
Abstract
Background:
The American Association of Poison Control Center (AAPCC) shows that in 2012 there were 0.3% of human exposures involving mushrooms. Only 17% of 6600 cases were then identified by the species. The present retrospective study was designed to identify the epidemiology of mushroom poisoning in adults admitted to Krakow’s Department of Clinical Toxicology (DCT) from 2002 to 2009.
Materials and Methods:
This study was conducted retrospectively after examining the files of 457 adult patients with wild mushroom poisoning. Mycological analysis was made and the species of the poisoning-inducing mushroom was determined. Furthermore, the circumstances related to the mushroom gathering, transport, storage, preparation, and consumption have been analyzed.
Results:
The analysis revealed that in 400 (87.53%) out of 457 cases, the clinical symptoms were caused by ingestion of identified edible mushroom species. The main reason for edible mushroom poisoning is associated with their incorrect processing after harvest. The analysis of the circumstances of mushroom collection, transport, and storage shows that the largest percentage of poisoning was connected with long-term storage of mushroom dishes, collecting, and storing them in plastic bags, and long storage of mushrooms.
Conclusion:
Based on spore analysis of the gastric content, edible mushrooms were responsible for the great majority of mushroom poisoning cases admitted to the DCT. The toxicity of edible mushroom is associated with proceeding with them during collection, transport, and storage. The medical history should be supplemented by questions concerning these circumstances. The identification of the mushroom by a mycologist is highly desirable.
Introduction
The gathering and consumption of wild mushrooms is a traditional social outing in Europe, Asia, and the United States. 1 –5 Mushrooms were described also as popular remedies in ancient oriental documents, and some of them became ingredients in traditional medicine. 6 The consumption of wild mushrooms is very popular in Poland. An estimated figure of over 10 million Poles participate in mushroom hunts each year, and from 18,000 to 20,000 tons of wild mushrooms are harvested annually, usually for personal consumption. From about 10,000 species of mushroom about 50–100 species are poisonous. 7
It is important to note that the most mushroom-derived toxins poisonous to humans are resistant to cooking, canning, freezing, or any other processing method. Therefore, the only way to avoid poisoning is to avoid consumption of the toxic species. There are no universal clinical care guidelines for the cases of mushroom poisoning. The choice of treatment is guided by the clinical symptoms, and for most mushroom toxins there is no antidote. 8 Modern methods of intensive care medicine have reduced mushroom mortality and morbidity substantially. 1,4 The diagnosis of mushroom poisoning should be based on mushroom identification, clinical features, and laboratory analyses. 9
Mushrooms have numerous spores characteristic for each species. 10,11 The gastric contents, the reminder of a mushroom dish, and the whole mushrooms themselves are subject to evaluation.
Most literature related to mushroom exposures and poisonings are clinical case reports, with few studies characterizing the epidemiology of exposures. 12 Additionally, in medical literature, there are studies investigating exposure to toxic mushrooms and subsequent hospitalizations in the United States 3,12,13 but comparable studies in Europe appear seldom, to our knowledge. 2,9
The observations supported by data in the literature indicated edible species as the most common cause of mushroom poisoning. 2,11 Since edible mushrooms do not have specific toxins, what is the cause of their toxicity? The preliminary study led us to believe that the circumstances of mushroom collection, transport, and storage might be related to the edible mushroom poisonings. 14 The study group consists of wild mushroom-poisoned adult patients admitted to the Department of Clinical Toxicology (DCT), Jagiellonian University Medical College in Krakow, Poland. In each case of mushroom poisoning, the detailed interview concerning the proceeding with mushroom during and after collection, and the mushroom dish was done. 14 The specialist mycologist made a spore analysis of the gastric contents and identified mushroom species. We performed this study to present descriptive epidemiological data on mushroom enquiries to the DCT in Krakow, with particular attention to the circumstances of their collection, transportation, and storage. The results have been compared with literature data. 11
Materials and methods
This study was conducted retrospectively after examining the files of adult (18 years and older) patients with wild mushroom poisoning who were admitted to the DCT from 2002 to 2009. The referral population, in Southeast Poland, amounts to about 7 million people. Demographic and detailed clinical information on exposure cases, circumstances of poisoning, symptoms, and the causality are recorded in a systematic and standardized manner by a physician trained in clinical toxicology. On admission to the DCT, the form concerning the circumstances related to the mushroom gathering, transport, storage, preparation, and consumption was completed. 14 A detailed history was taken from each patient.
