
Abstract
Introduction:
Over the past decade, complementary and alternative medicine (CAM) has become increasingly popular around the world.
Objectives:
In this study, we aim to investigate how frequently CAM is used and the types of CAM methods used for dermatological disease in Eastern Turkey.
Materials and methods:
We recruited 1610 patients from our clinic for this study. The sociodemographic features and the CAM methods were investigated with a survey.
Results:
The most common dermatological disorders included contact dermatitis (21.4%), acne vulgaris (17.5%), fungal infections (10.9%), eczema (6.3%), and warts (5.7%). The ratio of patients using at least one CAM method was 43.7% and that of those using two or more CAM methods was 20.8%. The most commonly used CAM methods were those using henna, cologne, moisturizing cream, prayer, and herbal therapy. Some patients were found to use some interesting and unusual CAM methods, such as putting out a cigarette over the skin on the back for anthrax, applying raw meat for furuncle, using fuel oil and nitric acid for contact dermatitis.
Conclusions:
CAM methods are commonly used in our population. CAM methods often cause adverse reactions that may alter diagnostic skin findings and interfere with the efficacy of other medical therapies. Therefore, physicians should ask their patients about the use of CAM methods while collecting patient history. Physicians have a critical role in preventing improper use of CAM. In addition, further investigations into the efficacy, benefits, and risks of CAM methods should be carried out for better insight into those CAM methods.
Introduction
The National Center for Complementary and Alternative Medicine (NCCAM), a division of the National Institutes of Health, defines complementary and alternative medicine (CAM) as “a group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.” 1
The frequency of usage of CAM has been increasing in general population. 2,3 The prevalence of CAM use in the general population around the world ranged from 9 to 65%. 4 The incidence of CAM use in certain patient groups including rheumatic diseases, acquired immunodeficiency syndrome (AIDS), or cancer has been relatively well established. 5 In parallel with the increase in CAM use in the general population, the frequency of CAM use for dermatological diseases has been increasing. In the literature, the studies focused on the frequency of CAM use in psoriasis, atopic dermatitis, and acne are present. 6–8 However, the studies on the comparative frequency of CAM use in different countries are limited. 9–12
Herein, we investigated the frequency of CAM use and the types of CAM methods employed for dermatological disease in Eastern Turkey.
Methods
We recruited the patients who came to our dermatology clinic from January 1 to April 30, 2011, a 4-month period. Patients with any skin disease were included. The questions were answered by parents for patients who were younger than 12 years.
