
Abstract
Introduction:
Carbon monoxide (CO) is a colorless, tasteless, odorless, nonirritant gas and CO poisoning affects all organ systems.
Aim:
We aimed to detect any possible effects of CO exposure on the argyrophilic nucleolar organizing region (AgNOR)-associated protein synthesis of heart cells and whether there is any relationship between AgNOR protein amount and both carboxyhemoglobin (COHb) level and histopathological evaluation methods used for the detection of damage in heart tissue after CO exposure.
Materials and Methods:
The rats were divided into four groups (control, 1000, 3000, and 5000 ppm), each containing six rats. After CO intoxication, COHb levels were measured and the animals were killed on the 7th day. AgNOR staining was performed in the heart tissue. One hundred nuclei per rat were evaluated, and total AgNOR area/nuclear area and mean AgNOR number were analyzed for each nucleus. The CO exposure groups had significantly higher AgNOR values than the control group (p < 0.0001). According to cardiomyopathy (CMY) scoring methods, the differences between groups 3 and 4 and groups 1 and 2 were significant (p < 0.05). A significant positive correlation between AgNOR values and both CMY and COHb levels were detected.
Conclusion:
The detection of AgNOR protein amount may give information about the CMY levels and be used to detect the CO intoxication levels instead of COHb in later periods.
Introduction
Carbon monoxide (CO) is a colorless, tasteless, odorless, and nonirritant gas and is lighter than air. CO appears as an end product of incomplete combustion of carbon-containing fuels. CO is generated by smoking or using an oven, a stove, or a gas heater in places without suitable aeration and chimneys. 1,2 CO causes hypoxia in all tissues by decreasing both oxygen-carrying capacity of hemoglobin (Hb) and oxygen delivery of Hb at tissue level after passing through the lungs without leading to any damage in lung tissue. 1,3
Affinity of CO to Hb is approximately 200 times greater than that of oxygen, which causes relative hypoxia. In addition, CO also binds to myoglobin, aggravating hypoxia in heart tissue. Heart tissue may be affected by CO poisoning. 4
CO poisoning affects all organ systems (especially, neuropsychiatric and cardiovascular systems). 5 –7 Acute or chronic poisoning with CO may cause death. 2,3
The nuclear organizing region (NOR) is the site of the ribosomal genes that are located on the secondary constrictions of five pairs of acrocentric chromosomes and can be stained with silver when active. 8 Ribosomal RNA of the genes are located in the nucleolus during transcription by RNA polymerase I. Approximately 400 copies per diploid genome of human ribosomal DNA genes are associated in clusters of tandem repeat units on the short arms of the acrocentric chromosomes. 9 Therefore, AgNOR staining is one of the most reliable methods currently used to visualize nucleoli in interphase nuclei. 8 We carried out different studies to detect the importance of the interphase quantity of AgNOR in hair root cells of humans, 10,11 tumor pathology, 12,13 developmental stages of Down syndrome in infants, 14 possible effects of CO exposure on the NOR protein synthesis of lung cells, 15 and so on.
To the best of our knowledge, there are no studies in the literature about the relationship between AgNOR proteins and CO exposure in heart cells. Thus, we performed the current study to detect any possible effects of CO exposure on the NOR protein synthesis of heart cells and to analyze whether there is any relationship not only between AgNOR protein amount and COHb level but also between the AgNOR evaluation methods and histopathological evaluation methods used for the detection of damage in heart tissue caused by CO exposure.
Methods
Animals and experimental procedures
This study was performed at Atatürk University Pharmacology Laboratory, Turkey, in 2014, using 24 adult male albino Wistar rats weighing between 200 g and 230 g selected from the same breed. The Ethics Committee of Atatürk University (AU Ethics Committee Number: 2014-67) approved the study. The rats were cared for in accordance with the guide for the care and use of laboratory animals. The rats were provided with standard rat feed and tap water in rhythmically lighted (12-h light/12-h dark) rooms at a temperature of 22 ± 2°C.