The database was reviewed by one doctor specializing in clinical toxicology. The diagnosis of mushroom poisoning was based on the history provided by the patients, symptoms, and physical examination. The laboratory tests conducted included blood analysis namely electrolytes (sodium and potassium), creatinine, glucose, alanine aminotransferase, aspartate aminotransferase, creatine kinase, total bilirubin, blood cell counts (red blood cells, white blood cells, hematocrit, hemoglobin, and platelets), and prothrombin time expressed as the international normalized ratio index. Additionally, when Amanita phalloides poisoning was suspected, urine analysis used for amanitin was conducted. Patients with co-ingestion of drugs in overdose or drugs of abuse, affected by diseases of the digestive system, and subjects treated with medicine that might affect gastrointestinal function were not enrolled. Febrile patients were excluded from the study because of infection suspicion, which could be responsible for reported complaints. In all of the included cases, the specialist mycologist made a spore analysis of the gastric contents. Microscopic examination of the gastric contents is aimed at determining the presence of spores and spore identification. The species of the poison-inducing mushroom was determined in all included cases.
Spore analysis was made with the use of a light microscope (type Olympus BX 50-F, Japan). Two microscopic specimens were made, one stained with Lugol’s solution, while the other one was not stained. The spores were evaluated at a magnification of ×400. The spores that were found were identified using atlases and then compared with the model spores—specimens of spores of a specific mushroom species. The spore models were obtained from mushrooms collected and identified by a specialist mycologist. The dried model sporocarps of mushrooms, containing spores, were stored in sealed containers. The preparation of the model spores was conducted at the same time as the mycological analysis of spores obtained from a poisoned patient. All the preparations were stained in the same way.
The results were compared with data that referred the mushroom species responsible for poisoning from the Regional Centre of Acute Poisoning in Sosnowiec (RCAPS), Southwest Poland, with 10 million population.
11
The same methods of spore analysis were used by RCAPS. The statistical analysis was performed using the STATISTICA data analysis software system, version 10 (StatSoft. Inc. 2011). We calculated the percentage
Results
We identified 457 patients poisoned by wild mushrooms (mean age 43.81 ± 18.53 years; 62.8% female) during the study period, among a total of 18,043 poisoning cases, where the frequency of wild mushroom poisoning was 2.53%. Apart from mushrooms that contain psychoactive toxins, the ingestion of toxic mushrooms was accidental and caused by misidentification of species. August, September, and October were the peak months for mushroom poisoning (Figure 1), and these months are generally warm and rainy.
