
Abstract
Waste management workers (WMWs) around the world are at risk of work-related health disorders. The influence of employment duration on individuals occupationally exposed to solid waste was investigated in this study. The study comprised (n = 280) 180 WMWs and 100 controls. Employment duration was obtained from questionnaire survey and categorized into three groups: group I (0.5–2 years), group II (>2–4 years) and group III (>4–6 years). Blood sample (10 ml) was collected from the antecubital vein of subjects for analysis. WMWs exhibited significantly (p < 0.001) elevated inflammatory markers (erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and ceruloplasmin (Cp)) relative to control. While Cp increased, ESR and CRP decreased with increasing WMWs’ employment duration. Alteration in oxidant/antioxidant markers was characterized by significant (p < 0.001) decrease in ferric-reducing ability of plasma (FRAP) and catalase activity together with marked (p < 0.01) elevation of thiobarbituric acid reactive substances (TBARS) and uric acid (UA). TBARS, UA and FRAP increased while catalase decreased with WMWs’ employment duration. In addition, WMWs exhibited significantly (p < 0.01) elevated immunoglobulin A (IgA) and IgG, which also increased and decreased, respectively, with job duration. The significantly (p < 0.01) decreased haemoglobin and haematocrit levels as well as the significantly (p < 0.001) elevated total leukocytes in WMWs increased with employment duration. Alanine aminotransferase increased and albumin decreased significantly (p < 0.05) in WMWs, and these changes also increased and decreased, respectively, with job duration. Data suggest that levels of alteration of important systemic markers of health/disease are related to WMWs’ employment or exposure duration.
Introduction
The increased volume and variety of solid wastes arising from increased flow of goods and services, changed lifestyle and consumption pattern of Nigerians in recent times is dangerously alarming and a major source of public health concern. The cities, which are the engines of social modernization and economic growth, and areas where globalization impacts are mainly manifested are worse hit. It is worrisome that the annual solid waste generation in Nigeria rose from about 4.5 million tonnes in 1999 to about 25 million tonnes in 2009. 1,2 These figures are expected to escalate further with previous report from a study by the European Environment Agency, which had indicated that the amount of municipal waste was expected to increase by 25% from 2005 to 2020. 3
Wastes are generally classified into groups that pose similar risks to the environment and human health to facilitate their management and appropriate disposal. They have been classified as one of the six types according to Waste Classification Guidelines (2009) as follows: (1) special waste, comprising of clinical and related waste, asbestos waste and waste tyres; (2) liquid waste, which refers to any waste that has an angle of repose of less than 5° above horizontal, becomes free-flowing at or below 60°C or when it is transported or is generally not capable of being picked up by a spade or a shovel; (3) hazardous waste, for example, coal tar or coal tar pitch waste, lead–acid or nickel–cadmium batteries, lead paint waste arising otherwise from residential premises or educational or child care institutions or any mixture of the wastes in this category; (4) general solid waste (putrescible), for example, household waste that contains putrescible organics, waste from litter bins collected by or on behalf of local councils, manure and night soil, disposable nappies, incontinence pads or sanitary napkins, food waste, animal waste, grit or screenings from sewage treatment systems that have been dewatered so that the grit or screenings do not contain free liquids or any mixture of the wastes referred to above; (5) general solid waste (non-putrescible), for example, glass, plastic, rubber, plasterboard, ceramics, bricks, concrete or metal; paper or cardboard; household waste from municipal clean-up that does not contain food waste; garden waste; wood waste; waste contaminated with lead (including lead paint waste) from residential premises or educational or child care institutions; building cavity dust waste removed from residential premises or educational or child care institutions; synthetic fibre waste (from materials such as fibreglass, polyesters and other plastics); virgin excavated natural material; building and demolition waste; asphalt waste; biosolids and so on and (6) restricted solid waste. Although no wastes have been pre-classified by the Environmental Protection Authority (EPA) as ‘restricted solid waste’ currently, restricted solid waste therefore only includes wastes assessed and classified as such in using chemical assessment where (i) the waste is not a special waste, liquid waste, a waste pre-classified by the EPA or a waste possessing hazardous characteristics and (ii) the composition of the waste is not known.
