
Abstract
Aim:
To describe various types of Chinese hospitals’ emergency department (ED) physicians’ knowledge of antidotes and the comparative availability of toxicological treatments at these hospitals.
Methods:
We emailed a written survey to the ED doctors of 900 hospitals in China. The hospitals’ names and addresses were obtained and randomly selected from the 6214 hospitals registered by the Chinese Medical Association. The survey included 23 questions on antidotes to commonly seen poisonings as well as questions on the availability of antidotes and decontamination techniques at each hospital.
Results:
Six hundred and fifty three hospital emergency directors responded to the survey 72.6% response rate). Overall knowledge of antidotes is not high and varied depending on antidote. Physicians in Eastern China, those working in tertiary-level hospitals and those working in hospitals with higher numbers of beds performed significantly better. On average, only 35.6% of the 23 antidotes were available in all reporting hospitals; 54.1% can get these antidotes from nearby hospitals and 42.0% can get them from a local CDC poison control center. However, only 57.3% can get a requested antidote within two hours. Gastric lavage is the most widely used decontamination procedure, and the availability of extracorporeal decontamination techniques is between 67.2% and 79.6% (depending on type).
Conclusion:
Knowledge of specific antidotes correlated significantly with size, type, and region of hospital in China rather than with individual physician characteristics. Significant antidotes remain unavailable or unavailable within 2 h in about half of all hospitals surveyed, although all major acute decontamination treatments and techniques seem quite prevalent.
Introduction
Poisoning is a very important cause of morbidity and mortality in China. It is the fifth leading cause of injury-related mortality and its incidence is rising. 1 For comparison, in the United States, the American Association of Poison Control Centers’ (AAPCC) National Poison Data System (NPDS) reported more than 2.1 million human poison exposures and approximately 2500 poisoning-related deaths in 2013 (7.9 deaths/million). 2 In China, there are 18.6 deaths/million in urban areas and 29.1 deaths/million in rural areas. There were a total of 31,000 poisoning-related deaths in 2012. Due to under-reporting, however, it is likely that the associated mortality is much higher than those statistics would indicate. 3 Looking at individual hospitals, poisonings are responsible for about 1.2–8.0% of hospital emergency department (ED) visits. 4,5 A meta-analysis published in 2008 showed the mortality rate of acute poisoning in China is 2.06%, 26.74% of which was contributed by organophosphates alone. 6
If a poisoning event is recognized early and appropriate supportive care is initiated rapidly, the majority of patient outcomes will be favorable. 7 The treatment of poisoning cases in the ED begins with stabilizing the patient and assessing vital signs, starting with the ABCs (airway, breathing, and circulation), followed by gastrointestinal (GI) decontamination as indicated, and/or the immediate use of a possible antidote. 8 One key issue in this chain of events, however, is how much does the physician working in ED know about antidotes? And how many resources are available to the physician for assistance as needed?
So far there are very limited studies evaluating physicians’ knowledge of antidotes for poisoning and the availability of the necessary resources to treat poisoning cases. Published research in this area has concentrated mainly on the investigation of antidote availability. Over the past few years, several studies have shown that antidote unavailability is common in health-care facilities and sufficient stocking of antidotes remains a worldwide problem. 9 –12 There are so far no studies to date that have addressed the level of preparedness of Chinese hospital EDs and their physicians for the management of acute toxic exposures and poisonings. We initiated a countrywide survey to describe various types of Chinese hospitals’ ED physicians’ knowledge of antidotes and the comparative availability of toxicological treatments at these hospitals.
Materials and methods
Study design and population
We e-mailed a written survey to the ED directors of 900 hospitals in China. The hospital names and addresses were obtained and randomly selected from the 6214 hospitals registered by the Chinese Medical Association using a computerized random number generator. The Chinese Medical Association is a nationwide academic group that has more than 500,000 individual members. Hospital characteristics were abstracted from the system, including bed capacity, hospital level, teaching hospital or not, and location category (urban or rural) of the hospital. The survey was asked to be completed by one of the physicians on the shift the day the e-mail was received. They were required to provide their basic personal information and specialty, seniority, rank, the way they acquired their toxicology knowledge, and the place they are working in. To maximize the response rate, researchers contacted appropriate staff by telephone, before and after the survey e-mail out. Surveys were e-mailed to hospitals in January 2014.
