
Abstract
Venlafaxine is commonly used in the United States for approved and non-Food and Drug Administration–approved indications in adults. It is used off-label to treat children for psychiatric diagnoses. The aim of the study was to describe venlafaxine toxicities in children and to identify the venlafaxine dose per weight that correlates with toxicities. An 11-year retrospective study of venlafaxine ingestion in children was performed using the California Poison Control System (CPCS) database. Data was extracted from phone calls received by CPCS clinicians and follow-up phone calls made to assess the patient’s progress in a health-care setting. Inclusion criteria were venlafaxine ingestion cases reported to CPCS between January 2001 and December 2011, children aged 20 years and under, venlafaxine as the only ingested substance, managed in a health-care facility, and followed to a known outcome. Two hundred sixty-two cases met the study criteria. Common presentations included gastrointestinal (14.9%), altered mental status (13.7%), and tachycardia (13.4%). The majority of the cases resulted in no effect (51.5%) or minor effect (19.9%). The average estimated dose per weight was 18.3 mg/kg in all patients and 64.5 mg/kg in those experiencing moderate-to-severe adverse effects. Seizures occurred in only 4 of the 262 cases at doses ranging from 1500 to 7500 mg. Although the estimated dose per weight exceeded 10 mg/kg for the majority of the cases, only 12 cases resulted in moderate or severe outcomes. The majority of venlafaxine ingestion cases in children resulted in either no clinical effects or minor clinical effects.
Introduction
Serotonin–norepinephrine reuptake inhibitors (SNRIs) marketed in the United States are a class of neuropsychiatric medications with a wide spectrum of indications. Venlafaxine, the first SNRI approved by the Food and Drug Administration (FDA) in 1993, is approved for the treatment of adult patients diagnosed with major depressive disorder, generalized anxiety disorder, panic disorder with or without agoraphobia, and social phobia. 1 Some other non-FDA–approved indications include attention-deficit hyperactivity disorder (ADHD), binge eating disorder, bipolar disorder-depressed phase, diabetic neuropathy, menopausal flushing, obsessive–compulsive disorder, posttraumatic stress disorder, and premenstrual dysphoric disorder. 2,3 The safety and efficacy of venlafaxine are not established in children. It is used off-label in this population to treat children diagnosed with depression, ADHD, and/or anxiety disorders. 1,4 –7
Venlafaxine is associated with a wide variety of adverse drug reactions (ADRs). 8 Gastrointestinal ADRs include nausea (37%), constipation (15%), vomiting (6%), diarrhea (8%), and dyspepsia (5%). Central nervous system ADRs include headache (34%), dizziness (16%), somnolence (14%), insomnia (11% to 25%), fatigue (11%), and nervousness (9%). Venlafaxine is associated with cardiovascular ADRs including sustained hypertension (10–15 mm of mercury (mmHg)) and arrhythmias. 8,9 Additionally, dose-related increases in heart rate (HR) by 3–8 beats per minute (b/min) are possible with venlafaxine ingestion.
A review of 235 patients aged from 27 to 43 years who had ingested venlafaxine (median dose: 1500 mg; interquartile range: 919–2800 mg) found that most common toxic effects were tachycardia (40.0%), hypertension (28.4%), and mydriasis (36.6%). Corrected QT prolongation (QTc > 450 ms) occurred in 7 men (11.1%) and 17 women (10.5%). 10 Transient arrhythmias were a rare effect, occurring in only three patients. The review reported a positive correlation between the quantity of venlafaxine ingested and HR.
Many venlafaxine poisonings in adults are documented in the form of case reports and reviews. 9 –20 A number of adult overdoses (dosage range of 5–8.4 g) have resulted in serious toxicities.
Greater venlafaxine ingestions (12.75 and 14.7 g) in adults resulted in deaths. 16,21 The threshold dose for severe and potentially life-threatening overdoses in adults is 1500 mg as these doses have been associated with seizures. Overdoses of greater than 8000 mg precipitate PR, QRS, and QT prolongation that can trigger ventricular tachycardia and cardiac arrest. 22 Additionally, as described above, signs and symptoms of serotonin syndrome such as autonomic instability and encephalopathy can manifest with overdose.
