
Abstract
Introduction:
Chronic obstructive pulmonary disease (COPD) due to sulfur mustard (SM), known as mustard lung, is an important late pulmonary complication of SM poisoning. Due to the possible role of systemic inflammation in mustard lung, we evaluated the serum levels of adiponectin and leptin in these patients.
Materials and methods:
Thirty nonsmoker mustard lung patients in stable phase were enrolled into this study. Also, 30 COPD and 21 healthy participants were entered as control groups. Complete lung function tests were performed in the participants. The serum levels of adiponectin and leptin were measured in all groups.
Results:
There were no statistically significant differences in mean adiponectin and leptin levels among the groups (p = 0.38 and p = 0.35, respectively). There was a downward trend in leptin to adiponectin ratio from lower to higher stages of global initiative for chronic obstructive lung disease guidelines in mustard lung patients, which was not statistically significant (p = 0.8).
Conclusion:
Our results showed that there is no difference in mean adipokine levels in stable mustard lung patients compared with control groups. There was a foot-point in the alterations of serum adipokines regarding the severity of COPD, which needs to be documented by larger sample group.
Introduction
Chronic obstructive pulmonary disease (COPD) is a debilitating disorder, associated with high morbidity and mortality worldwide. 1 Sulfur mustard (SM), a chemical warfare agent used for almost 100 years, induces chronic and acute sequels in respiratory tract. 2 Chronic SM lung toxicity involves both upper and lower respiratory tracts. 3 During Iran–Iraq conflict, between 1981 and 1989, SM was used as chemical warfare agent and a considerable number of Iranian veterans were poisoned by its inhalation. 4 Of SM chronic complications, pulmonary complications seem to be the most common. 5 COPD due to SM, known as “mustard lung” is an important late toxic pulmonary consequence after SM exposure. 6
It is now well accepted that the systemic inflammation is a hallmark of COPD, and the term “systemic inflammatory syndrome” was proposed before. 7 Given the fact that there is an increased airway and systemic inflammatory markers in COPD, various biomarkers are demonstrated to rise during exacerbations. 8 Interleukin 6 (IL-6) and C-reactive protein (CRP), for instance, seem to be higher during infection. 8 There are conflicting data regarding the role of inflammatory and anti-inflammatory markers in mustard lung pathogenesis. Systemic inflammation has been shown to induce late pulmonary complications of SM exposure in some studies. 9 Nevertheless, it has been the subject of debate. 5
Over recent years, emerging data have demonstrated the crucial role of adipokines in COPD pathogenesis, whether stable or in exacerbation period. 1,7,10 Adipokines namely leptin and adiponectin are secreted from adipose tissue. 11 Leptin is secreted from white fat and inflammatory states induce its secretion. 12 Adiponectin is the most abundant protein secreted by fat tissue. 13 Adiponectin applies cardioprotective, antineoplastic, and anti-inflammatory effects. 14 Despite its anti-inflammatory effects on cardiovascular system, few studies have shown increased concentration of serum adiponectin in COPD. 1 It may indicate that adiponectin has also proinflammatory characteristics. Leptin, once discovered to have control over the food intake, recently has been shown to have proinflammatory roles. 15
Mouse studies have revealed that adiponectin has proinflammatory effects in certain circumstances and anti-inflammatory actions in the others. 11 The human data regarding the role of adiponectin in airway inflammation are inconclusive and different subgroups demonstrate various amounts. 11
Considering the possible role of adiponectin and leptin in SM poisoning lung complications, we did the present study to evaluate the concentration of these two main adipokines in chemical warfare patients (CWPs), who suffer from mustard lung, during the stable phase.
Materials and methods
Participants
Thirty CWPs who had documented SM poisoning history and suffered COPD entered the study (group 1). There were two control groups, 30 COPD patients (group 2) and 21 healthy nonsmoker adults (group 3). The age, sex, and body mass index (BMI) of controls were matched with the subjects. All COPD patients had irreversible airway obstruction according to the definition of American Thoracic Society (ATS; forced expiratory volume in 1s (FEV1) to forced vital capacity (FVC) <70% after 400 μg of albuterol inhalation). 16 One respiratory physician visited all patients. Exclusion criteria included asthma, bronchiectasis, tuberculosis, acute pulmonary infection, cardiovascular disorder, and other systemic illnesses (e.g. diabetes mellitus) and history of exacerbation or hospital admission in last 2 months. Smoking was an exclusion criterion for mustard lung patients in this study. All the participants were male.
This study was approved by the ethics committee of the Mashhad University of Medical Sciences, code number: 89413. All patients provided informed consent.
Measurements
Weight and height of all patients were measured by a nurse. BMI was calculated as weight (in kilogram) to height (in square meter). FEV1, FVC, and FEV1–FVC ratio were measured by standard spirometric techniques (multifunctional spirometer HI-801; Chest M.I. Inc., Tokyo, Japan). Severity of COPD was evaluated according to FEV1 based on global initiative for chronic obstructive lung disease (GOLD) guidelines. 17 All the patients performed a 6-min walk distance test according to the ATS guidelines. 18 Pulse oximetry was performed before and after the test. The Modified Medical Research Council scale was applied in patients for the assessment of severity of dyspnea. 19 According to the functional lung parameters, the BODE (BMI, obstruction, dyspnea, and exercise capacity) index was calculated in all patients. 19
Laboratory tests
Blood samples were obtained after 14 h fasting condition. Serum adiponectin and leptin concentrations were measured using enzyme-linked immunosorbent assay (Bender MedSystem, Medical System Diagnostic GmBH, Vienna, Austria). The values <10 ng/ml for adiponectin and <6 ng/ml for leptin were considered normal. Serum was stored at −70°C prior to analysis.
Statistical analysis
For summarizing the demographic characteristics of the groups, descriptive statistics were used. The continuous data are presented as percentages and means ± SDs. The normality of continuous variables was checked using the one sample Kolmogorov–Smirnov test. For continuous and categorical variables, independent student’s t tests and χ 2 tests were used to evaluate the statistical significance of any difference or relationship between parameters, respectively. Also, for comparison of variables among groups, analysis of variance (ANOVA) test was used.
Pearson’s and Spearman’s correlation coefficients were calculated. The value of p < 0.05 was considered significant. The data were analyzed using statistical package for social sciences (SPSS, version 11.5, Chicago, IL, USA).
Results
Participants
A total number of 81 participants were enrolled into this study. As shown in Figures 1 and 2, there were no statistically significant differences in mean serum levels of adiponectin and leptin among groups (p = 0.38 and p = 0.35, respectively).

