
Abstract
We investigated the red blood cell (RBC) acetylcholinesterase (AChE) activities and butyrylcholinesterase (BChE) activities at presentation to the emergency department (ED) and at 24 h after presentation following poisoning by dichlorvos, fenitrothion, or ethyl p-nitrophenol thio-benzene phosphonate (EPN). Although the patients from different groups had similar characteristics at presentation such as time interval from ingestion to presentation to the ED and the amount of organophosphate ingested, the dichlorvos group had significantly lower BChE levels than the fenitrothion group and lower RBC cholinesterase activity than the EPN group. Patients poisoned with EPN or dichlorvos had significantly higher inhibition of BChE activities from baseline than RBC AChE activities at presentation. Twenty four hours after administration of pralidoxime, RBC AChE activities had increased in patients in the dichlorvos and EPN groups, while RBC AChE activities had slightly decreased in the fenitrothion group. BChE activities increased significantly in the dichlorvos group but decreased in the EPN group. The recovery patterns of RBC AChE and BChE activities did not match in any particular individual. This study showed that the patterns of inhibition and recovery of the activities of two cholinesterases after treatment are highly variable according to the organophosphate and in different individuals.
Introduction
Organophosphates (OPs) inhibit serine esterase through phosphorylation of the serine hydroxyl moiety. Acetylcholinesterase (AChE), which eliminates acetylcholine (Ach) from the central and peripheral nervous systems, is a primary target esterase of OPs, and the accumulation of Ach in the nerve terminals lead to clinical features of toxicity. Additionally, OPs inhibit butyrylcholinesterase (BChE), which is another serine esterase; however, phosphorylation of BChE does not appear to result in the toxic response of OPs. 1
Blood cholinesterase (ChE) consists of red blood cell (RBC) AChE and BChE. Because AChE is encoded by a single gene and the molecular diversity of this gene is typically confined to the membrane anchoring tail rather than to the catalytic unit, RBC AChE is considered to be a surrogate for neuronal AChE. RBC AChE activity has been assessed in multiple studies either to demonstrate the efficacy of oximes against OP poisoning or to compare the kinetics of RBC AChE and neuronal AChE. 2,3 However, the necessary tests for measuring RBC AChE activity are not readily available in most hospitals. BChE activities can be more rapidly assayed compared to RBC AChE activities in the clinical field, and the assessment of BChE activity is useful for establishing a diagnosis of exposure to OP and to monitor OP elimination. 4,5 Additionally, many studies have focused on the initial BChE activities for predicting the outcome. 6–8
During the treatment of patients poisoned with OPs, we observed that some patients had low BChE activity levels, despite having normal RBC AChE activity levels at presentation after OP poisoning. Some patients showed increased BChE activity after the administration of pralidoxime (PAM), despite exhibiting decreased RBC AChE activity. Several in vitro studies have demonstrated variabilities in the reactivation and inhibition of ChEs according to OP chemical formulation. 9,10 Chaou et al. reported a trend of slower recovery of BChE activity in chlorpyrifos-poisoned patients and a trend of faster recovery of BChE activity in methamidophos-poisoned patients compared with those in patients poisoned with other OPs. 11 However, the issue of different recovery patterns of both RBC AChE and BChE activities over time in OP-poisoned patients has been addressed less frequently.
In this study, we aimed to compare RBC AChE and BChE activities over time after PAM administration following poisoning by the three most common OPs in South Korea.
Methods
Study design
This single-institution, retrospective cross-sectional study was performed by a chart review. The study design was approved by the institutional review board of Chonnam National University Hospital (Gwangju, South Korea).