The survey included questions on patients’ dermatological diagnosis, age, sex, occupation, education level, living place (rural or urban area), number of previous doctor visits for the same reason, use of CAM, types of CAM methods (including henna, cologne, moisturizing cream, invocation, and herbal therapy), and sources that recommended using that type of CAM (including family, neighbor, friends, television, newspaper, Internet, doctor, pharmacist, and other medical staff).
The study protocol was carried out in accordance with the Helsinki Declaration and approved by the local research committee for ethics. All subjects were informed about the study protocol and written consents were obtained from all the participants.
Statistical analysis was performed with SPSS software (Statistical Package for the Social Sciences, version 15.0, SSPS Inc, Chicago, Ill, USA). Besides descriptive statistical analysis (mean ± SD, percentage), a chi-square test was used for group comparison. p < 0.05 was considered as a statistically significant
Results
Of these patients, 62.6% (1008 patients) were female and 37.4% (602 patients) were male. The mean age was 27.70 years (range from 1 year to 92 years). The analysis of patients’ education level showed 29.6% were illiterate, 23.4% had elementary school degree, 19.9% middle-school degree, 19.9% high-school degree, and 13.7% college degree.
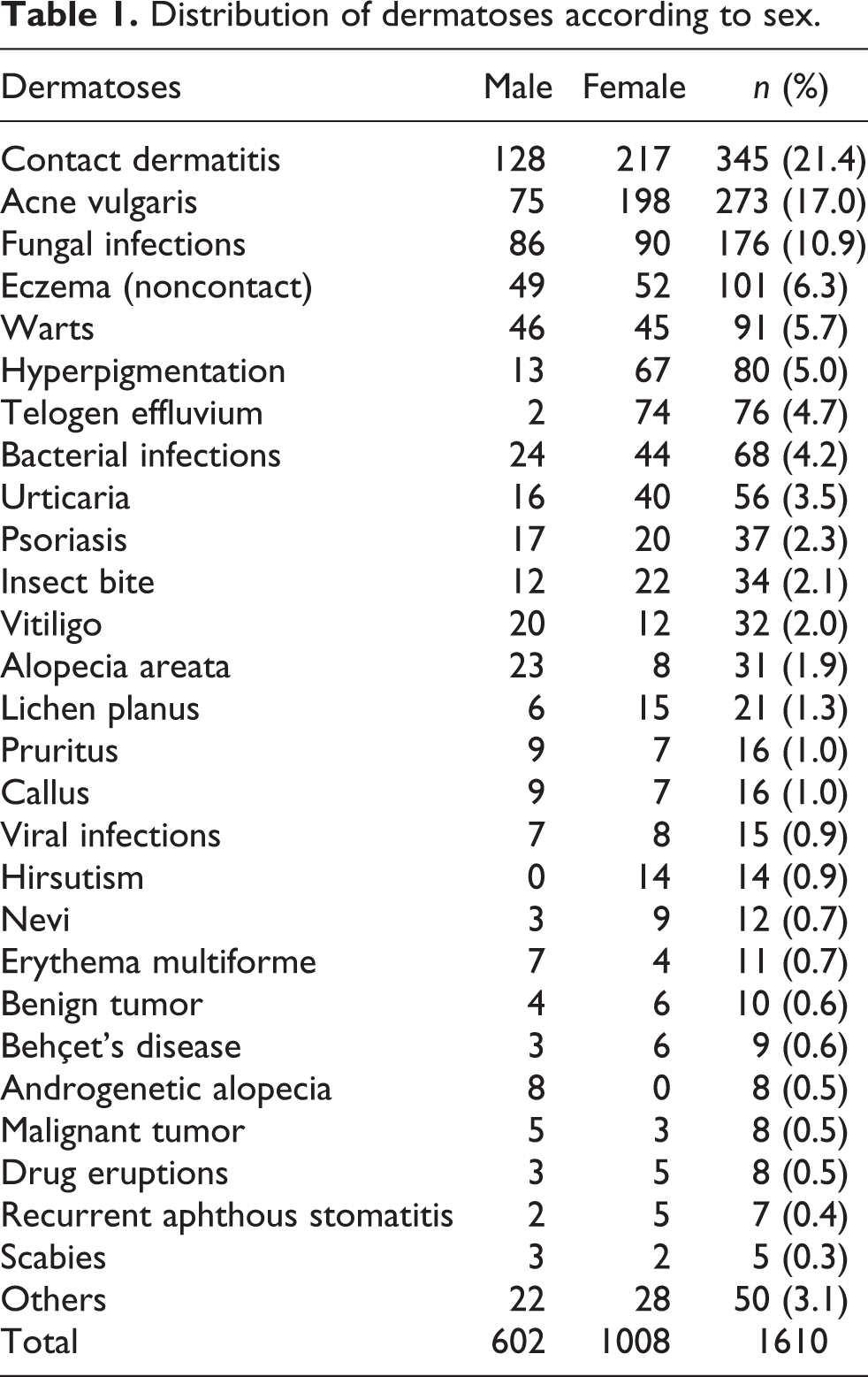
The most common five dermatological diseases were contact dermatitis 21.4% (345 patients), acne vulgaris 17% (273 patients), fungal infections 10.9% (176 patients), eczema (noncontact) 6.3% (101 patients), and warts 5.7% (91 patients). The disease distribution according to sex is shown in Table 1. The frequency of the patients using at least one type of CAM method was 43.7% (704 patients), and the frequency of patients using two or more CAM methods was 20.8% (335 patients). The most common diagnoses of the patients using CAM were contact dermatitis (24.0%), acne vulgaris (17.5%), fungal infections (10.7%), and viral infections (7.5%) (Figure 1). The most commonly used CAM methods were henna (Figure 2), cologne, moisturizing cream, invocation, herbal therapy (Figure 3), and lemon juice (Figure 4). The sex distribution according to CAM use is shown in Table 2. In some patients, use of interesting and unusual CAM methods was detected such as putting out a cigarette over the back skin for anthrax (Figure 5); raw meat for furuncle and paronychia (Figure 6); fuel oil nitric acid and car battery for contact dermatitis; fuel oil for tattoo (Figure 7) and hot glass for herpes simplex infection; eating hedgehog for psoriasis: pitch for pruritus (Figure 8) and leeching for contact dermatitis and tinea pedis.