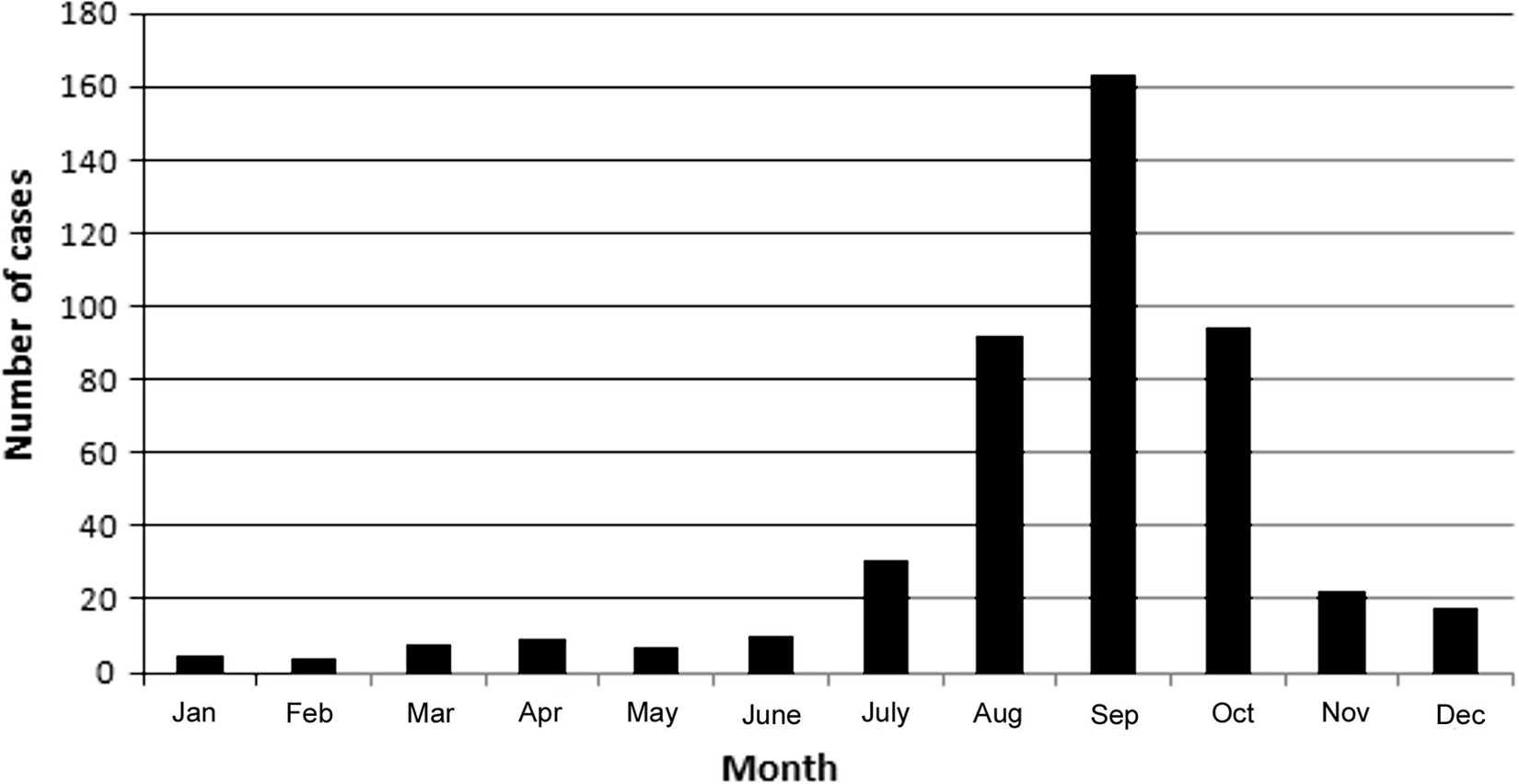
Monthly variation for cases of mushroom poisoning reported to the Department of Clinical Toxicology in the years 2002–2009.
In 400 (
Poisoning caused by different species of mushrooms (edible and toxic) observed by the DCT in the years 2002–2009.

DCT: Department of Clinical Toxicology in Krakow. N: number of poisoning; p: percentages of poisoning [%] of the total poisoning caused by both, edible and toxic species; n = 457 total cases of poisoning.
The results of the mycological analysis are reported in Table 1. These analyses were carried out among patients of DCT in the years 2002–2009. It was shown that the incidences of poisonings were caused by both edible and toxic species of mushrooms. Statistically significant differences existed between the percentages of poisoning caused by different mushroom species (value of the Fisher–Snedecor statistics F = 8.74, critical value of the Fisher–Snedecor statistics F
αν1ν2 = 1.614, where α = 0.05 is significance level and ν
1 = 18 and ν
2 = ∞ are degrees of freedom). Poisoning caused by edible species of mushrooms represented as much as 400 (
The mushroom gaining method used by poisoned patients of the DCT in the years 2002–2009.

DCT: Department of Clinical Toxicology in Krakow. N: number of poisoning; p: percentage of the mushrooms gaining methods used by poisoned patients by edible species only [%]; n = 400 of the total poisoning cases caused by edible species.