Patients
Patients who were 18 years or older and presented to the emergency department (ED) after dichlorvos ingestion, fenitrothion ingestion, or ethyl p-nitrophenol thio-benzene phosphonate (EPN) ingestion between 2004 and 2013 were included in the study. Because dichlorvos, fenitrothion, and EPN accounted for 59% of OP poisoning cases in our hospital, we limited our study to patients who were poisoned with one of these three OPs. In South Korea, dichlorvos is the most common dimethyl OP, followed by fenitrothion, for OP poisoning, and EPN is the most common unclassified OP. 12 The characteristics of the three OPs are described in Table 1.
Characteristics of three organophosphates.

AchE: acetylcholinesterase; WHO: World Health Organization; EPN: ethyl p-nitrophenol thio-benzene phosphonate.
For inclusion in the study, each patient must have had their RBC AChE and BChE activities measured at presentation and at 24 h after PAM administration. The diagnosis of OP poisoning was made based on the following criteria: a history of OP ingestion provided by the patient or a witness, clinical manifestations consistent with OP poisoning, and improvement in signs and symptoms after treatment with atropine and PAM. The chemical formulation of OP was determined based on the medical records indicating the chemical name or the brand name on the bottle that the patient or witness brought to the ED.
The exclusion criteria included mixed ingestion with other drugs, a history of other preexisting comorbid conditions, a history of liver disease, hemoglobinopathy, a transfer to another hospital or discharge against medical advice before the final outcome was assessed, PAM administration at another hospital before presentation to our ED, presentation after 24 h from OP ingestion, and pregnancy. Additionally, the patients who were given a different dose of PAM compared to that according to our hospital treatment guidelines during the first 24 h were excluded.
To compare RBC AChE and BChE activities after OP poisoning, the patients were divided into three groups according to the chemical formulation of the ingested OP.
All the patients in the study received decontamination, the administration of atropine and PAM, and general supportive measures, such as mechanical ventilator support in the intensive care unit (ICU). Atropine was administered either as a continuous infusion or as a bolus injection every 15 min and was titrated to achieve adequate atropinization, established by the drying of bronchial secretions. Additionally, bolus administration of 2 g PAM was performed, followed by 0.5 g/h for 3 days. When an intermediate syndrome was diagnosed based on clinical symptoms, an additional dose of PAM was administered. The need for mechanical ventilator support and admission to the ICU was assessed by the on-call emergency physician. Patients underwent weaning from the mechanical ventilator if they were satisfied with our hospital’s criteria for weaning.
Collected or calculated data
The medical records were reviewed, and the following data were collected or calculated: age, gender, intent of exposure, the chemical formulation of the OP ingested, the time interval from ingestion to arrival at our hospital, laboratory test results (including RBC AChE and BChE activities), the degrees of inhibition of RBC AChE and BChE activities at presentation, the increases in RBC AChE and BChE activities after the first 24 h from presentation, total amounts of atropine and PAM administered during hospitalization, duration of mechanical ventilation, duration of ICU stay, and survival outcome.
The amount of OP ingested was estimated as a spoonful (5 mL), a mouthful (25 mL), a cup (100 mL), or a bottle (300 mL).
RBC AChE and BChE activities were measured photometrically using the Modular P analyzer (Roche, Seoul, South Korea). The blood sample for RBC AChE was collected into ethylenediaminetetraacetic acid-treated tubes, and the blood sample was immediately stored at 4°C. The test for measuring RBC AChE activity was based on the reaction during which ChE splits Ach into acetate and thiocholine; the latter reacts with dithiobisnitrobenzoic acid to form the yellow-colored 5-mercapto-2-nitrobenzoic acid.
13
The rate of color formation is directly proportional to the ChE activity. The RBC AChE activity was calculated with reference to the respective hematocrit level and plasma and whole blood ChE activities. The calculation for RBC AChE activity is as follows:
Serum was collected for the BChE assay after centrifugation at 2000 g for 15 min, and the samples were stored at 4°C. BChE catalyzes the hydrolysis of butyrylthiocholine to thiocholine and butyrate. Thiocholine instantaneously reduces yellow hexacyanoferrate (III) to almost colorless hexacyanoferrate (II), and the decrease in color is measured at wavelengths between 405 nm and 415 nm. 14 The lowest measurable level is 100 U/L, and the normal range of BChE activity is 5320–12,920 U/L.
