
Abstract
The second-generation selective 5-HT2 receptor antagonists and reuptake inhibitors (SARIs) class antidepressants are known to have fewer cardiovascular side effects than the older ones. However, several case reports showed that trazodone, one of the second-generation SARIs, induces QT prolongation, cardiac arrhythmia, and ventricular tachycardia. Although these clinical cases suggested trazodone-induced cardiotoxicity, the toxicological actions of trazodone on cardiac action potentials (APs) beyond the human ether-a-go-go related gene (hERG) remain unclear. To elucidate the cellular mechanism for the adverse cardiac effects of trazodone, we investigated its effects on cardiac APs and ion channels using whole-cell patch clamp techniques in human-induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CMs) and transiently transfected human embryonic kidney cells (HEK293) with cardiac ion channel complementary DNA. Trazodone dose-dependently decreased the maximum upstroke velocity (Vmax) and prolonged the AP duration, inducing early after depolarizations at 3 and 10 μM that triggered ventricular arrhythmias in hiPSC-CMs. Trazodone also inhibited all of the major ion channels (IKr, IKs, INa, and ICa), with an especially high inhibitory potency on hERG. These data indicate that the prolonged AP duration and decreased Vmax due to trazodone are mainly the result of hERG and sodium ion inhibition, and its inhibitory effects on cardiac ion channels can be exhibited in hiPSC-CMs.
Introduction
Depressive disorders acting on the autonomic neurocardiac system may occur in patients with heart disease and are associated with cardiovascular mortality. 1 –4 First-generation antidepressants, such as tricyclic antidepressants (TCAs) were demonstrated to have fewer cardiovascular side effects; however, their broad mechanisms of action led to unwanted ventricular arrhythmias and sudden cardiac death, resulting in their removal from the market. 5,6 To overcome the cardiotoxicity of first-generation antidepressants, second-generation antidepressants, such as selective serotonin reuptake inhibitors 7 –9 and the selective 5-HT2 receptor antagonists and reuptake inhibitors (SARIs), which simultaneously act as postsynaptic serotonin receptor antagonists and presynaptic serotonin reuptake inhibitors, 10 –12 were introduced. These drugs are as effective as TCAs, but have higher safety and tolerability profiles. Thus, they are preferred over first-generation antidepressants.
Although trazodone, a tetracyclic SARI, is known to have fewer cardiovascular side effects than TCAs, 13 an increasing number of trazodone studies have raised concerns regarding its cardiac safety. Several previous studies showed that trazodone inhibits human ether-a-go-go related gene (hERG) channels by interacting at the aromatic binding site of Y652 and F656 in the S6 domain of hERG. 14,15 Trazodone also inhibits outward potassium ion (K+) channels, which includes transient outward K currents and transiently, rapidly inactivating (voltage-gated potassium) Kv channels . 16,17 In addition, trazodone was reported to cause QT prolongation and torsade de pointes at both therapeutic doses 18,19 and overdose levels. 20,21 Although the likely mechanism for drug-induced long QT syndrome (LQTS) is the interaction of trazodone with KCNH2-encoded hERG K channels, 15,22 additional genes associated with LQTS can also cause life-threatening cardiac arrhythmias. 23 Mutations in genes encoding cardiac ionic channels can disrupt the fine balance of ionic currents that shape the action potential (AP) and may lead to life-threatening arrhythmias. For example, mutations to the KCNQ1/KCNE1-encoded slow component of the delayed rectifying K current (IKs) channel, KCNH2-encoded rectifier potassium (IKr) channel, and SCN5A-encoded inward sodium (Na) current (INa) channel can cause LQT1 or LQT5, LQT2 or LQT6, and LQT3, respectively. 24 –26
Cardiac electrophysiological assessment of the SARI trazodone is necessary to identify the mechanisms underlying its cardiovascular side effects; however, the effect of trazodone on cardiac APs, mediated by depolarization and repolarization via ion channels, remains unclear. To elucidate the cellular mechanism of trazodone-induced cardiac adverse events, we investigated the effects of trazodone on electrophysiological cardiac characteristics using the whole-cell patch clamp technique. We evaluated the effect of trazodone on APs in human-induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CMs), which express the major cardiac ion channels and recapitulate spontaneous mechanical and electrical activity similar to adult cardiomyocytes. 27 –30 We further evaluated the effect of trazodone on major ion channels, including IKr, IKs, and INa, in human embryonic kidney (HEK293) cells overexpressing single ion channels and calcium ion (Ca+) current (ICa) in hiPSC-CMs. The results of these assays provide a cardiac electrical basis for trazodone cardiotoxicity and shed light on the cardiac risk potential of trazodone beyond the current gold standard assay for hERG.
