
Abstract
Despite extensive use of organochlorinated pesticides (OCPs) such as dichlorodiphenyltrichloroethane (DDT) in Italy in the 1940s to 1970s, especially for public health control of malaria mosquitoes, information on their exposure levels among the general population is limited. These OCPs can be a source of health risk to human. A total of 137 blood samples were collected from residents of the general population of three Italian towns, Novafeltria, Pavia and Milan, to determine the levels of eight OCPs in blood serum. The concentrations of beta-hexachlorocyclohexane, hexachlorobenzene (HCB), 1,1-dichloro-2-(o-chlorophenyl)-2-(p-chlorophenyl)ethylene, 1,1-dichloro-2,2-bis(p-chlorophenyl)-ethylene (p,p'-DDE), 1,1-dichloro-2-(o-chlorophenyl)-2-(p-chlorophenyl)ethane, 1,1-dichloro-2,2-bis (4-chlorophenyl)ethane, 1,1,1-trichloro-2-(o-chlorophenyl)-2-(p-chlorophenyl)-ethane and 1,1,1-trichloro-2,2-bis(p-chlorophenyl) ethane were measured by gas chromatography–mass spectrometry. Variations in serum concentrations of OCPs with respect to place of residence, gender, age and body mass index (BMI) were evaluated by non-parametric tests. p,p'-DDE and HCB were the most abundant and major contributors of total OCP concentration. Their levels differed significantly between the three towns with a trend Milan > Novafeltria > Pavia ( p < 0.0001). Females had significantly higher concentrations of HCB and p,p'-DDE than males in the overall population sample. HCB concentrations were significantly higher in females than in males of Milan (p = 0.029). We observed positive correlations of p,p'-DDE and HCB with age in Novafeltria subjects (r = 0.468, p = 0.004). Total OCP concentrations differed significantly across BMI categories (p = 0.018) in overall population. We have demonstrated a clear pattern of the main OCPs in a fairly large population. Generally, our study provides information on OCPs exposure among the Italian general population and provides indications for further investigations.
Introduction
Organochlorinated pesticides (OCPs) are a structurally heterogeneous class of chlorinated organic compounds (OCs), which contain several chlorine atoms per molecule. Among OCPs of prominent concern are dichlorodiphenyltrichloroethane (DDT) and its metabolites, chlordane, hexachlorobenzene (HCB) and hexachlorocyclohexane (HCH) isomers. They were used since the mid-1940s as insecticides in agriculture and in public health for the control of parasite-borne diseases. Ecological and human health concern led to intensive campaign against their use, leading to a gradual ban or restriction of their production and use in most countries starting in the early 1970s and finally ending with the Stockholm Protocol in 2001. 1 –3 Some compounds such as DDT and lindane are still effectively used in tropical countries, to control malaria vectors through the practice of ‘indoor residual spraying’ 4 and for treatment of lice and scabies, 5 respectively.
Their high content of chlorine in a mostly rigid carbon atom scaffold makes the molecules highly soluble in the lipid compartment of living organisms and poorly degradable in the environment by physical, chemical and biological processes. 3 The consequence of both properties, together with widespread and high-intensity use as pesticides for at least 30 years, led to exposure to these chemicals of virtually every person and living organism on earth at different magnitudes. 3,6 Due to their long environmental and biological half-lives, most banned OCPs are still present at trace levels in several foods and thus represent a source of exposure for the general population in all the corners of the world, with significant geographically based differences. 7 –10 Main sources of exposure are some sea foods, milk and dairy products, meat and poultry, fats and oils.
The insecticide DDT is produced as a technical mixture of three isomeric forms, the most prevalent form being the para,para (p, p′) isomer; ortho,ortho (o,o′)- and ortho,para (o,p′) isomers being present in minor and variable amounts. Its main by- and bio-transformation products are dichlorodiphenyldichloroethylene (DDE) and dichlorodiphenyldichloroethane (DDD).
Photochemical chlorination of benzene affords complex and variable mixtures of HCH products, of which the gamma (γ) isomer, also known as lindane, is still used as an insecticide in agriculture and in the treatment of scabies, body lice and head lice in humans. Compared to other isomers, beta (β)-HCH shows a higher bioaccumulation, with a half-life in human body of about 7.2 years 11 and a mean bioaccumulation factor of 5274. 12
HCB was widely used as a fungicide. Its environmental half-life in soil and in air is of approximately 3–6 years and 0.63–6.28 years, respectively. 13 In human, the half-life of HCB is thought to be extremely long in the range of 6 years. 14
These OCPs can constitute a source of health risk. 7,8,15 –17 In experimental models, DDT isomers are capable of inducing alterations in reproduction and development due to their hormone-altering actions. 1,1,1-Trichloro-2-(o-chlorophenyl)-2-(p chlorophenyl)-ethane (o,p′-DDT) has the strongest estrogen-like properties, and 1,1-dichloro-2,2-bis(p-chlorophenyl)-ethylene (p, p′-DDE) has anti-androgenic properties. 1,1-Dichloro-2-(o-chlorophenyl)-2-(p-chlorophenyl)ethane (o,p′-DDD; mitotane) is used as an anticancer drug for adrenocortical carcinoma due to its hormone disrupting properties. All HCH isomers can affect liver and kidney. 15 In humans, the most sensitive target organs that HCB affects are the liver, the ovary and the central nervous system. 13
The International Agency for Research on Cancer has classified DDT, all HCH isomers and HCB as ‘possibly carcinogenic to humans’ (group 2B). 18,19 Apart from cancer risk, or possibly as one causal mechanism of OCP-triggered cancer, the endocrine disruption activity of these substances deserves attention. In particular, DDT isomers are capable of inducing alterations in human reproduction and development due to their hormone-altering actions. For instance, o,p′-DDT isomer has the strongest estrogen-like properties, 20 whereas p, p′-DDE has anti-androgenic properties, which has been shown to alter the development of reproductive organs when administered perinatally to rats. 21
Ubiquitous presence of DDT in human tissues has been demonstrated in hundreds of studies, most of which are collected and reviewed in monographs by United Nations agencies. 18,20 The human specimens most commonly used for OCPs measurement are blood (serum) but also visceral and female breast adipose tissue from autopsies and from living subjects.
