
Abstract
To evaluate effects of halofuginone (H) on radiation-induced lung injury (RILI), 60 rats were divided into six groups: Group (G) 1 control, G2 radiotherapy (RT) only, G3 and G4 2. 5 and 5 μg H and G5 and G6 RT + 2.5 and 5 μg H groups, respectively. A single dose of 12 Gy RT was given to both lungs. H was applied intraperitoneally with daily doses, until animals were killed at 6 and 16 weeks after RT. At 6th and 16th weeks of RT, five rats from each group were killed. Lung tissues were dissected for light and electron microscopy. Chronic inflammation, fibrosis and transforming growth factor-beta (TGF)-β scores of all study groups were significantly different at 6th and 16th week (p < 0.001). Chronic inflammation, fibrosis and TGF-β scores of G2 were higher than G5 and G6 at 6th and 16th weeks of RT. At 16th week, fibrosis and TGF-β scores of G5 were higher than G6 (p = 0.040 and 0.028, respectively). Electron microscopical findings also supported these results. Therefore, H may ameliorate RILI. The effect of the H was more prominent at higher dose and after long-term follow-up. These findings should be clarified with further studies.
Introduction
The lung is one of the most sensitive organs to ionizing radiation, and damage to normal lung tissue remains a major dose-limiting factor for patients receiving radiation to the thorax. 1,2 Radiation-induced lung injury (RILI), which is also named as ‘radiation pneumonopathy’, is a continuous process and regarded as the result of an abnormal healing response. Subclinical early damage in pneumocytes type I progress to an acute interstitial inflammation at 6–12 weeks after the onset of radiotherapy (RT) and further to lung fibrosis after many months and years. Inflammation is an essential part of the normal wound-healing process. 1,3 Clinically, RILI is typically divided into two phases: pneumonitis and fibrosis. The fibrotic phase tends to manifest >3 months after treatment. Fibrosis is part of the wound-healing process. Therefore, radiation fibrosis is a form of chronic lung damage that usually evolves over 4–24 months after irradiation. 3
The alveolar epithelium consists of type I and type II epithelial cells. Type I cells cover approximately 90% of the alveolar surface and type II cells are the precursors of type I cells. In steady state, the turnover time of the alveolar epithelium is approximately 4–5 weeks. However, after toxic injury, type I epithelial cells are denuded and the proliferation of type II cells is stimulated up to 10-fold. 4 Stimulation of type II cells promotes the secretion of growth factors and proteases and degradation of the extracellular matrix to allow removal of dead cells by normal processes. 3 Pulmonary irradiation also reduces microvessel density and lung perfusion and promotes hypoxia. 5 All of these injuries stimulate the recruitment of a variety of inflammatory cells to the site of the injury and it leads to establishment of chronic inflammation and fibrosis. In this phase, vascular damage and collagen deposition become apparent. Vascular injury and activation of coagulation cascade, cellular adhesion molecules, pro-inflammatory and profibrotic cytokines and oxidative stress seem to play a vital role in the development of radiation fibrosis. 6 Transforming growth factor-beta 1 (TGF-β1) plays an integral role in fibrosis formation by promoting the chemoattraction of fibroblasts and their conversion to myofibroblasts. 1
Halofuginone (H) is a low molecular weight plant-derived alkaloid isolated from the Dichroa febrifuga plant that exhibits antifibrotic activity and inhibition of type I collagen synthesis. 7 As fibrosis is the result of an increase in type 1 collagen, it is assumed that selective inhibition of type 1 collagen synthesis may inhibit formation of fibrosis without affecting tissue structure in female mice. 8 This study was designed to determine whether H treatment would inhibit TGF-β signalling pathway and ameliorate the radiation-induced lung fibrosis. We compared two different doses of H, as 2.5 μ/day and 5 μ/day, in order to compare the efficacy of different doses on radiation-induced pulmonary fibrosis.