The degree of inhibition of ChE activities at presentation was calculated by dividing the level of ChE activities at presentation by the estimated baseline levels of ChE activities. The mean level of ChE activities at presentation in patients, who directly presented to our ED during the study period at a median time interval of 3 h after ingesting another pesticide that did not have an anti-ChE effect was regarded as the estimated baseline.
The increase in RBC AChE and BChE activities at 24 h after presentation was calculated using the following formula: 100 × (ChE activities at 24 h after presentation – ChE activities at presentation)/ChE activities at presentation.
Statistical analysis
The baseline patient characteristics are presented as frequencies for categorical variables and as medians and interquartile ranges for continuous variables. Continuous variables were compared using the Mann–Whitney test or the Kruskal–Wallis H test. The post hoc comparison was conducted using the Mann–Whitney test with a Bonferroni adjustment. Fisher’s exact test or the χ 2 test was performed to make comparisons between the categorical variables. The values of p < 0.05 were considered to be statistically significant. All statistical analyses were performed using the Statistical Package for the Social Sciences version 21.0.
Results
ChE activities at presentation
Among 102 patients who presented to our ED after dichlorvos, fenitrothion, or EPN ingestion, both ChEs activities at presentation and at 24 h after PAM administration were available for 58 (56.9%) patients. After the application of exclusion criteria, 46 patients were eligible for inclusion in the study (Figure 1).

Study flow diagram. OP: organophosphate; RBC AChE: red blood cell acetylcholinesterase; BChE: butyrylcholinesterase; PAM: pralidoxime.
The demographic data and clinical characteristics of 46 patients are summarized in Table 2. These patients presented to the ED at a median time interval of 3.0 h after poisoning, and the estimated median volume of OP ingestion was 100 mL. Mechanical ventilation was required in 39 (84.8%) patients, and the total mortality rate was 4.3%.
Clinical characteristics of patients.a

EPN: ethyl p-nitrophenol thio-benzene phosphonate; RBC AChE: red blood cell acetylcholinesterase; BChE: butyrylcholibesterase; ICU: intensive care unit; GCS: Glasgow Coma Scale; MV: mechanical ventilation.
aContinuous variables were compared using the Mann–Whitney test or the Kruskal–Wallis H test. Fisher’s exact test or the χ 2 test was performed for comparison between the categorical variables.
bTime interval from ingestion to presentation to the emergency department.
Parameters such as age, gender, the amount of OP ingested, and the time interval from ingestion to presentation to our ED did not differ according to the chemical formulations of the ingested OPs.
ChE activities at presentation were available for 32 patients who presented to our ED after ingesting another pesticide without anti-ChE action during the study period. There were no significant differences in age (p = 0.570) or gender (p = 0.304) between these 32 patients and the 46 enrolled patients. The mean level of RBC AChE activities and BChE activities, regarded as the estimated baseline level, were 12,159 and 7093 U/L, respectively. Upon analysis of the degrees of inhibition of the activities of both ChEs at presentation in an individual, by referencing an estimated baseline level, dichlorvos and EPN were found to inhibit BChE activities more significantly than RBC AChE activities (p = 0.002 for dichlorvos and p = 0.001 for EPN). In contrast, fenitrothion inhibited both BChE and RBC AChE activities to similar degrees (Figure 2).

Inhibition of RBC AChE and BChE activities at presentation according to the OP. Bar represents the mean ± SEM. Dichlorvos and EPN inhibited BChE activities more significantly than RBC AChE activities at presentation. Both ChE activities in 32 patients who ingested another pesticide without anti-ChE action were used as the baseline ChE activities (RBC AChE: 12,159 U/L and BChE: 7093 U/L). The baseline ChE activity was designated as 1. The normal range of RBC AChE activity and BChE activity is 11,188–16,698 U/L and 5320–12,920 U/L. **p < 0.01: comparing RBC AChE with BChE. RBC: red blood cell; AChE: acetylcholinesterase; BChE: butyrylcholibesterase; OP: organophosphate; ChE: cholinesterase; EPN: ethyl p-nitrophenol thio-benzene phosphonate.