Three steel tubes, each containing 10 L of CO–air mixture at three different concentrations (1000, 3000, and 5000 ppm) were taken from Habas Industrial and Medical Gases Production Industries Inc., Kocaeli, Turkey. Rats were exposed to CO in an enclosed transparent jar with dimensions of 20 × 40 × 60 cm3. There were an inlet and an outlet opening of 2 cm in diameter at opposite sides of the jar. The rats were divided into four groups, each containing six rats, as in the study performed by Colakoglu et al., as follows:
15
Group 1: control group; Group 2: 1000 ppm CO–air mixture; Group 3: 3000 ppm CO–air mixture; and Group 4: 5000 ppm CO–air mixture.
Each experimental group was exposed to CO in different densities (1000, 3000, and 5000 ppm) at a flow rate of 4 L/min for 30 min in the transparent jar. Then, rats were anesthetized with ketamine hydrochloride (50 mg/kg intraperitoneally; Ketalar; Parke-Davis, Eczacibasi, Istanbul, Turkey) and xylazine hydrochloride (3 mg/kg, intraperitoneally; Rompun; Bayer AG, Leverkusen, Germany), and blood samples for blood gas analysis were taken by performing right jugular vein catheterization (the venous catheter was tunneled subcutaneously and externalized at the nape of neck) in each group. The catheter was removed after blood sample was taken, and each rat was taken to a different cage.
One week after exposure to CO, the animals were anesthetized by administering ketamine hydrochloride + xylazine hydrochloride, intraperitoneally. For the surgical procedure, the animals were placed in the supine position, and the anterior thoracic wall was shaved and disinfected using 10% povidone–iodine solution. Thoracotomy was performed through a midline incision. Perfusion fixation was achieved by intracardiac administration of 10% formaldehyde solution and hearts of rats were taken. Samples were placed in 10% formaldehyde solution to make sure complete fixation was achieved.
Biochemical analysis
COHb level was calculated with blood gas analysis to determine the level of CO. The relationship between COHb level and cardiac injury was evaluated. Blood gas analysis was performed with ABL 800 (Radiometer, Carlsbad, California, USA) device using its own original commercial reactive substances.
Histopathological evaluation
For histopathological evaluation, the heart tissues were dissected and the tissue samples fixed in 10% buffered formaldehyde for 24 h, processed using a graded ethanol, xylene, and paraffin series, and embedded in paraffin. The paraffin sections were cut into 4 mm thick slices and stained with hematoxylin and eosin (HE) for light microscopic examination. The sections were viewed and photographed using a Nikon light microscope (Nikon Eclipse i80, Tokyo, Japan), with an attached photographic machine (Nikon DS-Fi1). Each specimen was scored for the degree of severity of histopathological changes as follows: myocardial fiber swelling and interstitial edema (+1); disorganization of myocardial fiber with or without fibroblastic proliferation (+1); myo-cytolysis/necrosis of myocardial fibers (+1); (D) myocardial fiber vacuolation (perinuclear vacuolation) (+1); and when no damage is noted (0) as it was done in the study performed by Saad et al. The above changes were judged as significant if seen in three or more high-power fields. The cardiomyopathy (CMY) severity scores were graded from 0 to 3: 0 represents no CMY, 1 represents mild CMY, 2 represents moderate CMY, and 3 or more represents severe CMY. In this study, we also evaluated the presence or absence of hemorrhage and nuclear enlargement (nucleomegaly), which were not evaluated in the study performed by Saad et al. 16 Histopathological evaluation was made by an experienced pathologist.