Survey content and administration
The survey was developed in accordance with guidelines for the design and conduct of self-administered surveys for clinicians. 13 After completing a literature review, a local panel of experts assisted in item generation, reduction, and pretesting. The complete electronic survey was then piloted with ten hospitals to ensure ease of use, precise description, and comprehensibility.
The survey used a fill-in-the-blank format and consisted of three parts. (A copy of the survey is shown in the supplementary file.) The first part queried knowledge of antidotes to 23 kinds of commonly seen poisonings, including 2 kinds of pesticides: organophosphates and (anticoagulant) rodenticides; 2 kinds of biological toxins: datura and snake bites; 8 kinds of chemicals: carbon monoxide, nitrite, methanol, cyanide, fluoride, lead, iron, and thallium; 11 kinds of medicines: acetaminophen, opiates, benzodiazepines, tricyclic antidepressants, heparin, beta blockers, sulfonylurea, digoxin, methotrexate, isoniazid, and sodium valproate. Every time they gave the right antidote answer to the poisoning they received +1 point to their total score, with a score of 23 being the highest. At the end of survey, the responders were required to list the top three human poisoning-related substances they encounter in their ED most frequently.
The second part of the survey queried the stocking status in their emergency department of several antidotes and, if unavailable, whether they can get them from their local Centers for Disease Control and Prevention (CDC) or another nearby hospital and how long they think it would take to get.
The third part of the survey queried what kinds of decontamination techniques were available in their hospital, including cathartic, charcoal, lavage, whole bowel irrigation, hemofiltration, hemodialysis, and/or hemoperfusion.
Ethical statement
This study received approval from the Ethic Department of Peking Union Medical College Hospital before the initiation of the study. The study was a non-interventional study involving anonymized doctors. No information about any participant was reported in the article. All the participants in this study consented to having the results of their surveys published in this study.
Statistical analysis
The data are presented as a mean ± standard deviation. Comparison of the data was undertaken by independent Student’s t test or non-parametric Mann–Whitney U test. Stepwise multiple linear regression analysis was performed to identify characteristics that were independently and significantly associated with antidote knowledge. Statistical analysis was undertaken by SPSS version 16 (IBM Corporation, Armonk, New York, USA).
Results
Questionnaires were e-mailed to 900 hospital emergency directors and 653 (72.6%) were returned. In all reporting hospitals, 311 can only handle adult poisonings while 342 can also treat pediatric poisonings. Responders included physicians in all 31 provinces in mainland China. All respondents who were physicians working in a hospital’s emergency room/department (e.g. Emergency Medicine, Internal Medicine and Intensive Care Medicine, etc.) were enrolled.
The general situation of the respondents and their corresponding scores are listed in Table 1. Physicians in Eastern China, those working in tertiary-level hospitals, and those working in hospitals with higher numbers of beds preformed significantly better. Those results with significant differences were analyzed with stepwise multiple linear regression. As a result, we found that hospital region and tertiary hospital-level status were the independent factors associated with higher scores (β = −0.236, p < 0.001 and β = −0.148, p = 0.003, respectively).
Responders and their corresponding scores.

Knowledge of different individual antidotes varied significantly between different distinguishing categories. In 6 out of 23 antidote questions, physicians of differing specialty performed significantly differently. In 10 out of 23 antidote questions, physicians of differing seniority performed significantly differently. In the comparison of different rank physician, only 2 out of 23 antidote questions had significant differences. In 5 out of 23 antidote questions, physicians with different ways of acquiring knowledge performed significantly differently. In 5 out of 23 antidote questions, physicians of differing hospital character performed significantly differently. In 4 out of 23 antidote questions, physicians of differing hospital location performed significantly differently. The results are listed in Table 2.
Distinguishing categories and their respective significant antidote knowledge variations (all p < 0.05).

The overall correct rate of identifying different antidotes in the survey is shown in Figures 1 and 2, with digoxin the highest in the medications group and organophosphates the highest in the pesticides, biological toxins, and chemicals group. The three most commonly seen poisonings as polled in the questionnaires are shown in Figure 3. The leading types of poisonings the responding Chinese physicians saw were organophosphates, sedatives, and carbon monoxide.