In Nigeria and most other developing countries, achieving effective municipal solid waste (MSW) management remains a major challenge and waste generation and accumulation continue to constitute important environmental and public health concern. Although the general population is at risk of adverse health consequences due to exposure to MSW, the waste management workers (WMWs), however, are prone to greater health risks from occupational exposure, which predisposes them to frequent and continuous contact with the harmful components of the waste materials. The MSW, most of which is dumped in low-lying areas at the outskirts of the cities, serves as the breeding ground for different types of pathogenic organisms. Individuals involved in the collection, transport, transfer and management of this waste are exposed to elevated concentrations of biological aerosols such as microbial and non-microbial volatile organic compounds. 4,5
Several studies have related exposure to bioaerosol to the presence of airway inflammation and subsequent symptoms in workers in the household waste collecting and organic waste composting industries. 6–8 Airway inflammation, in these studies, was mainly mediated by neutrophils and independent of specific antibodies, probably caused by direct interaction of inflammatory biological agents such as endotoxins or glucans with epithelial tissues and infiltrating white blood cells (WBCs). Similarly, exposure to wastes has been associated with hypersensitivity pneumonitis, occupational asthma, sinusitis, runny or stuffy nose, frequent sneezing, headache, dry cough, wheezing breath and chest discomfort or pain. 9 The production of proinflammatory cytokines, such as interleukin (IL)-1β, IL-6, IL-8, and tumour necrosis factor-α plays a major role in these inflammatory processes. 10,11 Furthermore, systemic inflammatory, oxidative stress and immune-related changes have also been reported in separate studies following occupational exposure to wastes. 12–15 Although only a few studies have reported alterations in the levels of important biomarkers of health and disease following occupational exposure to solid wastes, rarely have these studies paid any attention to interrelationship between specific biomarkers, particularly in relation to employment or job duration. In the present study, therefore, we investigated how important biomarkers of systemic inflammation, antioxidant/oxidative stress status, immune and haematological functions are altered in relation to employment or job duration of MSW management workers of Ogun State in southwest Nigeria.
Materials and methods
Subjects and study design
The study comprised of a total of 280 subjects (aged between 25 and 57 years with a median of 37 years), consisting of 180 male and female (0.9:1.1) WMWs and 100 male and female (0.9:1.1) healthy non-WMWs. These subjects were selected by purposive sampling in line with our previous study, 15 from five private waste management companies in Ijebu-Ode, Ago-Iwoye and Sagamu cities of Ogun State in southwest Nigeria. The WMWs work 8 h daily for 6 days every week. The length of employment, which was used as a measure of duration of exposure, 16 was obtained from a questionnaire survey and categorized by convenience into three groups: group I (0.5–2 years), group II (>2–4 years) and group III (>4–6 years). The study was conducted simultaneously in control and WMWs to eliminate the confounding effect of seasonal variation on health response. Exclusion criteria included medical conditions like diabetes, asthma, hypertension, malaria and individuals on medications capable of interfering with inflammatory, immune and non-immune-related haematological and oxidative stress parameters. 17–20 Individuals with any visible wound or lesion, which may predispose to infection and/or inflammation, were also not recruited. Informed written consent was obtained from subjects in accordance with Helsinki Declaration 21 before the commencement of study. Study protocol was approved by the Scientific and Ethics Review Committee (SERC) of the Olabisi Onabanjo University Teaching Hospital (approval number OOUTH/DA.226/T/2).
Blood sample (10 ml) was collected from the antecubital vein of the subjects after an overnight fast of 12–14 h for analysis and dispensed into plain bottle (3.0 ml), lithium heparin bottle (4.0 ml) and tripotassium ethylenediaminetetraacetic acid bottle (3.0 ml) for the determination of immunological response markers, biochemical and haematological parameters, respectively.
Evaluation of systemic inflammation
Systemic inflammation was evaluated by measuring plasma ceruloplasmin (Cp), C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). Cp was estimated from its oxidase activity using o-dianisidine dihydrochloride as described by Schoslnsky et al. 22 Briefly, equal volumes of sodium acetate buffer and serum sample in two test tubes were incubated at 30°C in water bath for 5 and 15 min, respectively, with o-dianisidine dihydrochloride reagent followed by sulfuric acid (9.0 M) to form the purplish-red solution measured spectrophotometrically at 540 nm. Cp oxidase activity was quantified using the product of difference in absorbance of the purplish-red solution and Σ = 9.6 M absorptivity of coloured solution in terms of substrate consumed (milliliter per micromole per centimetre).
CRP was determined following the principle described by Eda et al. 23 Serum CRP concentration was measured by immunoturbidimetry with latex particles coated with monoclonal anti-CRP antibodies sensitized with specific antibodies. The precipitate (concentration of which is directly proportional to the concentration of CRP in the serum) was determined turbidimetrically at 552 nm, with inter-assay and intra-assay coefficient of variation of 2.9% and 1.8%, respectively.
ESR was measured according to the method described by Westergren. 24 Briefly, blood sample well-mixed with trisodium citrate was drawn up into the Westergren tube to the 200 mm mark. This was placed vertical and left unperturbed, free from draughts or direct exposure to sunlight for 60 min. The height of the clear plasma above the upper limit of the column of sedimenting cells was read to the nearest millimetre.
Assessment of humoral and cell-mediated immunity
Immunoglobulin (Ig) classes (IgG, IgA and IgM) were quantified by the single radial immunodiffusion method based on the principle of antigen–antibody precipitation reaction in agar plates. 25 Briefly, agar plates were prepared by incorporating antihuman IgG, IgA and IgM (Dade Behring, Germany) into 3% noble agar (Difco Laboratories, Detroit, Michigan, USA) in phosphate-buffered saline. Test samples were placed in small antigen wells and allowed to diffuse into the agar to form a ring of antigen–antibody precipitate around the well. The diameter of the precipitate ring was measured to the nearest 0.1 mm using a Hyland viewer with a micrometer eyepiece (Fisher Scientific Co, Pittsburgh, PA, USA) and this is proportionate to the concentration of the immunoglobulin. Specific Ig concentration in the test samples was determined by comparing the ring diameter with the standard graphic curve obtained with the standard Ig concentrations.