Among European countries, Italy used DDT extensively since 1945 upto the 1970s for controlling flies and mosquitoes (particularly malaria vectors). This led to the improvement in health conditions especially in the Po river delta, in central-southern coastal and in insular Italy. Exposure measurement aimed at health risk assessment of these pollutants in the general population is still a matter of public health concern. Despite long-time use, measurements are mainly targeted at environmental contamination and only limited information is available on actual human burden of these pollutants in the country. Between 1972 and 2011, about 16 international published articles reported OCPs concentration in the Italian population, 22 –37 and lack of detailed exposure data hinders adequate human risk assessment. 36
This project is aimed at improving existing knowledge on exposure of the Italian general population to concerning persistent organic pollutants (POPs), such as OCPs and other pollutants. This article reports on our study on OCPs, while another report deals those on polychlorinated biphenyls.
Materials and methods
Our research group collected, in the frame of routine health checks of the general population, serum samples and selected information from a total number of 137 subjects not exposed to POPs from identified sources. Among them, 36 live in Novafeltria (a 7000-inhabitant small town in Central Italy), 59 live in Pavia (a 70,000-inhabitant small old city in Northern Italy) and 42 live in Milan (the 1,300,000-inhabitant largest city in Northern Italy and the second-largest in Italy).
Recruited subjects signed consent forms to participate in the project and supplied information on age and gender, height and weight, lifestyle (usual diet, cigarette smoking, alcohol consumption and physical exercises), some details on occupation, drinking water sources and use of medications, which were collected during interview using data collection forms.
Blood sample collection
A 10 ml venous blood sample was obtained from each subject from the antecubital vein and collected in silicone-coated Vacutainer® (Becton & Dickinson, Franklin Lakes, NJ, USA) without anticoagulants. Serum was separated within 24 h after collection, kept at 4°C until shipment and frozen at −20°C upon receipt at the laboratory until analysis.
Determination of serum concentrations of triglycerides and total cholesterol
Serum concentrations of triglycerides and total cholesterol were measured by standard clinical chemistry at Fondazione Salvatore Maugeri in Pavia. These parameters were used to define total lipid concentrations using the equation reported in Philip et al.
38
(equation (1)).

where total lipid is expressed in grams per litre (g/L); total cholesterol is expressed in g/L [(normal range: 120–220 milligrams (mg)/100 millilitre (mL)]; triglycerides are expressed in g/L (normal range: 40–170 mg/100 mL).
Gas chromatography–mass spectrometry measurement of OCPs from blood serum
The analytical technique for the determination of these compounds is described by Turci et al. 25 In brief, an ethyl ether–hexane extract of organic-soluble compound of blood serum was purified by solid-phase extraction on a polychlorinated biphenyl (PCB)-specific sorbent and the analytes were measured by gas chromatography–mass spectrometry. Minimum detectable levels of the eight analytes, expressed as Limit of Detection (LoD), were in the range of 0.05–0.50 nanograms per millilitre (ng/mL).
The following eight targeted OCPs were selected based on their presence in the environment and potential toxicity: β-HCH; HCB; 1,1-dichloro-2-(o-chlorophenyl)-2-(p-chlorophenyl)ethylene (o, p′-DDE); p, p′-DDE; o, p′-DDD; 1,1-dichloro-2,2-bis (4-chlorophenyl)ethane (p, p′-DDD); o, p′-DDT and 1,1,1-trichloro-2,2-bis(p-chlorophenyl) ethane (p, p′-DDT).
The individual OCP concentrations were adjusted for total lipid to give better estimate of the body burden. 39 Adjustment was computed by dividing the crude serum OCP concentration (ng/mL) by total lipid concentration in serum (g/L) to yield OCP concentration in nanograms per gram of serum lipids, which was finally converted to picomoles per gram serum lipid (pmol/g serum lipid). 40 The same conversion was applied to the results published in the scientific literature, which were used as reference in the interpretation of our own measurements. When results in the literature were expressed without lipid adjustment and no blood lipid levels were reported, an adjustment was nevertheless performed by taking the lower and upper levels of normal concentrations of cholesterol and triglycerides in equation (1).
Statistical analysis
The data were analyzed using the Statistical Package for Social Sciences (SPSS) software version 17.0 (SPSS Inc., Chicago, Illinois, USA) and custom Microsoft Excel© 2003 spreadsheets. A bar chart was used to present prevalence of each OCP in the study population subgroups (Supplementary Figure S1).
All statistical analyses were performed at serum lipid-adjusted concentrations and were restricted to β-HCH, HCB, p, p′-DDE, p, p′-DDD, o,p′-DDD and o,p′-DDT, which were detected in more than 50% of the population sample. For those samples with values below LoD, a value of one half the LoD was assigned and calculation of the medians included these values.
Statistical analyses were conducted to assess inter-individual variability in OCP levels and to highlight differences with respect to sex, age, body mass index (BMI) and residence. The dependent variable in this study is serum lipid-adjusted OCP concentrations under investigation. The OCP concentrations were summarized for the overall population of three sites and for the individual sites and separately for males and females using medians, minimum and maximum values. Shapiro–Wilks’ test was used to check the distribution of OCPs. Since distribution of OCP levels among the subjects was non-symmetrical, all statistical tests were performed by non-parametric tests, and medians were used as a measure of central tendency. The Kruskal–Wallis (KW) test was used to test the difference in concentration of individual OCPs between the samples from Novafeltria, Pavia and Milan. The Mann–Whitney U test assessed the difference in total DDT concentrations between the gender groups. All statistical tests were considered significant at the 0.05 level (two tailed).
Results
The main characteristics of the individual subjects and the analytical results obtained for each of them are collected and are available as supplementary data.