Knowledge of antidotes to select medications.

Knowledge of antidotes to pesticides, biological toxins and chemicals.

Percentage chosen as one of the three most commonly seen poisonings (top 10).
Availability of the 23 antidotes is shown in Table 3. On average, 35.6% of the 23 antidotes are available in all the reporting hospitals; 54.1% can get the antidotes from nearby hospitals and 42.0% can get them from the local CDC poisoning control center. Totally 57.3% can get a requested antidote within 2 h. The antidotes available were significantly fewer in rural areas and non-tertiary hospitals. The availability of special decontamination procedures and extracorporeal decontamination techniques are shown in Figures 4 and 5. Of all the respondents, 94.4% can do gastric lavage, 83.2% can do cathartics, 45.5% have charcoal, and 40.3% can give whole bowel irrigation; 72.0–79.6% of respondents have hemofiltration and hemodialysis available, 67.2% of them can do hemoperfusion; 22.5% of them do not have extracorporeal techniques available.
Availability of the 23 antidotes.

ap < 0.01: rural compared to urban.
bp< 0.01: non-tertiary hospitals compared to tertiary hospitals.
cp < 0.05: rural compared to urban.
dp < 0.05: non-tertiary hospitals compared to tertiary hospitals.
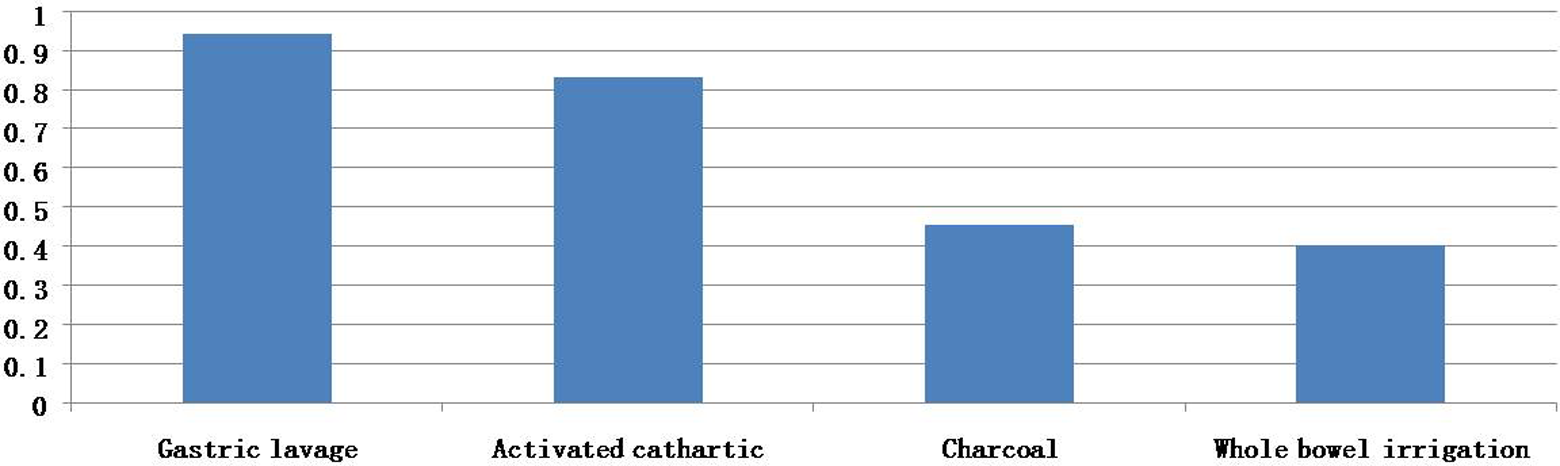
Availability of decontamination procedures.

Availability of extracorporeal decontamination techniques.
The information about the 247 non responder hospitals is limited. But we can get the hospital characteristics from the system; 179 (72.5%) of them have a bed capacity of less than 500; 206 (83.4%) of them are non-tertiary hospitals; 198 (80.2%) of them are non-teaching hospitals; 174(70.4%) of them are located in rural area, and 184(74.5%) of them are in West China.