The data concerning the circumstances of collection, transport, and storage of mushrooms as well as storage of mushroom dishes are presented in Table 3. The analysis revealed that the percentages of the long-term storage of mushroom dishes (
Poisoning caused by edible mushroom species depends on circumstances of mushroom collection, transport, and storage.

N: number of poisoning, p: percentage of circumstances of mushrooms collection, transport and storage [%], n = 400 of the total poisoning cases caused by edible species.
In Table 4, the data on the occurrence of poisoning caused by mushrooms as recorded by the DCT in Krakow was compared to those recorded by the RCAPS.
11
The percentage of poisoning caused by edible mushrooms recorded in the years 2003–2007 by the RCAPS (
Comparison of the poisoning caused by both edible and toxic mushroom species recorded by the DCT in Krakow and The Regional Center of Acute Poisoning, Sosnowiec.

N: number of poisoning; p: percentage of poisoning; n1 = 457 and n2 = 320 of the total poisoning cases (caused by both edible and toxic species) in Krakow and Sosnowiec respectively.
Discussion
In the case of mushroom poisoning an important diagnostic factor is the interval between the intake of the dish and the occurrence of manifestations from the gastrointestinal tract. Hepatotoxic mushrooms, for example, the A. phalloides group, trigger initial gastrointestinal symptoms after ≥6 h. An appropriate account of this history of this taken from the patient is also extremely important. Early diagnosis and the identification of the mushroom species are of substantial prognostic significance. 1,4 A lack of mushroom identification may complicate the management of the poisoned patient. 2 Unfortunately, in most cases, mycological analysis is impossible to provide immediately. As such, mushroom identification cannot delay the treatment. When interviewing patients suspected of mushroom poisoning, a detailed history concerning the ingestion should be obtained. The mushroom ingested is often difficult to identify, and the actual ingested mushroom is usually not available for examination. Attempts made to use systems for electronic identification based on reported characteristics have likewise been unsuccessful. 3 If whole mushrooms or mushroom fragments are available, they should be saved for identification by an experienced mycologist.
The latest annual report from the American Association of Poison Control Center (AAPCC) showed 6600 cases of exposure to mushrooms in 2012, but only 17% were identified by the species. 15 Mushroom identification requires specialist expertise and is beyond the capabilities of health care professionals. The use of a method such as the Internet for the purpose of mushroom identification is wholly inadequate for untrained personnel. Incorrect identification could potentially impact on patient care. 9 Also the verbal descriptions of mushrooms are subjective because the mushroom morphology can differ depending on the season, the stage of growth, local habitat, and environmental conditions. 9,13 Photographic images are useful, but they are not a substitute for formal identification using actual specimens when such material is available. 9
Analysis of mushroom spores detected in gastrointestinal contents allows for the determination of the mushroom species that may have caused the poisoning before any changes occur in other diagnostic parameters. The type of investigated material is also an important factor that can determine the validity of such studies. The highest importance is ascribed to samples of gastrointestinal contents rich in non digested food, when collected in the initial hours of poisoning. These include vomit and secured remnants of uneaten food and mushroom peelings. Such materials include entire fragments of sporocarps, which, when examined macroscopically and microscopically, reveal the morphological properties allowing prompt identification of the genus. Microscopic examination of the above materials is aimed at determining the presence of spores and spore identification via comparison with standard fungal spores.
Our results describe the epidemiology of wild mushroom poisoning in the years 2002–2009 in Southeast Poland. In this study, we show that inquiries regarding mushroom poisoning amount to a relatively infrequent 2.53% reason for contacting the DCT in Krakow. Wild mushroom poisonings commonly occurred in autumn and summer, corresponding with the mushroom season in Poland (Figure 1).
The biggest percentage of poisoning was connected with independent mushroom collection (Table 2). The suspicion of toxic mushroom species as a causative agent of poisoning seems obvious. However, our results show that the biggest percentage of poisoning is caused by edible species (Table 1). The relationship between poisoning percentages caused by toxic and edible species was similar in the RCAPS data (Table 4).