Methods and materials
Study design
The study included 60 adult female Wistar–Albino rats (250–300 g), the use of which was approved by the Selcuk University Animal Care and Use Committee. Animals were housed four per cage in a controlled animal holding room with a 12/12-h light/dark cycle; temperature and relative humidity were continually monitored to provide standard laboratory conditions. Food and water were provided ad libitum. The 60 female Wistar rats included in the study were randomly grouped into six groups containing 10 rats each: G1 was defined as control group in which the rats were sham irradiated. G2 was the radiation-only group receiving a single dose of RT (12 Gy) but no medication. G3 and G4 were 2.5 μg and 5 μg H groups and rats in these groups were given H (Collgard Biopharmaceuticals Ltd, Petah Tikva, Israel) in a single dose of 2.5 μg and 5 μg daily intraperitoneal injection for 16 weeks, respectively. G5 and G6 were defined as 2.5 μg H + RT and 5 μg H + RT groups and rats in these groups were given H in a single dose of 2.5 μg and 5 μg daily intraperitoneal injection for 16 weeks, starting immediately after administration of 12 Gy single dose RT (Table 1). The rats from G1 and G2 were given sodium chloride (NaCl) intraperitoneally in the same timing procedure with H groups (G3, G4, G5 and G6).
The abbreviations used for the study groups.

H: halofuginone.
Irradiation protocol
RT was applied under general anaesthesia with intraperitoneally administered 90 mg/kg ketamine hydrochloride and 10 mg/kg xyalazine. A single dose of 12 Gy that has been shown to lead lung fibrosis 9 with 6 MV photon beams was applied via a single anterior field to 2 cm depth with source-axis distance technique; 1 cm elasto-gel bolus was used to build-up the radiation dose on the lungs and to provide contour regularity. The field size was 4 × 4 cm2 and included the both lungs.
H protocol
H is in crystalline form. Crystalline H was dissolved in a 0.44 M, pH 4.3 lactic acid tampon and stock solutions of 1–2 mg/ml were prepared and stored at 4°C at which it could remain stable for at least 4 months. Study solutions for injection were prepared by diluting the stock solutions daily using 0.9% NaCl (0.1 mg/1 ml). The study solutions were used within 1 h following preparation.
Morphologic studies
At the 6th and 16th weeks of the RT, five animals from each group were killed for morphological examination. The animals were anaesthetized and killed by cervical dislocation, and both lungs were removed from the chests of the animals.
Histopathologic evaluation
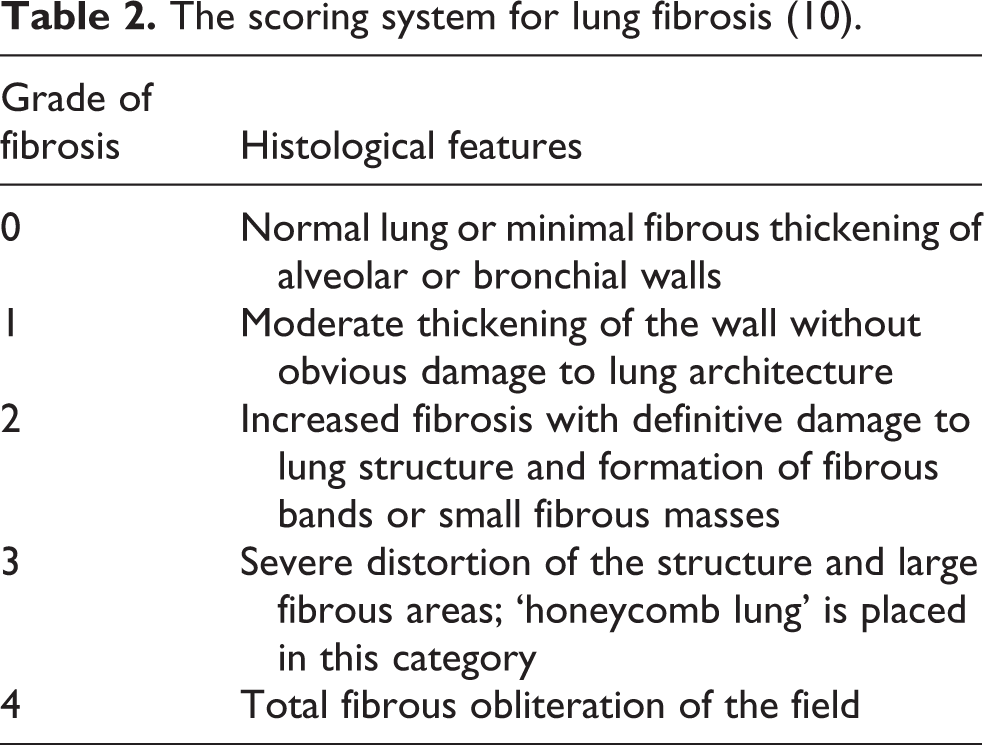
The bilateral whole lungs of each rat were excised and fixed in 10% neutral buffered formalin. Two lobes of each lung for each rat were processed and embedded in paraffin for light microscopic examination. The 4-µm thick sections obtained with microtome were stained with haematoxylin and eosin to evaluate the inflammation and with histochemical Masson’s trichrome staining to identify the fibrosis in the lung. Extend of the chronic inflammatory cells including lymphocytes on alveolar walls was graded on a scale of 0 (normal) to 3 (severe). Fibrosis was defined as the thickened alveolar walls with superimposed collagen. As a quantitative end point, extend of the radiation induced fibrosis was graded on a scale of 0 (normal lung or minimal fibrous thickening) to 4 (total fibrous obliteration of the field), as described in Table 2. 10 The pathologist was not aware of the treatment groups at the time of the histological examination of the specimens. After examining the whole sections for each rat, the average value of fibrosis and chronic inflammation per rat was taken as the fibrosis and inflammation scores and mean values of each group were calculated.
