
Abstract
Introduction:
Impaired diastolic flow is characterized by decreased left ventricular (LV) filling diastole, abnormal LV distensibility, or delayed relaxation. B-Type natriuretic peptide (BNP) is an indicator of various cardiovascular diseases and body volume status. The aim of this study was to determine whether the lowering of dialysate sodium (Na) levels is effective on LV systolic and diastolic parameters and BNP in the maintenance of hemodialysis patients.
Materials and Methods:
The study included 49 chronic hemodialysis patients. Left atrium (LA) diameter and LV ejection fraction, LV systolic and diastolic diameter, deceleration time (DT), pulmonary artery pressure (PAP), inferior vena cava diameter (IVCD), early diastolic transmitral flow (E) and late diastolic transmitral flow (A) velocities, E/A ratio, isovolumic relaxation time, peak early diastolic velocity (E′), late diastolic velocity (A′) of tissue Doppler mitral annulus, and flow propagation velocity of mitral inflow (V p) were measured before and 6 months after hemodialysis with low Na dialysate.
Results:
Six months after low Na hemodialysis, a decrease was observed in echocardiographic parameters such as PAP and IVCD (p < 0.05, p < 0.001, and p < 0.001, respectively). However, a significant difference was not observed in LA diameter. In LV diastolic measurement of E and A waves, E/A ratio, DT, V p, septal E′ and A′, and lateral E′ and A′ exhibited significant improvement by low Na HD. BNP level was significantly reduced (p < 0.001).
Conclusions:
Lowered dialysate Na concentration improves PAP, IVCD, and LV diastolic properties assessed by mitral inflow filling, tissue Doppler velocity, and mitral inflow velocity propagation.
Introduction
End-stage renal disease (ESRD) affects approximately 15% of the adult population and leads to high morbidity and mortality. 1,2 Cardiovascular disease (CVD) is the leading cause of mortality in ESRD patients, accounting for more than 50% of all deaths. 3 Patients with ESRD have high prevalence of cardiac risk factors such as hypertension (HT), which has been reported as an independent risk factor for CVD in hemodialysis (HD) patients. 4
ESRD causes increased extracellular volume regardless of the presence of edema. HT can be caused by even a relatively normal sodium (Na) intake. Patients with ESRD are particularly susceptible to Na burden. This susceptibility increases with the progression of renal disease. 5 Patients with renal failure who undergo HD cannot constrain their Na intake, and thus develop a significant saline excess between dialyses. Dialysate Na concentration is an important factor in Na overload. Large changes in circulating volume via Na intake or dialysate, including increase of left ventricular (LV) filling pressure, have been demonstrated to result in significant alterations in transmitral flow Doppler indices. 6,7
Diastolic dysfunction is associated with abnormal mechanical functions of the myocardium and consists of impaired filling and delayed LV relaxation, irrespective of whether the ejection fraction is normal or depressed. 8,9 ESRD patients are mostly characterized by LV hypertrophy and LV diastolic impairment. 10 Doppler echocardiography has been reported as an effective noninvasive tool for the evaluation of LV diastolic function, with characteristic observed changes in the transmitral Doppler flow caused by impaired LV filling. 11
Markers of body volume status and various CVD include natriuretic peptides, 12 B-type natriuretic peptide (BNP), and N-terminal pro brain natriuretic peptide (NT-proBNP). BNP is synthesized as an amino acid precursor protein, produced by the LV as a result of elevated myocardial wall stress. 12 BNP and NT-proBNP have been commonly reported as effective biochemical markers for ventricular dysfunction and heart failure. 13,14
The aim of this study was to determine whether the lowering of dialysate Na levels has any effect on LV systolic and diastolic parameters, BNP, and interdialytic weight gain (IDWG) in the maintenance of HD patients.
Materials and methods
Patients
Fifty-nine patients were enrolled in the study. Of these, 51 were suitable, but only 49 (18 women and 31 men) completed the study. Informed consent was obtained from each patient prior to enrollment. The study was approved by the local ethics committee of Yuzuncu Yil University Medical School. The study was conducted between February 2014 and October 2014.