Study population
The main characteristics of the study subjects are indicated in Table 1. Our study population composed of 65 (47%) females and 71 (52%) males. The distribution of gender in Pavia and Milan was skewed with female and male subjects underrepresented, respectively. The mean body weight of the study subjects was 69.85 kg and mean BMI was 24.01 kg/m2, which are consistent with the reported mean weight and mean BMI of a representative general Italian adult population of 18 years old or above (69.4 kg and 24.5 kg/m2, respectively). 41 On average, our study population had individuals who were in the normal or healthy range in terms of BMI classification.
Main characteristics of population study expressed as valid percentages (and absolute number) for gender and medians (minima and maxima) for age, body weight and body mass index.

BMI: body mass index.
Serum concentrations of OCPs and of their metabolites
A summary of the levels of individual OCPs in the subjects classified by residence and gender is reported in Table 2. To understand the complex pattern of OCPs, the targeted analytes were shrunk to chemically and metabolically analogous groups, by summing together the DDT-like compounds (DDT, DDE and DDD) with p,p′- and o,p′-chlorine substitution (p,p′-DDX and o,p′-DDX, respectively). Thus p,p'-DDX was computed as the sum of p,p'-DDE and p,p'-DDD whereas o,p'-DDX as the sum of o,p'-DDD and o,p'-DDT. Total OCP was computed as the sum of levels of all OCPs analyzed from an individual subject, whereas total DDT included the summation of DDT-related compounds (all isomers of DDT + DDE + DDD). This data reduction approach leads to six OCP groups (Table 3).
Median, minimum, maximum and significant values of OCPs (in picomoles per gram serum lipid) between female and male subjects from three Italian population subgroups.a

Min.: minimum; med.: medium; max.: maximum; OCPs: organochlorinated pesticides; p,p'-DDE: 1,1-dichloro-2,2-bis(p-chlorophenyl)-ethylene; HCB: hexachlorobenzene; β-HCH: beta-hexachlorocyclohexane; DDT: dichlorodiphenyltrichloroethane; p,p'-DDD: 1,1-dichloro-2,2-bis (4-chlorophenyl)ethane; o,p'-DDT: 1,1,1-trichloro-2-(o-chlorophenyl)-2-(p chlorophenyl)-ethane; o,p'-DDD: 1,1-dichloro-2-(o-chlorophenyl)-2-(p-chlorophenyl)ethane.
a Significant difference in distribution of HCB was observed between males and females in only Milan (p = 0.029, females > males). In Novafeltria and Pavia, there was no evidence of significant difference in distribution of all analyzed OCPs between males and females.
Main results of the measurement of OCPs in the examined subjects (in pmol/g serum lipids).a

Min.: minimum; med.: medium; max.: maximum; OCPs: organochlorinated pesticides; p,p'-DDE: 1,1-dichloro-2,2-bis(p-chlorophenyl)-ethylene; HCB: hexachlorobenzene; β-HCH: beta-hexachlorocyclohexane; DDT: dichlorodiphenyltrichloroethane; ∑p,p'-DDX: (p,p'-DDE + p,p'-DDD); ∑o,p'-DDX: (o,p'-DDD + o,p'-DDT); ∑DDT: (∑p,p'-DDX + ∑o,p'-DDX); ∑OCP: (β-HCH + HCB + ∑DDT).
a One subject from Milan was excluded from the analysis due to the lack of most data.
The most persistent isomer of HCH (β-HCH) was detected in 74 samples (54%), with a median concentration of 123 pmol/g lipid (28–1023 pmol/g lipid). HCB and p,p′-DDE were the most frequently detected OCPs in the overall study population (99 and 97%, respectively), with median concentrations of 154 and 395 pmol/g lipid, respectively. p, p′-DDT and o,p′-DDE were the least detected and thus they were excluded from the analysis. The median levels of total OCP, total DDT, total p, p′-DDX and o,p′-DDX were 1756, 1229, 514 and 173 pmol/g lipid, respectively, in the overall sample population (Supplementary Table S2).
Distribution of OCPs by places of residence
Novafeltria
The median total OCP and total DDT in Novafeltria (36 subjects) were 1375 and 1055 pmol/g lipid, respectively. HCB with a median concentration of 209 pmol/g lipid was found in all analyzed samples, while β-HCH was detected in only 11% of the samples. The main metabolite of DDT (p, p′-DDE) was the most abundant OCP in Novafeltria detected in 35 samples (median: 428 pmol/g lipid). o,p′-DDT and o,p′-DDD were detected in 28 samples equivalent to 34% of 82 analyzed samples and 37% of 75 analyzed samples, respectively. p, p′-DDD was detected in 29 samples, accounting for 29% of the analyzed samples (n = 84) in the overall sample population.
Pavia
The median total OCP and total DDT in Pavia (59 subjects) were 1285 and 767 pmol/g lipid, respectively. HCB and β-HCH were detected in all 59 samples with median concentrations of 100 and 323 pmol/g lipid, respectively. This account for 44% (n = 135) and 80% (n = 74) of the overall samples with detectable levels of HCB and β-HCH, respectively. p, p′-DDE was detected in 58, accounting for 44% of subjects with detectable levels in the overall population (n = 133, median: 163 pmol/g lipid). o,p′-DDT, o,p′-DDD, p, p′-DDD and o,p′-DDE were detected in 62% (51/82), 63% (47/75), 55% (46/84) and 27% (3/11) of the samples with detectable levels of these OCPs, respectively.
Milan
The median total OCP and total DDT of 41 subjects (98%) in Milan were 5286 and 4651 pmol/g lipid, respectively. β-HCH, o,p′-DDE and o,p′-DDD were under detection limit in all samples, whereas p, p′-DDT was detected in only one sample with a concentration of 395 pmol/g lipid. As in other sites, HCB and p,p′-DDE were the most frequently detected among the 40 samples accounting for 30% of the samples analyzed in the overall population sample (n = 135, n = 133). o,p′-DDT, p,p′-DDD and p,p′-DDT were the least prevalent in this population subgroup.