The adiponectin levels (mean ± SD) in CWPs, COPDs, and healthy controls (p = 0.38). CWPs: chemical warfare patients; COPD: chronic obstructive pulmonary disease patient.
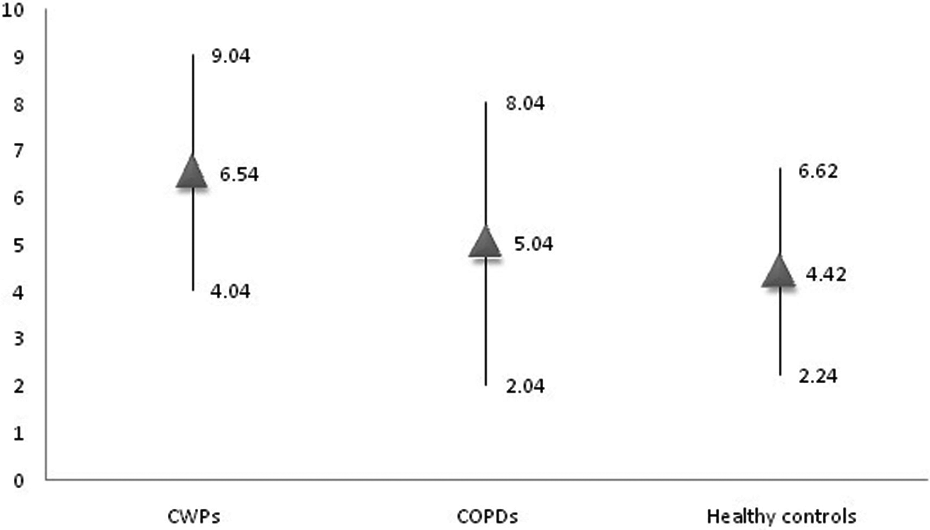
The leptin levels (mean ± SD) in CWPs, COPDs, and healthy controls (p = 0.35). CWPs: chemical warfare patients; COPD: chronic obstructive pulmonary disease patient.
Table 1 demonstrates demographic and laboratory data of CWP and COPD groups. The frequency of different stages of GOLD in both groups is shown in Table 2. There were no statistical difference in lung function parameters between CWPs and COPD patients (p = 0.6).
Demographic and laboratory data of CWP and COPD groups.

