
Abstract
Context:
Cardiac dysfunction is one of the most serious consequences of scorpion envenomation. The best tool to evaluate cardiac function is echocardiography, but it is not available at all emergency departments. Many studies aimed to describe biological predictive factors of cardiac dysfunction in scorpion envenomation. Troponin is one of these biomarkers but its correlation with myocarditis is not well established. The aim of this study was to evaluate correlation between troponin levels and cardiac dysfunction in moderate scorpion envenomation.
Methods:
A retrospective monocentric study including patients admitted in the emergency department for moderate scorpion envenomation with troponin measurement during their early management. On arrival, an electrocardiogram and a chest X-ray were realized for all patients.
Results:
We enrolled 132 patients with a mean age at 31.3 ± 24.4 years and a 1.35 sex-ratio. All patients had moderate systemic manifestations. There were 28 patients with clinical manifestations of cardiac dysfunction without life-threatening troubles (21.2%). Troponin was undetectable in 69 patients (56%). The mean value of troponin level (pg/ml) was higher in patients with clinical manifestations of left ventricular dysfunction (1.80 ± 3.8 vs. 0.11 ± 0.5; p = 0.02). Troponin levels were significantly higher in patients with positive T wave on electrocardiogram.
Conclusion:
In patients with moderate scorpion envenomation with positive T wave, high values of troponin suggest the presence of cardiac dysfunction.
Introduction
Cardiac dysfunction is one of the most serious consequences of scorpion envenomation. 1 –3 Scorpion stings are still a serious public health problem in North Africa and many other tropical or subtropical regions around the world. The clinical manifestations include pain, vomiting, nausea, sweating, and/or arterial hypertension. Severe forms are mainly characterized by cardiopulmonary complications such as pulmonary edema and/or cardiogenic shock. 4 However, respiratory manifestations can exist despite the absence of cardiac dysfunction. 5,6 To improve prognosis of these patients, it is important to early detect signs of cardiac dysfunction at the emergency department (ED).
Electrocardiographic abnormalities were described in scorpion-envenomed patients. Sinus tachycardia is the most frequent abnormality but these signs lack sensitivity and specificity. 2 Echocardiography is the best tool to detect cardiac dysfunction in scorpion envenomation. 7 –11 However, it is not available in all EDs, especially in developing countries. Nowadays, troponin measurement is routinely done as a cardiac injury biomarker at EDs. Physicians’ decisions are guided by the baseline troponin level or its kinetic in serial measurements. Nevertheless, cut-off predicting cardiac dysfunction in scorpion-envenomed patients is still not well studied. 12 For this reason, we conducted this study to evaluate whether troponin level elevation correlates with evidences of acute myocarditis in scorpion stung patients.
Methods
Clinical setting
This is a retrospective study conducted over a period of 3 years (from January 1, 2013, to December 31, 2015). The study population consisted of consecutive patients admitted for scorpion envenomation at the ED of Habib Bourguiba University Hospital, in Sfax, which is the unique surgical academic facility in the south of Tunisia. Patients with life-threatening pathologies or requiring continuous monitoring are admitted in the emergency room (ER), a 10-bed unit where monitors and trained caregivers are available. Because of the lack of echocardiography in our department, patients requiring heart exploration are referred to the Cardiology Department of Hedi Chaker Hospital in Sfax.
Inclusion criteria
All patients admitted at the ER for moderate envenomation were included (stage 2) 13,14 at the first clinical examination, with troponin measurement on admission or during their management at ED. Cases without any measurement of troponin at ED were excluded. Severe cases (stage 3) at the first evaluation were excluded. In our department, a daily evaluation is performed by expert staff. The diagnosis of cardiac dysfunction was retained on clinical, biological, and/or radiological manifestations. Scorpion stung patients without cardiac dysfunction on admission, who exhibited signs of heart failure, were diagnosed during ER stay. We compared the group of patients who had no heart dysfunction during their observation at ER and those who exhibited signs of heart failure.