Adenosine deaminase (ADA) activity was determined at 37°C according to the method described by Martinek. 26 This was based on the principle of Berthelot reaction in which ammonia liberated from adenosine reacts to produce a coloured indophenol complex, which was then quantified spectrophotometrically (UNICO Spectrophotometer 2100, United Products Instruments, Inc. Dayton, USA). One unit of ADA activity was defined as the amount of enzyme required to release 1 mmol of ammonia per minute from adenosine under standard assay conditions, and the results were expressed as units per litre per minute.
Haematological assessment
Haematological parameters were measured using a fully automated Haematology Analyzer Mindray BC 3000 PLUS (Mindray Bio-Medical Electronics Co. Ltd, Shenzhen, China). WBC differential counts were estimated microscopically from Leishman’s-stained blood smear preparations on glass slides according to the procedure described by Dacie and Lewis. 27
Evaluation of oxidant/antioxidant markers
Lipid peroxide levels were measured according to the method of Varshney and Kale, 28 and thiobarbituric acid reactive substances (TBARS) were quantified spectrophotometrically at 532 nm using Σ = 1.56 × 105 M−1 cm−1 as molar extinction coefficient. 29 Uric acid (UA) was determined following the principle described by Fossati et al. 30 using commercial kit obtained from Randox Laboratories Ltd (Crumlin, UK). Ferric-reducing ability of plasma (FRAP) was determined by measuring the ability of plasma to reduce ferric to ferrous ion by the method of Benzie and Strain. 31 Reduced glutathione (GSH) content was measured by the method of Beutler et al. 32 using 5,5′dithiobis-2-nitrobenzoic acid. Catalase (CAT) activity, which was based on the ability of the enzyme to induce the disappearance of hydrogen peroxide, was determined according to the spectrophotometric method described by Claiborne. 33 Superoxide dismutase (SOD) activity was determined according to the method described by Magwere et al. 34 and based on the ability of the enzyme to inhibit the spontaneous oxidation of epinephrine to adrenochrome.
Assessment of hepatic and renal functions
Liver function was assessed by measuring plasma activities of aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP) as well as total cholesterol (TC) and triglyceride (TG) concentrations. AST and ALT activities were determined following the principle described by Reitman and Frankel, 35 while ALP activity was estimated according to the method described by Roy. 36 TC and TG were estimated by the principle described by Trinder 37 using commercial kits obtained from Randox Laboratories Ltd (Crumlin, UK). Renal function was assessed by measuring blood urea nitrogen (BUN) and plasma creatinine concentrations following the principle of condensation of diacetyl with urea described by Fearon 38 and the method described by Jaffe et al., 39 respectively, using commercial kits obtained from Randox Laboratories Ltd. (Crumlin, UK).
Statistical analysis
Results are expressed as mean ± SD. Differences between groups were determined by one-way analysis of variance using Statistical Package for Social Sciences (SPSS) software for windows. Post hoc test was performed for inter-group comparisons using the least significant difference (LSD) test, 40 and p < 0.05 was considered significant.
Results
Biophysical characteristics
The biophysical characteristics of subjects are presented in Table 1. Both WMW groups and control are comparable with respect to mean age and blood pressure (both systolic and diastolic). The body mass index (BMI) of subjects in all groups falls within healthy range (reference value 18.5 to 24.9). Smoking and alcohol-use pattern are also comparable and not significantly different between the various groups. There is a significant difference in male to female ratio with control and group III (i.e. >4–6 years) having more male subjects when compared with the other two groups.
Biophysical data of control and solid waste workers in relation with employment duration.

SBP: systolic blood pressure, DBP: diastolic blood pressure, BMI: body mass index, M: male, F: female.
aData expressed as mean ± SD.
bHealthy BMI range is from 18.5 to 24.9.
cPercentage of individuals.
Systemic inflammation
Figure 1 summarizes the levels of ESR, Cp and CRP of WMWs and control. All parameters increased with increasing job or employment duration. ESR significantly (p < 0.001) increased by 72.1%, 53.7% and 16.8%, Cp by 15.6%, 19.5% and 50.2% and CRP by 46.2%, 38.5% and 23.1% in WMW groups I, II and III (i.e. 0.5–2, >2–4 and >4–6 years), respectively, when compared with control.

Changes in inflammatory indices of solid waste workers in relation to employment duration compared with control. Data are expressed as mean ± SD. Data in parentheses represent percentage of subjects with values outside the reference range. Reference value: ESR (5–15 mm hr−1), Cp (62–140 U/l), CRP (0.3–1.5 mg 100 ml−1). WMWs: Waste management workers; ESR: erythrocyte sedimentation rate; Cp: ceruloplasmin; CRP: C-reactive protein. a p < 0.001 when compared with control. b p < 0.05 when compared with control. c p < 0.05 when compared with WMWs >2–4 years. d p < 0.05 when compared with WMWs >4–6 years. e p < 0.001 when compared with WMWs 0.5–2 years.