Comparison of both the ChE activities according to each OP revealed that the dichlorvos group had a significantly lower BChE activity at presentation compared with the fenitrothion group (p = 0.006) and lower RBC AChE activities than the EPN group (p = 0.033; Table 2).
Changes in ChE activities after PAM administration
The RBC AChE activities increased 16.4% from presentation in the dichlorvos group and increased 2.4% in the EPN group over a period of 24 h, whereas the RBC AChE activities decreased slightly in the fenitrothion group (Figure 3).
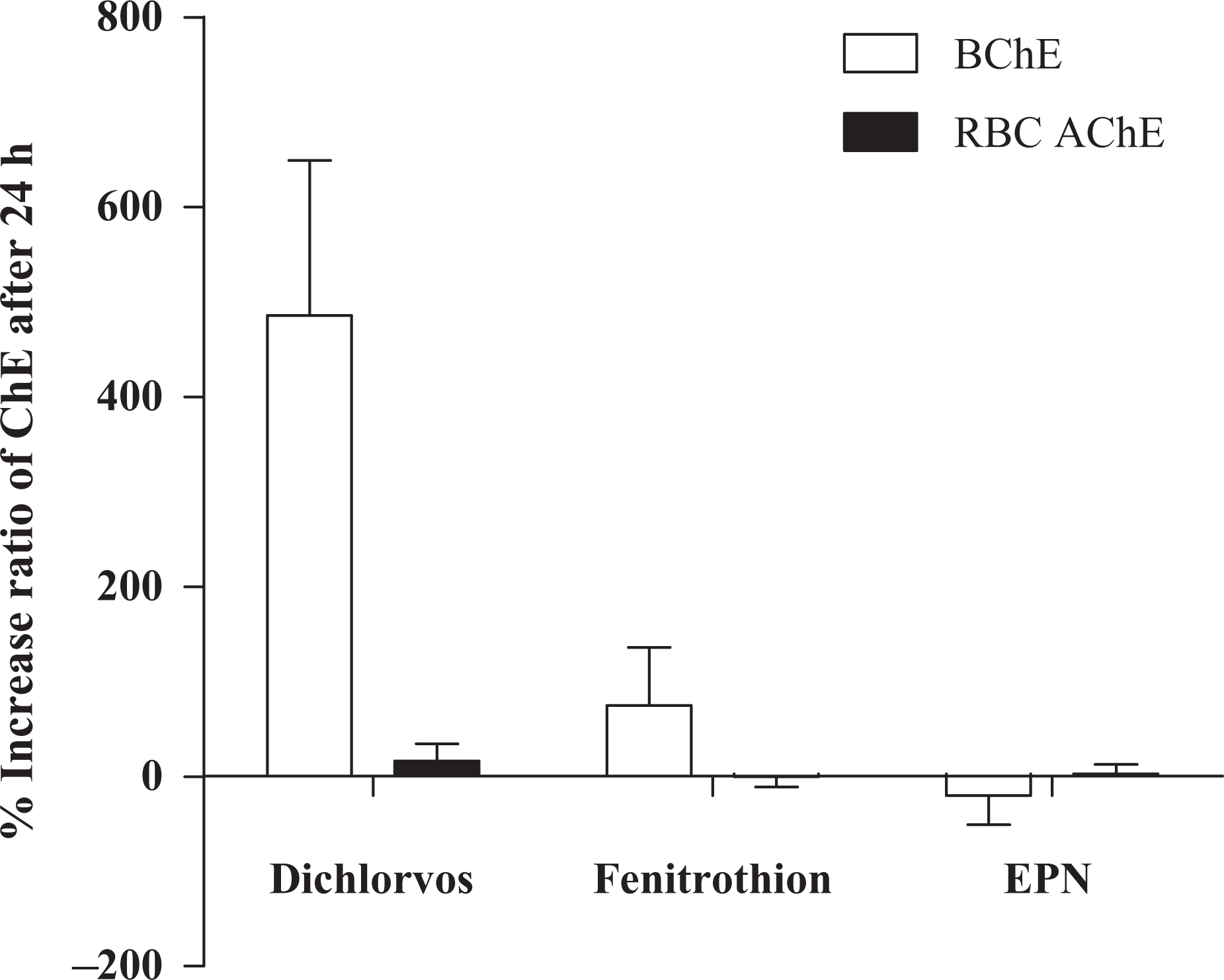
Change in RBC AChE and BChE activities at 24 h after administration of PAM according to the OP. Bar represents the mean ± SEM. RBC AChE activities increased by 16.4% in the dichlorvos group and by 2.4% in the EPN, whereas the fenitrothion group showed a 0.4% decrease in RBC AChE activities at 24 h after presentation despite administration of PAM. BChE activities increased in dichlorvos and fenitrothion groups, in contrast to a decrease in the EPN group. RBC: red blood cell; AChE: acetylcholinesterase; BChE: butyrylcholibesterase; OP: organophosphate; EPN: ethyl p-nitrophenol thio-benzene phosphonate; PAM: pralidoxime.
The BChE activities increased by 485.4% in the dichlorvos group and by 74.8% in the fenitrothion group over a period of 24 h after PAM administration, while the BChE activities decreased in the EPN group (Figure 3).
Comparison of the trend for recovery of RBC AChE activities against the trend for recovery of BChE activities in individuals showed that dichlorvos-poisoned patients experienced increases in both ChE activities over time following PAM administration. In contrast, EPN- and fenitrothion-poisoned patients experienced opposite trends for the recovery of the two ChE activities over time (Figure 3).
Discussion
The RBC AChE and BChE activities at presentation
The inhibition of ChE activities at presentation, before administration of an oxime, may be determined by the characteristics of the specific OP, including the chemical formulation, fat solubility, and its metabolism. 