
Abstract
This study is designed to observe the effects of N-acetylcysteine (NAC) on doxorubucine-induced cardiac toxicity in rats both histologically and biochemically. Totally 32 rats divided equally into four groups were studied. The first group received only 200 mg/kg NAC intraperitoneal (i.p.) once every 24 h for 5 days (group 1); the second group received 20 mg/kg doxorubucine (DOX) i.p. single dose plus NAC 200 mg/kg i.p. once every 24 h for 5 days (group 2); the third group received DOX 20 mg/kg DOX i.p. single dose (group 3) and the fourth group, which is also the control group, received saline (group 4). Following 24 h of the final dose, blood samples were drawn from a portal vein and heart tissue were obtained. Tissue thiobarbituric acid reactive substance (TBARS) and nitric oxide (NO) levels were highest in the DOX group. In the DOX-treated rats, serum TBARS, NO, aspartate transaminase, lactate dehydrogenase and creatine kinase levels were highest when compared with other groups. Except for serum superoxide dismutase levels, all other parameters differed significantly between the DOX plus NAC group and the DOX group. In the DOX plus NAC group, general architecture was preserved better than the DOX group and myofibril loss was minimal compared with the DOX group. NAC demonstrated, both biochemically and histologically, to be effective in the prevention of DOX-induced cardiotoxicity in rat models. Evaluation of NAC’s effect on DOX toxicity warrants further clinical trials on cancer patients.
Keywords
Introduction
Doxorubicin (DOX) is a potent, broad-spectrum cancer chemotherapeutic agent widely used in the treatment of hematologic malignancies and solid tumors. 1 Unfortunately, it is notorious for its serious toxic effects on the cardiovascular system such as congestive heart failure, rhythm disturbances and cardiomyopathy leading to left ventricular dysfunction. 2 At the cellular level, DOX has been shown to cause disruption of the cardiac myocyte structure, including damage to the microtubules, sarcomere disruption, dilatation of the sarcoplasmic reticulum, mitochondrial injury and loss of myofibrils.3,4 There are several mechanisms hypothesized to explain DOX-induced cardiotoxicity, including free radical production that can damage cells by lipid peroxidation, decreases in antioxidant enzyme levels, inducing mitochondrial apoptosis pathways and altered intracellular calcium homeostasis.4–6
In organism, the oxidant–antioxidant system is balanced. DOX has been accepted as one of the causative factors of the disruption and may change the oxidant–antioxidant status. Reactive oxygen species (ROS), namely, superoxide anion, hydroxyl radical, hydrogen peroxide, nitrogen species and sulfur-centered radicals are the major culprits of free radical damage. These metabolites and the induction of lipid peroxidation products such as malonyl aldehyde (MDA) are responsible for severe cellular injury. In addition to the free radical formation, DOX has been shown to result in cardiotoxicity by reducing the activity of antioxidant enzymes such as catalase, glutathione peroxidase (GSH-Px) and superoxide dismutase (SOD).7,8 Antioxidants (vitamins C, E, selenium, etc.) are heterogenous molecules responsible for scavenging ROS thus alleviating their detrimental effects and exhibit protective effect for DOX-induced cardiotoxicity. Glutathione (GSH) is an important nonenzymatic endogenous antioxidant. N-acetylcysteine (NAC) is a thiol-containing compound widely used as a mucolytic drug in the treatment of chronic obstructive pulmonary disease. Its mechanisms of action include replenishing depleted GSH stores, direct scavenging of ROS, inhibition of neutrophil activity and tumor necrosis factor production. 9
We designed the following study to establish the protective effect of NAC against DOX-induced cardiotoxicity in rats and the changes in oxidant–antioxidant status of myocardium.
Materials and methods
All the animal experiment protocols were approved by the Animal Ethical Committee of Mustafa Kemal University. Experiments were performed on 32 mixed strain albino Wistar rats that were obtained from the experimental research center of Fırat University. The first group received only 200 mg/kg NAC 10 intraperitoneal (i.p.) once every 24 h for 5 days (group 1); the second group received 20 mg/kg DOX i.p. single dose 11 plus NAC 200 mg/kg i.p. once every 24 h for 5 days (group 2); the third group received 20 mg/kg DOX i.p. single dose (group 3) and the fourth group, which is also the control group, received saline (group 4). At the end of the experiment, 24 h after the last dose given at the end of day 5, general anesthesia with ketamine (50 mg/kg) and xylazine (10 mg/kg) was administered subcutaneously, and the blood samples were drawn by opening the animals at the midline and dissecting the portal vein. Then hearts were quickly removed and divided equally into two longitudinal sections. One of these parts was placed in formaldehyde solution for routine histopathological examination by light microscopy. The other half was frozen in liquid nitrogen and then stored at −70°C until assayed for the thiobarbituric acid reactive substance (TBARS), a lipid peroxidation product.