Methods
Cell culture
hiPSC-CMs (iCell Cardiomyocytes; Cellular Dynamics International, Madison, Wisconsin, USA) were cultured for single-cell electrophysiology recordings. Frozen vials of hiPSC-CM were thawed in a water bath maintained at 37°C and mixed with an ice-cold plating medium (iCell Cardiomyocyte Plating Medium). The cells were transferred to four-well culture plates containing 0.1% gelatin-coated glass coverslips. The cells were then maintained in a culture incubator at 37°C in an atmosphere of 93% air and 7% carbon dioxide. After 2 days of culture, the plating medium was replaced with the culture medium (iCell Cardiomyocyte Maintenance Medium). This medium was changed every 48 h. HEK293 cells were transiently transfected with cardiac major ionic channel cDNA using lipofectamine. The transfected cDNAs, including IKr (Kv11.1, KCNH2), IKs (KvLQT1 and minK, KCNQ1/KCNE1), and INa (Nav1.5, SCN5A) were tagged with green fluorescent protein.
Whole-cell patch clamp recordings in hiPSC-CMs
Whole cell hiPSC-CM recordings were performed at 37°C using an external solution containing (in mM): sodium chloride (NaCl), 145; potassium chloride (KCl), 5.4; (4-2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES), 10; magnesium chloride (MgCl2), 3.5; glucose, 5; calcium chloride (CaCl2), 1.8; 4-aminopyridine (4-AP), 2; and tetrodotoxin (TTX), 0.01. The internal solution contained (in mM): Cs-Asp (cesium aspartate), 120; cesium chloride, 20; NaCl, 5; tetraethylammonium chloride, 10; HEPES, 10; ethylene glycol tetraacetic acid (EGTA), 10; and magnesium adenosine triphosphate (Mg-ATP), 5. We recorded typical APs of the hiPSC-CMs in the current-clamp mode. Spontaneous beating activity of single hiPSC-CMs were recorded and only hiPSC-CMs that could beat stably were included in the analysis. Following stabilization of the AP waveforms, the average from five recorded APs was analyzed for each test concentration. In the voltage-clamp mode, a standardized step protocol was used to elicit the major cardiac calcium ion (Ca2+) currents (ICa). To elicit ICa in hiPSC-CMs, the cells were held at −40 mV and depolarized to 0 mV for 300 ms. The ICa was isolated by eliminating the fast Na and K currents with TTX and 4-AP in the external solution.