Patient management at ED
In our region, there are three main species of scorpions: Androctonus australis, Buthus occitanus, and Androctonus aeneas. 15,16 Following a scorpion sting, admission at ED is decided if there are any systemic abnormalities. Stage 2 of severity is retained if there are no severe troubles and stage 3 of severity is defined by the presence of at least one life-threatening systemic manifestation. 14
All patients underwent electrocardiogram, chest X-ray, and troponin I measurement on admission. During their surveillance in the ER, myocarditis is suspected each time there are troubles in respiratory status (dyspnea, hypoxia, X-ray signs of acute pulmonary edema) or in hemodynamic status (pulmonary edema, electrocardiogram abnormalities, shock). In our hospital, a troponin I level less than 0.01 pg/ml is considered to be undetectable. In patients with suspected myocarditis, echocardiography was performed—by the same physician—at the Cardiology Department of Hedi Chaker Hospital as soon as it was possible.
Statistical analysis
Data are expressed as numbers and rates. Descriptive statistics were used to illustrate subjects’ demographic characteristics. Comparison of characteristics of the two groups was performed by the χ 2 test or Fischer’s exact test as appropriate. Continuous variables were expressed as means ± standard deviation and the subgroups were compared by Student’s t-test. Risk factors were evaluated in univariate analysis for compared data. A p value less than 0.05 was considered as statistically significant.
Results
We enrolled 132 patients from 320 admissions for scorpion envenomation. Most patients (67.2%) were admitted to ED more than 2 h after a scorpion sting. The most observed scorpion specie was A. australis (56.1%).
Table 1 shows clinical manifestations recorded of all included population group. On admission, all of the patients had minor systemic signs and were at stage 2 of scorpion envenomation. There were 28 patients who developed clinical manifestations of cardiac dysfunction (21.2%) during their management at ED (Table 1). Twenty of these patients have had chest X-ray signs of pulmonary edema (15.2%).
Demographic and clinical data.

SD: standard deviation.
Troponin measurement was done during the first 4 h of envenomation in 43 patients (32.6%). Serum troponin increased only by the 60th min after sting. It was undetectable in 74 patients (56%). The value of troponin level varied between 0.02 pg/ml and 13.80 pg/ml on admission (Figure 1). Troponin measurement was redone for 23 patients having electrocardiogram (ECG) modifications, chest pain, or worsening respiratory status. It showed an increase in 21 cases (91.3%), while it was undetectable in the two remaining cases (Figure 2). The first troponin level/second troponin level ratio ranged between 0.4 and 662 with a mean value at 55.70 ± 157.30. The mean value of troponin level was higher in patients with clinical manifestations of left ventricular dysfunction (1.80 ± 3.80 vs. 0.11 ± 0.50; p = 0.02).