Discussion
The primary findings of our study are as follows: (1) the top three leading types of poisonings reported in our survey are organophosphates, sedatives, and carbon monoxide. (2) Knowledge of antidotes is not high and varied depending on the antidote and physician's hosptial. (3) The availability of antidotes in responding hospitals is not satisfactory. (4) Gastric lavage is the most widely used decontamination procedure, and the availability of extracorporeal decontamination techniques is not bad compared to other Asian countries. 10,14
Appropriate knowledge of the antidotes is essential for the successful treatment of intoxicated patients. However, the availability of antidotes, special decontamination procedures, and extracorporeal decontamination techniques are equally crucial to successfully treating patients. Currently, there are no generally recognized specific criteria that define the preparedness of an ED for the management of acute toxic exposures and poisonings in China. A list of commonly required resources and items that might be used for the treatment of acute poisonings was compiled from published recommendations. 7,15,16 Our results demonstrated that, overall, physicians in responding hospitals in China had some knowledge on the use the various antidotes, although their knowledge varied depending on the antidote and their specialty.
In this survey, although the result may subject to personal bias, the leading types of poisonings the responding Chinese physicians saw were organophosphates, sedatives, and carbon monoxide. Organophosphates are the one with the highest score, with 88.76% of responders reporting them among the top 3. This result is similar to reports from India, Sri Lanka, and some African countries. 17 –19 Official data for 2005 suggest that 19.6% of India’s suicides were self-poisonings with insecticides. 20 National mortality data from Sri Lanka indicates that 54% of suicides were by pesticide ingestion in that same year. 21
The situation is very different in the United States. The 31st Annual Report of the AAPCC’s NPDS shows the top three in the United States in 2013 were analgesics (11.5%), cosmetics/personal care products (7.7%), and household cleaning substances (7.6%). 2 Why the difference? The most important reason is probably that the majority of clinically significant poisonings that present to EDs in China are suicides, which contributes to 37.2–57. 9% of all poisonings in China. 3,5 The easiest way to commit suicide is to take something poisonous close at hand. Organophosphates are the most widely used pesticide in rural areas, and sedatives are very widely used in urban areas, leading to their wide availability. In winter, the main energy source for heating in China is coal, of which there is a large supply in northern China. Inappropriate use and venting of coal-fired heaters will generate carbon monoxide, and houses in winter are actively made less-well ventilated because of the cold. Analgesics are not a common source of poisoning in Chinese EDs since, in the general Chinese cultural context, people are encouraged to be patient and tolerant of pain and narcotics are tightly regulated. One investigation showed nearly 100% of surveyed patients believed that all analgesics are optional and only 38.5% was willing to take analgesics even if they had cancer pain. 22
Antidotes play a critical role in the care of poisoned or overdosed patients. World Health Organization (WHO) Guidelines for Poison Control Centers recommend that all antidotes needed immediately (within 30 min) should be stocked at all hospitals. 23 In the United States, in the top four single categories of poisonings associated with the largest number of fatalities, three have antidotes, which are opioids, acetaminophen, and tricyclic antidepressants. 2 Similarly, all of the leading three kinds of poisonings in China in this survey have antidotes. In our results, the percentage of physicians knowing the correct antidotes for organophosphates, sedatives, and carbon monoxide are 98.8%, 73.7%, and 84.4%, respectively. For sedatives and carbon monoxide, these numbers are not good enough, perhaps because flumazenil and hyperbaric oxygen are controversial and not commonly available throughout China. This phenomenon may also reflect a lack of toxicology continuing education in China, especially as compared to that in the United States. 24
When we looked at the overall results of the survey, we found that the average test score was 14 out of 23 (61.5% correct). Respondent test results did not differ significantly based on their medical specialty, physician level (e.g. attending vs. resident), how many years of practice they have had, or how they acquired their toxicology knowledge. But it differed significantly between tertiary and non-tertiary hospital physicians and also between hospitals of differing numbers of hospital beds. Though the number of hospital beds did not seem to be an independent influencing factor based on our further statistical analysis. These results suggest that in China the type of hospital a physician works in has a stronger influence on their toxicology knowledge than their own background.