Immune function
Figure 2 shows the result for humoral and cellular immunity of both WMWs and control. Immune function changes across the groups revealed significant (p < 0.01) increase in IgA by 17.32%, 27.18% and 46.13% and IgG by 45.54%, 40.49% and 7.39% in WMW groups I, II and III (i.e. 0.5–2, >2–4 and >4–6 years), respectively, when compared with control. While the changes in IgA levels increased with the length of employment, IgG was observed to decrease across the group. Other immune markers did not change significantly (p > 0.05) across the groups relative to the control.
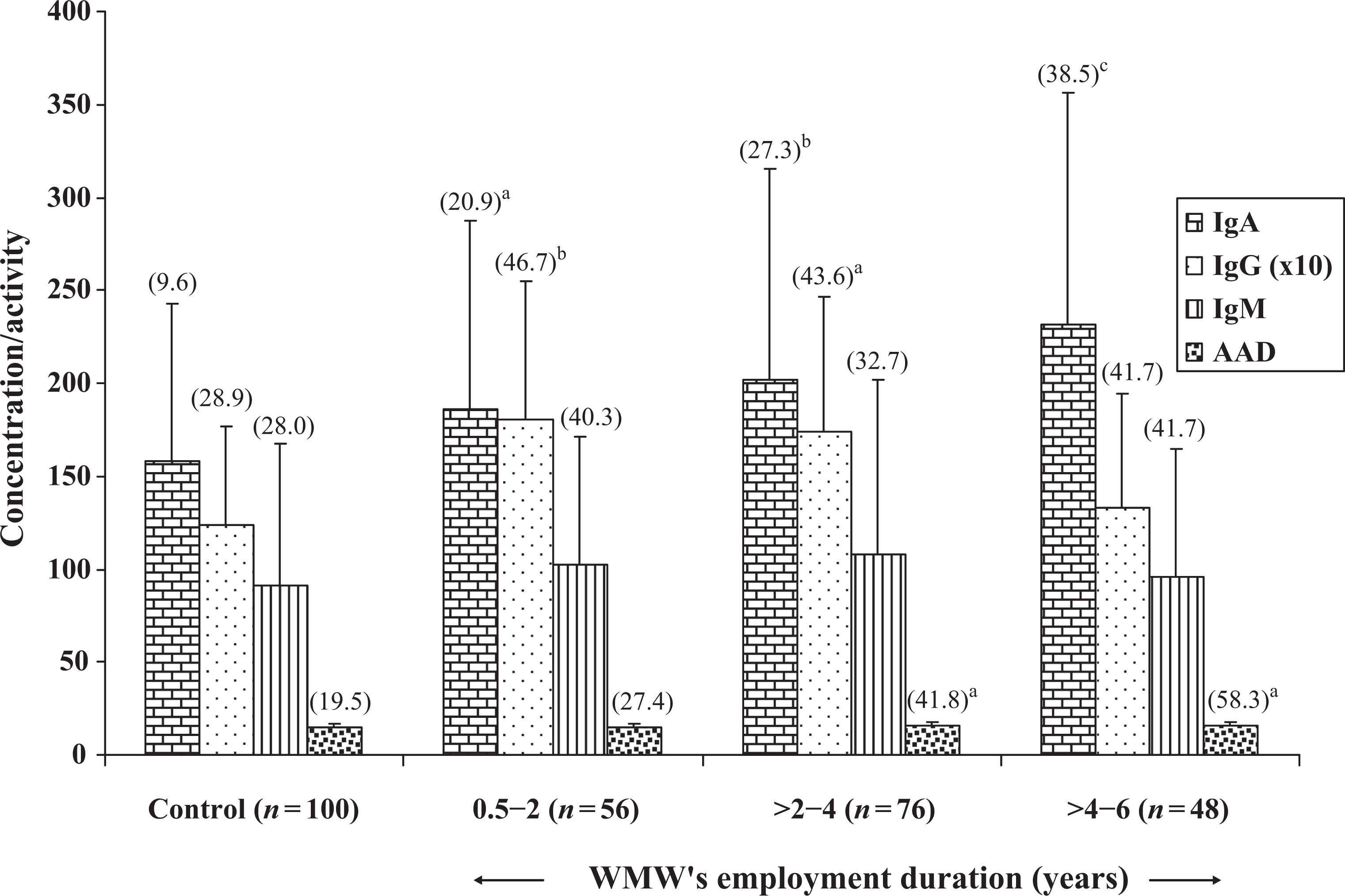
Changes in immune markers of solid waste workers in relation to job duration compared with control. Data are mean ± SD. Data in parentheses represent percentage of subjects with values outside the reference range. Reference value: IgA (81–211 mg dl−1), IgG (688–1251 mg dl−1), IgM (65–134 mg dl−1), ADA (5–15 U ml−1). WMWs: Waste management workers. Ig: Immunoglobulin (in milligram per decilitre), ADA: adenosine deaminase (in units per litre). a p < 0.05 when compared with control. b p < 0.01 when compared with control. c p < 0.001 when compared with control.