Comparison among places of residence
A trend of the median level of total OCP, total DDT, p, p′-DDE and HCB was observed among the residents in the investigated sites (Figure 1). Pavia showed the lowest median level for these OCPs, while Milan the highest level. These levels were significantly different across these sites (Milan > Novafeltria > Pavia, p < 0.0001). The highest median levels of total o,p′-DDX, β-HCH, o,p′-DDD, p,p′-DDD and o,p′-DDT were observed in Pavia and the lowest in Milan. The distribution of these OCPs differed significantly across the sites (Pavia > Novafeltria > Milan, p
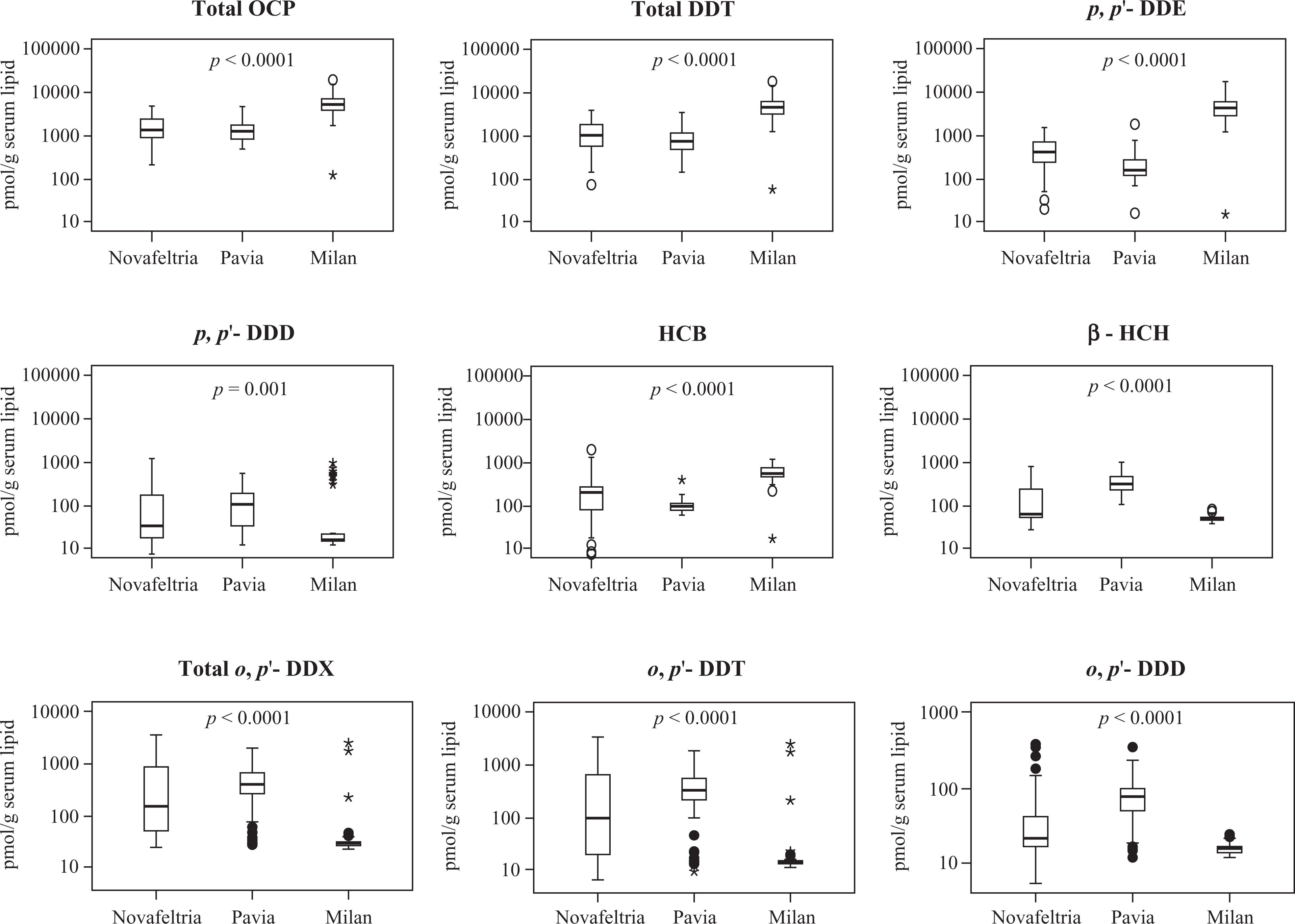
Distribution of OCPs concentration expressed in picomoles per gram serum lipid (logarithmic scale) among the study population stratified by geographical locations. Displayed results are for total OCPs, total DDTs and some individual OCPs with significantly different distribution across the investigated study sites. O indicates mild outliers and * indicates extreme outliers. OCPs: organochlorinated pesticides; DDT: dichlorodiphenyltrichloroethane.
Distribution of OCPs by gender
In the overall sample, females had significantly higher median total OCP than males (3050 and 1489 pmol/g lipids, respectively; p < 0.0001). Similar observation was seen for total DDT (medians: 2417 and 995 pmol/g lipid for females and males, respectively; p = 0.001).
The fungicide HCB was detected in 64 female samples (99%), while p,p′-DDE in 62 samples (95%) with median levels of 482 and 789 pmol/g lipid, respectively. These OCPs were detected in all 71 male subjects with median levels of 107 and 268 pmol/g lipids, respectively. The level of HCB and p,p′-DDE differed significantly between females and males (p < 0.0001). Out of 65 female samples analyzed, p,p′-DDD was detected in 40 samples (62%), o,p′-DDD and o,p′-DDT were detected in 31 samples (48%). o,p-DDE and p,p′-DDT were the least abundant among female subjects. Gender distributions of total OCP, total DDT, p, p′-DDE, p, p′-DDD, HCB and β-HCH are illustrated in Figure 2.