The reports of toxicity with venlafaxine are mostly in adults. Toxicities in children have not been reported on extensively. An overdose of 7200 mg venlafaxine extended release (XR) in a case of a 13-year-old girl resulted in a brief, self-limited, generalized tonic–clonic seizure approximately 1 hour (h) after ingestion. She presented to the emergency department (ED) 90 min after ingestion with dilated pupils, temperature of 97.5 F, pulse of 142 b/min, 14 r/min, and blood pressure (BP) of 98/75 mmHg. In the ED, she experienced two additional seizures, with her last one treated with lorazepam 2 mg intravenously. After activated charcoal was administered and 3.5 h after ingestion, she continued to have dilated pupils and mild sinus tachycardia with a HR of 115 b/min. 23
The primary goal of this study was to summarize CPCS data in children who have ingested venlafaxine. Due to the off-label use of this medication in children and also the potential for accidental ingestion, understanding the effect of venlafaxine in the pediatric population is essential. In adults, venlafaxine ingestion greater than 10 mg/kg usually results in hospital referrals per CPCS protocols. It is generally recognized that ingestion of doses less than 5.5 mg/kg in children is unlikely to result in toxicity. 22 However, this research group wanted to assess whether this tentative toxicity threshold in children was consistent with their observations among a large number of cases in the CPCS database. The aim of the study was to describe toxicities in children who have ingested venlafaxine and to identify the venlafaxine dose per weight that correlates with severe toxicities.
Materials and methods
Data source and study population
The CPCS database was queried to gather patient data for this study. This retrospective review examined phone calls made to CPCS regarding children during an 11-year time span from January 2001 to December 2011. Data was extracted from phone calls taken by clinicians at CPCS and follow-up calls made to and from CPCS to assess the patient’s progress after being taken to a health-care setting.
Institutional Review Board (IRB) approval was obtained from the University of California San Francisco Committee on Human Research. All cases were blinded prior to analysis to protect patient identifier information. Only researchers identified in the IRB proposal had full access to the blinded data. All researchers completed a National Institutes of Health human subjects training program. The study was performed in accordance with the ethical standards of the Declaration of Helsinki.
Inclusion criteria were as follows: (1) venlafaxine ingestion cases reported to CPCS between January 2001 and December 2011, (2) age less than 20 years, (3) venlafaxine as the only ingested substance, (4) managed in a health-care facility, and (5) case followed to a known outcome or judged as non-toxic. Twenty years of age was selected as the cutoff for inclusion age since it marks the end of teenage years, and according to the World Health Organization, 10- to 19-year-olds are considered adolescents. Exclusion criteria were as follows: (1) persons aged 20 years and older, (2) venlafaxine cases with missing doses, (3) multiple drug ingestions in the last 24 h, (4) cases with multiple persons involved in the ingestion scenario since it would be difficult to quantify each person’s ingestion, (5) unable to follow cases, (6) unrelated cases, and (7) confirmed non-exposure cases.
There were 704 SNRI single-substance exposure cases reported to the CPCS between 2001 and 2011. Of these, 394 (56%) involved venlafaxine ingestion, 141 (20%) duloxetine, 141 (20%) milnacipran, and 28 (4%) desvenlafaxine. Figure 1 summarizes the reasons for exclusion such that the final database consisted of 262 patients with 121 of those cases not having a reported weight. For patient cases that did not have recorded weights in the CPCS data, Center for Disease Control and Prevention (CDC) growth charts from the year 2000 were used to estimate weights based on 50th percentile weight reporting with respect to gender and height. 24

Venlafaxine case calls to CPCS from January 2001 to December 2011. CPCS: California Poison Control System.