Whole-cell voltage-clamp recordings in HEK293 cells
IKr, IKs, and INa currents were recorded with whole-cell voltage clamps using normal Tyrode’s solution. The extracellular solution for recording the IKr, IKs, and INa contained (in mM): NaCl, 143; KCl, 5.4; HEPES, 5; monosodium phosphate, 0.33; MgCl2, 0.5; glucose, 10; and CaCl2, 1.8 (pH was adjusted to 7.40 using sodium hydroxide (NaOH)). The internal solution for IKr contained (in mM): KCl, 130; EGTA, 5; HEPES, 10; MgCl2, 1; and Mg-ATP, 5 (pH was adjusted to 7.25 using potassium hydroxide (KOH)). The internal solution for IKs contained (in mM): KCl, 150; EGTA, 5; HEPES, 10; MgCl2, 2; CaCl2, 1; and Na2-ATP, 5 (pH was adjusted to 7.25 with KOH). The internal solution for INa contained (in mM): cesium fluoride, 105; NaCl, 35; EGTA, 10; and HEPES, 10 (pH was adjusted to 7.25 using NaOH). A standardized step protocol was used to elicit major cardiac ion currents (IKr, IKs, and INa). The cells were held at −80 mV and depolarized to +20 mV for 2 s, followed by repolarization for 2 s to −40 mV to activate hERG tail currents. To elicit IKs, a −80 mV holding potential was used, followed by a 2 s depolarization to +60 mV, followed by a repolarization step to −20 mV for 2 s. To elicit INa, the cells were held at −100 mV and depolarized to −40 mV for 50 ms. Ionic current amplitudes normalized for membrane capacitance are represented as pA/pF to simulate current density values and to compensate for differences in cell size.
Statistical analysis of data
pCLAMP (Axon Instruments, Foster City, California, USA), Origin 8 (OriginLab Corp, Northampton, Massachusetts, USA), and Excel (Microsoft, Redmond, Washington, USA) software were used for data acquisition and analysis. The concentration–response relationships for drug-induced blockage were calculated using SigmaPlot (Systat Software, San Jose, California, USA). The half-maximal inhibitory concentration (IC50) value, defined as the drug concentration that reduced the ionic currents by 50%, was obtained using the sigmoidal Hill equation:
Results
Effects of trazodone on AP waveforms in hiPSC-CMs
To assess whether the changes in cardiac AP properties were due to the effect of trazodone, we obtained current-clamp recordings in hiPSC-CMs (Figure 1). A spontaneous beating activity was recorded and AP-related parameters were quantified as the control condition in hiPSC-CMs (n = 21). The maximum diastolic potential (MDP), maximum upstroke velocity (Vmax), total amplitude (TA), AP duration at 90% (APD90), and at 60% (APD60) waveforms were analyzed and only ventricular CMs that had an AP duration longer than 300 ms were included in the analysis. The representative AP traces in control conditions and in the presence of trazodone are shown in Figure 1(a). The average from five recorded APs was analyzed at each test concentration and dose–response studies indicated that APs were completely inhibited after treatment with 100 μM trazodone (n = 3, data not shown). Trazodone prolonged APD90 and APD60 at 3 μM and early after depolarizations (EADs) were induced by 10 μM trazodone, suggesting that trazodone affects the AP waveforms of hiPSC-CMs in a concentration-dependent manner (Figure 1(a)). The AP-related parameters showed no significant effect from trazodone on the MDP and TA (n = 5, Figure 1(b) and (d)); however, a dose-dependent dramatic decrease in Vmax was caused by trazodone (n = 5, Figure 1(c)). Further, trazodone prolonged the APD and induced EADs in a concentration-dependent manner (n = 5, Figure 1(e) and (f)). These results demonstrated that trazodone significantly reduced AP Vmax prolonging their 90% and 60% durations.