Conventional wisdom in China has patients going to the largest hospital first if they have any disease, leading to patients jamming into larger hospitals and leaving very few patients in smaller hospitals, a phenomenon which has been reported in published studies. 25 Our results in this study support this conventional wisdom. One possible cause of this disparity may a “self-fulfilling prophecy” given the divergent patient numbers. Physicians in larger hospitals (although relatively overworked compared to their smaller hospital counterparts) will have had more experience in treating a broader range of poisonings than those physicians working in smaller hospitals. Another reason might be that the ED director’s training in larger hospitals might have included exposure to toxicological emergencies. Another important independent factor influencing test scores was geographic region. Physicians from Western China scored nearly 1/5 lower than physicians from Eastern China. This is not necessarily surprising, because in China the Western region is still developing compared to the more urban Eastern region. The economic resources and population between these two regions are significantly different.
When comparing the location of the hospital, physicians in rural hospitals and physicians in urban hospitals showed no significant differences in their total scores. Only in 4 out of 23 antidote questions, physicians in urban hospitals performed better than physicians in rural hospitals. Similarly, physicians in teaching hospitals and physicians in non-teaching hospitals showed no significant differences in their total scores. In only 5 out of 23 antidote questions, physicians in teaching hospitals performed better.
Although our study showed hospital factors were more likely to predict test outcomes, individual physician factors are not totally unimportant. In our survey, the knowledge of rodenticide, datura (a common poisonous plant with an anticholinergic toxidrome) and methanol poisoning antidotes is much higher in emergency medicine physicians than in non-emergency physicians. On the other hand, knowledge of beta blockers, sulfonylurea, and isoniazid poisoning antidotes is lower in emergency medicine physicians. This difference may be because the latter three medications are all frequently used by internal medicine physicians who were the majority of the non-emergency physicians surveyed. Additionally, overdoses with these three medications are relatively uncommon in China and may not be as actively taught to emergency medicine physicians. 3 On the other hand, in 10 out of 23 antidote questions, physicians of differing seniority performed significantly differently. Interestingly, the groups with highest scores were not always the physicians with the highest seniority (which would be those with over 10 years’ experience), but were those physicians with “only” 3–5 years or 5–10 years of work experience. This may be because emergency medicine is a relatively young specialty in China with a history of only 30 years. The development of toxicology in China is even shorter. Most of the emergency medicine physicians are, in fact, former internal medicine physicians with limited formal emergency medicine training. Formal emergency medicine training has only existed for the past 10 years. Finally, there is still no formal training of emergency medicine trainees in clinical toxicology in China. 3
Lack of significant difference between individual physicians was dramatically shown in another comparison: different rank physician groups. In China, physicians are distinguished by three ranks: primary-level physicians, most of who are residents, and middle- and high-level physicians, most of whom are attending doctors. Rank is mainly distinguished by how much research physicians have done and less by their patient care. In this comparison, only 2 out of 23 antidote questions had significant differences. Rank level is a classification with Chinese characteristics and is very important in a Chinese doctors’ career. But it seemed to have little influence on a doctor’s antidote knowledge score in our survey.
Do the ways physicians acquire their toxicology knowledge matter? Our data showed that only in 5 out of 23 antidote questions, physicians with different ways of acquiring knowledge performed significantly differently. In 4 out of the 5, physicians who got their toxicology knowledge from checking the literature scored highest.
Beside physician knowledge, the antidote stocking status in the emergency department was also queried. These results were shockingly poor, as we predicted previously. 3 On average, only 35.6% of the 23 antidotes are available in all the reporting hospitals. Additionally, only 54.1% can get the antidotes from nearby hospitals and only 42.0% can get them from the local CDC poisoning control center. Even factoring in those hospitals with access to a nearby source (hospital or CDC), only 57.3% can get a requested antidote within 2 h. Fortunately, the antidotes for organophosphates, which are pralidoxime and atropine, are readily available in all of the reporting hospitals – probably because organophosphate poisonings are so commonly seen. The stocking situation is even worse in rural areas and non-tertiary hospitals. Lower hospital rank and hospitals in rural areas stocked less antidotes, consistent with findings from other studies. 26 –28 Possible reasons include budget constraints in these hospitals, perceived lack of antidote need, short antidote expiry dates or the assumption that patients or antidotes could be transferred quickly if needed. However, smaller hospitals can still expect to receive patients with acute poisonings. In the United States, there are national consensus guidelines to guarantee the availability of key antidotes, 16 which include a recommended list and the quantities of antidotes that should be readily available in hospitals that provide emergency care. Some of the antidotes should be available for immediate administration on a patient’s arrival, which requires stocking in the ED at most hospitals; other antidotes should be available within 60 min and can be stocked in the hospital pharmacy provided that prompt delivery to the ED can be assured. It seems stocking critical antidotes in only select local hospitals or CDC centers is unlikely to satisfy acute poisoning treatment time frames.