Percentages of unconventional therapy use according to diagnosis. RAS: recurrent aphthous stomatitis.

Application of henna for tinea pedis.

Lesions of psoriasis and herbal therapy.

Irritant contact dermatitis after lemon juice application for eczema.

Putting out a cigarette over the back skin for anthrax.

Application of raw meat for paronychia.

Application of fuel oil for tattoo.

Pitch application for pruritis.
Distribution of dermatoses according to sex.
Distribution of unconventional therapy according to the sex of the patients.

a p < 0.05, statistically significant.
There was no statistically significant difference between CAM use and sex, age, education level, and living place. There was statistically significant correlation between the frequency of CAM use and the frequency of clinic visit due to dermatological symptoms. The frequency of CAM use at first visit was 68.6%, in patients having two to five visits was 26.3%, and in patients having more than six visits was 5.1%. The analysis of relationship between CAM use and dermatological diseases showed that lemon juice (24%) was more commonly used for acne vulgaris, henna (51%) for fungal infections, cologne (33%) for eczemas, grape molasses (86%) for aphthous stomatitis, and onion (33%) for bacterial infections. The frequency of the most common three CAM methods according to dermatological diseases is shown in Table 3.
The most common used three CAM modalities for dermatological disease.

Discussion
The study was carried out in people from a lower socioeconomic class on Eastern Turkey. The use of CAM was 43.7%. This result is consistent with other studies. On the other hand, we did not find any relationship with the use of CAM and the education level of the study population. CAM was used for many different indications, some of which were extraordinary and very different.
For dermatology patients, the prevalence of CAM use is high. Only a few studies on the prevalence of CAM use have been performed for different countries, and only one study on the prevalence of CAM use for Turkey. 12 In Sweden, Berg and Arnetz 13 reported a 35% lifetime prevalence of CAM use among 118 patients. The frequency of CAM use was 43.7% in our study. Our rate was lower than that showed in one study from the United States (49%), and higher than the results from other studies from Turkey (33.5%), Singapore (25.7%), and Taiwan (41%). 9–12 These differences may depend on social, cultural, and religious differences.
In our study, no statistically significant difference between CAM use and sex, age, education level, and living place was detected that was similar to the findings of Gonul et al. 12 The study from Singapore showed the frequency of CAM use increased in patients with higher education levels and prolonged disease duration. 9 In our study, there was no significant correlation between CAM use and education level. However, there was correlation between the frequency of CAM use and the frequency of clinic visits due to dermatological symptoms. The frequency of CAM use at first visit was 68.6%, and in patients having more than six visits was 5.1%. This finding may imply that most of these patients first applied CAM methods, and then used other medical treatments when CAM methods were ineffective.
The types of CAM methods used show wide variation. Currently, NCCAM divides CAM into the following categories: alternative medical systems (acupuncture, ayurveda, homeopathy, and naturopathy), biologically based therapies (chelation, folk medicine, nonvitamin nonmineral natural products, diet-based therapies, and megavitamin therapy), manipulative and body-based therapies (chiropractic care, massage), and mind–body therapies (biofeedback, relaxation techniques, hypnosis, yoga, Tai Chi, Qi Gong, healing rituals, energy healing, or Reiki). 1 Gonul et al. study showed cologne, moisturizing cream, invocation, herbal therapy, and olive oil were the most common CAM methods. 12 One of the recent studies showed the use of CAM is common in the United States and the most commonly used CAM modality was nonvitamin, nonmineral, natural products (i.e. herbals). 14 The other common methods such as acupuncture, ayurveda, and homeopathy were not used in our patients group. The most commonly used methods were henna (13.7%), cologne (11.6%), invocation (8.9%), moisturizing cream (8.8%), and herbal therapy (6.9%). In addition, different CAM methods were used such as Turkish delight, dough, and onion for bacterial infections; and water from Lake for eczemas. Those different applications may be related to regional differences and people’s belief in the healing features of the water of Lake Van. The relationship between used CAM modalities and sex showed use of garlic was more common in males, and use of herbal therapy, lemon juice, egg, and cosmetic products more common in females. The common use of garlic in males may be due to a higher incidence of alopecia areata in males.