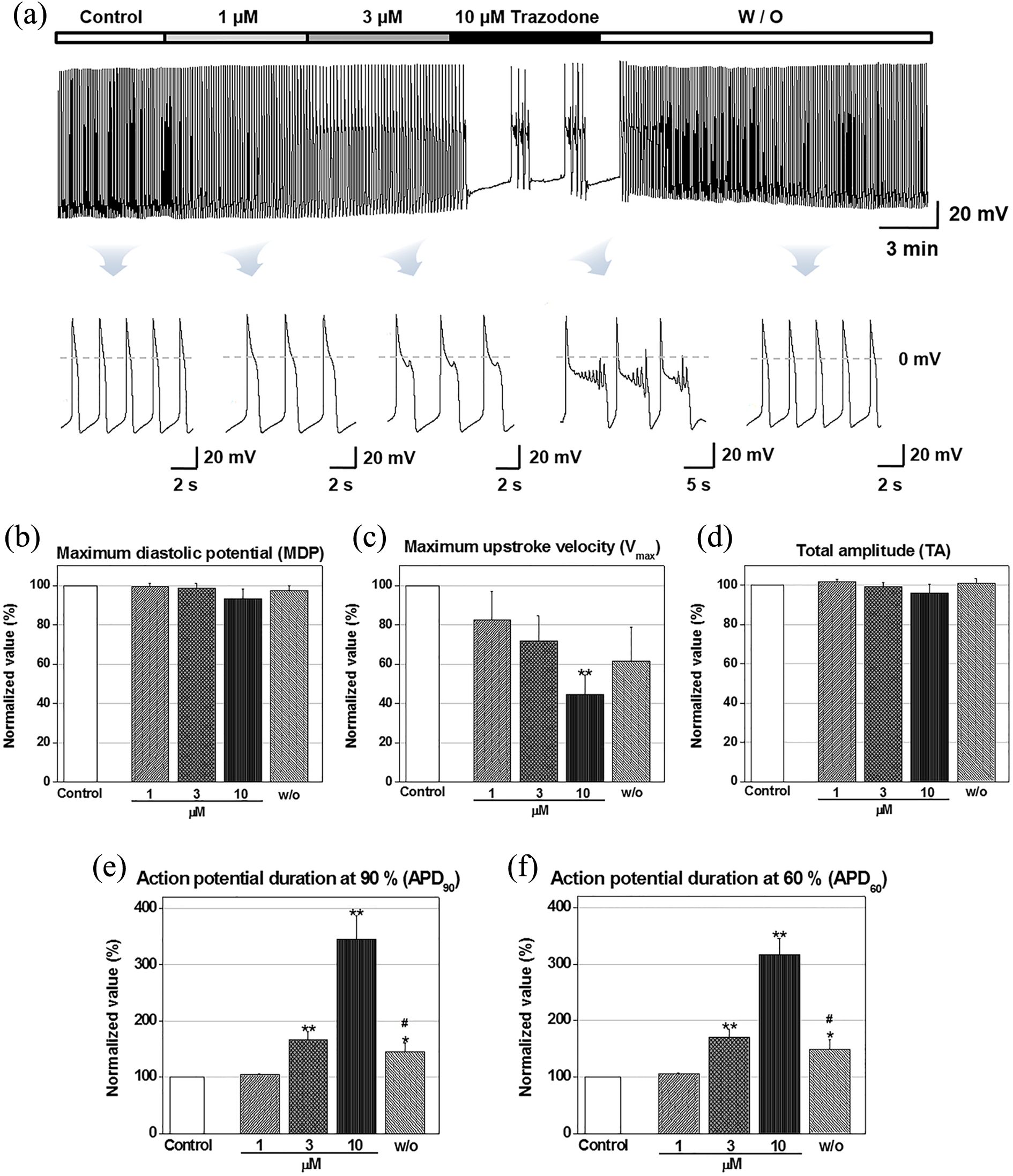
Cardiac actions of the SARI trazodone on action potential waveforms in hiPSC-CMs. (a) Representative traces induced by 1 μM trazodone. Representative traces show the typical waveform of EAD induced by 3 and 10 μM trazodone. (b) to (f), Normalized AP parameters in control and in the presence of trazodone. MDP: maximum diastolic potential; Vmax: maximum upstroke velocity; TA: total amplitude; APD90: action potential duration at 90% repolarization; APD60: action potential duration at 60% repolarization (mean ± SEM, *p < 0.05, **p < 0.01); SARI: selective 5-HT2 receptor antagonists and reuptake inhibitor; hiPSC-CM: human-induced pluripotent stem cell-derived cardiomyocyte; EAD: early after depolarization; AP: action potential.
