowledged that poisoning occurring in patients with early symptoms after consumption (i.e. typically comprised between 30 min and 6 h) is relatively harmless and can generally be managed with symptomatic therapy, whereas delayed symptoms (i.e. later than sixth hour from ingestion) are thought to be unspecific severity indices, underlying that the toxins may be cause of delayed severe evolution. 16 Nonetheless, different mushroom species are often consumed in the same meal, possibly having both “early” and “delayed” toxicity, representing an additional source of mystification. Moreover, new forms of mushrooms toxicity, as well as new poisonous species, are increasingly being described. 17 –25
Due to the aforementioned confounding factors, the management and risk evaluation of mushroom poisoning is often challenging for the emergency physicians (EPs). The type of mushrooms is frequently unknown even by the patient, whereas more than one single species has often been mixed and consumed. The initial presentation and the heterogeneity of symptoms can sometimes be misleading and worrying, but they do not correlate with severe complications of mushroom poisoning. 16
There is limited, sparse, and dated information about clinical characteristics and management of ED visits for mushroom poisoning in Europe, and in particular in Italy. 26 As such, the aim of this study was to analyze and describe the epidemiology, clinical presentation, morbidity, and mortality of mushroom-poisoned patients admitted to the three EDs in the Province of Parma, Northern Italy.
Methods
Nearly 20 years ago (in 1996), the local healthcare administration instituted a service of mycological consultation, available on call 24/365 for the three hospitals operating in the Province of Parma, Emilia Romagna Region, northern Italy. Beginning from 1996, the EPs of the three hospitals have been offered the possibility to have an identification of the fungal species in all cases of suspected or confirmed mushroom poisoning, both after macroscopic analysis (i.e. with examination of remainders of the meal, gastric lavage, or vomited material) and with microcopy identification of the spores, which are highly species specific. Data stored in the database of the mycological consultation service were matched with clinical data (i.e. symptoms, significant organ involvement, treatment, and disposition) retrieved from the hospitals’ database, from January 1, 1996 to December 31, 2016. This has allowed to obtain a clear epidemiological picture of mushroom poisonings in our province as well as a “real-world” figure about the current management of mushroom poisoning.
The three hospitals (i.e. a university and teaching hospital and two rural hospitals) serve a population of approximately 440,000 inhabitants and are the only hospitals in the area. The study population so included virtually all mushroom poisoning episodes occurred in the community. Urban and rural populations are represented in a nearly equal frequency, according to the distribution of the population in our area. The climate of the province is considered typical of the central-southern Pianura Padana area (also known as “Po river valley”), including a significant portion of hills and mountains (not exceeding the altitude of 2000 m), and thus continental with precipitations peaking in fall and spring. The peak of raining season is in October and November (averaging 96 and 114 mm per month, respectively), whereas January and July are the driest months (averaging 40 and 47 mm per month, respectively). The summer is hot, with peak temperatures between 30 and 35°C, whereas the winter is cold, with minimum temperatures occasionally below −10°C. 27 Since mushroom biology is highly influenced by the rainfall, air temperature, and humidity, these climate characteristics are of paramount importance for influencing the seasonality of mushroom poisoning episodes.
Due to the retrospective nature of the study and the maintenance of anonymity of all subjects, the consensus of the ethical committee was unnecessary. The study was performed in accordance with the Declaration of Helsinki, under the terms of relevant local legislation.