Determination of nitric oxide activity
Nitric oxide (NO) has very short half-life. The oxidation products of NO, nitrite (NO2), and subsequently nitrate (NO3) serve as an index of NO production. The method for measuring plasma nitrite and nitrate levels was based on the Griess reaction. 12 Samples were initially deproteinized with Somogyi reagent. Total nitrite was measured by spectrophotometry at 545 nm after conversion of nitrate into nitrite by copperized cadmium granules. A standard curve was established from nitrite standards to analyze unknown sample concentrations. Results were expressed as micromoles per gram wet tissue (millimole per gram of wet tissue).
Determination of SOD activity
The principle of the total SOD activity method is based, briefly, on the inhibition of nitro blue tetrazolium (NBT) reduction by the generated xanthine/xanthine oxidase system. 13 Activity was assessed in the ethanol phase of the serum after the addition of 1.0 ml of ethanol/chloroform mixture to the same volume of the serum and centrifuged. One unit of SOD was defined as the enzyme amount causing 50% inhibition in the NBT reduction rate.
Determination of TBARS levels
The TBARS levels were determined by a method based on the reaction with TBA at 90–100°C. 14 In the TBA test reaction, MDA or MDA-like substances (i.e. the by-product of lipid peroxidation process of the polyunsaturated fatty acids [PUFAs]) and TBA react together for the production of a pink-colored pigment with a maximum absorption at 532 nm. The sample (serum and tissue homogenate) was mixed with two volumes of 10% cold trichloroacetic acid to precipitate the protein. The precipitate was pelleted by centrifugation and an aliquot of the supernatant was reacted with an equal volume of 0.67% TBA in a boiling water bath for 10 min. After cooling, the absorbance was read at 532 nm (Ultra spec Plus, Pharmacia LKB Biochrom Ltd, England). Results were expressed as nanomole per gram of wet tissue and nanomole of gram protein for serum, by reference to a standard curve prepared from measurements made with a standard solution.
Biochemical parameters
Plasma aspartate transaminase (AST), lactate dehydrogenase (LDH), and creatine kinase (CK) enzyme activities were measured with an Olympus AU600 (Olympus Diagnostics, Tokyo, Japan) autoanalyzer. The results were expressed as international units per liter (Ul)−1.
Histological evaluation
Immediately after killing, a sample of the heart tissue was fixed in 10% neutral formalin. The washed tissue was dehydrated in graded alcohol series (70%–100%) and finally cleared in xylene. The tissue was embedded in paraffin wax. Sections were cut at 5 µm thickness and stained with hematoxylin and eosin. The sections were then viewed under an Olympus CX-40 light microscope for histopathological examination. Histological changes were graded as: 0, normal; 1, minimal inflammatory cell infiltration; 2, widespread inflammatory cell infiltration without any evidence of fibrosis and 3, minimal or widespread inflammatory cell infiltration with fibrosis. 15
Statistical analysis
All data presented are expressed as mean and standard deviation (SD). Statistical analysis was performed using the SPSS 15.0 (SPSS Inc., Chicago, Illinois, USA) statistical software package. The Kruskal–Wallis H test was used to compare four groups of independent, nonparametric numerical data. The significances of the difference between the groups in the numbers of tissue and blood concentrations were tested using Mann–Whitney U test. Significance was set at p < 0.05.
Results
Tissue TBARS and NO levels were highest in the DOC group (group 3). NO levels differed significantly between group 2 (DOX plus NAC) and group 3 (DOX only) (p <0.01). Markers of tissue damage did not differ significantly between groups 2 and 4 (p > 0.01; Table 1). When compared with group 4, serum SOD, TBARS, NO, AST, LDH and CK levels were significantly higher in group 3 due to tissue damage (p = 0.002). Serum SOD levels were highest in group 1. In DOX-treated rats, serum TBARS, NO, AST, LDH and CK levels were highest when compared with other groups. Except for serum SOD levels, all other parameters differed significantly between groups 2 and 3 (p = 0.002). Serum SOD, CK and LDH levels differed significantly between groups 2 and 4 (p < 0.01; Table 2).
MDA and NO values in the heart of the four groups of rats