AgNOR detection
The heart tissue samples (with dimensions of approximately 1 × 1 × 1 cm3) were obtained from the heart tissue of the animals. After routine histological follow up, the pieces of heart tissue in the paraffin blocks were cut to 4-µm thick sections. Before AgNOR staining, the tissue sections were deparaffinized in xylene and then rehydrated in graded alcohol solutions. The slides were air-dried at room temperature for 15 min before being fixed in absolute methanol for 5 min. AgNOR staining method was performed according to the Benn and Perle protocol and the Lindner protocol, with a slight modification for all groups. 17,18
Slides containing stained tissue sections were viewed using a light microscope (Eclipse 80i, Nikon) and photographed using a digital camera (Digital Sight DS-fi1, Nikon). The captured images were transferred to image processing software (ImageJ version 1.47t, National Institutes of Health, Bethesda, Maryland, USA), and the evaluation was performed using the “freehand selections” tool. One hundred nuclei per animal were evaluated, and the mean AgNOR number and total AgNOR area per nuclear area (TAA/NA) for each nucleus were detected.
Statistical analysis
Statistical Package for Social Sciences (SPSS, Inc., Chicago, Illinois, USA) for Windows 11.5 was used for statistical analysis. While evaluating the study data, in addition to descriptive statistical methods (mean, standard deviation (SD)), one-way analysis of variance (Bonferroni test for post hoc analysis) was used while analyzing quantitative data if there were more than two groups. Chi-square test (Fisher’s exact test) was used for categorical data analysis. Results were given as mean ± SD in 95% confidence interval, and p < 0.05 was considered to be statistically significant.
Results
Biochemical findings