Baron et al. found that CAM was more commonly used for eczema (34%) or for psoriasis (31%). 11 Similarly, See et al. showed that dermatological diseases that commonly employed CAM were psoriasis (39%) and dermatitis/eczema (33%). 9 In Gonul et al.’s study, the most commonly used CAM for dermatological diseases were acne, psoriasis, and contact dermatitis, respectively. 12 In our study, the most common CAM used dermatological diseases were contact dermatis, acne, fungal infections, and warts, respectively. In our study, the frequency of CAM use for psoriasis was lower and might be related to low prevalence of psoriasis in our patient group.
In our study, there was a relationship between CAM methods and some type of disease including contact dermatitis and the application of henna and humectants; acne and the application of lemon juice; fungal infections and the application of henna; fungal infections and the application of cologne; warts and spiritual healing; bacterial infections and the application of onion; telogen effluvium and the application of olive oil; alopecia areata and the application of garlic; and pruritus and the application of cologne. The patients usually used cologne and lemon juice for disinfectant purposes, and used moisturizing cream for symptomatic relaxation.
The benefit–risk analysis is very challenging in CAM use due to the presence of limited studies and lack of enough knowledge on the methods employed. 15 In general, herbal remedies usually are considered natural and safe; however, herbal remedies may cause serious and life-threatening adverse effects. The most common side effect is contact dermatitis. 16 In addition, more serious adverse effects due to herbal remedies have been reported in the literature, for instance, two cases developed nephropathy and subsequently end-stage renal failure after taking herbal remedies to treat eczema. 9 In particular, Chinese herbal remedies with severe side effects have been reported. Chinese herbals usually contain high levels of arsenic that may cause intoxication, Bowen disease, arsenic keratosis, and even squamous cell carcinoma. 16 Eleven cases of liver damage after using Chinese herbal remedies for skin conditions were reported. 17 In addition, dilated cardiomyopathy was reported after applying Chinese herbal medicine for treating eczema. 18 The side effects of CAM are not limited to herbal remedies. 19 Systemic side effects related to essential oils used for aromatherapy were reported as well. 20 In our study, no CAM therapy-related systemic side effects were detected. In addition, herbal remedies used for other medical conditions may produce skin lesions (Figure 9). 21 Besides these side effects, CAM use may cause delays in receiving proper medical treatment, or discontinuation/rejection of medical treatments, and increased unnecessary expense. In our study, the high frequency of CAM use at first visit might cause a delay in receiving proper medical treatment and alterations in the existent skin findings that made the accurate diagnosis more challenging.

Irritant contact dermatitis after garlic application for arthralgia.
CAM use is common in dermatological diseases. Most patients tend to hide their CAM use. Our results indicate that the use of CAM methods is widespread. The use of CAM may cause adverse side effects, alter diagnostic skin findings, and interact with other medical treatments that may affect the efficacy of medical treatments. Therefore, physicians should take a detailed medical history, including CAM use. Physicians have a critical role in preventing improper use of CAM. In addition, further investigations on the efficacy, benefits, and risks of CAM methods should be performed for better insight into those CAM methods.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.