Inclusion criteria included a creatinine clearance level of <10 mL/min/1.73 m2 and an ongoing chronic HD treatment for at least 1 year. Exclusion criteria included heart failure (LV ejection fraction <40%), secondary HT, liver and autoimmune disease, pulmonary disease or history of pulmonary embolism, heart valve disease, malignancies, hemoglobin levels <8 g/dL, and predisposition to hypotension. Patient records were studied to analyze patient demographics, etiology of ESRD, history of HT and antihypertensive medication, serum levels of Na, diabetes mellitus, smoking status, and hemoglobin, albumin, and lipid profiles.
Mean HD time was 51.7 ± 26.4 months. Dialysis was performed using synthetic polysulfone membranes (hollow fiber, low flux, K UF <20, 1.6 m2) with bicarbonate dialysate (with 33 mmol/L concentration) and 300–350 mL/min flow three times a week, with each session lasting 4 h. Concentrations of calcium, magnesium, and Na in the dialysate for the last 6 months were 1.5 mmol/L, 0.5 mmol/L, and 140 mEq/L, respectively.
Study protocol
Patients were evaluated before and 6 months after low-Na dialysate. The baseline Na concentration was 140 mEq/L, which was then lowered to 137 mEq/L to investigate the effect of low Na concentration. To rule out the acute effects of dialysis on measured parameters, all measurements were collected on a non-dialysis day, 24 h after the midweek session.
Echocardiographic examination
An echocardiographic examination was conducted for each patient by a single operator 6 months after low Na dialysate. Longitudinal scanning of the echocardiographic parameters was performed using a 3 MHz transducer (Vivid 3, General Electric). M-mode echocardiographic measurements were obtained from the left parasternal window and measurements were taken in accordance with the guidelines of the American Society of Echocardiography. 11 The measurements included left atrium (LA), LV systolic diameter (LVSD), LV diastolic diameter (LVDD), interventricular septum (IVS), posterior wall, pulmonary artery pressure (PAP), and inferior vena cava diameter (IVCD).
Diastolic function was assessed through the analysis of the mitral flow parameters. The sample volume was placed on the tips of the mitral leaflets, and the transmitral pulsed-Doppler measurements were performed using the apical four-chamber view. The measurements included deceleration time (DT), early diastolic transmitral flow (E), late diastolic transmitral flow (A) velocity, E/A ratio, and isovolumic relaxation time (IVRT). Velocities and time intervals were expressed in centimeter per second and millisecond, respectively.
The color M-mode of LV inflow and pulsed-wave tissue Doppler velocities were determined using the apical four-chamber view. Tissue Doppler velocities of the longitudinal mitral annular motion were assessed at both septal and lateral annular borders. Spectral pulsed-wave Doppler was used with the settings adjusted to record the high-amplitude/low-velocity myocardial signals. Tissue Doppler mitral annulus velocities including peak early diastolic velocity (E′) and late diastolic velocity (A′) were also assessed. The ultrasound beam was directed parallel to the flow identified by two-dimensional color images from the mitral valve orifice to the apex. Color gains were optimized to acquire the largest signal with no saturation effects. An early filling wave front was detected, which was consistent with the rapid filling phase. The slope of this wave front, which corresponded to the flow propagation velocity (V p), was assessed at 2 cm and at the apical leading edge of the color flow from the mitral annulus. 15
IDWG was described as the alteration in body weight between two consecutive HD sessions and was determined based on the subtraction of the dry weight from the weight prior to dialysis. During the dialysis sessions, symptoms associated with dialysis were monitored including cramps or hypotensive attacks in addition to any requirement for saline infusion arising from hypotensive attacks/cramps.
Hypotensive attacks were described as a decrease of 20 mmHg in SBP caused by the symptoms necessitating emergency medical care, Trendelenburg position, or saline infusion. Cramps were described as the symptoms necessitating emergency medical care or saline infusion with no reduction of BP. Saline infusion was described as infusion of 100 mL of saline solution (0.9%) for 5 min for the improvement of cramps or hypotensive attacks. Minor complications were described as headache and dizziness related to low Na dialysis.