It was seen that COHb levels increase in correlation with the density of CO inhaled when COHb levels of experimental groups were compared with each other. COHb levels of groups 1 to group 4 were 1.67 ± 0.33%, 29.50 ± 0.42%, 43.00 ± 0.93%, and 52.00 ± 0.82%, respectively. There was a statistically significant difference between COHb level of the control group and COHb levels of the other groups (p < 0.0001). Additionally, there were statistically significant differences between COHb levels of all groups (p < 0.0001). Figure 1 shows COHb levels of all groups.

COHb levels of our groups. COHb: carboxyhemoglobin.
Histopathological findings
Myocardial fiber swelling and interstitial edema, disorganization of myocardial fibers with or without fibroblastic proliferation, myo-cytolysis/necrosis of myocardial fibers, and myocardial fiber vacuolation were evaluated during histopathological examination. Histopathological findings of the study are shown in Table 1. This evaluation showed that there were no pathological changes in heart tissues of rats in group 1. There was no swelling, disorganization, necrosis or vacuolation (HE 400×; Figure 2(a)). Myocardial fiber swelling, interstitial edema, and nucleomegaly were detected in group 2 (HE 400×; Figure 2(b)). Statistically significant increase in histopathological changes except necrosis were found in groups 3 and 4 compared to groups 1 2 (p < 0.05, HE 400×; Figure 2(c) and (d)).
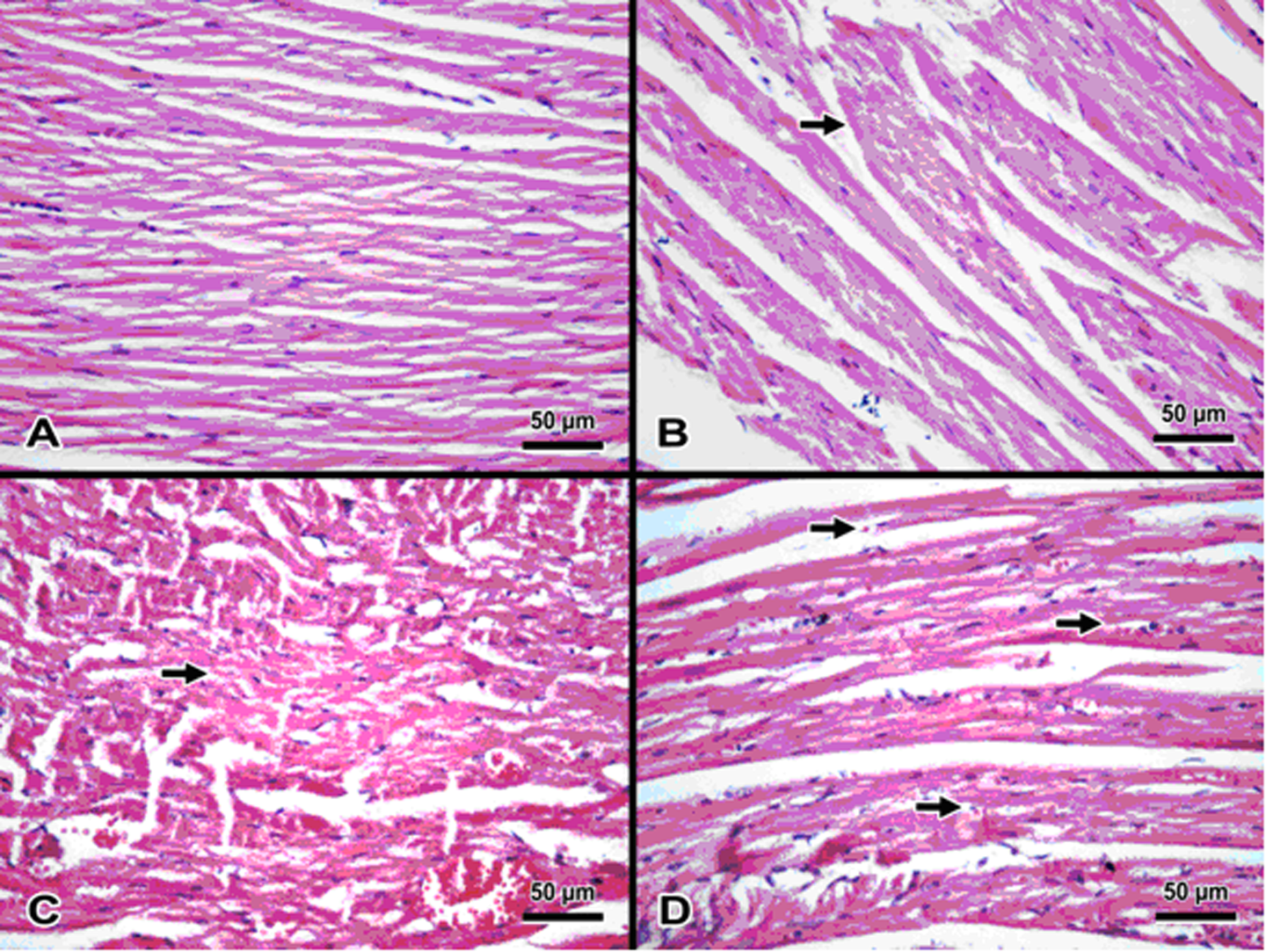
(a) Group 1: myocytes with normal appearance including small fusiform nuclei and smooth cytoplasms with marked Z lines (HE ×400). (b) Group 2: myocytes with mild cytoplasmic enlargement (cellular swelling, arrow; HE ×400). (c) Group 3: myocytes with nucleomegaly (arrow), cytoplasmic vacuoles and swelling and loss of arrangement and polarization (disorganization; He ×400). (d) Group 4: myocytes with cytoplasmic swelling, hemorrhage (arrow) and nucleomegaly (HE ×400).
Histopathological features of our groups.