Effects of trazodone on cardiac repolarization-related currents: IKr and IKs in HEK293
To investigate the cellular mechanism underlying the effects of trazodone on repolarization-related currents, KCNH2-encoded fast components of the delayed IKr current and KCNQ1/KCNE1-encoded slow components of the delayed rectifier K current (IKs) were recorded using voltage-clamp recordings in HEK293 cells. The fast and slow components of the K channel-specific outward currents (IKr and IKs, respectively) were activated by each step protocol. Trazodone inhibited the IKr peak amplitude in a concentration-dependent manner (Figure 2(a)) and produced a high affinity for IKr with an IC50 value of 2.83 ± 0.04 μM (Figure 2(b), n = 3). Ten micromoles of trazodone (Figure 2(c)) completely blocked the peak IKr current density, but it did not affect the activation- and inactivation-state I-V relationships (Figure 2(d) and (e), n = 3). Trazodone also inhibited the peak amplitude of IKs in a concentration-dependent manner (Figure 3(a)), but had a low affinity for IKs with an IC50 value of 67.5 ± 0.05 μM (Figure 3(b), n = 3). Trazodone at 300 μM completely blocked the peak IKs current density but did not affect the I-V relationships (n = 3, data not shown). These results indicated that trazodone has a higher inhibitory potency on IKr than IKs in HEK293.

Effect of the SARI trazodone on IKr in HEK293. (a) Representative traces demonstrating the effect of trazodone on HEK293 IKr at doses of 0.1, 0.3, 1, 3, and 10 μM, respectively. (b) Dose–response relationship of trazodone, providing an IC50 value of 2.83 ± 0.04 μM (mean ± SEM). (c) Representative I-V traces of IKr in control cells (top) and in the presence of trazodone (bottom). (d) Activation-state I-V relationships of IKr in control and in the presence of trazodone (mean ± SEM, *p < 0.05, **p < 0.01). (e) Inactivation-state I-V relationships of IKr in control and in the presence of trazodone (mean ± SEM, *p < 0.05, **p < 0.01). SARI: selective 5-HT2 receptor antagonists and reuptake inhibitor; IC50: half-maximal inhibitory concentration; I-V: current–voltage.

Effect of the SARI trazodone on IKs in HEK293. (a) Representative traces demonstrating the effect of trazodone on HEK293 IKs at doses of 1, 3, 10, 30, 100, and 300 μM, respectively. (b) Dose–response relationship of trazodone, providing an IC50 value of 67.5 ± 0.05 μM (mean ± SEM). SARI: selective 5-HT2 receptor antagonists and reuptake inhibitor; IC50: half-maximal inhibitory concentration.
Effects of trazodone on cardiac depolarization-related currents: INa in HEK293 and ICa in hiPSC-CMs
To investigate the effect of trazodone on the depolarization-related currents, the SCN5A-encoded inward Na current (INa) was recorded in HEK293 and the Ca2+-specific inward current (ICa) was recorded in hiPSC-CMs. Trazodone inhibited the peak amplitude of INa in a concentration-dependent manner (Figure 4(a)) but produced a slightly high affinity for INa with an IC50 value of 11.07 ± 0.09 μM (Figure 4(b), n = 4). Trazodone at 100 μM completely blocked the peak INa current density but did not affect the I-V relationships (n = 3, data not shown). We verified the ICa of hiPSC-CMs using a selective Ca2+ channel antagonist, nifedipine, which inhibited the peak amplitude of ICa in a concentration-dependent manner with an IC50 value of 0.84 μM (n = 4, data not shown). Trazodone inhibited the ICa peak amplitude in a concentration-dependent manner (Figure 5(a)) but showed a low affinity for ICa with an IC50 value of 19.05 ± 0.13 μM (Figure 5(b), n = 3). Trazodone at 300 μM completely blocked the peak ICa current density, but it did not affect the I-V relationships (n = 4, data not shown). These results indicated that trazodone is more effective in inhibiting INa in HEK293 than ICa in hiPSC-CMs.