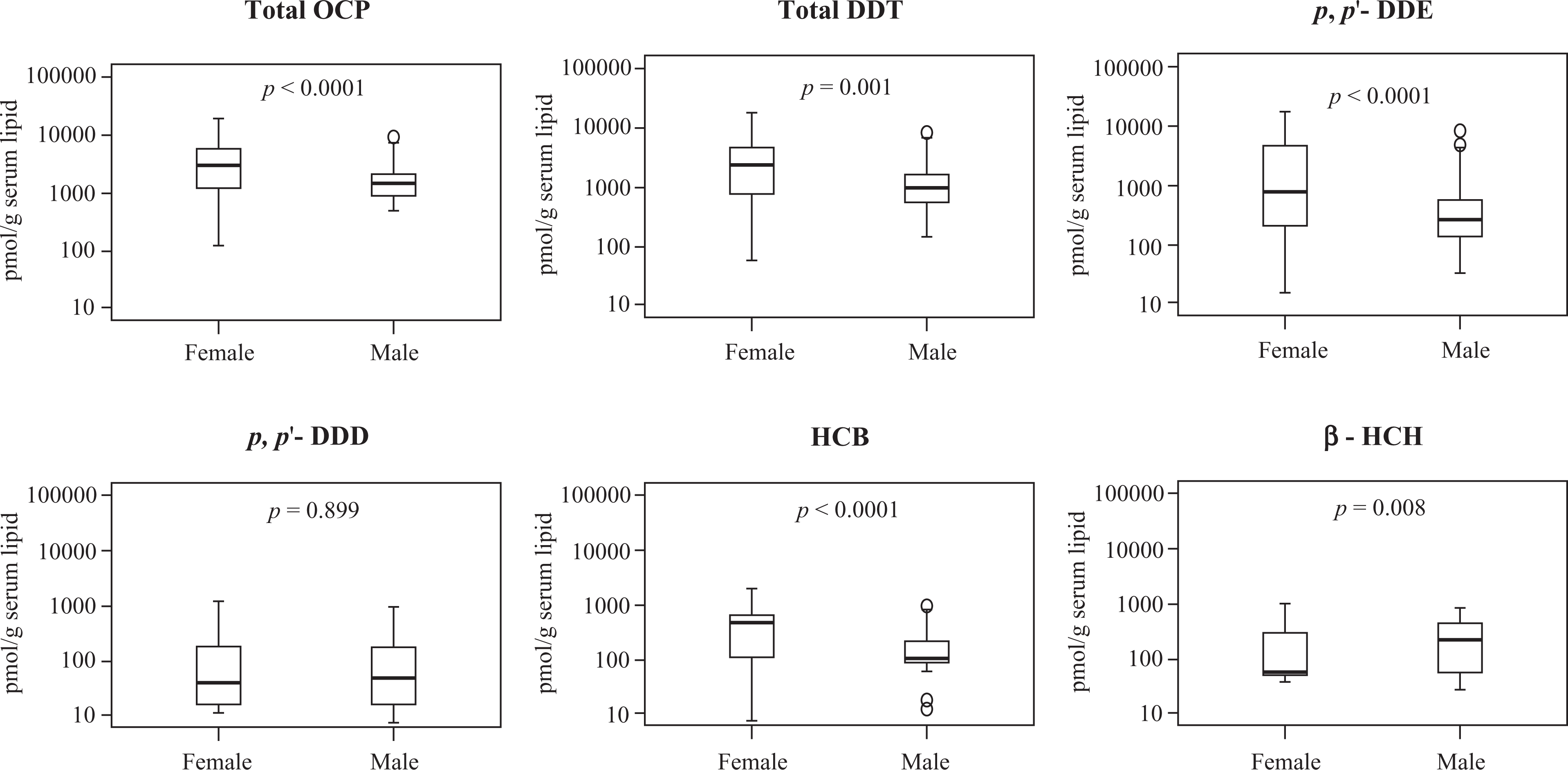
Distribution of OCPs concentration expressed in picomoles per gram serum lipid (logarithmic scale) among the study population stratified by gender. Displayed results are for total OCP, total DDT, p,p'-DDE, HCB and β-HCH with significantly different concentrations between males and females (except p,p'-DDD). OCPs: organochlorinated pesticides; DDT: dichlorodiphenyltrichloroethane; p,p'-DDE: 1,1-dichloro-2,2-bis(p-chlorophenyl)-ethylene; HCB: hexachlorobenzene; β-HCH: beta-hexachlorocyclohexane.
Based on individual study site, β-HCH was detected in 15 subjects of Novafeltria, eight of them were females (53%) with a median concentration of 65 pmol/g lipid. HCB was detected in all 17 women (median: 220 pmol/g lipid), whereas p,p′-DDE, p,p′-DDD and o,p′-DDT were found in 16, 14 and 13 subjects, respectively, with median concentrations of 538, 49 and 78 21 pmol/g lipid, respectively.
Among male subjects of Novafeltria, seven subjects (47%) had detectable β-HCH with a median of 59 pmol/g lipid. HCB and p,p′-DDE found in all 19 subjects with a median concentration of 189 and 339 pmol/g lipid, respectively. p,p′-DDD, o,p′-DDT and o,p′-DDD were detected in 15 subjects with median concentration of 31, 118 and 21 pmol/g lipid, respectively. There was no evidence of significant difference in the levels of all analyzed OCPs between males and females (Table 2).
In Pavia, β-HCH and HCB were detected in all 17 females (29%) with median concentrations of 327 and 86 pmol/g lipid, respectively. p,p′-DDE and p,p′-DDD were each detected in 16 subjects with median concentrations of 143 and 116 pmol/g lipid, respectively. o,p′-DDD and o,p′-DDT were detected in 14 and 15 subjects, respectively, with median concentrations of 81 and 330 pmol/g lipid. In males group, β-HCH, HCB and p,p′-DDE were detected in all 42 subjects. The median concentrations of these OCPs were 303, 100 and 173 pmol/g lipid, respectively. p,p′-DDD, o,p′-DDT and o,p′-DDD were detected in 30 (66%), 37 (73%) and 32 (68%) subjects, respectively, with median concentrations of 86, 337 and 72 pmol/g lipid. As for Novafeltria, no evidence to account for the significant difference between males and females for all analyzed OCPs (Table 2).