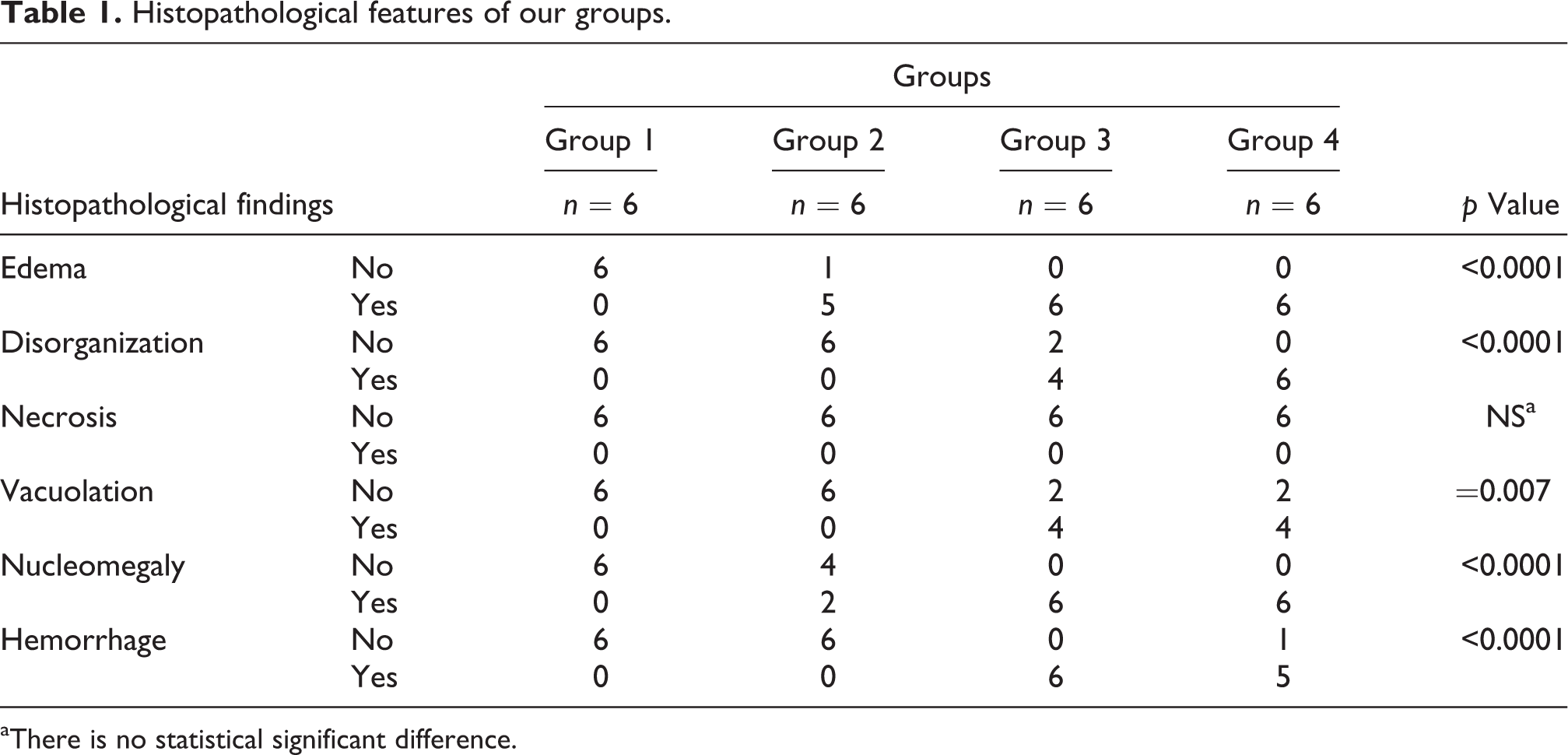
aThere is no statistical significant difference.
In addition, a statistically significant difference was found between groups 1 and 2 compared to groups 3 and 4 in terms of nucleomegaly and hemorrhage.
Although no CMY was seen in the control group, mild CMY was present in one rat but the other six rats were normal in group 2 (1000 ppm). Five rats in group 3 (3000 ppm) and six rats in group 4 (5000 ppm) were evaluated as having moderate to severe CMY when the CMY scoring system used by Saad et al. 16 was applied to our groups (Table 2).
CMY scoring method according to COHb levels.

NS: not significant.
aGroup 1 versus group 2 = NS; group 3 versus group 4 = NS, but group 3 and group 4 versus group 1 and group 2 (p = 0.04) was found to be statistically significant.
AgNOR measurement findings
When the density of CO inhaled by rats was increased (as 1000, 3000, and 5000 ppm), there was a statistically significant difference between the control group and each of the other groups in terms of TAA/NA and mean AgNOR number (p < 0.0001; Table 3, Figure 3).
TAA/NA and mean AgNOR number values of groups.