Results
Overall, 443 cases of mushroom poisoning have been identified in the hospitals’ database, 241 in the university hospital, 102 and 100 in the 2 other rural hospitals. Mycologist consultation was obtained in 379 cases, whereas in 64 other cases, mycologist counseling was not requested, mostly due to the very mild symptomatology of the poisoning or due to the mycological expertise of some of the EPs. Figure 1 shows the annual distribution, highlighting a considerable yearly difference, which is attributable to the different rainfall. Despite annual differences, mushroom poisoning episodes were found to peak each year during the autumn, reflecting the local biology of these organisms (Figure 2). Globally, the mushroom species could not be identified in 46 cases (10.4%) of poisoning, whereas in the remaining 397 cases (89.6%), a final identification could be attained. All the ages are represented in the entire study population, following a near-Gaussian distribution, and peaking in the fifth decade. Interestingly, some children aged between 1 and 6 years were also included in the hospitals’ database, despite the intake of mushrooms is discouraged at this age. The explanation is that the children in our community spontaneously assumed mushrooms found in the fields surrounding their schools or houses. Even more surprisingly, three pregnant women, needing careful observation and monitoring, were also identified. Several cluster poisonings (families, friends eating the same meal, etc.) were recorded, whereas single-patient episodes were 175, so that 60.5% of cases were attributable to cluster pattern (2 patients: 53 clusters; 3 patients: 15; 4 patients: 11; 5 patients: 7; 6 patients: 5; 7 patients: 0; 8 patients: 1). Overall, 108 cases (i.e. 24.4%) were caused by edible mushrooms ingestion, usually for long-term storage of mushrooms or dishes, storage in plastic bags, or inappropriate cooking. Among these, Boletus edulis was the most frequent species (i.e. 63 cases, 58 as single species, and 5 cases in association with A. cesarea). This is reasonable, since both species are highly consumed in our country.

Annual distribution of mushroom poisoning in the Province of Parma, years 1996–2016.
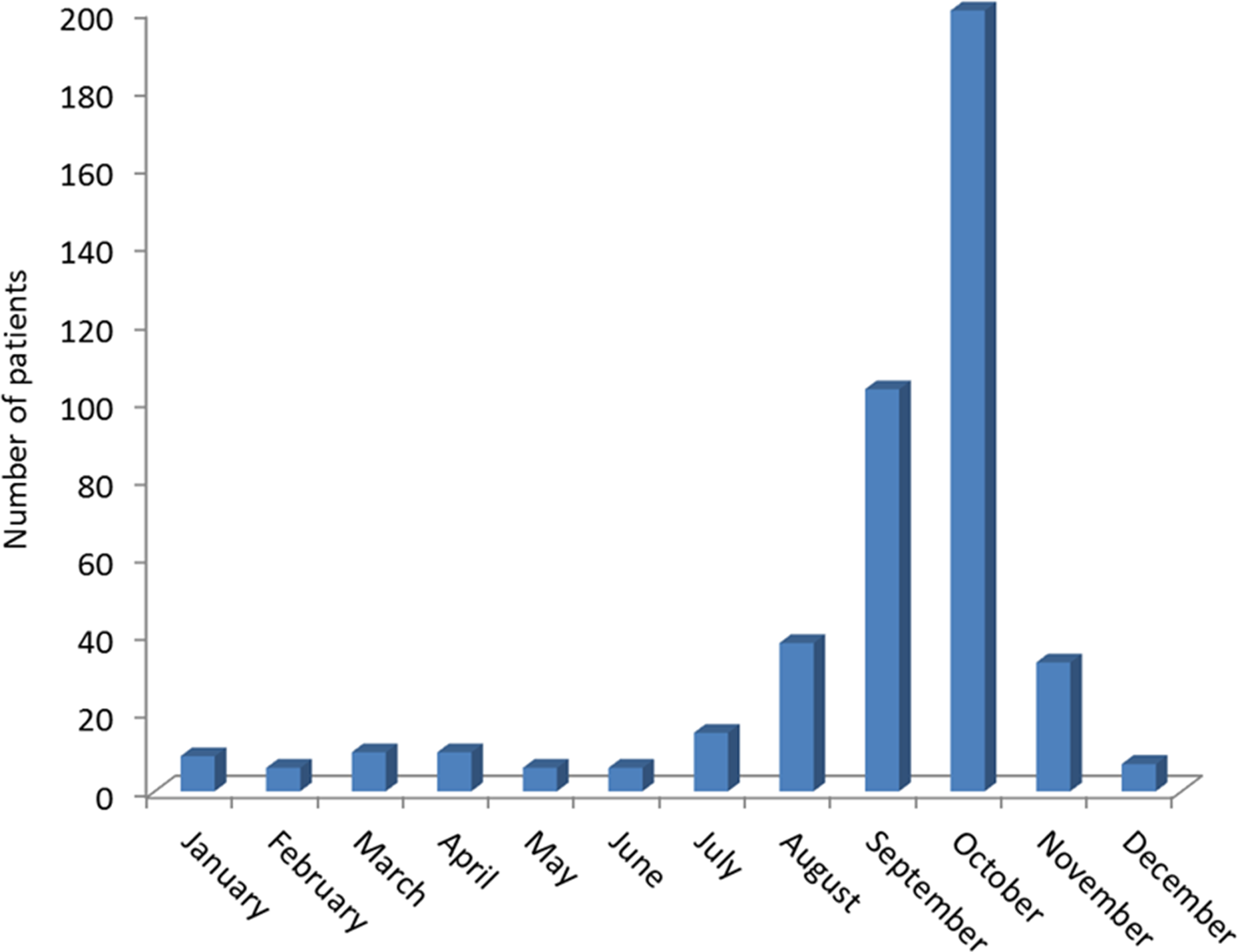
Monthly distribution of mushroom poisoning in the Province of Parma. Bar represents the sum of patients diagnosed during the same month throughout the study period (i.e. 1996–2016).