Oxidant/antioxidant parameters
Figure 3 depicts blood levels of TBARS, GSH, UA and FRAP, while the activities of SOD and CAT are shown in Figure 4 in WMWs and control. Changes in oxidative stress markers include significant increase in TBARS by 64.32%, 71.35% and 92.39% (p < 0.001) and UA by 17.09%, 17.59% and 18.59% (p < 0.01) as well as significant (p < 0.001) decrease in FRAP by 16.91%, 17.82% and 21.89% and CAT activity by 11.51%, 8.53% and 5.02% in WMW groups I, II and III (i.e. 0.5–2, >2–4 and >4–6 years), respectively, when compared with control. Apart from CAT activity, which decreased across the groups, TBARS, UA and FRAP increased with increasing employment duration of WMWs. Other oxidative stress markers did not change significantly (p > 0.05) across the groups relative to the control.

Changes in non-enzymic markers of oxidative stress in solid waste workers in relation to job duration compared with control. Data are mean ± SD. TBARS: thiobarbituric acid reactive substances (in nanomoles per litre), GSH: reduced glutathione (in milligram per decilitre), UA: uric acid (in milligram per decilitre), FRAP: Ferric-reducing ability of plasma (in millimole per litre). a p < 0.01 when compared with control. b p < 0.001 when compared with control. c p < 0.05 when compared with control.

Changes in markers of oxidative stress/antioxidant status of solid waste workers in relation to job duration compared with control. Data are mean ± SD. SOD: superoxide dismutase (expressed as units of enzymes required to inhibit autooxidation of adrenaline to adrenochrome), CAT: catalase (expressed as micromoles of hydrogen peroxide consumed per minute per milligram of haemoglobin). a p < 0.05 when compared with control; b p < 0.001 when compared with control; c p < 0.01 when compared with control.
Haematological parameters
Table 2 shows the haematological parameters of WMWs’ groups and control. Haematological changes include significant decrease (p < 0.01) in haemoglobin by 3.73%, 5.44% and 6.26% and haematocrit by 3.91%, 4.82% and 5.32%, while significant increase (p < 0.001) in WBC by 11.76%, 15.68% and 31.37% in WMW groups I, II and III (i.e. 0.5–2, >2–4 and >4–6 years), respectively. WBC differential counts showed that neutrophils increased by 4.09% in WMW group I, 0.5–2 years, and decreased by 1.72% and 5.59% in WMW groups II and III, >2–4 and >4–6 years, respectively, relative to control. Lymphocytes decreased by 2.07% in WMW group I (i.e. 0.5–2 years), and increased by 5.64% and 9.55% in WMW groups II and III (i.e. >2–4 and >4–6 years), respectively, relative to control. Eosinophil increased significantly (p < 0.01) by 44.62%, 50.00% and 58.17% and monocytes significantly increased (p < 0.05) by 25.44%, 26.03% and 36.09% in WMW groups I, II and III (i.e. 0.5–2, >2–4 and >4–6 years), respectively, relative to control. No significant (p > 0.05) change was observed in platelet count across the groups relative to control.
Changes in haematological parameters in various groups of solid waste workers in relation to job duration compared with control.a
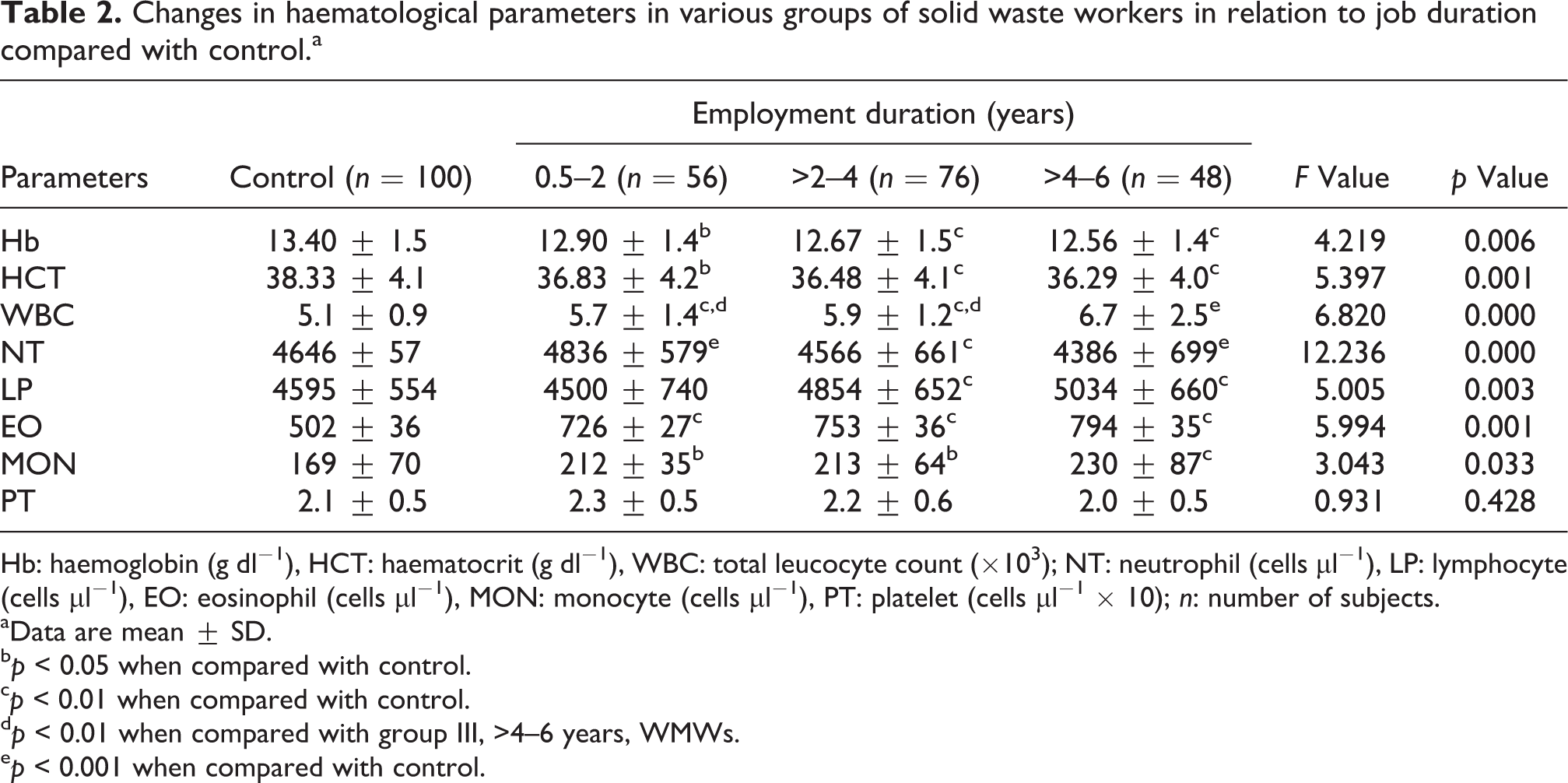