TAA/NA: total argyrophilic nucleolar organizing region area/nuclear area; AgNOR: argyrophilic nucleolar organizing region; ANOVA: analysis of variance.
aThere was a difference between the control group and each of the other groups (ANOVA and post hoc tests (Bonferroni)).
bThere was no difference between 1000 ppm group and 3000 ppm group; and 3000 ppm group and 5000 ppm group in terms of TAA/NA (p = 0.177 and p = 0.997, respectively).
cThere was no difference between 1000 ppm group and 3000 ppm group, 1000 ppm group and 5000 ppm group, and 3000 ppm group and 5000 ppm group in terms of mean AgNOR number (p = 0.128, p = 0.139, and p = 0.997, respectively).
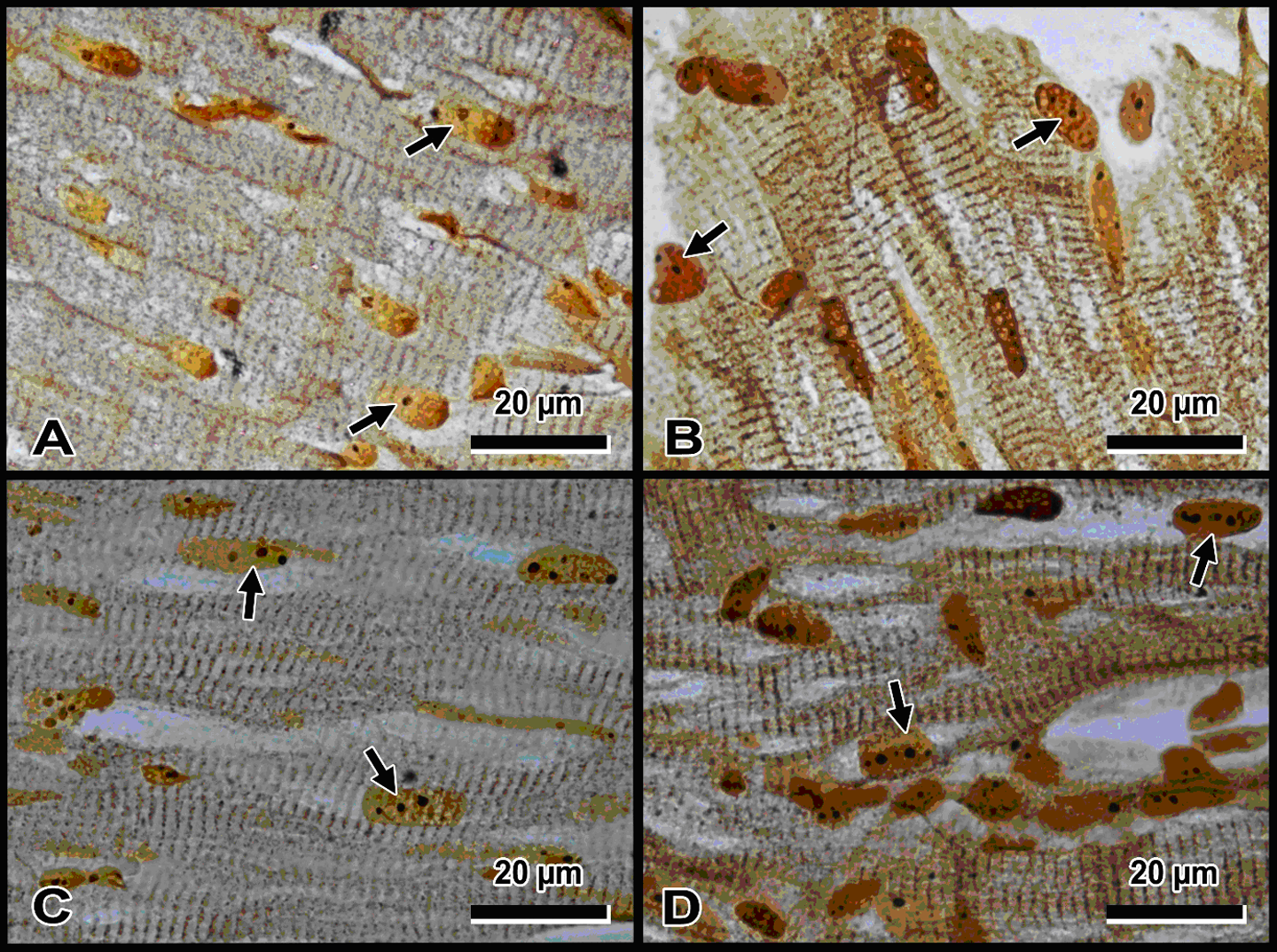
Silver-stained NORs (arrows) in heart cells. (a) Group 1, (b) group 2, (c) group 3, and (d) group 4 (×1000 magnification). NOR: nucleolar organizing region.