The scoring system for lung fibrosis (10).
Immunohistochemistry staining and scoring procedure
Paraffin-embedded tissues of chosen slides were collected, and 4 µm thick sections were prepared for immunohistochemistry. The sections were deparaffinized at 37°C oven overnight. Immunohistochemical staining was performed using an automatic staining machine (Ventana, Benchmark XT, France). The sections were boiled at sodium citrate buffer at 95°C for 60 min and then incubated with primary antibody anti TGF-β rabbit polyclonal antibody (ABCAM, ab92486, Cambridge, UK) at a dilution of 1:100 for 52 min. The sections were incubated with the secondary antibody for 20 min at room temperature, incubated with Ultra I-view detection kit (Roche Diagnostics Ltd, UK) and counterstained with haematoxylin for 8 min.
The immunohistochemical TGF-β-stained slides were evaluated and scored by a single pathologist blinded to patients’ data. On light microscopic evaluation of each 4 µm thick section, 10 different fields magnified 100× were reviewed. Immuno-reactivity scoring system, which was previously described by Wang et al., 11 was used to determine TGF-β expression levels. This system depends on multiplication of staining intensity and TGF-β-positive alveolar cell percentage. The percentage of positive cells was scored as 0, negative; 1, 1–25%; 2, 26–50%; 3, 51–75%; and 4, 76–100% and the staining intensity as 0 (−), 1 (+), 2 (++) and 3 (+++).
Ultrastructural evaluation with electron microscopy
The tissue samples that were taken from the animals at 6th and 16th weeks after RT were put into 2.5% gluteraldehyde for 24 h for primary fixation. The same application was done to the rats of the H and control groups after the administration of the drug or NaCl in the same timing procedure. Then, these samples were washed with Sorenson’s phosphate buffer solution (pH: 7.4) and they were postfixed in 1% osmium tetroxide. After postfixation, they were washed with the same buffer and dehydrated in increasing concentrations of alcohol series. After dehydration, the tissues were washed with propylene oxide and embedded in epoxy resin embedding media. The semi-thin and ultra-thin sections of the obtained tissue blocks were cut with an ultramicrotome (LKB Nova, Sweden). These semi-thin sections, which were 2 µm in thickness, were stained with methylene blue and examined under a light microscope (Nikon, Japan). Following this procedure, trimming was done to the tissue blocks and their ultra-thin sections which were about 60 nm in thickness were taken by the same ultramicrotome. These ultra-thin sections were stained with uranyl acetate and lead citrate and they were examined under Jeol JEM 1200 EX (Japan) transmission electron microscope. The electron micrographs of the specimens were taken by the same microscope.
Statistical method
The statistical package for social sciences (SPSS) v. 13.0 was used for statistical analyses. As the pathological scores were ordinal in nature, the differences in pathological findings between the study groups were analysed using the Kruskal–Wallis test. When an overall statistically significant difference was observed, pairwise comparisons were performed using the Mann–Whitney U test. Bonferroni correction was used for multiple comparisons. A 5% type-I error level was used for the statistical significance cut-off for overall comparisons. p < 0.05 was considered for statistical significance level.