BMI: body mass index; COPD: chronic obstructive pulmonary disease; CWP: chemical warfare patient; FEV1: forced expiratory volume in 1s; 6MWD: 6-min walk distance; SpO2: oxygen saturation by pulse oximeter; BODE: BMI, obstruction, dyspnea, exercise; SGRQ: ST George Respiratory Questionnaire.
aData are shown as mean ± SD.
bThe value of p < 0.05 is considered significant.
The frequency of patients in different GOLD stages in CWP and COPD groups.

COPD: chronic obstructive pulmonary disease; CWP: chemical warfare patient; GOLD: global initiative for obstructive lung disease.
The serum adiponectin and lung function parameters in CWP and COPD groups
The mean concentrations of adiponectin according to the different stages of GOLD in patients are shown in Figure 3. The concentration of adiponectin increased with accordance to GOLD stage acceleration in COPD group. Mean adiponectin concentration was 2.2 ± 1.9 ng/ml and 5.2 ± 3.5 ng/ml in GOLD score 1 and 4, respectively. While mean adiponectin concentration was higher in GOLD score 4, the difference was not statistically significant. In CWPs, there was no upward trend in mean adiponectin concentration with GOLD score elevation. There was no statistically significant correlation between serum adiponectin and studied lung function parameters, as shown in Table 3. One-way ANOVA test did not show any statistically significant difference in adiponectin concentration according to GOLD staging in groups.

The mean adiponectin levels in different stages of GOLD in CWPs and COPDs. CWPs: chemical warfare patients; COPD: chronic obstructive pulmonary disease patient; GOLD: global initiative for chronic obstructive lung disease.
The correlation of serum adiponectin and studied lung function parameters.

COPD: chronic obstructive pulmonary disease; CWP: chemical warfare patient; FEV1: forced expiratory volume in 1s; 6MWD: 6-min walk distance; SpO2: oxygen saturation by pulse oximeter; BODE: body mass index, obstruction, dyspnea, exercise; SGRQ: ST George Respiratory Questionnaire; MMRC: Modified Medical Research Council.
The serum leptin and lung function parameters in CWP and COPD groups
The mean concentrations of leptin in patients according to the different stages of GOLD are shown in Figure 4. We did not find statistically significant correlation between the serum level of leptin and studied lung function parameters in patients (Table 4).

The mean leptin levels in different stages of GOLD in CWPs and COPDs. CWPs: chemical warfare patients; COPD: chronic obstructive pulmonary disease patient; GOLD: global initiative for chronic obstructive lung disease.
The correlation of serum leptin and studied lung function parameters.

COPD: chronic obstructive pulmonary disease; CWP: chemical warfare patient; FEV1: forced expiratory volume in 1s; 6MWD: 6-min walk distance; SpO2: oxygen saturation by pulse oximeter; BODE: body mass index, obstruction, dyspnea, exercise; SGRQ: ST George Respiratory Questionnaire; MMRC: Modified Medical Research Council.
The correlation of serum adiponectin and leptin levels and BMI
In both mustard lung and COPD groups, there was statistically significant correlation between leptin and adiponectin and BMI as shown in Figures 5 to 8.

The correlation of serum leptin with BMI in COPDs (r = 0.7, p = 0.001). BMI: body mass index; COPD: chronic obstructive pulmonary disease patient.