Statistical analysis
Data were analyzed using SPSS for Windows 15.0 (SPSS Inc., Chicago, Illinois, USA). Quantitative variables are expressed as the mean ± standard deviation and qualitative variables as numbers and percentages. Changes from baseline to 6 months posttreatment in the observed parameters were assessed using a paired t test for normally distributed quantitative variables and a Wilcoxon test for non-normally distributed variables. A χ 2 test was used for qualitative variables. A p value of <0.05 was considered significant.
Results
Fifty-nine patients were enrolled into the study. Of these, 51 patients were suitable for the study, but 49 patients (18 women and 31 men) completed the study because 2 patients withdrew due to intradialytic cramps or hypotensive attacks associated with low Na dialysate. Baseline clinical and laboratory data of the subjects are given in Table 1.
Demographic and clinical characteristics of the patients.a
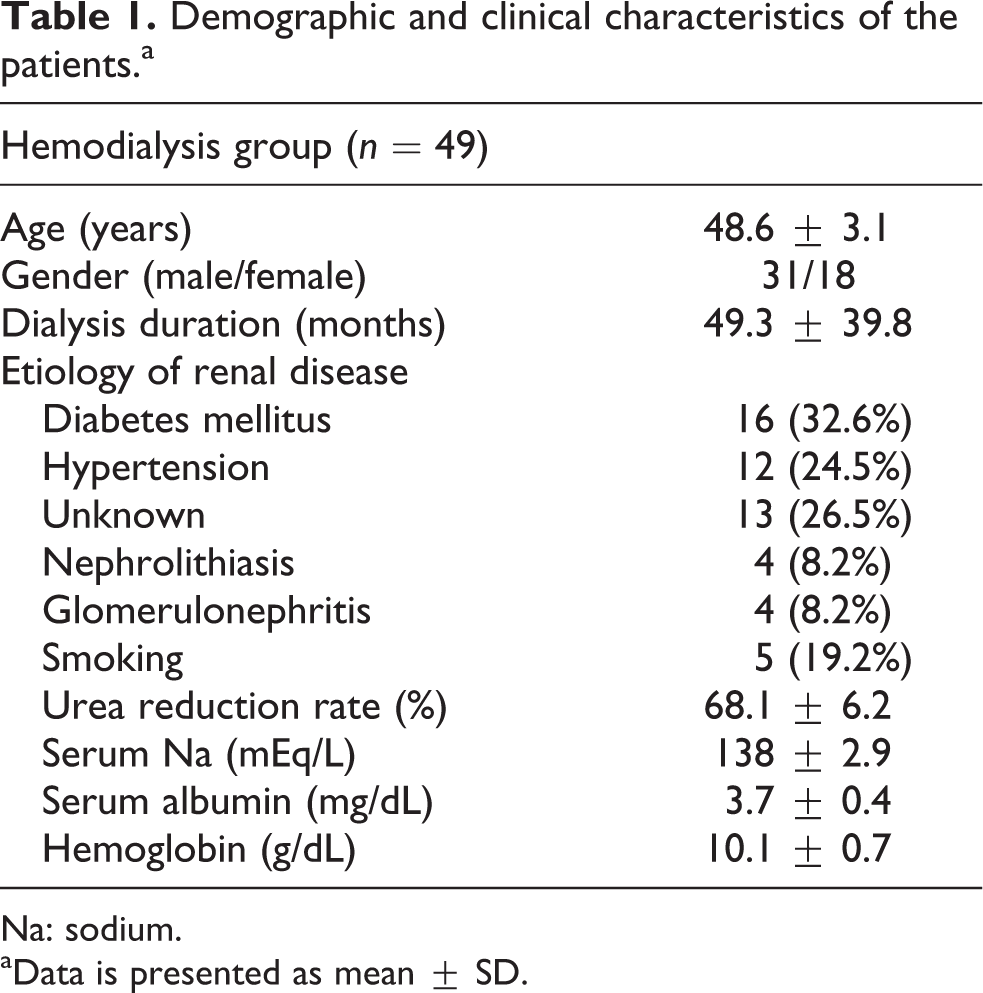
Na: sodium.
aData is presented as mean ± SD.