There was a strong positive correlation between TAA/NA ratio and both histopathological CMY score (r = 0.761; p < 0.0001) and COHb level (r = 0.894; p < 0.0001). Additionally, a strong positive correlation between NOR number per cell and both histopathological CMY score (r = 0.698; p < 0.0001) and COHb level (r = 0.865; p < 0.001) was found. There was also a strong positive correlation between histopathological heart failure score and COHb level (r = 0.815; p < 0.0001; Figure 4).

Correlation between CMY and AgNOR values, and correlation between COHb and AgNOR values. CMY: cardiomyopathy; AgNOR: argyrophilic nucleolar organizing region; COHb: carboxyhemoglobin.
Discussion
CO is one of the most commonly seen causative agents in both accidental and intentional fatal intoxications occurring through inhalation. Although the exact mechanism of CO poisoning is not known, it is suggested that CO causes a relative anemia and asphyxia or tissue hypoxia by competing with oxygen to bind to Hb and decreasing oxygen transport and delivery to tissues. 7,19
CO intoxication may cause damage to all tissues, including especially those with high oxygen consumption and a high level of susceptibility to hypoxia such as brain and heart tissues. Myoglobin is the depot site of oxygen molecules and plays its role in intracellular transport of oxygen. After binding CO, oxygen-carrying capacity of myoglobin decreases and that leads to decreased oxygen transport to myocardial cells and finally to myocardial dysfunction. 4,20
Symptoms and signs caused by hypoxia in cardiovascular system may include anginal chest pain, palpitations, weak capillary filling, hypotension, disrupted circulation, pulmonary edema, and cardiac arrest. 6,21,22
CO poisoning may be diagnosed by measuring COHb level in early stages. COHb level can be measured with a pulse oximetry device capable of detecting CO or spectrophotometrically using a specific blood gas analysis. If it is measured high, the patient has CO intoxication, but it does not rule out poisoning when its level is normal if the patient was given 100% oxygen prior to measurement or if a significant time lag was present between removal of patient from exposure and measurement of CO level. In our study, we measured COHb level using blood gas analysis. We took blood samples from jugular vein instead of intracardiac sampling in order to avoid cardiac damage during blood sampling procedure. We saw that COHb level increases as the density of CO inhaled increases. It has been reported that COHb levels may not be reliable while evaluating the degree of intoxication, 2,23 but COHb level is related to the level of damage to tissues and organs although symptoms may differ from one patient to another. We saw that the difference between groups 1 and 2 (which have relatively low COHb levels) and groups 3 and 4 (which have more prominently increased COHb levels and moderate to severe CMY) is statistically significant in regard to histopathological changes of cardiac injury. We also saw using AgNOR method that cardiac injury is increased in group 3 and group 4. Hemorrhagic and necrotic foci have been detected throughout all parts of heart tissue, especially in septal and papillary muscles in the case of CO intoxication. Although the evidence of myocardial involvement may appear promptly and prominently, it may sometimes appear a few days later or may not even appear at all. 24 The activity of the plasma membrane energy-dependent sodium pump is reduced in hypoxia. Failure of this active transport system causes sodium to enter and accumulate inside cells and potassium to diffuse out. The net gain of solute is accompanied by isosmotic gain of water, causing cell swelling and dilation of the endoplasmic reticulum. Reactive nuclear enlargement and stasis of and hemorrhage from vascular structures are seen due to effects of inflammatory mediators in tissues with cellular damage. Although we saw nuclear enlargement and hemorrhage as a result of ischemia caused by CO intoxication in especially groups 3 and 4, we did not see necrosis in any group.