In Milan, HCB and p,p′-DDE were detected in 40 subjects, of them 10 were male subjects (25%). Their median concentrations were 472 and 3397 pmol/g lipid, respectively. o,p′-DDT (median 14 pmol/g lipid) and p,p′-DDD (median 16 pmol/g lipid) were each detected in only two samples. Among female subjects of Milan, HCB and p,p′-DDE had median concentrations of 627 and 5363 pmol/g lipid, respectively. Contrary to Novafeltria and Pavia, significant difference in the distribution of HCB was observed between males and females from Milan (p = 0.029), females having higher median level than males (Table 2).
Distribution of OCPs by subjects’ age
To evaluate the effect of age, subjects’ age was categorized into four 15-year groups (10–25, 26–40, 41–55 and 56–70) and compared the total content and the distribution of the analyzed OCPs across them for the overall population and for the individual sites. No subject was younger than 19 years, while the majority of subjects were between 26–40 and 41–55 years (approximately 41 and 34%, respectively) and 14 were of 56–70 years. Compared with other sites Milan had younger subjects (Table 4).
Absolute frequency of study subjects in each age category for the pooled population sample and individual population subgroups.

DDT: dichlorodiphenyltrichloroethane.
The median concentrations of total OCPs in the overall population sample were found to be 3060, 1678, 1536 and 1636 pmol/g lipid across these age groups, respectively. In Novafeltria, the distribution of total OCPs (p = 0.015) and total DDT (p = 0.039) differed significantly across these age groups. However, the significance value for total p,p′-DDX was within the significance limit level (p = 0.051). The median concentrations along the respective age groups were 539, 1112, 1618 and 1782 pmol/g lipid (for total OCPs); 251, 375, 706 and 1091 pmol/g (for total p, p′-DDX) and 331, 781, 1458 and 1444 pmol/g lipid (for total DDT). The distribution of these OCP groups monotonically increased with subject age (r 2 = 0.181, p = 0.01; r 2 = 0.138, p = 0.026 and r 2 = 0.156, p = 0.017 for total OCP, total p, p′-DDX and total DDT, respectively). In Milan, distribution of these OCP groups was not statistically significantly different across the age groups although their median levels increase consistently across these age groups (5115, 5337, 5494 and 19,363 pmol/g lipid for total OCP; 4428, 4693, 4999 and 18,103 pmol/g lipid for total DDT; 4297, 4512, 4973 and 18,077 pmol/g lipid for total p,p′-DDX).
As for individual analytes, the concentration of only β-HCH presented a statistically significant increasing trend across these age groups for only Pavia population subgroup ( p = 0.027). The median concentrations of this compound for the four age groups 10–25, 26–40, 41–55 and 56–70 were 305, 401, 249 and 467 pmol/g lipid, respectively. However, correlation analysis did not reveal any significant correlation with age (r = 0.021, p = 0.874). There is no evidence for significant difference in distribution for other detected OCPs across these age groups, as illustrated in Supplementary Figure S2.
Distribution of OCPs by BMI
The minimum and maximum BMI in our study population were 17.58 and 38.53 kg/m2, respectively. Four main BMI categories and a total of 11 sub-classes as per international classification 42 reflect the status of the body fat in population studies, ranging from those underweight (BMI < 18.50 kg/m2) to those severely obese (BMI ≥ 40 kg/m2). Based on this classification our study group had four (3%) underweight individuals, 89 (65%) normal and 43 (32%) overweight (Supplementary Table S4). None of the subjects fell into the severely underweight or severely obese.
Supplementary Figure S3 illustrates the distribution of these OCPs across the main BMI categories. Statistical test was performed to assess the influence of BMI on individual OCP level and total OCP levels in both entire data set and individual population subgroups. Considering the entire data set, significant difference was observed in the distribution of total OCP and total DDT across the four categories namely <18.50, 18.50–22.99, 23.00–24.99 and ≥25.00 kg/m2 (p = 0.018 and 0.023, respectively). The median levels of total OCP in these categories were 1097, 3050, 1359, 1855 pmol/g lipid (for total OCP) and 696, 2497, 963 and 1307 pmol/g lipid (for total DDT). However, when analyses were restricted to individual sites, the significance value of p,p′-DDE fell exactly on the limit of significance level ( p = 0.050) for the Pavia group. Otherwise, there was no evidence of significant difference in distribution of all other individual OCPs and total OCP across the BMI categories in all investigated population subgroups.
Discussion
Exposure to ubiquitous pollutants of high concern such as OCPs (mainly DDT) and chlorinated biphenyls was measured in the Italian general population starting in the early 1960s and more than 50 articles have reported concentrations in biological compartments such as blood serum, adipose tissue and human breast milk. In this article, we address only OCPs, whilst PCBs that were measured in a similar but not coincident cohort are reported and discussed in a separate article (Mrema et al., submitted to This Journal, 2012).
The population recruited in our study has, on the overall, a fair gender distribution with reference to that of the general Italian population derived from census. 42 This is the case for the Novafeltria cohort, while those for Pavia and Milan are grossly skewed, with more males in Pavia and more females in Milan. The age distribution of our population does not match that of the Italian population, 41 since it lacks the extremes of age (<19 and >75 years), mainly due to the difficulty of accessing the younger and to ethical considerations on blood withdrawal in the very elderly. The age ranges were 22–59, 20–70 and 19–69 years for Novafeltria, Pavia and Milan subjects, respectively. Significant difference in age distribution was observed between these sites (KW test, p < 0.0001) with the highest median age (44.5 years) in Novafeltria population (Table 1). The lack of representativeness of our study sample to the general population of Italy, mainly for age and gender structure, was unavoidable due to constraints in the experimental approach (collection of blood samples over time, during routine health surveys of the enrolled subjects). For the same reasons, we could not collect parity and lactation history data of women. This could better be used to explain and understand the difference in OCPs distribution among the gender group since breastfeeding is known to be a major pathway of excretion and transmission of mothers’ body burden of OCs to their newborns. 43
Although persistent OCPs such as DDT were banned in Italy since 1978, to date detectable levels are still found in the Italian general population as evident in this study. We have demonstrated a clear pattern of the level of total OCP, total DDTs, p,p′-DDE and HCB among the healthy residents in the three investigated locations of Italy. These levels were significantly different across these sites (Milan > Novafeltria > Pavia, p < 0.0001) with Milan having the highest median level.