Thirty-three patients (67.3%) presented with HT and were taking antihypertensive medication. The average number of antihypertensive drugs per patient was 2.4 ± 0.6. The most commonly prescribed antihypertensive medications were calcium channel blockers, followed by angiotensin receptor blockers and beta blockers.
Six months after low Na HD, a significant reduction was observed in systolic blood pressure and in echocardiographic parameters, including PAP and IVCD (p = 0.05, p < 0.001, and p < 0.001, respectively; Table 2). LA diameter and serum Na level were also reduced, but no significant difference was observed (p > 0.05).
Clinical evaluation and M-mode echocardiography parameters of study groups.a

LA: left atrium; LVDD: left ventricular diastolic diameter; LVSD: left ventricular systolic diameter; PAP: pulmonary artery pressure; IVCD: inferior vena cava diameter.
aBold values indicate statistical significance.
Diastolic filling parameters including E and A wave, E/A ratio, DT of E wave and mitral color M-mode V p were significantly improved. In addition, while IVRT was reduced, this change was not significant. On the other hand, tissue Doppler velocities, including lateral and septal early diastolic velocity (E′) and A′, were increased (Table 3).
Pulse Doppler indices of study groups.a
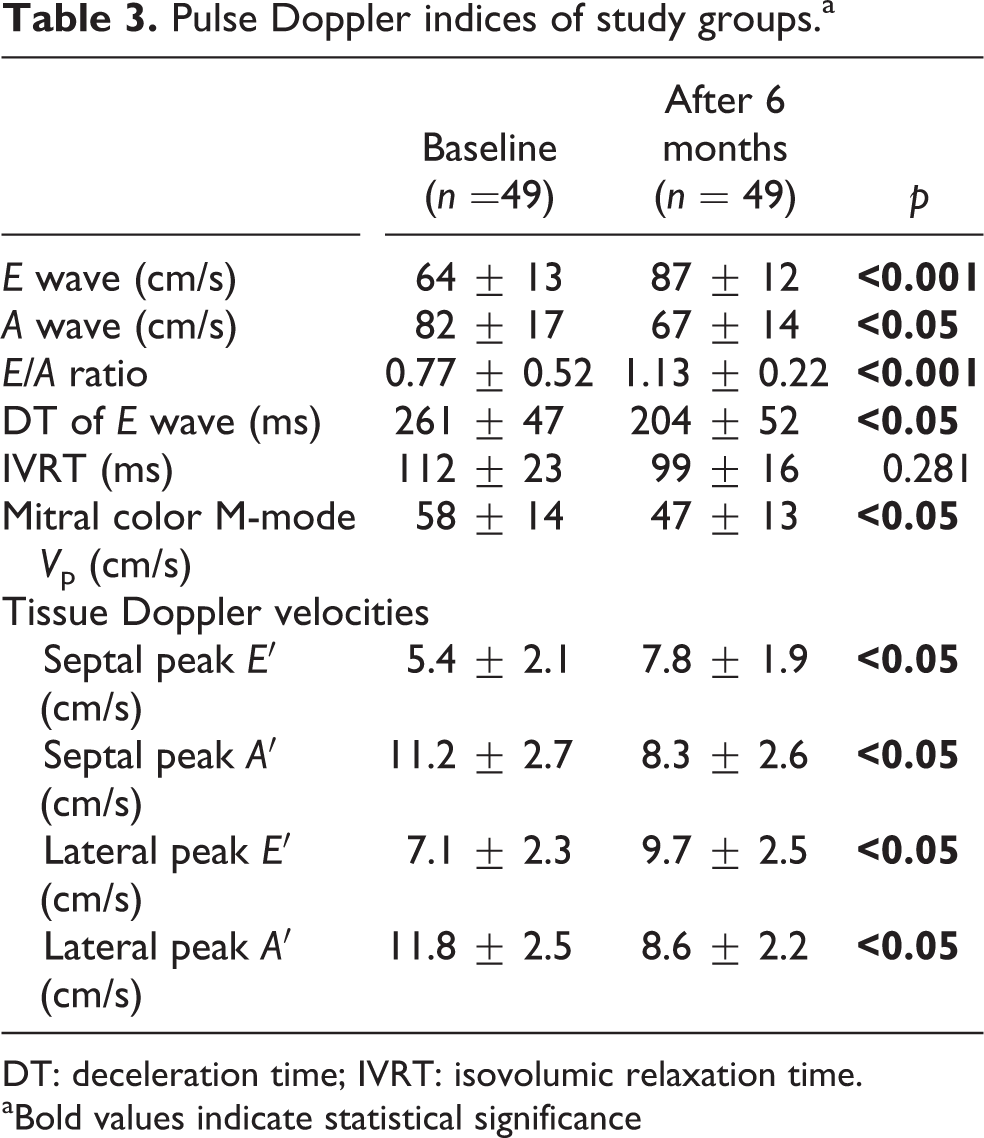
DT: deceleration time; IVRT: isovolumic relaxation time.