15 The dichlorvos group showed more inhibition of both ChE activities at presentation than either the fenitrothion group or EPN group, despite similarities in the time intervals from ingestion to presentation to our ED and the amount of ingested OP (Table 2). This finding supports that the speed of inhibition is different according to the specific OP. 4,15 Dichlorvos directly acts as a potent anti-ChE, whereas fenitrothion and EPN require a cytochrome P450-mediated desulfation reaction before they can exert their potent anti-ChE activities because these OPs each have a sulfur atom bound to the phosphate atom. 15–17 This direct inhibition by the parent form itself may account for the observed rapid inhibition of ChE in the dichlorvos group.
Currently, few data are available in the literature describing the selective inhibition of ChEs according to OPs in humans. Paraxon methyl had a 2.7-fold higher inhibitory potency for BChE activities, whereas paraxon ethyl had a 20-fold lower inhibitory potency for BChE activities compared with RBC AChE activities. 9 Chlorpyrifos oxon, which is an active metabolite of chlorpyrifose, significantly inhibited BChE activities, but not RBC AChE activities. 18 In this study, EPN and dichlorvos appeared to inhibit BChE activities more significantly than RBC AChE activities (Figure 2). Consistently, plasma BChE was reportedly more inhibited than RBC AChE in eight patients exposed to dichlorvos. 19
In this study, although the EPN group had a poor outcome with regard to the duration of ICU admission and hospitalization compared to that of the other two groups (ICU admission: p < 0.001 for the dichlorvos and fenitrothion groups; hospitalization: p = 0.003 for the dichlorvos group, p = 0.006 for the fenitrothion group), the EPN group did not have lower activities of both ChEs at presentation compared with the other two groups. This finding is consistent with that of other studies, which demonstrated that BChE activities at presentation do not predict patient outcome. 20,21 Selective inhibition and varying rates of inhibition by OPs may have resulted in the lack of the predictability of ChEs at presentation. This possibility suggests that the level of ChE activities at presentation should be interpreted according to the chemical formulation of the OP and that patients with OP poisoning should not be treated as a homogenous group in any study related to ChE activities at presentation.