DOX: doxorubicin; MDA: malonyl aldehyde; NAC: N-acetylcysteine; NO: nitric oxide.
Blood SOD, MDA, NO, AST, LDH and CK levels

AST: aspartate transaminase; CK: creatine kinase; DOX: doxorubicin; LDH: lactate dehydrogenase; MDA: malonyl aldehyde; NAC: N-acetylcysteine; NO: nitric oxide.
Tissue sections of groups 1 and 4 showed normal cardiac histology (Figure 1). In DOX-treated group, hemorrhage, interstitial edema and loss of myofibrils with fiber disorganization were observed (Figure 2). In higher magnifications, myofibril loss with cytoplasmic vacuolization was seen (Figure 3). In group 2, general architecture was preserved better than the DOX group, however, edema and fiber disorganization remained in some regions (Figure 4). Myofibril loss was minimal compared with the DOX group (Figure 5). The results are summarized in Table 3.
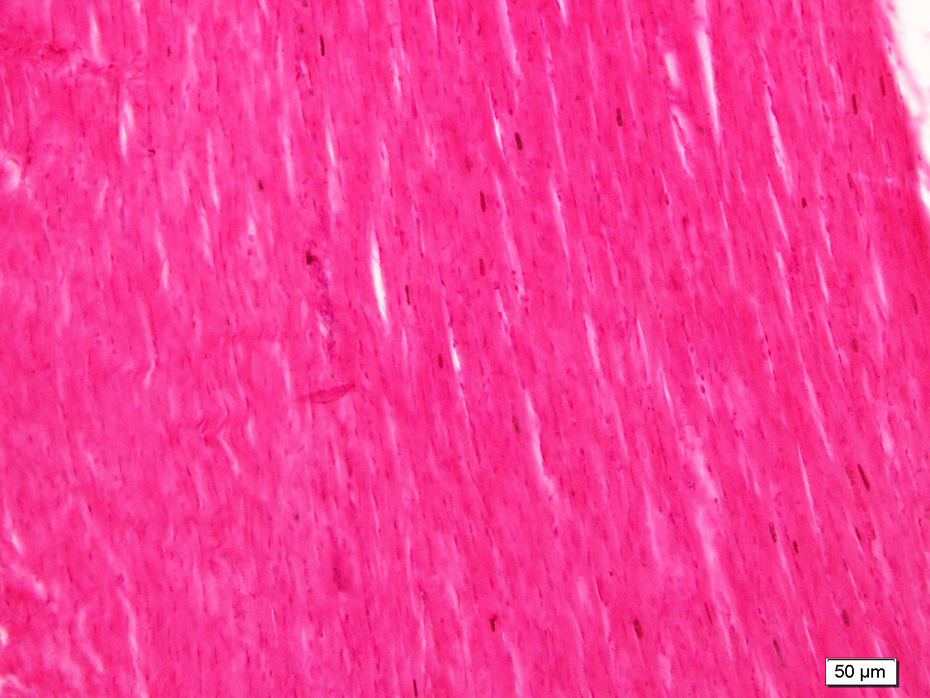
Normal cardiac morphology in the NAC group. NAC: N-acetylcysteine.

Hemorhage (→), interstitial edema (*) and loss of myofibrils with fiber disorganization in the doxorubicin group.

Myofibril loss (*) with cytoplasmic vacuolization (→) in the doxorubicin group.