Troponin values at the first measurement (pg/ml).
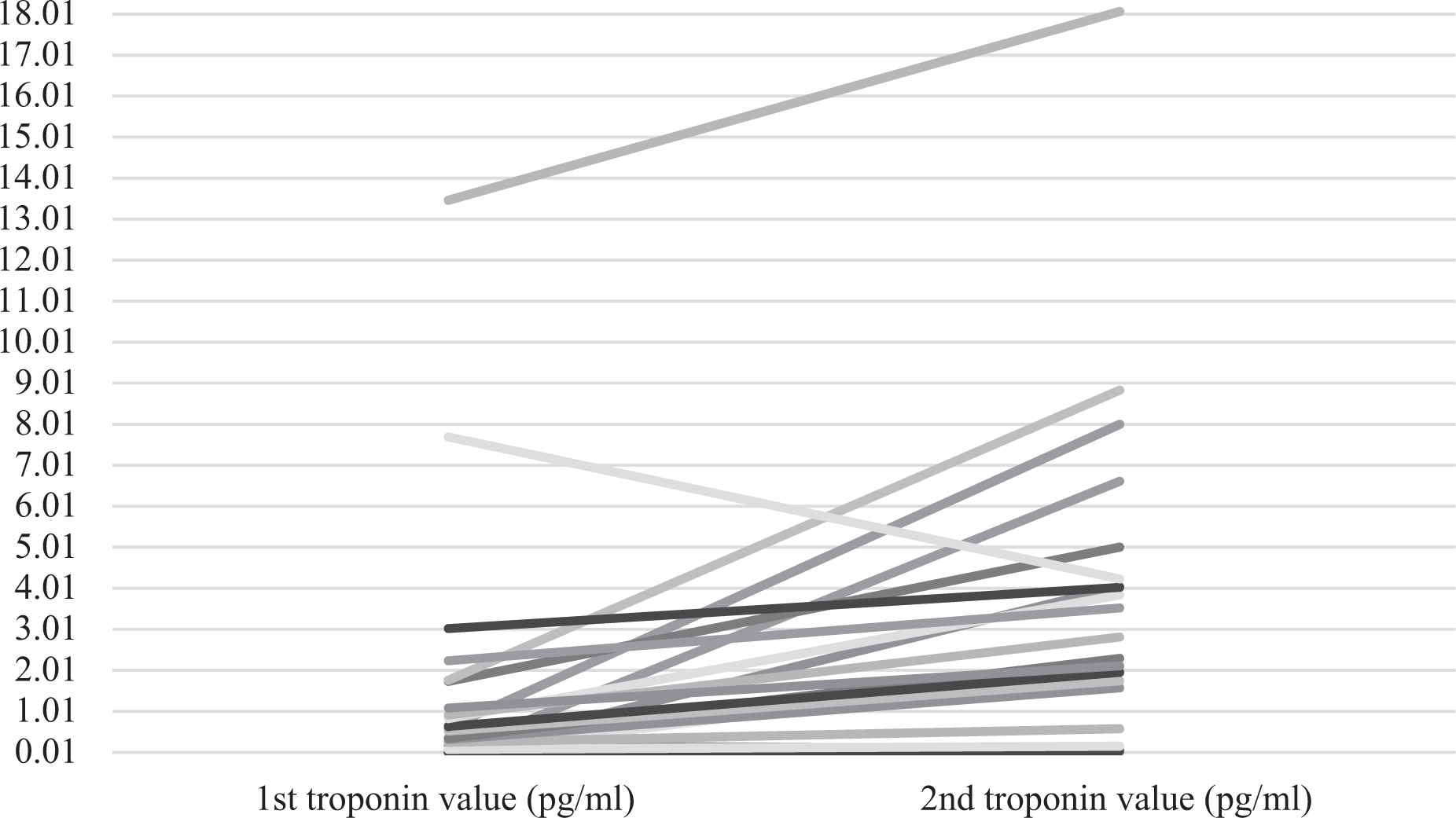
Trends of troponin values between the first and the second measurement.
An echocardiography was performed during the first 24 h of admission for 18 patients having clinical signs of left ventricular failure, confirmed in only 11 patients. In this subgroup, the baseline troponin level was positive in 77.7% of cases (14/18 patients). The four patients with an undetectable troponin on admission had an increase of troponin level at the second measurement with a ratio varying between 1.3 times and 662 times.
No patient had to be intubated, but dobutamine was administered to 18 patients. One hundred and nine patients were discharged within 24 h after hospitalization. Only one patient (0.7%) was referred to intensive care unit and was discharged 3 days later. Twelve patients (9.1%) were transferred to the cardiology department and 10 patients (7.6%) to the pediatric ward.
Troponin levels were significantly higher in patients suffering from dyspnea, vomiting, excitation, or sweating (Table 2). There was no correlation with clinical examination abnormalities (cardiac or pulmonary auscultation) or chest X-ray signs of pulmonary edema. However, there was a high correlation between positive T wave on electrocardiogram, low left ventricular ejection fraction on echocardiography, and the need of oxygen or dobutamine to stabilize respiratory status (Table 2). Only one patient (0.7%) had elevated troponin levels with no evidence of myocarditis on echocardiography. Cut-off of troponin level predicting myocarditis on echocardiography was at 0.03 pg/ml (Figure 1).
Correlation between troponin levels and myocarditis signs after scorpion envenomation.

SD: standard deviation; ED: emergency department.
Discussion
Our results show that in patients with moderate scorpion envenomation with positive T wave, high values of troponin suggest the presence of cardiac dysfunction.
Cardiac dysfunction is still the leading cause of mortality in scorpion stung patients. Its mechanisms are complex and are still being debated. Mainly three hypotheses explain cardiac dysfunction after a scorpion sting. It is linked to massive release of catecholamines, 17 direct effect of scorpion venom on myocardial fibers, 18 and myocardial ischemia. 1,2,16,19,20 Early diagnosis of cardiac dysfunction is extremely important in decision-making concerning therapeutic management and time of discharge from emergency department.