Data collection
Age, gender, drug formulation (immediate-release vs. extended-release), dose (mg/kg), time from venlafaxine ingestion to poison center notification (min), use of single-dose–activated charcoal (SDAC), other treatment modalities, symptoms, and CPCS-determined case outcomes were recorded from each case. Exposure amounts were estimated maximum amounts based upon available or missing number of pills as reported to the CPCS clinician by the person who called into the poison center.
The CPCS clinician, to whom the case was reported, determined the severity of the outcome of the cases. Poison center clinicians categorize each followed case outcome as “no effect,” “minor,” “moderate,” and “major effect” using American Association of Poison Control Centers (AAPCC) defined case outcomes. AAPCC defined outcomes categories are as follows: “No effect”—The patient developed no symptoms as a result of the exposure. “Judged as non-toxic–expect no effect”—The poison specialist did not follow the patient to a known outcome but does not expect an effect (i.e., an accidental therapeutic ingestion). “Minor”—Symptoms developed which are minimally bothersome to the patient, usually resolve rapidly and usually involve skin or mucous membranes (e.g. lethargy, drowsiness, nausea, and vomiting). “Moderate”—Symptoms are more pronounced, more prolonged, or more of a systemic nature than minor symptoms (e.g. electrocardiogram (ECG) changes or diaphoresis). “Major”—Symptoms are life-threatening/death or resulted in significant residual disability or disfigurement (e.g. seizures and death).
Data analyses
All statistical analyses were conducted using STATA version 12 (StataCorp Inc., College Station, Texas, USA). Descriptive statistics were used to analyze the data. Continuous data were reported as mean ± standard deviation, and categorical data were reported as numbers, frequency, and percentages.
Results
From the 394 cases of venlafaxine ingestion in children reported to the CPCS between 2001 and 2011, 132 (33.5%) were excluded and 262 (66.5%) were included (Figure 1). The excluded cases were (1) those who could not be followed up (n = 63), (2) the patient had ingested multiple drugs/coingestants (n = 38), (3) cases with multiple persons involved in the ingestion scenario (n = 18), (4) unrelated problem (n = 11), and (5) confirmed non-exposures (n = 2).
Table 1 describes the baseline characteristics of the cases that were included in the study. The patient ages ranged from 7 months to 19 years, with the majority of the patients being female (n = 170, 64.9%). The average dose per weight was estimated to be approximately 18.3 mg/kg in all patients. In 56.1% of the patients, the estimated dose per weight exceeded the 10 mg/kg toxic threshold. The majority of the cases included in the study resulted in either no effect (51.5%) or minor effect (19.9%). Table 2 summarizes the classification of the severity of the cases by the CPCS clinicians.
Baseline characteristics of 262 venlafaxine cases called into the CPCS from January 2001 to December 2011.a

CPCS: California Poison Control System; SD: standard deviation; SDAC: single-dose–activated charcoal.
a N = 262.
Case outcomes as determined by CPCS clinicians.a
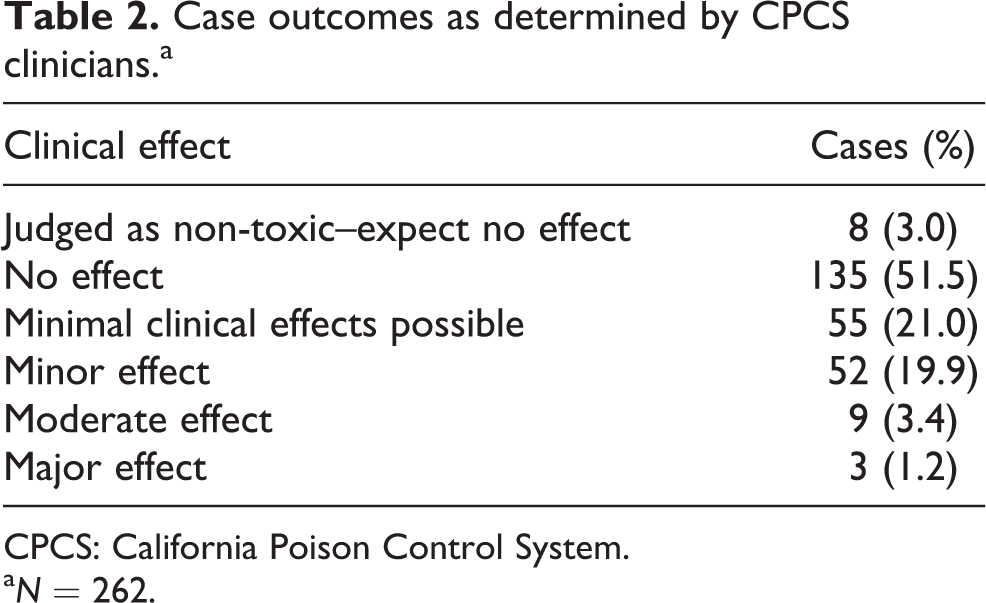
CPCS: California Poison Control System.