Results
Histopathological and immunohistochemical findings
In the control group, histological sections of the rats’ lung exhibited alveolar structures surrounded by the dense capillary nets. Alveoli were separated from each other by thin alveolar septum and covered by the layer of epithelial cells. The chronic inflammation, fibrosis and TGF-β scores between study groups were significantly different at sixth week of RT (p < 0.001 for all; Table 3). All of the scores were higher in RT groups (G2, G5 and G6) than non-RT (G1, G3 and G4). When non-RT groups compared with respect to the inflammation, fibrosis and TGF-β scores at sixth week of RT, Mann–Whitney U test revealed that there weren’t any significant difference between the groups. On the other hand, the inflammation, fibrosis and TGF-β scores of RT-only group were higher than both RT + 2.5 μg H group and RT + 5 μg H group (p values were 0.001 and <0.001 for inflammation; <0.001 and <0.001 for fibrosis and <0.001 and <0.001 for TGF-β scores, respectively). When RT + H groups (either 2.5 μg or 5 μg) compared there weren’t any significant difference with respect of all parameters at sixth week of RT (Table 4).
The semiquantitative scoring of chronic inflammation, fibrosis and TGF-β staining at 6th and 16th weeks of RT.

RT: radiotherapy; H: halofuginone; TGF-β: transforming growth factor-beta.
aScores for chronic inflammation are 0 = none, 1 = mild, 2 = moderate, 3 = severe.
bScores for fibrosis are 0 = none, 1 = mild, 2 = moderate, 3 = severe, 4 = total lung fibrosis.
cScores of TGF-β are 0 (−), 1 (+), 2 (++) and 3 (+++).
Pairwise comparisons of the RT groups regarding to inflammation, fibrosis, and TGF-β scores at 6th and 16th weeks of RT.

G: group; RT: radiotherapy; TGF-β: transforming growth factor-beta.
aBonferroni Correction was used to evaluate the significance levels of type-I error for pairwise comparisons. p < 0.05.
At 16th week of RT, Kruskal–Wallis test revealed that there were significant differences between the study groups in terms of the chronic inflammation, fibrosis and TGF-β (p < 0.001 for all; Table 3). In parallel to the sixth weeks findings, for all the parameters RT groups had higher scores than non-RT groups. There weren’t any significant differences in between the non-RT groups again for all parameters. The inflammation, fibrosis and TGF-β scores of RT group were significantly higher than RT + 2.5 μg H and RT + 5 μg H groups at 16th week of RT (p values were 0.039 and 0.001 for inflammation; 0.042 and 0.001 for fibrosis and <0.001 and <0.001 for TGF-β scores, respectively). When RT + H groups compared at 16th week of RT, the fibrosis and TGF-β scores of RT + 2.5 μg H group were significantly higher than RT + 5 μg H group (p values were 0.040 and 0.028, respectively; Table 4, Figures 1 and 2).

Histochemical Masson trichrome staining (×200): Section from the lungs of the rats from (a) control group, (b) RT + 5 H group, (c) RT + 2.5 H group and (d) RT-only group at 16th week of RT. (a) Control group: Normal alveolar structures with thin alveolar walls. (b) RT + 5 H group: There were thickening in the alveolar walls with mild fibrosis. (c) RT + 2.5 H group: There were thickening in the alveolar walls with moderate fibrosis. (d) RT-only group: There were thickening in the alveolar walls with severe fibrosis and partial lung obliteration. RT: radiotherapy; H: halofuginone.

Immunohistochemical TGF-β staining (×200): Section from the lungs of the rats from (a) control group, (b) RT + 5 H group, (c) RT + 2.5 H group and (d) RT-only group at 16th week of RT. (a) Control group: There were a few TGF-β-positive alveolar epithelial cells or fibroblasts with a staining of low intensity. (b) RT + 5 H group: TGF-β positivity was lower than group c and d. (c) RT + 2.5 H group: TGF-β positivity was lower than group (d). (d) RT-only group: There were intense and diffuse TGF-β positivity in alveolar epithelial cells or fibroblasts. RT: radiotherapy; H: halofuginone; TGF-β: transforming growth factor-beta.
Ultrastructural findings
The sixth-week electron microscopic examinations revealed that there were no apparent changes detected ultrastructurally in the control group, 2.5 μg and 5 μg H groups. In the control group, the alveolocapillary membrane, bronchi and bronchioles were ultrastructurally normal. We didn’t observe any vacuoles in the alveolar epithelial cells. There wasn’t any intercellular oedema in the bronchioles and lower respiratory systems. However, in the RT-only group, there were vacuoles in the alveolar epithelial cells. The alveolocapillary membrane was ultrastructurally normal. The bronchi and bronchioles were ultrastructurally normal in this group. The ultrastructural finding of both RT + 2.5 μg H and RT + 5 μg H groups were same with RT-only group. Our sixth week findings revealed that all the RT groups independent from H application had similar findings.