In fact, management of moderate scorpion-envenomed patients is mainly conducted at EDs and is still controversial as these patients have systemic manifestations with no life-threatening signs. In typical cases, cardiac dysfunction can be missed by clinical examination. However, in some situations (i.e. borderline cases with tachypnea and/or bronchial hypersecretion), clinical examination fails to confirm or infirm the diagnosis of heart dysfunction. In such a situation, many complementary tools are required to retain the diagnosis of heart failure. Therefore, biological markers can help in the early detection of myocardial injury, and thus, in the decision about appropriate management. 21,22
Many studies have shown a significant correlation between elevated troponin levels and signs of cardiac injury due to myocardial infarction, chest trauma, myocarditis, and so on. 2,4 –6,23 In these situations, physicians’ decisions are guided by the baseline troponin level or the rise of levels in serial measurements.
On the other hand, and to our best knowledge, there are few studies exploring the value of troponin levels in scorpion-envenomed patients. Moreover, cut-off predicting cardiac dysfunction in scorpion envenomed patients is still not well studied. Consequently, it is important to define it because elevated serum levels of troponin do not necessarily indicate myocardial injury.
In fact, scorpion envenomation can be associated with systemic inflammatory response syndrome which is proved to be associated with significant rise of troponin. 19,24
The first study which provided evidence of correlation between high levels of troponin on admission and myocardial injury in scorpion envenomation was realized in 2003 by Meki et al. 25 In this study, the authors found a 100% specificity and sensitivity of high levels of troponin for diagnosis of myocardial injury in relation to echography finding in the envenomed victims. Serum troponin I levels in moderate cases were at 1.03 ± 0.25 ng/ml compared to 4.73 ± 0.76 ng/ml in severe cases (p < 0.005). In this study, a troponin cut-off value of 1ng/ml was significantly associated with cardiac dysfunction. Sagarad et al. found a mean level of troponin at 2.30 ± mcg/l among patients having a low ventricular ejection function with a cut-off value of 0.11 ng/ml. 6 In our study, the troponin level predicting myocardial injury was at 0.03 mcg/l with an 87% sensitivity and a 71% specificity. Moreover, we found a good correlation between positive T waves and high level of troponin.
Timing of serum troponin measurement is also important to determine. 25,26 Indeed, Sofer et al. 26 showed that troponin level on arrival was not predictive of cardiac dysfunction. Cupo and Hering. 2 found a detectable troponin among patients arriving more than 3 h after scorpion envenomation with normalization within 4–5 days. In an animal experimental research, Elatrous et al. found that serum troponin increased only by the 120th min median (10 ng/ml compared to 0.2 at baseline). 12 In our study, troponin levels increased within 1 h after the sting.
Echocardiography is the best tool in detecting myocarditis even if delay between envenomation and arrival to ED is short. If not feasible, serum troponin elevation seems to be correlated with myocarditis in scorpion envenomation.
Although our research is one of the rare studies exploring the value of troponin in positive diagnosis of cardiac dysfunction following scorpion envenomation, we must mention that some methodological concerns are to consider. First, the small size of our sample limits the generalization of the results. However, it is worth mentioning that our sample is larger than previous published samples. 25,4
Second, the included patients are those who had had troponin measurement on admission, and we have no idea why it was done. In fact, we cannot exclude that there were probably other clinical manifestations predicting heart dysfunction that were not reported in medical files.
The third limit is the retrospective gathering of data. As a consequence, clinical manifestations were recorded by several physicians and we cannot exclude the overlooking of several clinical manifestations in some patients.
Finally, the lack of patient follow-up after discharge can represent in itself a study limitation.
Conclusion
This study shows that troponin measurement in severe scorpion-envenomed patients can represent a reliable tool in the detection of cardiac dysfunction. To enhance our results, further prospective studies should be interesting to realize using this cut-off of troponin level with a follow-up after discharge.
Footnotes
Acknowledgements
All authors thank Professor Chokri Khalaf for his help in the redaction of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.