The changes in RBC AChE and BChE activities following PAM administration according to OPs
This study was not aimed at investigating whether PAM is clinically beneficial or harmful in the management of OP poisoning. Here, we merely demonstrate changes in the activities of both ChEs after PAM administration. In vitro experiments have shown that oximes are effective reactivators of human AChE inhibited by OP. 22 A recent double-blind placebo-controlled trial including 235 OP-poisoned patients showed that the same dosage of PAM that we used reactivated RBC AChE, despite no clinical beneficial effect on mortality or the need for intubation. 23
In this study, RBC AChE activities increased in the dichlorvos group at 24 h after presentation, in contrast with the slight decrease of RBC AChE activities in the fenitrothion group, despite administration of same 14 g of PAM. In contrast, the BChE activities recovered in the dichlorvos and fenitrothion groups, while BChE activities decreased in the EPN group (Figure 3).
Inhibited AChE undergoes reactivation by PAM, spontaneous reactivation, or aging. The variations in the speeds of each of these reactions, according to the specific OPs, contribute to the variable recovery patterns of inhibited ChEs. 4
In terms of the aging process, the half-lives of dimethyl OP and diethyl OP are 3.7 and 33 h, respectively. 4 There are currently no data available about aging kinetics in EPN; however, aging appeared to occur within 4 h because RBC AChE failed to be reactivated if the patient presented to the ED more than 4 h after ingestion (Figure 4).