aBold values indicate statistical significance
Finally, the average number of antihypertensive medications decreased from 2.4 ± 0.9 to 1.6 ± 0.6 (p = 0.05), and BNP level decreased significantly with low Na HD (p < 0.001; Table 4).
BNP and inter-dialytic weight gain of study group.a

IDGW: inter-dialytic weight gain; BNP: brain natriuretic peptide.
aBold values indicate statistical significance
Discussion
In this study, we investigated the effects of low Na dialysate on M-mode echocardiographic and diastolic filling parameters and BNP levels in HD patients. Our most important findings were reductions in systolic blood pressure, PAP, IVCD, pulsed Doppler indices, tissue Doppler velocities, and BNP. In addition, a significant decrease was detected in the number of antihypertensive medications and IDWG.
ESRD leads to increased extracellular volume regardless of the presence of edema. In renal failure and HD, the patients who cannot constrain Na intake develop a significant saline excess between dialyses. Dialysate Na concentration is an important issue for Na overloads. 5 Eventually, HD results in chronic volume and pressure overload, causing ventricular hypertrophy, which is commonly related to diffuse interstitial fibrosis leading to diastolic dysfunction. 16,17 Moreover, the fluid changes arising from HD have been shown to be associated with significant changes in transmitral flow Doppler indices. 6,7
Echocardiography is a conventional method for the determination of LV diastolic function. Transmitral pulsed-Doppler indices such as IVRT, peak early filling velocity (E), A velocity, DT of the E wave, and E/A ratio have been commonly used in the determination of LV filling characteristics. 18,19 Most of the conventional echocardiographic parameters of LV diastolic function have been shown to be load dependent. 20 Similarly, the few studies on the use of Doppler echocardiography in HD patients have reported that there is a significant reduction in the peak E velocity and the E/A ratio following HD due to preload dependence. 6,21 In our study, we used these conventional echocardiographic LV diastolic parameters to assess low Na HD effects over a 6-month period. At the end of the treatment, E wave increased from 64 ± 13 to 87 ± 12 (p < 0.001), E/A ratio increased from 0.77 ± 0.52 to 1.13 ± 0.22 (p = 0.001), A wave decreased from 82 ± 17 to 67 ± 14 (p = 0.05), and DT of E wave (ms) decreased from 261 ± 47 to 204 ± 52 (p = 0.05). IVRT (ms) decreased, but no significant difference was established (p > 0.05).
Clinical studies have demonstrated that the assessment of mitral annular velocities by tissue Doppler imaging (TDI) can be easily and safely performed for the measurement of global LV systolic and diastolic function. 22 A number of studies have reported TDI preload independence, 23 whereas the others 24 have suggested a lack of TDI preload dependence. For instance, Ishizaka et al. 25 reported that failing hearts are more susceptible to load changes. In other studies, 26,27 decreased TDI parameters in the presence of normal systolic and diastolic function have been shown to be associated with the sensitivity of normal hearts to loading conditions. Nagueh et al. 26 reported that the presence of normal and enhanced relaxation states leads to E′ load dependence and leads to E′ load independence in the presence of impaired LV relaxation. In the present study, we showed that septal and lateral wall TDI parameters (p = 0.05) were improved.