a N = 262.
Vital signs were typically reported when out of range (Table 3). For example, from the 142 cases that had HRs reported, 104 cases had a HR greater than or equal to 100 b/min, 46 cases had a HR greater than or equal to 120 b/min, and 4 cases had a HR greater than or equal to 160 b/min. The average HR (111 ± 23) and respiratory rate (23 ± 7) were elevated. BP was greater than 140/90 in 5% of the cases, with normal average systolic BP 123 ± 19 and diastolic BP 71 ± 16.
Recorded vital signs in cases where data were reported.a

SD: standard deviation; O2: oxygen; b/min: beats per minute; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; BP: blood pressure.
a N = 262.
Table 4 lists the toxicities recorded by the CPCS clinician. Most common observations were gastrointestinal (nausea, vomiting, and abdominal pain) and altered mental status (lethargy/drowsy, somnolence, agitation/irritation, nervousness, and confusion). Lethargy/drowsy (n = 26, 9.9%), vomiting (n = 20, 7.6%), and nausea (n = 16, 6.1%) were the most prevalent. It is important to note that four children (1.5%) experienced the serious effect of seizures.
Clinical presentations of venlafaxine oral ingestion in children.a

a N = 262.
The majority of cases (10 out of 12 cases) classified as moderate effect or major effect by CPCS occurred in teenagers (Table 5). Table 5 describes the outcomes of each of the 12 cases classified as having either moderate effect or major effect by the CPCS clinician. Sometimes, additional information was recorded in each case that was not present as objective data within the case. These data are represented in the last column of Table 5 as additional ADRs. For example, although the BP recorded for the 13-year-old female described in Table 5 was 135/84, there was an additional comment within the case that the patient experienced hypotension. This may have occurred at some time during the inpatient facility stay.
Outcomes for cases classified as moderate or major effect by CPCS clinician.a

CPCS: California Poison Control System; Sz: seizure; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; RR: respiratory rate; N/V: nausea/vomiting; ADRs: adverse drug reactions; F: female; M: male; b/min: beats per minute.
aMean dose ± SD = 2853 ± 3064 mg and mean dose per weight ± SD = 64.4 ± 58.5 mg/kg.
Discussion
Even though a majority of the cases (147, 56.1%) resulted in an exposure of greater than 10 mg/kg, over 50% of the cases were classified as having no clinical effect by the CPCS clinician (Tables 1 and 2). Only 12 (4.5%) out of the 262 cases considered were classified by the CPCS clinicians as resulting in moderate (nine cases) and major (three cases) effects (Table 5). The estimated dose per weight was less than 5.5 mg/kg in only two of these cases, and in one of these cases, weight was unavailable and estimated using CDC data. Of significance is that in the moderate and severe cases the mean estimated dose was over 2 gm (2853 ± 3064 mg) and the mean estimated dose per weight was well over the 10 mg/kg threshold (64.4 ± 58.5 mg/kg). Given these findings, perhaps the 5.5 mg/kg estimation commonly cited in the literature for venlafaxine toxicity threshold in pediatrics is rather conservative.