The vast majority of cases (i.e. 408, 92%) were characterized by simple gastrointestinal toxicity, usually managed conservatively with symptomatic agents (in most cases metoclopramide) and hydration. Atropine was used for 9/13 cholinergic syndromes (4 mild cases did not need to be treated with the antidote). The most severe cases (n = 20) were all caused by amatoxin poisoning, 11 by A. phalloides and 9 by Lepiota brunneoincarnata. One of these cases, attributable to A. phalloides poisoning, needed liver transplantation and survived. All the other patients also survived after administration of charcoal, acetylcysteine, intensive care unit admission, and forced hydration. It should be noted that in Northern Italy, penicillin G and silibinin are not usually prescribed for amatoxin poisoning, thus acetylcysteine is the antidote widely used for this indication. We observed 13 cases of cholinergic (i.e. muscarinic) toxicity, usually due to Inocybe or Clitocybe spp., 2 cases of hallucinogenic toxicity (due to Panaeolus spp.), and 46 cases of “mixed” toxicities (i.e. cholinergic + hallucinogenic, gastrointestinal + cholinergic, and gastrointestinal + hallucinogenic). No case of amatoxin poisoning belonged to the “mixed toxydrome” group.
Overall, 69/408 cases needed hospitalization, including all 20 cases of amatoxin poisoning, 9/13 cases of cholinergic syndromes, and 40 cases due to comorbidities (usually elderly or pregnant women) rather than to the severity of the mushroom poisoning itself.
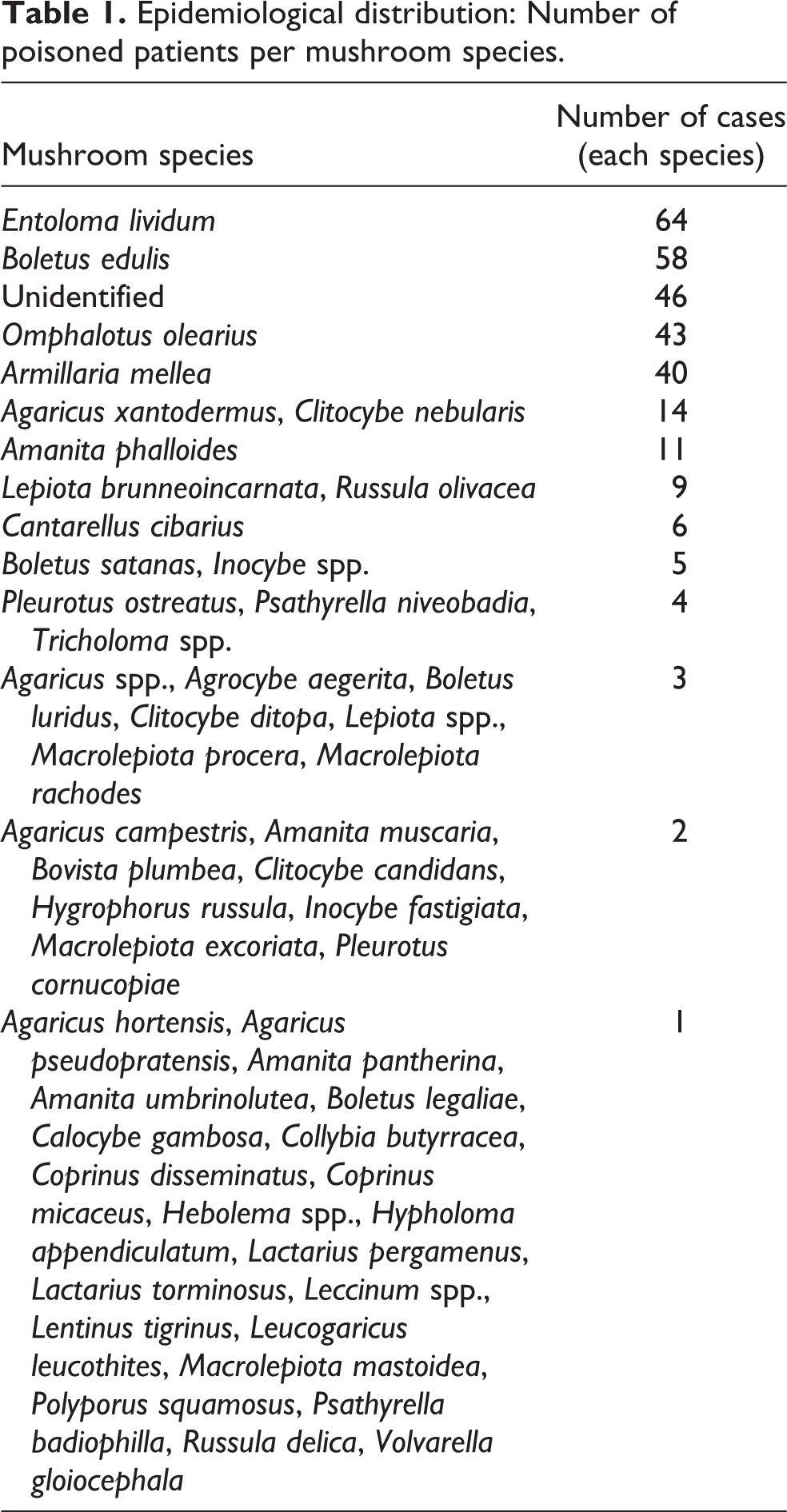
A summary of the species-based epidemiology in our patient sample is shown in Table 1. Interestingly, several cases (49, 11% of the total population) were associated with mixed meal assumption (i.e. more than one species consumed during the same meal), but no case of amatoxin poisoning was found among these. The epidemiology of the mixed cases is described in Table 2.
Epidemiological distribution: Number of poisoned patients per mushroom species.
Epidemiological distribution: Number of poisoned patients per mushroom mixed meal.

Discussion and conclusions
Although mushroom poisoning is less frequent than other forms of intoxication commonly seen in our country, the results of this large retrospective observational study confirm that it still represents a meaningful reason for ED admission. Most cases were found to have a favorable outcome, only presenting with gastrointestinal complaints and needing symptomatic treatments. Nevertheless, early identification and management of potentially life-threatening cases may still be regarded as a challenge for the EPs, mainly for the complex identification of the species and frequent ingestion of mixed meals. Mushroom intoxication sometimes overlaps with pre-existing clinical conditions, leading to clinical dilemmas. 28 The scenario is further complicated by a certain degree of classification uncertainty and several homonymies as well as by the continuous identification of new fungal species, including toxic mushrooms. 