Effect of the SARI trazodone on INa in HEK293. (a) Representative traces demonstrating the effect of trazodone on HEK293 INa at doses of 1, 3, 10, 30, and 100 μM, respectively. (b) Dose–response relationship of trazodone, providing an IC50 value of 11.07 ± 0.09 μM (mean ± SEM). SARI: selective 5-HT2 receptor antagonists and reuptake inhibitor; IC50: half-maximal inhibitory concentration.
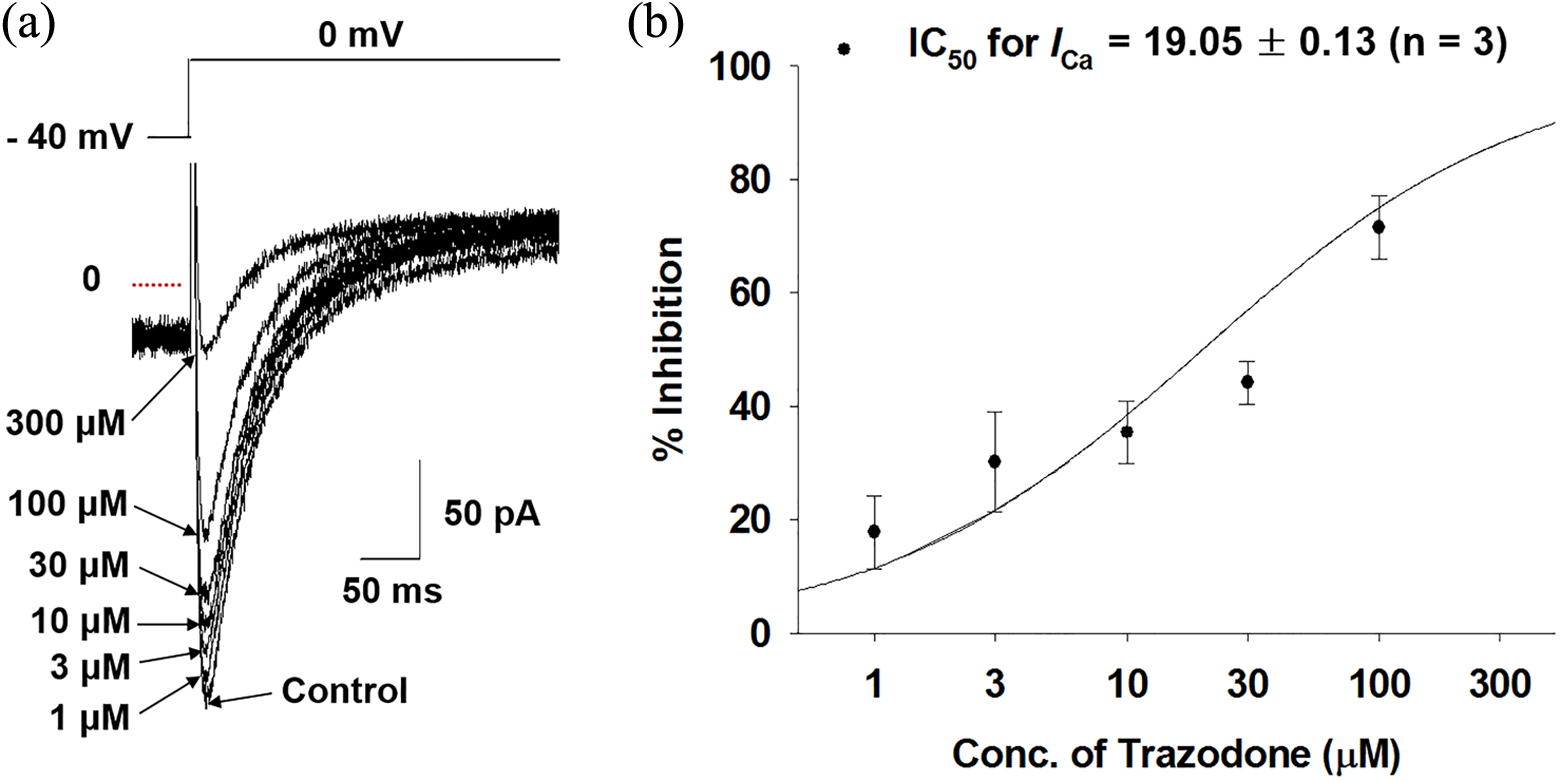
Cardiac actions of the SARI trazodone on ICa in hiPSC-CMs. (a) Representative traces demonstrating the effect of trazodone on hiPSC-CMs ICa at doses of 1, 3, 10, 30, 100, and 300 μM, respectively. (b) Dose–response relationship of trazodone, providing an IC50 value of 19.05 ± 0.13 μM (mean ± SEM). SARI: selective 5-HT2 receptor antagonists and reuptake inhibitor; IC50: half-maximal inhibitory concentration; hiPSC-CM: human-induced pluripotent stem cell-derived cardiomyocyte.
Discussion
Most clinical studies using SARIs suggest that trazodone has significant advantages over first-generation antidepressants; however, recent studies indicate that trazodone may have cardiovascular side effects. 18 –21 Several clinical studies suggest that cardiotoxicity is induced via trazodone acting on hERG channels, which are involved in cardiac repolarization, thereby inducing QT prolongation and ventricular arrhythmias. 15,22 Although it is widely accepted that ventricular arrhythmias are primarily caused by IKr inhibition, drug-induced inhibition of IKr does not show a clear correlation with QT prolongation risk and the occurrence of arrhythmias. 31 Thus, further studies are required to evaluate whether trazodone affects cardiac APs during ion channel depolarization or repolarization beyond the hERG.