The analysis of the circumstances of mushroom collection, transport, and storage shows that the largest percentage of poisoning was caused by long-term storage of mushroom dishes, collecting and storing in plastic bags, and long storage of mushrooms (Table 3). It should be emphasized that the main reason for edible mushroom poisoning is due to their incorrect processing after harvest (Table 3).
There are some reports of mushroom poisoning from different parts of the world. 2,7,9,11,12,13 Poisoning in the majority of cases was not serious from a clinical aspect. The most common symptoms were nausea, vomiting, abdominal pain, and diarrhea. The mainstay of therapy was symptomatic and supportive. Unfortunately, in most cases, it was not possible to determine the type of mushroom ingested by the patients, but some of them were edible species. 2,11
The mushrooms contain choline, which as a result of autolysis transforms to toxic neurine (vinyl-trimethyl-ammonium hydroxide CH2=CHN(CH3)3 OH). 16 The vomiting principles in an animal model of Rhodophyllus rhodopolius poisoning were connected with large amounts of choline, muscarine, and muscaridine. 17 Scientific studies on neurine are few—with the most recent dating back to the mid-1950s. Neurine possesses muscarinic (M1) and nicotinic receptors’ agonist property. 18
Edible mushroom species are known to have factors that could lead to a health disorder. Repeated meals, large amounts ingested, incorrect preparation, and ingestion of raw mushrooms may lead to severe symptoms. 2,9,12 Gastroenteritis can be induced by edible mushroom species containing large amounts of mucus; for example, the sticky bum, S. luteus, and fragments of this mushroom can remain in the stomach even for 3 days while manifesting symptoms of gastritis. 19 The gastrointestinal disturbances may result from the low activity of trehalase in the small intestine mucosa. Trehalase is a glycoside hydrolase enzyme which catalyses the conversion of trehalose to glucose. 20
The results of our observations indicate additional, but so far not yet described, factors. As indicated in the patient form, 14 the fruit bodies of these mushrooms were mechanically damaged during transportation or were stored 2 days or more prior to consumption.
Our study included 457 patients diagnosed with mushroom poisoning based on the history provided by the patients, symptoms, physical examination, and laboratory tests. The analysis revealed that 12.47% of the patients were poisoned with mushrooms containing specific toxins such as cyclopeptides, muscarine, psilocybin, muscimol/ibotenic acid, and gastrointestinal irritants (Table 1). In 87.53% of the patients, nausea, vomiting, stomach ache or diarrhoea occurred within 30 min to 4 h after the ingestion of the edible mushrooms. Laboratory testing did not show any significant abnormalities. The edible species that induced poisoning most frequently were the honey mushroom, the parasol mushroom, the sticky bum, the chanterelle, and the field mushroom (Table 1). The results of the epidemiological data, from RCAPS, indicated that the most frequent cases of poisoning were caused by edible mushrooms, with usually little effect. 11 The same method for mushroom identification was used by us and RCAPS enabling comparison of the data with our results. Unfortunately, detailed medical history concerning mushroom collection, transport, and storage and proceeding with mushroom dish were not conducted in RCAPS.
The main limitation of the study is its retrospective character. The DCT is a tertiary referral centre. In some cases, when the species of mushrooms were known and the course of poisoning mild, patients were treated in different hospitals in our region. This accounts for the selection bias in this study. Moreover pernicious vomiting causes the stomach to empty, leading to the gastric contents being poor in spores. This resulted in spore identification being impossible in 38 cases. The pediatric cases of mushroom poisoning were not analyzed, thus significantly impoverishing the study.
Conclusions
Based on spore analysis of the gastric content, edible mushrooms were responsible for the great majority of mushroom poisoning cases admitted to the DCT. The toxicity of edible mushroom is associated with proceeding with them during collection, transport, and storage. The medical history should be supplemented by questions concerning these circumstances. The identification of the mushroom by a mycologist is highly desirable.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.