In 4 of the 12 cases classified as moderate and major effect, the exposed patient felt nausea/vomiting. In 3 of the 12 cases, the patient felt sleepy or drowsy. The more serious toxicity of experiencing seizures occurred in 4 of the 262 cases (1.5%) at doses of 1500, 1800, 2250, and 7500 mg. Although eight cases of mydriasis (3.0%) were reported in total, only one case of mydriasis was reported within the moderate or severe effect cases. The majority of the 12 cases had HRs well above 100 b/min. However, it is important to note that pediatrics commonly have higher HRs than the adults’ normal range of 60–100 b/min, sometimes ranging up to 190 b/min in newborns and 160 b/min in infants. 25,26 In this study, the case of the 19-year-old male who experienced a major clinical effect after consuming 7500 mg of venlafaxine somewhat resembles the case of the 13-year-old girl reported in the literatures with an ingestion of 7200 mg, as both teenagers experienced seizures subsequently. 23
Many of the children exposed to venlafaxine demonstrated similar effects as expected in adults such as nausea, vomiting, tachycardia, and somnolence. Nausea and vomiting occurred in 6.1% and 7.6% of the children, respectively. In adults, nausea is more prevalent (37%) and vomiting occurs in about 6%. 8 Lethargy/drowsiness occurred in approximately 10% of the pediatrics, whereas it is observed in around 14% of adults. The discrepancies in prevalence of effects among children and adults may be due to a number of reasons. Children may have difficulty in expressing their symptoms, especially during an accidental exposure or overdose. Additionally, documentation may not be all comprehensive since it was based on reports to the CPCS clinician.
In contrast to the adult data, however, no ECG changes were reported in the cases considered. When ECG results were available, they were marked as normal. Also, unlike the reports of adult overdoses in the literatures, none of the 262 pediatric cases called in resulted in fatality. The maximum pediatric venlafaxine dose in this study was 9 g, and the doses resulting in fatalities in adults were above 10 g. 16,21 In contrast to many of the adult reports that include plasma concentrations along with dose or dose per weight, peak plasma levels were not available for the children in this study through the CPCS. 21,27
Although this study aimed to provide a more thorough description of cases of venlafaxine ingestion in pediatrics, it is not without limitations. As stated previously, around one-third of the cases of venlafaxine ingestion in pediatrics that was reported to the CPCS between 2001 and 2011 did not meet criteria for the study for various reasons (Figure 1). Including these cases would have resulted in a more comprehensive description. Also, this study was retrospective in nature, many variables could not be controlled for within the study, and data were not collected with the objectives of this study in mind. The exact dosage of medication taken was typically reported by family members and estimated at best. Conclusions cannot be made based on peak plasma levels for either venlafaxine or o-desmethylvenlafaxine, as this information was not provided. Vital signs and toxicity effects, when collected, were reported to CPCS rather than reviewed directly. Additionally, CPCS outcomes were set at the time of call by the clinician and could not be independently verified after the fact. It is important also to note that correlation does not guarantee causation. For example, it is unclear and difficult to tease out whether nausea/vomiting reported (Table 4) was due to venlafaxine adverse effects, the use of SDAC, or inherent patient characteristics. Another limitation is that all children up to 20 years of age were grouped broadly together. Since the outcomes of cases were categorized by the CPCS clinicians, it was assumed that difference in enzymatic pathways for metabolism between pediatric groups, such as neonates, infants, toddlers, children, and adolescents, was taken into account when the severity of outcomes classifications was made. It should be noted that ages were specifically reported in Table 5 for the moderate and major outcomes.
The majority of venlafaxine ingestion cases in children up to 20 years old that were reported to the CPCS between 2001 and 2011 resulted in either no clinical effects or minor clinical effects. Only a handful of cases resulted in more severe adverse effects such as seizures (1500, 2250, 1800, and 7500 mg). The findings of this study can be useful for clinicians when anticipating effects in pediatric patients presenting with accidental venlafaxine ingestion. This data can improve clinical decision making in pediatric overdoses or accidental ingestion scenarios.
Footnotes
Acknowledgement
The authors would like to thank John F. Inciardi, PharmD, DSc, for his initial review of statistics.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.