18 –25 Therefore, official identification of mushroom species is of pivotal importance. This may allow easy management and discharge of the vast majority of low-toxicity cases, whereas more severe cases may receive strengthened monitoring or more aggressive management. Unfortunately, literature data attest that the rate of correct identification of mushroom species is considerably low, between 5% and 27%. 29 –32 This is mostly attributable to the difficulties in obtaining mycologist’s counseling in many facilities as well as to misleading paucity and vagueness of symptoms, so that the EPs may be discouraged to ask for mycologist consultation. Unlike other healthcare facilities, a 24/365 on-call accessibility to counseling has become available since 1996 in the hospitals of our province, allowing early identification of the vast majority of mushroom species. Notably, the species could be identified in 89.6% cases of poisoned patients in our population, which is the highest rate ever reported in the scientific literature to the best of our knowledge. All the local EPs are encouraged to immediately ask for mycologist counseling in the presence of a suspect mushroom intoxication. Moreover, all available biological samples (remainders of dishes, fresh mushrooms, and gastric content obtained both by vomiting or by gastric lavage) are systematically collected for accurate examination and spore analysis. In cases of delayed-symptom presentation, when biological samples are often unavailable, urine assessment of amatoxin may be useful. 33,34 However, the assay is expensive, not suited for automation, available in a rather limited number of specialized laboratories and so characterized by a rather long turnaround time, often unsuitable for early diagnosis and timely patient management. Therefore, the results of amatoxin testing may be useful for confirming rather than for making an early diagnosis of amatoxin toxicity. 35 Interesting perspective emerges from innovative molecular biology techniques adapted to be used with gastric aspiration fluids or cooked mushrooms, but they are yet not ready for prime time in clinical practice due to the high cost, the need for skilled personnel, and the long turnaround time. 36
As in other studies, we identified a high prevalence of edible mushrooms causing ED presentation. 9,13,32 In agreement with two previous Swiss studies, B. edulis was the most frequent species. 9,32 Cluster presentation accounted for over 60% of cases, a rate slightly higher than that reported in other studies. 32 Notably, all patients of the same cluster complained for similar symptoms. Interestingly, no cluster of amatoxin poisoning was recorded.