The correlation of serum adiponectin with BMI in COPDs (r = −0.3, p = 0.04). BMI: body mass index; COPD: chronic obstructive pulmonary disease patient.

The correlation of serum leptin with BMI in CWPs (r = 0.4, p = 0.03). BMI: body mass index; CWPs: chemical warfare patients.

The correlation of serum adiponectin with BMI in CWPs (r = −0.6, p = 0.003). BMI: body mass index; CWPs: chemical warfare patients.
According to BMI percentile, the adiponectin level was the highest in those with BMI <22.9 kg/m2.
The leptin/adiponectin ratio in different stages of GOLD in mustard lung patients
As it is mentioned in Figure 9, there was a downward trend in leptin/adiponectin ratio from GOLD 1 to 4, but it was not statistically different among stages in mustard lung patients (p = 0.8).
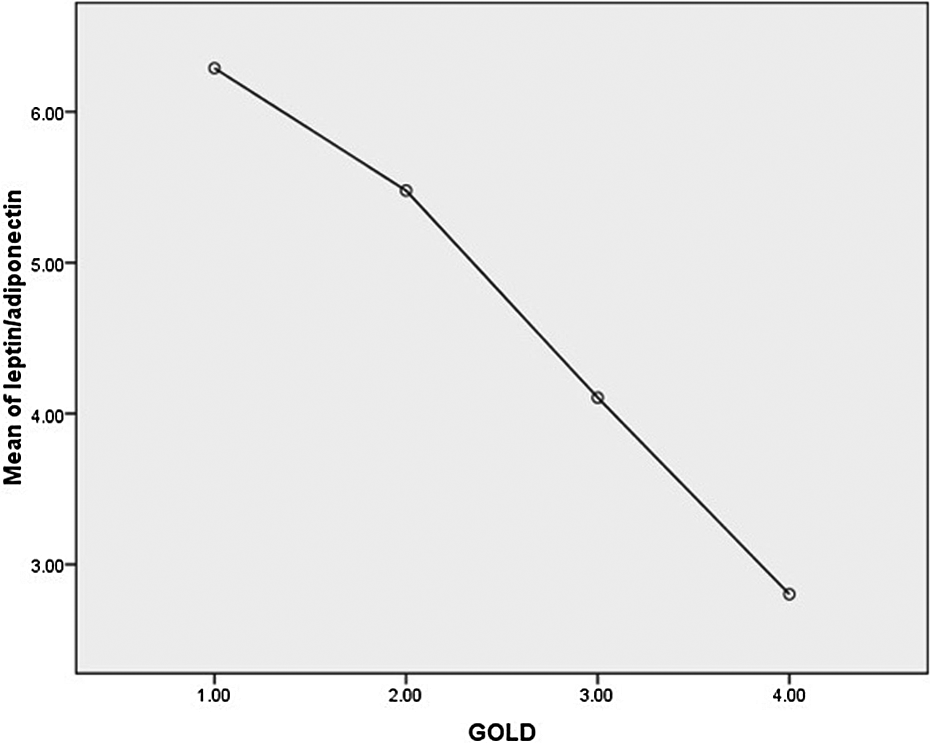
The leptin/adiponectin ratio in different GOLD stages in mustard lung patients (p = 0.8). GOLD: GOLD: global initiative for chronic obstructive lung disease.
Discussion
Based on emerging data, which is considered pivotal for adipokines in inflammatory processes, we evaluated these hormones in mustard lung patients. To our knowledge, the present study was the only research that has evaluated the serum level of adipokines in this group of the patients. We did not find any difference in serum adiponectin and leptin levels among the mustard lung patients, COPD patients, and healthy controls. There was a downward trend in serum leptin/adiponectin ratio from GOLD stage 1 to 4 in mustard lung patients. There were statistically significant correlations between BMI and serum leptin and adiponectin in mustard lung patients.
COPD is associated with persistent systemic inflammation, and several studies have reported the important role of serum inflammatory biomarkers like CRP, IL-8, IL-6, and tumor necrosis factor α in stable COPD patients. 20 The mechanistic pathway by which COPD results in systemic inflammation has not been elucidated yet. It has been proposed that lungs and peripheral tissues like adipose tissue are the main sources of inflammatory mediators. 13 There are three possibilities for this issue: the spillover of respiratory inflammation into systemic circulation, 21 genetic and constitutional factors may predispose COPD patients to both systemic and pulmonary inflammation, 22 and conversely, systemic inflammation may induce COPD. 23 Also, it should be noted that smoking by itself may contribute to the inflammation in COPD. 7,24,25
The role of adipokines in respiratory system has provoked debates. 26 Hypoxia or obesity in COPD patients may exaggerate the inflammatory basis by increased production and release of proinflammatory adipokines. 7 It has been proposed that adipose tissue represents a significant contributor of systemic inflammation in lower stages of COPD. 7 Systemic and airway leptin is shown to be increased in accordance with COPD severity 11 and is correlated with BMI values. 7
Sulfur mustard, a chemical weapon, is shown to induce considerable numbers of inflammatory cytokines including IL-1and IL-6. 27 It has been proposed that both oxidative stress and apoptosis are the recognized mechanisms that are more involved in mustard lung. 6 Given to the probable role of adipokines in COPD pathogenesis, we evaluated the concentration of leptin and adiponectin in mustard lung patients.