Irreversible injury is associated morphologically with severe swelling of mitochondria, extensive damage to plasma membranes, and swelling of lysosomes. Large, flocculant, amorphous densities develop in the mitochondrial matrix. In the myocardium, irreversible injury and necrosis can be seen as early as 30–40 min after ischemia. 25
In our previous study, we showed that the AgNOR protein amount increased depending on the increase of CO exposure in the lung cells (Colakoglu et al. 2015). In our current study, the total AgNOR number per total nuclear number and TAA/NA increased depending on the increase of CO exposure in the heart cells, too.
All cells tend to protect their situation toward dangerous agents such as CO. CO intoxication causes tissue hypoxia. Hypoxia may cause cardiac dysfunctions, leading to cardiac arrest. It may be said that these proteins occur against CO exposure or trigger the synthesis of some other proteins that have protective roles in the heart cells. Thus, these proteins may be used for the prevention of the cardiac dysfunctions and cardiac arrest. In this way, new therapeutic approaches may be developed in the treatment of CO intoxication in the future.
In the current study, significant positive correlation was detected between mean TAA/NA and histopathological heart insufficient score. For mean AgNOR number, this correlation is significant too. The results of the histopathological examination can be obtained with the evaluation of myocardial fiber swelling and interstitial edema, disorganization of myocardial fiber with or without fibroblastic proliferation, myo-cytolysis/necrosis of myocardial fibers, and myocardial fiber vacuolation. Thus, it may be said that only detection of AgNOR protein synthesis may be used to obtain knowledge about the degree of damage to the heart cells, instead of the histopathological scoring method requiring an experienced pathologist.
CO intoxication can be diagnosed early phese of CO exposure, assaying serum COHb level. However, COHb levels sometimes can be not helpful in the diagnosis and direction of the treatment, as the half-life of room air is 4–6 h. Therefore, it is especially difficult to diagnose CO intoxication via COHb levels in patients presenting late or who died after a significant time interval passed since removal of the patient from exposure. According to our results, significant positive correlation between mean TAA/NA and COHb levels and between AgNOR number and COHb (r = 0.865; p < 0.0001) was detected. Thus our method may be used for the detection of CO intoxication. Also when COHb levels seem normal in the intoxication doubt autopsies, our evaluation methods can be adapted for use to obtain more certain knowledge about the CO intoxication levels in forensic science.
Both the AgNOR values may be used as indirect indicators for evaluating the degree of heart cell damage rate (instead of histopathological scoring method) and CO intoxication levels (instead of COHb level). Additional studies should be conducted to obtain more certain knowledge about this topic. In this way, new therapeutic approaches may be developed in the treatment of cardiac dysfunctions caused from hypoxia.
Limitations of the study
This study is a pioneer one. Disadvantages of these types of studies are due to lack of similar studies to compare with and limitations occurring naturally in all animal studies. But studies about AgNOR in CO intoxication have been started to be performed recently. We suggest that new studies on this subject with autopsy series may provide significant additional information.
Conclusion
It was detected that when the CO levels (as ppm) are increased, the COHb levels increase, too. So depending on the increasing CO levels, the degree of CMY increases. Additionally, depending on the increasing CO levels, the amounts of AgNOR protein levels increase, too. Thus it may be said that the detection of AgNOR protein amount may be used as an indicator to obtain the knowledge about the CMY levels. In addition to this, the AgNOR protein levels instead of histopathological evaluation score may be used to detect the level of damage to hearth cells. To obtain more certain knowledge about the current topic, additional studies including large number of series should be carried out.
Footnotes
Acknowledgement
We would like to thank to Dr. Arif Duran for sacrificing and dissecting our rats.
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.