Hb: haemoglobin (g dl−1), HCT: haematocrit (g dl−1), WBC: total leucocyte count (×103); NT: neutrophil (cells µl−1), LP: lymphocyte (cells µl−1), EO: eosinophil (cells µl−1), MON: monocyte (cells µl−1), PT: platelet (cells µl−1 × 10); n: number of subjects.
aData are mean ± SD.
b p < 0.05 when compared with control.
c p < 0.01 when compared with control.
d p < 0.01 when compared with group III, >4–6 years, WMWs.
e p < 0.001 when compared with control.
Hepatic and renal functions
The effect
Changes in liver and renal functions in various groups of solid waste workers in relation to job duration compared with controls.a

ALB: albumin (g dl−1), AST: aspartate aminotransferase (U l−1), ALT: alanine aminotransferase (U l−1), ALP: alkaline phosphatase (U l−1), TC: total cholesterol (mg dl−1), TG: triglyceride (mg dl−1), BUN: blood urea nitrogen (mg dl−1), CREA: creatinine (mg dl−1).
aData are mean ± SD. Data in parentheses represent percentage of subjects with values outside the reference range. Reference value: ALB (3–5 g l−1), AST (6–24 U l−1), ALT (2–12 U l−1), ALP (10–35 U l−1), TC (120–200 mg dl−1), TG (65–195 mg dl−1), BUN (15–35 mg dl−1), CREA (0.5–1.2 mg dl−1).
b p < 0.01 when compared with control.
c p < 0.05 when compared with control.
d p < 0.01 when compared with group II, >2–4 years, WMWs.
e p < 0.05 when compared with group III, >4–6 years, WMWs.
Discussion
Exposure to MSW elevated the levels of systemic inflammatory markers in all categories of WMWs in this study relative to control subjects suggesting ongoing inflammatory process in line with our previous report. 15 We observed that ESR and Cp decreased and increased, respectively, with increasing WMWs’ employment duration or years of exposure to solid wastes, while the change in CRP (which increased significantly relative to the non-WMWs control) between the various categories of WMWs appear insignificant. CRP and Cp are acute phase proteins with significant diagnostic roles in inflammatory conditions. 41 ESR, which can be influenced by Ig levels, provides a measure of inflammation and reflects concentrations of the acute phase proteins, fibrinogen and α-globulins. 42 CRP, on the other hand, plays a key role in the host’s defence against infection 43 and the levels are highest in bacterial infection. 44,45 During inflammatory processes, CRP level is known to rise dramatically in the body and the acute phase response develops in a wide range of acute and chronic inflammatory conditions like bacterial, viral or fungal infections due to a rise in the plasma concentration of IL-6 produced predominantly by macrophages and adipocytes. 46,47 Although the elevated levels of ESR decreased and that of CRP did not change significantly with increasing job duration among the WMWs in this study, the marked increase in Cp, which has been shown to increase late during inflammation and fluctuate less than other inflammatory markers, 48 strongly supports our previous observation that pointed to the presence of underlying chronic inflammatory processes relevant to occupational exposure in the WMWs. 15 Occupational exposure to MSW, therefore, seems to predispose to inflammatory responses reflected not just in local airway injuries8,9,12 but also elicit systemic inflammatory responses as suggested by the present study.