To frame our results within the general picture, a summary of the levels of OCPs measured in various Italian regions between 1972 and 2011 is shown in Table 5. Data on the body burden of OCPs are not abundant and studies are very heterogeneous in sample size and in the number of target analytes. Limited sample sizes of individual studies and limited collection of data on exposure determinants hamper extrapolation of exposure estimation to the general population for health promotion purposes. The original studies also report OCP concentrations using different units. To allow comparison of the levels of exposure with those of our study, we converted the results of some literature studies (Table 5) to pmol/g lipid as described in the Methodology section. 40
Concentration of OCPs (in picomoles per gram serum lipid) in blood serum and in other body compartments of Italians living in various regions (1972–2011).

OCPs: organochlorinated pesticides; o,p'-DDE: 1,1-dichloro-2-(o-chlorophenyl)-2-(p-chlorophenyl)ethylene p,p'-DDE: 1,1-dichloro-2,2-bis(p-chlorophenyl)-ethylene; HCB: hexachlorobenzene; β-HCH: beta-hexachlorocyclohexane; DDT: dichlorodiphenyltrichloroethane; p,p'-DDD: 1,1-dichloro-2,2-bis (4-chlorophenyl)ethane; p,p'-DDT: 1,1,1-trichloro-2,2-bis(p-chlorophenyl) ethane; o,p'-DDT: 1,1,1-trichloro-2-(o-chlorophenyl)-2-(p chlorophenyl)-ethane; o,p'-DDD: 1,1-dichloro-2-(o-chlorophenyl)-2-(p-chlorophenyl)ethane.
a Median.
b Geometric mean.
c Maximum level.
d Range.
e Individual measurement of the pooled sample.
f Mean.
g Concentrations are multiplied by 106.
h Concentrations are multiplied by 105.
i Concentrations are multiplied by 104.
In their study targeted at assessing the levels of several organochlorines in human breast milk collected in 2000–2001 from lactating mothers in Italy, Weiss et al. found high concentration of DDE (approximately 27 ng/g fresh weight) from Milan samples. 44 The authors hypothesized that the measured level may be due to the content of OCPs in food imported from countries where DDT is still used.
As for specific sources of exposure to OCPs, a significant association between plasma levels of DDT, DDE and PCBs and fish consumption was demonstrated in the Swedish population. 45,46 Also in Italy, intensive harvesting of Manila Clam and fishing in the polluted Venice lagoon caused an increase in the concentration of POPs in mother milk and blood serum of Venetians. 47 However, some studies failed to establish the evidence on the relationship between some POPs levels and consumption of particular type of foods. 28
In our cohort, the KW test revealed a significant difference in distribution of β-HCH with places of residence (p < 0.0001). Ingelido et al. 23 demonstrated similar trend in β-HCH serum concentration distributions among investigated subjects from northern, central and southern Italy (p = 0.03). However, the median level observed in our study (122.5 pmol/g lipid) is higher than that reported in their study (61.89 pmol/g lipid), but lower than that reported in Schiavone et al.’s study (250 pmol/g lipid). 33
HCB and p,p′-DDE are known to have long half-lives in human. 48,49 This guarantees their high prevalence (>90%) observed in our study population. The overall level of HCB observed in Milan population (median = 578, mean = 634 pmol/g lipid) is similar to that found in adipose tissue (mean 534 pmol/g serum lipid) reported elsewhere. 33 The observed level of p,p′-DDE in our study is 177 ng/g lipid (geometric mean; data not shown), much lower than that in the Spanish study (geometric mean 822 ng/g lipid). 50
Variations by gender in concentrations of some OCPs were observed in our subjects. When the three sites were considered together females had significantly higher levels of p,p′-DDE than males (p < 0.0001). This difference can be due to inter-gender physiological differences. In consistent with previous studies, 50 –53 we also observed higher HCB concentrations in women than in men. In addition to intergender physiological differences, our observation could also be related to differences in metabolism. It has been found that metabolism of HCB is higher in men than in women. 54 As p,p′-DDE and HCB were the major contributors of total OCPs, we also observed significant higher level of total OCPs in females than in male subjects. Contrary to our study, previous studies reported lower level of p,p′-DDE in women than in men, 50 –52,55 –57 which can be explained as the consequence of lactation and menstruation, 58,59 the major routes of OCs excretion in females.
In our population, serum p, p′-DDT was detected in 11 and 14% of female and male subjects, respectively. The maximum concentration of 207 ng/g lipid (data not shown) was found, a level which is comparable to 257 ng/g lipids reported in the study of Jakszyn et al. 50 but almost double of that measured in Sweden (124 ng/g lipid). 60,61 In the latter study, p, p′-DDT was highly prevalent in about 80% of females and 90% of males.
The distribution of β-HCH between females and males was statistically significantly different (Mann–Whitney U test, p = 0.008), males with higher median level than females (229 and 59 pmol/g lipids, respectively). While other studies observed the opposite trend for this OC, 55,52 Ingelido et al. failed to show the evidence for the significant differences in the distribution of β-HCH between genders (Mann–Whitney U test, p = 0.81). 23 This was also the case for our study when the analyses were restricted to the places of residence and gender.