In this study, we hypothesized that trazodone modulates cardiac APs, which is controlled by interactions between depolarizing (INa and ICa) and repolarizing (IKr and IKs) ion channels, including the hERG channel. Our cardiac electrophysiological studies demonstrated that trazodone modulated the AP waveforms of hiPSC-CMs by dose dependently inducing APD90 and APD60 prolongation and decreasing Vmax, without changing the MDP and TA. Trazodone completely inhibited APs at 100 μM (data not shown) and EADs were induced at 10 μM (Figure 1). As in previous studies, our results indicated that trazodone inhibited the hERG channel (Figure 2). Moreover, other major cardiac ion currents, including IKs (Figure 3), INa (Figure 4), and ICa (Figure 5), were also dose dependently inhibited by trazodone.
One potential mechanism by which trazodone dose dependently prolongs APD90 (Figure 1(e)) is inhibition of repolarization-related K+ currents. Trazodone inhibited IKr with an IC50 value of 2.83 ± 0.04 μM and blocked hERG by about 80% at a dose of 10 μM (Figure 2(b)). Trazodone also inhibited IKs but had a lower inhibitory potency, and IKs inhibition was approximately 30% at 10 μM trazodone (IC50 > 10 μM, Figure 3(b)). The other possible mechanism by which trazodone dose-dependently prolongs APD60 (Figure 1(f)) is correlated with the activation of Ca2+ currents. Trazodone adversely inhibited ICa; however, its inhibitory potency on ICa was low; ICa inhibition was about 40% at 10 μM trazodone (IC50 > 10 μM, Figure 5(b)). The effects of trazodone on Vmax (Figure 1(c)), which is an indirect indicator of the fast Na+ channel, suggest that it potently inhibits INa. Trazodone had a slightly high inhibitory potency and blocked INa by about 50% at 10 μM (IC50 > 10 μM, Figure 4(b)). Although the net effect of trazodone on AP properties depends on the overall balance between inward and outward currents, the IC50 value of IKr was 30-, 5-, and 10-fold more potent than IKs, INa, and ICa, respectively. These results suggest that trazodone potently and dose-dependently inhibits cardiac voltage-dependent ion channels, with its greatest effect occurring on hERG.