Cellular interaction involving cells of the immune and inflammatory systems plays important role in protection against foreign invaders. 49 WMWs are known to be exposed to large amount of microorganisms, which are abundant in organic matter of solid wastes. 50 Inhalation of these microorganisms may give rise to non-infectious symptoms and diseases either through activation of non-immune defence mechanisms or immune responses. 51 It is also well recognized that antibody formation is an important part in immune response and their levels are related to exposure levels of microorganisms. 52 Although markers of cell-mediated immune response did not change significantly in various categories of WMWs in this study, our results show marked activation of humoral immune response as evident by the significant elevation in IgA and IgG levels when compared with control. IgG and IgA are the major antibodies synthesized during the secondary response. IgA is known to appear selectively in the seromucous secretions, where it defends the exposed external surfaces of the body against the attack by microorganisms. 53 IgG, on the other hand, is the predominant species in non-mucosal tissues, since it diffuses more readily than the other Igs into the extravascular body spaces, where it carries the major burden of neutralizing bacterial toxins and binding to microorganisms to enhance their phagocytosis. We observed during the course of our study that inhalation of bioaerosol was a common occurrence among the WMWs because of their poor use of personal protective equipment. Inhalation of these harmful bioaerosol is capable of eliciting immune response and may explain the increase in IgA and IgG observed in these subjects. The significant elevation of serum IgA (known to positively correlate with seromucous IgA 54 ) across the WMW groups and its increase with increasing job duration may be associated with possible respiratory symptoms and other health outcomes frequently reported in most categories of solid waste workers, and our result seems to support observations from previous studies that have reported higher incidence and greater predisposition to respiratory symptoms and inhalation of biological aerosol as an important pathway of exposure to harmful components of MSW. 8,12,55 While these suggested health outcomes are possibilities, epidemiological studies though scanty have reported association between immune-related respiratory diseases and exposure to contaminants from solid wastes. According to Swan et al. 56 exposure to organic dust or bioaerosol impacts on respiratory health leading to conditions such as allergic rhinitis, asthma, chronic bronchitis and chronic obstructive pulmonary disease amongst others. Similarly, chronic bronchitis and bronchial asthma were among important morbidities detected among street sweepers in a study by Sabde and Zodpey. 57 The health of WMWs from manual sorting facilities studied over a period of 3 years also showed a decrease in lung function and an increase in total IgE indicative of allergic sensitization to atmospheric exposures. 58 Furthermore, symptoms of asthma developed in 33.3% of workers in a Danish sorting plant following occupational exposure. 59 A later study among this same category of workers also revealed that 53.3% became ill within 7 months of commencement of work at the plant and cases of occupational disease were reported in 60% of the waste workers. 60 Compost workers exhibited increased antibody concentrations of relevance to their exposures, providing strong evidence that these workers developed more effective immune systems as a result of their occupational exposures. 61 The fact that serum IgM did not change significantly in the WMWs when compared with controls is expected since IgM only appears early in the response to infection or antigenic stimulation, 53 and this finding is corroborated by the report of Eunha et al. 62 Although the marginal or non-significant increase in IgG in group III (i.e. >4–6 years) when compared with control may be difficult to explain; the place of adaptive responses or changes, however, may come to play in situation of chronic exposure. The decreased GSH and CAT activities in the WMWs that was observed to begin to increase after 0.5–2 years of job duration and with only marginal difference in these parameters between group III (i.e. >4–6 years) WMW group and the control appear to support this. The place of confounding factors may also be important here. However, smoking, alcohol use and age, which are important confounders, 49,63 were comparable. Therefore, the observed relationship between the parameters measured in our study and duration of employment or exposure to waste was not likely to have been distorted or affected by these confounding factors since they did not differ between the WMWs and control subjects.
Furthermore, a link between reactive oxygen species (ROS) generation and Ig production has long been recognized. 64,65 Igs have been reported to be capable of upregulating ROS synthesis in human macrophages. 65 Similarly, chronic inflammation, a prolonged pathological (sometimes silent) condition characterized by mononuclear immune cell infiltration, tissue destruction and fibrosis, usually exerts its cellular side effects mainly through excessive production of free radicals and depletion of antioxidants. 66 Our previous study, which revealed elevated levels of inflammatory and oxidative markers among WMWs, 15 corroborated this observation. In addition to the systemic inflammation, which may be a strong factor in the predisposition to oxidative stress observed in the WMWs, the induction of humoral immune response (which also is recognized to be capable of enhancing ROS synthesis), no doubt, is an important factor for the reduction in antioxidant defence and elevated lipid peroxidation observed in the WMWs in this study. Although it appears that some adaptive changes developed in the WMWs in response to exposure to MSW as also observed in some other studies67,68 when comparing some of the antioxidant/oxidative stress parameters between the various categories of the WMWs, the total antioxidant capacity as measured by the FRAP and extent of lipid peroxidation tend to gradually decrease and increase, respectively, with increasing employment duration. This seems to suggest that continuous (occupational) exposure to MSW may lead to progressive induction of inflammatory and immune responses, which in turn give rise to enhanced production of ROS. This may overwhelm the antioxidant defence mechanisms and attack cellular macromolecules. The usual net result of such free radical attack is a loss of cell integrity, enzyme function and genomic stability. 69,70 This may contribute to the widely reported ill health associated with occupational exposure to solid wastes in several studies.