The 16th-week examination of the rats from the control group, and H-only groups were normal. On the other hand, rats from RT-only group showed vacuoles both in the alveolar epithelial cells and in the capillary endothelial cells. There was intercellular oedema in the bronchioles and lower respiratory systems. The ultrastructural finding of 2.5 μg H + RT group was same with RT-only group. However, the rats from RT + 5 μg H group had similar findings with sixth-week RT + 5 μg H group. At 16th week of RT, the most prominent deterioration was observed in both RT + 2.5 μg H- and RT-only groups, as their findings were progressed from 6th week to 16th week. On the other hand, the ultrastructural findings of RT + 5 μg H groups did not deteriorated at 16th week of RT (Figure 3).

Electron micrograph showing ultrastructural appearance of (a) control group, (b) RT + 5 H group, (c) RT + 2.5 H group and (d) RT-only group at 16th week of RT (original magnification ×7500; v = vacuole, io = intercellular oedema). (a) Control group: electron micrograph showing alveolar epithelial cells (*), nucleus of an alveolar epithelial cell (n) and an erythrocyte (e) inside the alveolar capillary in the lung of a control group rat. (b) RT + 5 H group: There were vacuoles in the alveolar epithelial cells. The alveolocapillary membrane was ultrastructurally normal. The bronchi and bronchioles were normal. (c) RT + 2.5 H group: There were vacuoles in the bronchiole and the alveolar epithelial cells. There was a less severe intercellular oedema than the RT-only group. (d) RT-only group: There was an intercellular oedema in the bronchioles and lower respiratory system. Many vacuoles were observed in the bronchiole and the alveolar epithelial cells. RT: radiotherapy; H: halofuginone.
Discussion
The lung is one of the most sensitive tissues to ionizing radiation, and damage to normal tissue remains a major obstacle in the treatment of a variety of cancers. Modern treatment techniques including intensity modulated RT , image-guided RT and stereotactic body RT are still limited by toxicity of nearby normal tissues, thus impending further gains with these technologies. Additionally, most of the patients receive chemotherapeutic agents including Bleomycin which may exacerbate the RILI. Therefore, RILI is of critical importance and major dose-limiting factor for a radiation oncologist in attempting to deliver curative doses to the tumour. It has been well known that TGF-β is the master cytokine in the cellular events which result in radiation-induced fibrosis. 1 H specifically inhibits collagen α1 gene expression, resulted in a decrease in collagen synthesis, and the TGF-β-induced collagen synthesis. 8 By the light of these findings, we proposed that H may ameliorate the RILI 12 ; and we conducted to the current study. Our results suggested that H is an effective agent for amelioration of the RILI. The effect of H on RILI was same with using lower doses or higher doses at sixth week of RT. However, with long-term follow-up, our results suggested that using higher doses were more effective than lower doses with respect to the amelioration of RILI.
RILI is the reaction of the organ lung to radiation effects in various target cells. It starts as an exudative inflammation, with the clinical picture of interstitial pneumonia 6–12 weeks after irradiation, and proceeds to a productive chronic inflammation lasting several months and terminating, as other chronic inflammations do, in scar formation, called lung fibrosis. Numerous cytokines such as TNF-α, interleukin-1, platelet-derived growth factor, fibroblast growth factor and TGF-β have been reported to be increased within the irradiated tissue. 8 TGF-β levels are increased as early as 6 h after irradiation and remain elevated fibrotic lesions as long as 20 years. 7,13 RILI is typically divided into two phases: pneumonitis and fibrosis. The fibrotic phases tends to manifest >3 months after RT. 1 Therefore, in the current study, we killed the animals in two different periods as 6th and 16th weeks of RT, in order to define both the pneumonitic and fibrotic phases.
H, (7-bromo-6-chloro-3-[3-(3-hydroxy-2-piperidinyl)-2-oxopropyl]-4(3 H)-quanazolinone) an alkaloid isolated from the D. febrifuga plant, originally used in fowl as an anticoccidiostatic food supplement, reduces avain skin collagen content. In vitro, treating cultured dermal fibroblasts with H attenuated the incorporation of proline into collagenase digestible proteins, without affecting the production of noncollagenase proteins, cell proliferation or degradation. H specifically inhibits collagen α1 gene expression, resulted in a decrease in collagen synthesis, and the TGF-β-induced collagen synthesis. 8 It has been demonstrated that H reduces fibrosis formation in many pathological conditions. 8,14 –30 H has shown to reduce fibrosis in mice models with stretched skin due to scleroderma, 21 to decrease in the liver fibrosis model due to thiacetamide, 22 to lessen graft versus host disease, 23 to improve muscular dystrophies including dysferlinopathy, 20,24 and lessen mesangial cell proliferation and matrix deposition in the kidney, 25 to have beneficial effect the development of development of airway and lung parenchymal fibrosis in the mouse lung transplant model, 30 to inhibit proliferation and invasion of hepatocellular carcinoma HepG2 cell line, 31 to promote satellite cell activation and survival in muscular dystrophies 32 and to attenuated arthritis formation in subchondral bone. 33 To the best of our knowledge, current study is the first one evaluating the effect of H on RILI.