Recent studies have shown that color M-mode propagation velocity of mitral filling has been recognized as a relatively preload-independent parameter for the investigation of diastolic function in the general population with or without systolic dysfunction. 28,29 Color M-mode enables color-coded monitoring of concurrent velocities along the M-mode scan line (i.e., the line from the mitral annulus to inside the LV) during the intraventricular flow assessment of mitral inflow filling. Brun et al. 30 assessed the slope of the early filling wave front from the mitral leaflet tips to the apical leading edge of the V p and found a significant negative correlation between V p and time constant of relaxation (τ) assessed invasively in patients with cardiomyopathy and coronary artery disease. This correlation indicated the effectiveness of color M-mode in the diagnosis of diastolic dysfunction. However, in this parameter, no alteration resulted from maneuvers changing the preload, which were previously mentioned in the differentiation of significant changes in conventional pulsed-Doppler indices. Therefore, this feature of color M-mode is a significant advantage over pulsed-Doppler studies and makes it a favorable instrument for the investigation of diastolic function. In the current study, color M-mode propagation velocity of mitral filling was used to detect the effects of low Na HD on diastolic filling. Moreover, mitral color M-mode V p decreased from 58 ± 14 to 47 ± 13 cm/s (p = 0.05).
Patients with ESRD have a high prevalence of conventional and nonconventional cardiac risk factors. 4 Nevertheless, traditional CV risk factors have been insufficient to explain the severity and extent of CV complications in ESRD patients. 31 Mallamaci et al. 32 reported that the combined use of endothelial dysfunction (asymmetric dimethylarginine), biomarkers of inflammation (CRP), and myocardiopathy (BNP) in ESRD patients increases the explanatory power of all-cause and CV mortality by approximately 20%. Moreover, recent studies have shown that cardiac troponin T, BNP, NT-proBNP, and high-sensitivity CRP are significantly related to one another, indicating a complex relationship among inflammation, cardiac biomarkers, malnutrition, and overhydration in dialysis patients. 33
Not surprisingly, the level of BNP is higher in HD patients compared to other populations. 34 BNP is secreted as a result of the increase in myocardial wall stretch, which implies that circulating BNP is an effective indicator of volume status. 35 Similarly, a previous small-scale study of HD patients identified an association between plasma BNP and extracellular water assessed by bioimpedance. 36
Several differential studies have investigated the ability of BNP to estimate CV mortality and adverse CV results in patients with HD. Naganuma et al. 37 demonstrated an HR of 51.9 for cardiac death in HD patients with BNP >700 pg/mL, compared to patients with BNP <200 pg/mL. Roberts et al. 38 conducted a prospective study of 108 patients on dialysis, 64 predialysis patients, and 80 kidney transplant recipients and found a correlation between BNP and a 2- to 3-fold increased risk of death in patients on dialysis. In our study, we found that lowering the dialysate Na significantly improved the BNP level from 2.467.23 ± 643.42 to 1.674.36 ± 471.83 (p ≤ 0.001).
The pathogenesis of HT in patients with ESRD is multifactorial and involves volume expansion and impaired endothelial function. 1,2 In HD patients, Na intake is determined both by diet and by the Na concentration of the dialysate. 39 The pre- and post-HD BP levels recommended by the National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative guidelines are <140/90 and <130/80 mmHg, respectively. 40 In the present study, lowering the dialysate Na resulted in a significant improvement in systolic blood pressure and a decrease in the average number of antihypertensive medications (from 2.4 ± 0.9 to 1.6 ± 0.6, p = 0.05).
In conclusion, the results demonstrated that lowering of dialysate Na concentration improves conventional diastolic dysfunction, tissue Doppler parameters, color M-mode mitral propagation velocity, and BNP levels. Further large-scale controlled studies are needed to determine the safety and possible long-term complications of this approach in HD patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.