When a poisoned patient arrives in the ED, decontamination procedures can turn a potentially life-threatening intoxication into a less-threatening situation. The most commonly used procedures besides irrigation, food, and fresh air are activated charcoal, gastric lavage, emetics, cathartics, and whole bowel irrigation. Our data showed 94.4% of respondents can do gastric lavage, 83.2% can do cathartics, 45.5% have charcoal, and 40.3% can give whole bowel irrigation. While in the United States the most commonly used decontamination procedure is activated charcoal, followed by gastric lavage, cathartics and whole bowel irrigation. 2 However, similar to a report from Palestine, 14 it seems that in China gastric lavage is the most popular decontamination procedure 29 while the use of lavage in the United States is very limited. 2 This may be because organophosphates are the most commonly seen poisoning, consensus opinion supports the use of lavage within 1–2 h of ingestion. 30 Serious risks of the procedure include aspiration pneumonia, arrhythmia, fluid and electrolyte abnormalities, hypoxia, laryngospasm, and perforation of the GI tract or pharynx. 31 Availability of other decontamination resources besides gastric lavage in this study was not high, which is consistent with common practices recommended in the clinical literature, 31 –35 which support the limited use of all types of GI decontamination in acutely poisoned patients.
In some cases of acute poisoning, extracorporeal decontamination techniques such as hemodialysis and hemoperfusion may be needed, and our data showed 72.0–79.6% of respondents have hemofiltration and hemodialysis available, and 67.2% of them can do hemoperfusion for patients. Only 22.5% of them do not have extracorporeal techniques available. These results are better than those reported from Malaysia 10 and Palestine. 14 These results are likely mainly due to the development of nephrology departments in most hospitals in China, which would be available to perform these extracorporeal decontamination techniques as suggested by the Extracorporeal Treatments in Poisoning workgroup. 36
As we reported at the beginning, about 27% of hospital emergency directors did not return the survey, and nonresponders were more common among smaller, rural hospitals, the group that showed less knowledge in the survey and reported less availability of antidotes, special decontamination procedures, and extracorporeal decontamination techniques. So the true situation may actually be worse than what we found.
In conclusion, the burden of clinically significant poisonings in China is high. Knowledge of specific antidotes correlated more significantly with size, type, and region of hospital in China than individual physician characteristics. Significant antidotes remain unavailable or unavailable within 2 h in hospitals surveyed, although all major acute decontamination treatments and techniques seem quite prevalent. We believe more antidotes should be stocked and more directed education about the specific antidotes to common toxins be provided to physicians working in EDs in China.
Limitations
A limitation of our study is its reliance on voluntary reporting by physicians. We do not know for sure whether the respondent answered the survey without the help of outside sources of information. The significance and magnitude of this limitation is unknown. A second limitation is the hospitals chosen are all registered members of the Chinese Medical Association, which doesn’t fully represent all hospitals in China (e.g. the smallest rural hospitals are less common on this list). A third limitation is that China is very large, and poisoning epidemiology and physician knowledge may vary significantly between different areas. We did not distinguish in great detail between the different areas of China. We simply classified hospitals into an east area and west area because the development situation is very different between the two. The fourth limitation is the number of responders to our survey. About 27% of hospital emergency directors did not return the survey, and the nonresponders were mostly smaller, rural hospitals, the group that showed less knowledge in the survey and reported less availability of antidotes. So the true situation may actually be worse than what we found. Last but not least, we did not investigate the exact amounts of the antidotes in stock at the surveyed hospitals. Because all the responders in this survey were clinical physicians, they would have been unlikely to know current stocking levels in their hospitals’ pharmacies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.