In our study, there were no statistically significant differences in adipokine levels among the mustard lung patients, COPD patients, and healthy controls. Piehl-Aulin et al. 28 showed the same result in concern to the similar circulating levels of leptin in stable COPD patients to healthy control but about adiponectin, there are studies that demonstrated the difference in mean adiponectin levels between patients and healthy controls. 29 –32
There were no statistically significant correlations between FEV1 and adiponectin and leptin in mustard lung patients. Also, the study by Kirdar et al. showed similar result of no significant correlation between FEV1 and adiponectin levels in stable COPD patients. 33 While adiponectin concentration was higher in mustard lung patients with GOLD stage 4 than those with stage 1, the difference was not statistically significant (p = 0.4).The serum level of leptin was higher in mustard lung patients with GOLD stage 1. However, the difference was not statistically significant (p = 0.2). COPD group showed a constant increase in adiponectin serum level with GOLD stage elevation from 1 to 4. Again one-way ANOVA test demonstrated no statistically significant difference between groups (p = 0.06). Similar to CWPs group, leptin concentration was higher in GOLD stage 1. There was no statistically significant difference in leptin concentration between groups (p = 0.2).
We found statistically significant correlation between level of leptin and adiponectin and BMI both in mustard lung patients and COPD patients. This finding was in agreement with previous studies on COPD patients. 32
It has been documented that COPD that has developed due to SM poisoning, known as mustard lung, to some extent is different from COPD due to smoking. 6 As we mentioned earlier, smoking per se is one of the potential factors in the development of systemic inflammation in COPD patients. In this study, all the CWPs were nonsmokers. The decrement in the leptin/adiponectin ratio by acceleration of GOLD, although was not significant, shows the possibility of ongoing inflammatory process. We think that the small sample size in CWP group is an important limit factor in the data analysis.
This study does have limitations. First and foremost was small sample size, as we mentioned earlier. According to the exclusion criteria of CWPs, all patients who were smokers had been excluded. Second, following the first limitation, the frequency of GOLD stages in CWPs was unequal. Mean values would have been better if the frequency of the patients in stages 3 and 4 be extended. Finally, it seems logical to do a same study in exacerbation of mustard lung.
Conclusion
As there is a proposed role of systemic inflammation in mustard lung patients, we studied the serum levels of adiponectin and leptin. We did not find any statistically significant difference in mean adiponectin and leptin levels between mustard lung patients and the controls. There was a downward trend in leptin/adiponectin ratio by acceleration of GOLD stages in mustard lung patients, which was not significant.
Footnotes
Acknowledgment
The authors wish to thank to M. Aalami for his wonderful assistance in performing the study.
Conflict of interest
The authors declared no conflicts of interest.
Funding
This study was financially supported by Mashhad University of Medical Sciences (code number: 89413).