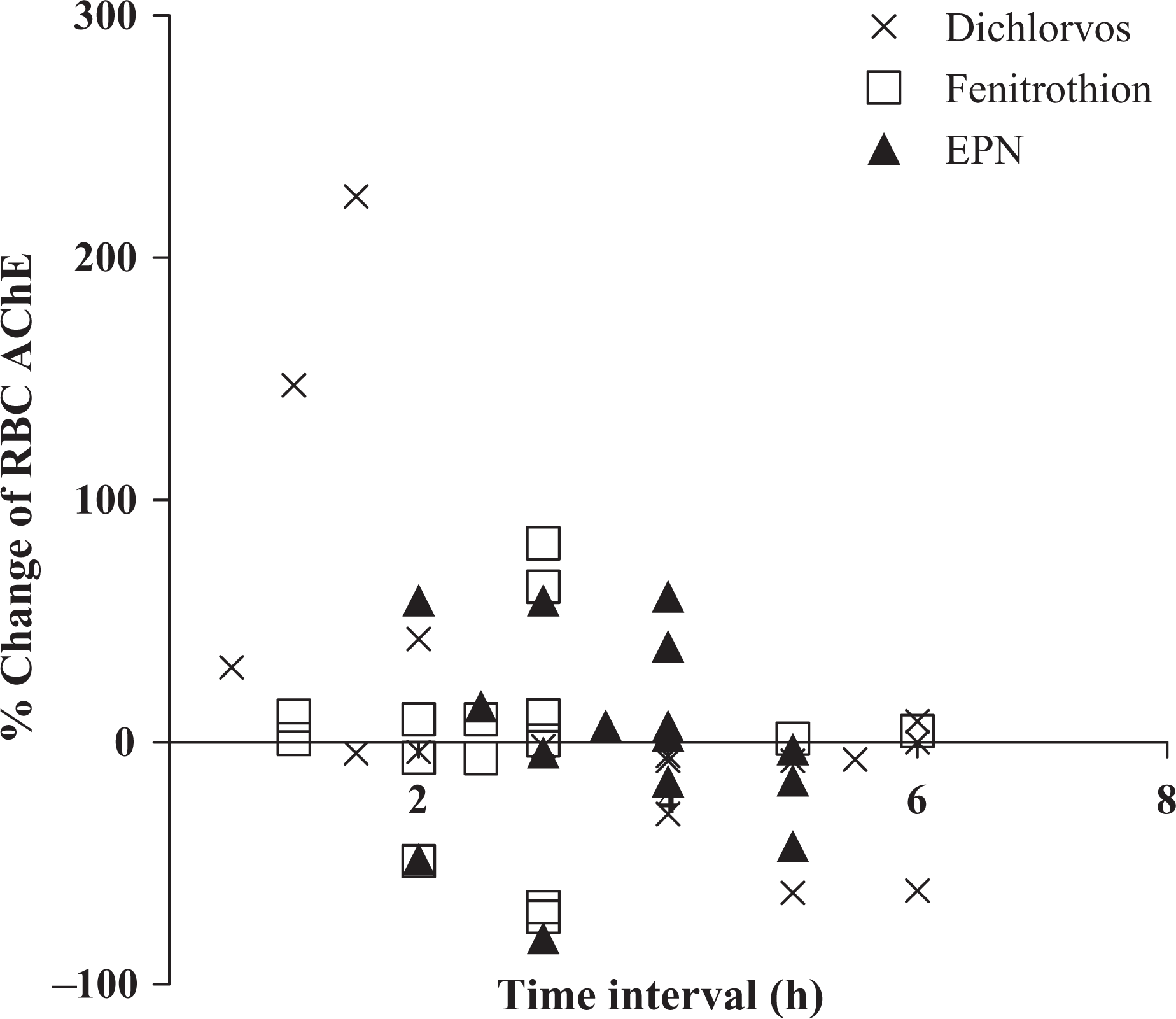
Time interval from ingestion to presentation versus change in (RBC AChE activities at 24 h after administration of PAM. The plot represents the change in RBC AChE activities versus time interval from ingestion to presentation. RBC: red blood cell; AChE: acetylcholinesterase; PAM: pralidoxime.
After considering that the half-life of the aging process is 3.7 h for dimethyl OP, 50% of inhibited RBC AChE activities can be reactivated in the two groups, who were given PAM within 3 h after ingestion. However, RBC AChE activities decreased in 40.0% of patients who received same dosage of PAM within 3 h after exposure to dichlorvos or fenitrothion (Figure 4). Goel et al. showed that RBC AChE activities increased up to 100% at 24 h after administration of 14 g of PAM in a patient who was given PAM at 6 h after exposure to dichlorvos. 24 These reactivation patterns, which did not fit the time course of aging kinetics, confirmed that both the blood concentration of OP and the OP elimination rate can affect the reactivation of RBC AChE activities by PAM. In rat blood, dichlorvos was not detected after 2 h because of rapid hydrolyzation by phosphatases, while 72% of fenitrothion and 89% of EPN was left at 24 h. 17 In killifish, the elimination half-lives of EPN and fenitrothion were 34.7 h and 6.3 h, respectively. 25 Most likely, re-inhibition of newly reactivated AChE by persistent EPN may lead to poor reactivation of RBC AChE in this study and poor patient outcomes.