Well-preserved general architecture with edema (*) and fiber disorganization (fd) in some regions in the NAC + doxorubicin group. NAC: N-acetylcysteine.

Minimal myofibril loss in the NAC + doxorubicin group. NAC: N-acetylcysteine.
Effects of DOX and DOX + NAC administration on the cardiac histology of the rats (n = number of animals)

DOX: doxorubicin; NAC: N-acetylcysteine.
Discussion
DOX is a potent and broad-spectrum chemotherapeutic agent commonly used in the treatment of hematologic and solid tumors. 1 However, there are serious toxic effects of DOX on the cardiovascular system, which limits its widespread use. 4 There are several mechanisms hypothesized to explain DOX-induced cardiotoxicity, the most popular being the ROS-mediated myocardial oxidative stress. Several antioxidant agents including, vitamin E, 16 vitamin C, 17 selenium, 18 erdostein 19 and carvedilol 20 have been reported to prevent cardiotoxicity due to DOX administration. Previous animal studies demonstrated antioxidant effects of NAC in heart, liver and kidney tissues with free radical injury.21–23 To our knowledge, our study is unique in evaluating the effects of NAC administration on DOX cardiotoxicity both biochemically and histologically.
We used serum CK, AST and LDH enzyme levels as markers of cardiac toxicity. Despite the fact that these enzymes are not specific for myocardial damage, it is reported their use in combination they may be more reliable indicators of myocardial damage. 24 In our study, AST, LDH and CK levels were highest in group 3 rats. When groups 3 and 4 were compared, levels of these enzymes were significantly different thus demonstrating DOX-induced cardiotoxicity. AST, LDH and CK levels were significantly different between groups 2 and 3. This finding supports the hypothesis that NAC prevents DOX-induced cardiotoxicity.
Free radical production that can damage cells by lipid peroxidation is one of the mechanisms known to be responsible for cardiotoxicity of DOX. Other proposed mechanisms for DOX-induced cardiotoxicity are disruption of cellular and mitochondrial Ca++ homeostasis, impaired expression of important cardiac proteins, disruption of cardiac myocyte cytoskeleton. 25 Superoxide, hydroxyl radicals and NO are major offenders of cardiac toxicity. It is documented that end-products of lipid peroxidation such as MAD contributes to cardiac toxicity of DOX.7,8 DOX disrupts the balance between oxidant and antioxidant molecules. In our study, it was documented that serum and tissue TBARS and NO levels differed significantly between both groups 3 and 4 and groups 2 and 3. This finding supports the hypothesis that DOX toxicity is primarily due to free radical injury and NAC seems to prevent this damage. In our study, serum SOD levels were significantly higher in the DOX-treated group compared with the control group. This may be attributed to the fact that antioxidant enzyme activity fails to detoxify end-products of lipid peroxidation due to DOX toxicity.
Detrimental effects of DOX application on cardiac tissues were previously shown histologically.26,27 They all reported similar histologic findings such as myocardial fibril loss, edema and fiber disorganization as reported in this study. Additionally, we showed protective effect of NAC on cardiac morphology with less myocardial fibril loss and better preserved general architecture compared with the group 3 and fibrosis was not observed.
In our study, we preferred NAC because it is a potent antioxidant. Our results demonstrate that NAC administration prevents DOX-induced cardiotoxicity. However, mild histologic findings of tissue damage were still observed in the DOX plus NAC group. This may be attributed to other detrimental effects of DOX apart from antioxidant injury, which cannot be prevented by NAC, such as the disruption of cardiac myocyte structure.
In conclusion, NAC was demonstrated, both biochemically and histologically, to be effective in the prevention of DOX-induced cardiotoxicity in rat models. However, how NAC affects antitumor properties of DOX was not documented. Evaluation of NAC’s effect on DOX toxicity warrants further clinical trials on cancer patients.
Footnotes
Conflict of Interest
The authors declare that they have no competing interests. The manuscript has been seen and approved by all authors, it is not under active consideration for publication, has not been accepted for publication, nor has it been published
Authors’ contributions
The authors CLH and DRH have contributed equally to the draft of the manuscript. Both authors have read and approved the final manuscript. The experiments received approval from the ethical committee.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.