Cardiotoxicity testing, including in vitro assays and in vivo animal models, is an important part of preclinical drug evaluation prior to first-in-human clinical trials; however, many drugs that have passed animal tests have unanticipated cardiotoxicity during clinical phases. 32 –34 Therefore, the development of a sensitive in vitro model suitable for cardiac safety testing is extremely important. The most well-known electrophysiological studies use immortalized mammalian cell lines overexpressing single ion channel; however, these are not representative of native human cardiomyocytes. Although the IC50 value of trazodone for IKr is important to gaining insight into the drug’s actions on APs, its additional inhibitory actions on Na+ and Ca2+ channels may exert other antiarrhythmic and proarrhythmic actions. Therefore, it is difficult to correlate in vitro IC50 values with the predictive arrhythmogenic properties of a drug.
Recently, hiPSC-CMs have been established as an attractive model for cardiac toxicity testing, as they express the major ion channels and recapitulate spontaneous mechanical and electrical activity, similar to adult cardiomyocytes. 27 –30 We evaluated the effect of trazodone on AP parameters in hiPSC-CMs, which is a physiologically relevant preclinical evaluation of drug-induced ventricular arrhythmias. Our findings indicated that hiPSC-CMs are sensitive and accurate predictors of trazodone-induced cardiotoxicity. Trazodone-induced prolonged APD may result from the complex interactions between Na+, Ca2+, and K+ currents, though its profound effect on ventricular APD may be related to its ability to regulate K+ channels. Although hiPSC-CMs have opened new horizons for drug screening and detecting undesired proarrhythmic side effects of preclinical drugs, 35 –37 they may still show gene expression profiles similar to immature human fetal cardiomyocytes. 38 –40 The electrophysiological properties of partially mature hiPSC-CMs have mixed subtypes and restricted functionality compared to human adult cardiomyocytes, which can limit their application in drug screening. 41 –43 To overcome this constraint, it will be crucial to develop a maturation protocol for hiPSC-CMs and verify and validate the obtained results in the initial screening steps.
Trazodone was developed as 150 mg and 300 mg caplets for once daily administration and known to be well absorbed after oral administration without selective localization in any tissue. 44 In a clinical setting, the plasma concentration of trazodone increases proportionally after administration of a single dose or under steady-state conditions. 45,46 Fagiolini et al. reported that plasma concentration (Cmax) of trazodone reached 1.2 μM after a single oral dose of 100 mg. Steady state Cmax of trazodone were 3.1 μM after administration of 100 mg three times a day, and 1.8 μM after 300 mg administration once daily for 1 week. 44 When compared with the potency of hERG inhibition (IC50, 2.83 μM), the Cmax overlaps with the ranges of inhibitory effects on hERG.
Collectively, our in vitro studies indicated that trazodone dose-dependently inhibits all of the major cardiac ion channels, including hERG. The prolonged APD and decreased Vmax due to trazodone are mainly the result of hERG and Na+ inhibition and hiPSC-CMs are sensitive models for detecting the repolarization and depolarization delay induced by trazodone. Our understanding of the cellular mechanisms of trazodone-induced cardiac toxicity may aid in preclinical trials, better dose selection, and reduction of unexpected, life-threatening cardiac arrhythmias.
Footnotes
Authors’ Note
These authors SL and HAL contributed equally to this work as first authors. The authors SJK and KSK contributed equally to this work as corresponding authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Ministry of Science, ICT & Future Planning (MSIP), Republic of Korea (No. NRF-2012M3A9C7050138).