In addition, the rate of spontaneous reactivation according to OPs varies. Although the spontaneous reactivation of these three OPs in humans has not been investigated, the half -lives for the spontaneous reactivation of AChE inhibited by dichlorvos and AChE inhibited by diazinon were 2.9 and 58.3 h in pigs, respectively. 26
The issue of whether PAM can reactivate BChE is controversial. Treatment with a 1 g bolus of PAM every 6 h failed to reactivate BChE over the first 24 h in patients poisoned with dimethoate, fenthion, chorpyrifos, or quinalphos. 1 No reactivation of BChE occurred in dimethoate- or fenthion-poisoned patients with 14 g of PAM. 1 In contrast, Jafari and Pourheidari showed that inhibition of human BChE by parathion and paraoxon was reversed by approximately 50% after the administration of 100 µM of PAM. 27 Considering that the resynthesis of BChE in the liver occurs at 7% per day after elimination of OP and that the half-life of the spontaneous reactivation of BChE was 10 h in sheep poisoned with dichlorvos, the increase of BChE activities up to 485.4% in the dichlorvos group may suggest the reactivation of BChE by PAM. 4,26 Administration of PAM failed to reactivate the BChE inhibited by EPN. The selective re-inhibition of reactivated BChE by persistent EPN may have partially accounted for the decrease in BChE activities after 24 h, despite PAM administration. Further study including a control group not receiving PAM is required to research the reactivation of BChE by PAM.
The difference in the individual recovery patterns of RBC AChE and BChE
Our study showed that the recovery patterns of the two ChEs varied among individuals (Figure 3). Particularly in the EPN and fenitrothion groups, the two ChEs exhibited opposite patterns of recovery after PAM administration. Consistent with our results, BChE was inhibited again for up to 48 h after maximal reactivation in the first hour after OP poisoning, whereas RBC AChE remained activated after the initial reactivation. 1 These results demonstrate that both the ChE assays cannot replace each other.
Limitations
The main limitation of this study is that the number of included patients was too small to draw definite conclusions. A further prospective study including a larger number of patients is needed. Second, 45.1% of patients who ingested one of the three OPs were enrolled. There may be a selection bias because more severe clinical cases were enrolled in the study due to the preferential use of RBC AChE and BChE assays in such patients who were expected to have poor prognoses. However, there were no differences in the potential factors related to clinical outcomes, such as the duration of hospitalization (p = 0.404), ICU stay (p = 0.361), mechanical ventilation (p = 0.427), and the amount of administered atropine (p = 0.242). There were also no differences in initial patient characteristics, such as age (p = 0.240), initial Glasgow Coma Scale (p = 0.146), and initial RBC AChE (p = 0.105) and BChE activities (p = 0.240) between the 46 patients enrolled and the 56 patients who ingested one of the three OPs but who were not enrolled in the study. Third, we used the levels of ChE activities in 32 patients who were poisoned with another pesticide as an estimated baseline level. These 32 patients were matched to our patients in terms of age and gender, but other individual factors that can affect the baseline levels of ChE activities were not considered. We reviewed the ChE assay results of some patients at discharge in this study, but the patients were discharged before normalization of ChE activity because of slow resynthesis of RBC AChE in the bone marrow after aging and the mobilization of the OPs stored in the adipose tissue. For example, the RBC AChE and BChE activities at discharge in a patient poisoned with EPN were 981 and 1492 U/L, respectively. Hence, we cannot use the levels of ChE activities at discharge as the baseline ChE level. A further prospective study to assess the baseline ChE levels during the months following discharge is needed to determine selective inhibition by OPs. Fourth, the time delay after blood sampling until analysis can interfere with the results of the activity assay for both ChEs. 4 Because of the retrospective design, we cannot exactly estimate the time delay; however, we stored the samples at 4°C until assay, and our hospital performs assays as soon as possible. Fourth, the volume ingested might be inaccurate, and the concentration of OP in the blood should be checked. The absence of a detectable OP concentration in the blood could weaken the comparison results among the three OPs. Further prospective studies to control for this influential factor are needed.
Conclusion
The selectivity and rate of inhibition of the two ChEs varies according to the chemical formulation of OPs in patients poisoned with dichlorvos, fenitrothion, or EPN. Additionally, the recovery pattern of the two ChEs varies according to the OP and among individuals after PAM administration. The chemical formulation of the OP should be considered when ChE activities are interpreted.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.