The differences in exposure between genders could not be accounted for as we did not have factors associated with our subjects that could provide better explanation. However, this variation is not anticipated in people of the general population. 51
Age is one of the personal characteristics that plays a role in differentiating the levels of OCPs, since it defines the time frame of accumulation of biologically persistent chemicals. Usually, it is expected that accumulation of these contaminants increases with age of the subjects. In this study, total OCP and total DDT presented a significant increasing median concentration across the age groups in Novafeltria population. This behaviour was also evident in distribution of total p,p′-DDX (Novafeltria) and β-HCH (Pavia) except that the median concentration of age 41–55 years was a little higher than that of age group 56–70 years for total DDX, while for β-HCH the median concentration of age group 41–55 years was slightly lower than that of 10–25 years. However, significant and positive correlations with age were found for total OCP, total DDT, total p,p′-DDX, p,p′-DDE and HCB (r = 0.479, p = 0.003; r = 0.446, p = 0.006; r = 0.454, p = 0.005; r = 0.468, p = 0.004 and r = 0.468, p = 0.004, respectively) in only Novafeltria group. Generally, the oldest part of the population was characterised by the highest median concentrations.
The increasing trend of median concentrations along the age groups was demonstrated by Ingelido et al., where 11, 18 and 39 ng/g lipid of β-HCH were found in subjects in the age ranges 20–35, 36–50 and 51–65 years, respectively. 23 This behaviour was also observed in Porta et al.’s study, where higher median concentrations of p,p′-DDE and HCB were found among the older subjects who were between 60 and 74 years of age when compared with the younger ones of age between 18 and 29 years. 52 Bates et al. also demonstrated increasing mean concentrations of dieldrin and p,p′-DDE along the age groups (15–24, 25–34, 35–49, 50–64 and 65+ years). 62
BMI is a relative measurement of the amount of body fat in different subjects much used in population studies. OCPs preferentially accumulate in body fat and thus a larger body burden is expected in subjects with higher BMI compared with those with lower BMI (Supplementary Table S4). We observed that in overall sample, subjects with progressively higher BMI had higher levels of total OCP (p =0.018) and total DDT (p = 0.023). There was no significant positive correlation between most OCPs and BMI with exception of HCB in Novafeltria (r = 0.435, p = 0.008) and Pavia (r = 0.268, p = 0.040). Sala et al. and Medehouenou et al. showed the increase in the levels of HCB, β-HCH and p,p′-DDE with BMI. 53,63
General comparison of our results with other studies conducted outside Italy showed lower median level of p, p′-DDE (125.42 ng/g lipid) than those reported in some Westernized Asian countries such as Japan and Korea (221 and 224 ng/g lipid, respectively), 55,64 in other European countries such as Romania and Sweden (1975 and 497 ng/g lipid, respectively), 51,65 in New Zealand (919 ng/g lipid) 57 and in the USA (204 ng/g lipid). 66 However, this level is slightly higher than 100 ng/g lipid reported in the United Kingdom. 67 β-HCH had a median concentration of 35.68 ng/g lipid, which was higher than those reported in some studies 62,67 but lower than in other studies. 51,55,64,65 HCB had a median of 43.84 ng/g lipid, which is higher than those reported in these studies 51,55,64,66,67 but lower than that in Glynn et al. (median of 65 ng/g lipid). 65 HCB had a geometric mean of 54.38 ng/g lipid (data not shown), which is lower than 379 ng/g lipid reported in the study of Jakszyn et al. 50 The observed concentrations of HCB among women in Novafeltria and Milan (geometric mean 193 and 564 pmol/g serum lipid, respectively) were higher than those observed among Italian women with endometriosis and those with other gynaecologic conditions (geometric mean 126 and 144 pmol/g lipid, respectively) 24 (Table 5).
To give a final picture of the outcome of our study, a further consideration may be useful. In particular, in the subjects who live in Milan and who are younger, many OCPs (β-HCH, p,p′-DDT, o,p′-DDE, o,p′-DDD in all genders and o,p′-DDT in females) were not detected. However, those which were detected surprisingly presented higher levels than in the older subjects of Novafeltria and Pavia. Milan is an industrial city in Northern Italy, where DDT and other chlorinated insecticides were used with much lower frequency than in other regions, such as rural and Southern Italy. In the same decades when DDT was used, Milan hosted a high immigration of formerly rural workers from Centre and Southern Italy, which raised its population by approximately 30% from 1950 to 1970. It is thus conceivable that the high level of OCPs observed in the current inhabitants of Milan may be due to several factors, among which: (a) the body burden of people coming from DDT-treated areas, including the contribution of contaminated agricultural food and (b) for the younger subjects, transmission of mothers’ body burden of DDT through pregnancy and breastfeeding. On the contrary, Pavia experienced much less and later immigration from remote areas of Italy, while Novafeltria never attracted considerable immigration from distant places. Mobility census in Italy was abolished in the early 1970s, demographic data of the examined subjects were not considered when this research was planned and this information is no more retrievable, due to the anonymity of subjects after the questionnaire was filled in, in order to test this hypothetical explanation.
In conclusion, our study has demonstrated a clear pattern of the main OCPs in a fairly large population. p,p′-DDE and HCB were the most abundant and major contributor of total OCP concentration. Their concentrations differ significantly between places of residence. In particular, the subjects who live in Milan, who are younger, presented higher levels of total OCP, total DDT, p, p′-DDE and HCB than in the older subjects of Novafeltria and Pavia. It is not clear what caused such elevated concentrations in this population since in this city there was no history of intensive use of pesticides in the past. Residential history, diet and industrial activities are thus suspected as determinants and this may warrant more detailed investigations on people living in Milan. Data collected in our study, however, provide information regarding the levels of OCPs exposure of the Italian general population and provide indications for the conduction of further investigations and open the way to planning more detailed investigations in other similar population studies.
Footnotes
Author’s Notes
The authors EJ Mrema and FM Rubino contributed equally to this manuscript
Conflict of Interest
The authors declared no conflict of interest.
Funding
This study was partially financially supported by the Italian Ministry of Health within research project entitled REALEXPO (2009-2010).