The human haematopoietic system is generally known to be extremely sensitive to inflammation because of the rapid synthesis and destruction of cells with heavy metabolic demands. The significant decrease in WMWs’ haemoglobin concentration with a corresponding decrease in haematocrit level when compared with the control in this study may be related to the observed elevated levels of inflammatory response in these individuals and supports previous observation that adverse haematological effects of inflammation are mainly the result of its disturbance of the haem biosynthesis pathway. 71 The observed decreases in both haemoglobin and haematocrit levels in the WMWs, however, did not change appreciably with increasing employment duration. Furthermore, the WMWs exhibited significantly elevated total leucocytes, eosinophils and monocytes when compared with the non-WMWs control, and this also increased with their employment or job duration. Neutrophil level, on the other hand, was significantly raised in WMWs of 0.5–2 years job duration, and values decreased as employment duration increases. In contrast to the observed changes in neutrophil levels, the lymphocyte levels of WMWs in 0.5 –2 years employment duration category was comparable with those of the control, and the levels significantly increased with increasing employment duration. Our results revealed an acute reaction phase primarily characterized by neutrophilia, eosinophilia and monocytosis at the early stages of employment or occupational exposure to solid wastes. With increasing employment duration, reactions switch or progress to subchronic/chronic stages with neutrophilia subsiding and reactive lymphocytosis becoming much more pronounced in addition to the already existing eosinophilia and monocytosis.
In spite of the observed biochemical changes described above, BMI, which is the most commonly used indicator to determine general nutritional status and known to positively correlate with certain health and longevity indicators, 72,73 was within the normal range for both WMWs and the non-WMWs control. Similarly, systolic and diastolic blood pressures, which have been demonstrated to increase linearly over a BMI range 74 as well as TC and TG levels were also comparable among all the groups. In addition, BUN and creatinine levels of the various categories of WMWs in this study were still comparable to those of the non-WMWs control in line with our previous report, 15 suggesting normal renal function in these subjects. Again, as pointed out in our previous report, it may be difficult to rule out renal impairment in these individuals since urea and creatinine measurements are usually more sensitive at advanced stages of renal failure. Although most of the parameters for assessing liver function did not change significantly between the various categories of WMWs when compared with the control subjects, the activity of the more specific liver marker, ALT, on the other hand, increased significantly with job duration. With palpable liver reported in a study by Ray et al., 9 though biochemical implications and confirmations of this were not investigated, it is possible that liver impairment could become clinically significant following prolonged job or employment duration. Same may also apply to other parameters observed to be within the normal range for healthy individuals, and this calls for effective surveillance programs and other relevant measures that would ensure the safety of these WMWs, whose roles are of public health importance and contribute immensely to the socioeconomic development of any nation.
It is important to mention that this present study is not without some limitations, and it is hoped that some of these challenges would create perspectives for future research. First, relating duration of exposure of workers to wastes in this study to the length of employment is based on the assumption that workers with similar or same duration of employment have equal exposure both qualitatively and quantitatively and are expected to exhibit same or similar adverse health effects or morbidities. This may not provide the best measure of individual exposure of the WMWs and the quantitative relationship between exposure and morbidity may not be accurately assessed and interpreted. Second, it is also important that the wastes are characterized to identify specific agents in order to facilitate improved knowledge of the chemical and toxicological profile of such compounds and determine their etiological role in the reported morbidities as it is expected that the association between the disease and exposure to the suspected causal agent should be consistent with the known biological activity of the suspected agent. It is hoped that future assessment of health risks associated with occupational exposure to solid wastes would involve a more accurate characterization of individual exposure in addition to evaluation based on the length of employment and also involve multisite studies on larger populations. Experimental models such as laboratory animals might also find relevance in evaluating the consequences of exposure to chemicals from wastes to strengthen any causal relationship observed in human or epidemiological analysis. This is particularly important because of the inherent weakness in health survey based on a self-reporting of symptoms by questionnaire as this method is subject to bias when the purpose of the research is known to the respondents.
Overall, our study provides additional useful information to support the growing body of evidence implicating haematologic alterations, oxidative stress as well as inflammatory and immune-mediated mechanisms in the widely reported adverse health effects associated with occupational exposure to MSWs and that the duration of exposure, as measured by workers’ employment duration, is an important factor in the severity of biochemical changes or alterations seen.
Footnotes
Acknowledgements
The authors gratefully acknowledge Profs EO Ogunyemi and PO Olatunji, Heads of Departments of Chemical Pathology and Haematology of the Olabisi Onabanjo University Teaching Hospital, Sagamu, Ogun State, Nigeria, respectively, for granting permission to use their laboratories. The technical assistance of Mrs Sade Osineye and Mr Stephen Adegbuyi is also gratefully acknowledged.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.