Ertugrul et al. 26 administered intraperitoneal H for 30 days to a group of rats after they traumatized the subglottic area, while they monitored the second group as controls. Their study suggested that fibrosis formation was significantly less in rats treated with H when compared to that of control group. Ozcelik et al. 27 administered intraperitoneal H for 21 days after producing corrosive substance injury in the rat oesophagus using 50% sodium hydroxide. They performed a histopathological examination and measured the hydroxyproline levels of oesophageal tissue of rats killed on day 21 in order to assess the fibrosis and stenosis index. Hydroxyproline levels and stricture formation in the H group were found to be significantly lower than that of the control group. Moreover, Dabak et al. 28 observed the effect of H on preventing oesophageal and hypopharyngeal fibrosis and suggested that H can be used safely to prevent radiation-induced oesophageal and hypopharyngeal fibrosis. Ishii et al. demonstrated that H is a protector against radiation-induced leg fibrosis by attenuating the induction of key members of the TGF-β signalling pathway, 18 without protecting against radiation-induced tumour re-growth delay. Therefore, the authors conducted a new study to determine if H might enhance the radiosensitivity of human tumour cell lines. 29 Their study revealed that H treatment inhibited cell growth, halted cell cycle progression, decreased radiation-induced DNA damage repair and decreased TGF-β receptor II protein levels, leading to increased cellular radiosensitization.
Lin et al. studied the antitumour effects of H in combination with RT using Lewis lung cancer cell lines and xenograft model mice. 34 Their study suggested that H inhibited type I collagen expression and angiopoiesis and hepatic and pulmonary metastases. Additionally, they confirmed the radiosensitizing effect of H, which was previously determined by Cook et al. 29 The authors evaluated the drug toxicity of H before starting the experiments. They found that H dose of 1.0 μg/day and 2.5 μg/day had no effect on mouse physiology after 3 weeks of observation for drug toxicity, but one mouse died with a dosage of 5.0 μg/day, and other mice were unresponsive. Therefore, they used a dose of 2.5 μg/day. However, in the current study, we observed no rat death due to either RT or H application. Additionally, our results suggested that the use of a dosage of 5.0 μg/day significantly improved radiation-induced lung fibrosis with long-term follow-up.
The irradiation doses used in routine clinical practice are different from the ones used in animal studies. Most patients in routine practice are treated with conventional fractionation to a total dose of 50–70 Gy, and it is given in 25–25 fractions. In animal studies, it is not practical to use the fractionated schemes. Therefore, the biologically equivalent dose of the same total dose in one fraction should be calculated. According to the linear quadratic model, the 12 Gy single dose of radiation, as used in the current study, corresponds to 30 Gy, in the fractions, when α/β ratio of 3–4 is used. In our previous study, we have demonstrated that a single 12 Gy dose is enough to determine lung fibrosis in Wistar–albino rats. 9 Therefore, we used a single dose of 12 Gy irradiation in the current study and we observed the lung fibrosis with this dose.
As conclusion, the current study is the first one observing the effect of H on RILI. Our results suggested that the use of H improves RILI. Since the chronic inflammation, fibrosis and TGF-β scores of RT-only group were higher than both low-dose and high-dose H + RT groups at both 6th and 16th weeks of RT. Additionally, we observed that at 16th week RT, the fibrosis and TGF-β scores of low-dose H + RT group were significantly higher than high-dose H + RT group. Electron microscopical findings also supported these results. Therefore, the effect of the H was more prominent in at higher dose and after long-term follow-up. The anti-fibrotic effects of H could potentially be attributed to its inhibitory effects on the TGF-β signalling pathway. These findings should be clarified with further preclinical and clinical studies.
There is no role of study sponsors in the study design, in the collection, analysis and interpretation of data; in the writing of the manuscript and in the decision to submit the manuscript for publication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Konya Training and Research Hospital.