The Italian Health Ministry officially advices against mushroom eating for children aged less than 12 years and pregnant women. Despite this, and despite it is widely acknowledged that mushrooms should be avoided in children due to their potential toxicity, we identified 7 cases of poisoning in children aged 1–6 years and 17 in children aged 7–12 years. This evidence reinforced the recommendation that major caution should be paid with children, since they sometimes eat mushrooms grown in the fields and do not communicate their habits to parents, relatives, or teachers. Even more surprisingly, three pregnant women were identified in our case series, who needed to be carefully observed and monitored due to potential fetal toxicity.
Another interesting aspect is the high rate of mixed meals (i.e. 11%). Experts traditionally recommend to classify the onset of symptoms in either less or more than 6 h. 16 Some severe mushroom poisonings, however, may be characterized by the early appearance of gastrointestinal toxicity, which seemingly resolves but is then followed by serious consequences such as liver or renal failure, rhabdomyolysis, or hemolytic anemia. Since 11% of our patients assumed multiple mushroom species, with rather different timing of symptoms onset, this criterion can be misleading and should be no longer proposed, especially when detailed information is unavailable. We strongly believe that in every region in which wild mushrooms are actively harvested and eaten, a service of mycologist counseling should be implemented.
As regards the seasonality, we found only one peak (i.e. late summer and autumn), whereas one previous Swiss study reported two different peaks, a former and small during spring and a latter and larger in autumn. Despite Switzerland is a region close to Italy, slight climatic differences exist as well as some different culinary habits (i.e. Morchella spp., growing during springtime, and sometimes confused with the toxic Gyromitra esculenta, is very appreciated in Switzerland but not in our region) and probably explain the difference between the studies. Due to the concentration of most cases of mushroom poisoning in a limited number of months, a mycologist service on call (when unavailable or unfeasible 24/365) should be implemented during periods characterized by the highest incidence of poisoning, which may obviously differ from one region to another.
The major strengths of our study are the duration of the observational period, extended to over 20 years, the considerable number of cases (i.e. 443), and the remarkable (probably the highest as for current literature data) identification rate of mushroom species. This has allowed a more accurate epidemiological analysis, albeit limited to northern Italy ecology.
Footnotes
Acknowledgements
The authors acknowledge Drs Giovanni Rossi, Gianluca Mezzadri, Pasqualino De Luca, Paolo Ghizzi, Anna Maria Rastelli, Emanuela Mariotti, Caterina Erta, and Vitantonietta Tritto, of the Mycological Consultation Service of the Local Health Agency of Parma, for supporting us in identification of mushroom species during the entire period of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.