
Abstract
Fatal alcohol and drug poisonings in Finland during the years 2004–2009 were studied. Cases were divided into those that occurred outside the hospitals (the majority of cases) and those that occurred within the hospitals (the minority of cases). Differences and similarities between the two groups were analysed. The postmortem toxicological investigation of all sudden and unexpected deaths in Finland is centralised at the Department of Forensic Medicine, University of Helsinki. We examined each fatal poisoning separately and verified the cause and place of death as well as the age and sex of the deceased. Fatal poisonings, including suicides, have remained unchanged for many years from the same high level, that is, about 1200 cases annually (22/100,000 inhabitants). The number of patients dying in hospitals due to poisoning has also remained stable (55–70 patients/year). However, the toxic agents involved in such poisonings have changed and deaths due to opioids are now being more numerous. The number of fatal unintentional drug poisonings rose significantly from 191 to 341 (3–6/100,000 inhabitants, p < 0.001) during the study years, and the difference between poisonings caused by drugs or alcohol also changed significantly (p < 0.001). Diminishing substantially, the number of all fatal poisonings will be challenging because of the high percentage of suicides. However, a reduction in unintentional drug overdoses, which are presently on the rise, should be possible.
Introduction
Epidemiological studies show that the intoxicated patients are a major group in healthcare and that the incidence of deaths from poisoning is rising, even in the developed countries such as the United Kingdom and Finland. 1 –4 Many case studies focussed on the signs, symptoms and treatments of different poisons, but studies focussing on the mortality due to poisoning, which cover the whole country are not numerous. 5 –7
Previous studies have shown that the deaths due to poisoning outside the healthcare system are much more numerous than those in hospital settings. 8 One study compared prehospital-treated cases of poisonings with those that were hospitalised for 1 year in Oslo, Norway. This study mainly revealed a wide variety of substances causing poisoning, but failed to comment on the resulting mortality. 9
In view of the high mortality from poisoning in Finland, this study aimed to investigate the fatal poisonings occurring both inside and outside the healthcare system. 4 These cases were divided according to the place of death. Those who died outside the hospital formed one group and those who were still alive at the moment of first contact with healthcare personnel formed the other group. Also of interest was whether the substances causing the deaths differed between the two groups and, how stable these numbers are from year to year.
Methods
All postmortem toxicology in Finland is centralised by the law at a single laboratory, known as the Hjelt Institute, Department of Forensic Medicine, University of Helsinki. The laboratory maintains a database that includes all toxicological findings, background information and demographic data as well as the causes and manner of death. The forensic pathologist who issues the death certificate assesses the main cause of poisoning, expresses the finding using International Classification of Diseases-10 codes and reports the background information collected by the police. In this study, suicides were established by means of a farewell letter or some other clear sign of intent, while all other cases were classified as accidents.
Most of the fatal poisonings happened without any contact with the healthcare system, while a smaller number died after treatment had been started. One major group of patients within the in-hospital group are those who were asystolic when found. Resuscitation was started, and the patients were brought to the hospital. In the intensive care unit, appropriate tests indicated brain death, and intensive care was terminated as it elicited no response.
In suspected poisonings, the postmortem laboratory investigations always include blood and urine alcohol determinations and a broad-scale urine and blood screening/confirmation for possible toxic substances. In most cases, more than one agent is detected and the forensic pathologist selects the agent with the most toxic profile. For similar agents, the one present in the highest concentration when compared with the therapeutic range is selected. The laboratory receives a copy of the official death certificate as feedback, which includes the cause and manner of death. Additionally, there are also a short description of the events, the medical history of the deceased and the results of the police enquiry when relevant. One of the authors (OL-R) studied all the unclear cases in detail.
Based on the special register at the Department of Forensic Medicine, we received information about those who had fatal poisonings but were still alive at the point of first contact with the healthcare system. They formed a heterogeneous group, some of whom were still able to call the ambulance themselves, whereas others were found unconscious and an asystolic condition was quickly recognised. The inclusion criterion was whether death occurred in the presence of healthcare personnel; one of the authors (OL-R) studied these cases in detail. No age limits were imposed. The toxic agents behind the fatalities were compared using the chi-square test.
Results
Number of poisonings and related deaths
The postmortem samples from approximately 7000 deceased persons are referred to the Department of Forensic Medicine every year for toxicological investigation, and a total of about 1200 fatal poisonings are detected annually. The incidence of fatal poisoning remained largely unchanged during the study years, varying only slightly from 1118 to 1231 (21–23/100,000 inhabitants), while the proportion of suicides was also quite stable at 24–28% (276–341 cases, 5–6/100,000) per year. The number of fatal poisonings in the presence of healthcare personnel varied from 52 to 71 (1/100,000 inhabitants, 6% of the entire group) between 2004 and 2009, while the proportion of suicides being 30–40% annually (Table 1), which is slightly higher than that in the overall cases. Table 1 shows all the fatal poisonings (including e.g. carbon monoxide poisonings) that happened in Finland during the years 2004–2009.
All fatal poisonings (and suicides) in Finland between 2004 and 2009 and the subgroup of cases in which death occurred in hospital

Male/female
In total numbers, men outnumbered women in fatal poisonings. Furthermore, investigation of the deaths in hospital settings revealed that the number of deaths among men was higher than that among women for every year except 2005 and 2009, when the distribution between the sexes was nearly equal. The mean age ranged from 49 to 55 years among males and from 50 to 64 years among females.
Toxic agents
The total number of fatal poisonings remained largely unchanged, but a certain trend emerged in the type of toxic agent causing the poisonings. In fatal poisonings, ethanol alone no longer dominates, as during the study years, drugs became more popular: 637 (in 2009) versus 432 poisoning deaths (in 2009) in all, and 46 (in 2009) versus 4 poisoning deaths (in 2009) in hospitals. The number of unintentional fatal poisonings with medicines during the study years increased from 191 (in 2004) to 341 poisoning deaths (in 2009; p < 0.001); a similar trend is also evident in the rise in the number of deaths in hospitals from 11 (in 2004) to 19 poisoning deaths (in 2009). The number of suicides involving a drug overdose, however, remained stable, ranging from 266 (in 2004) to 296 poisoning deaths (in 2009). Overall, fatal ethanol poisonings (545 in 2004 to 432 in 2009) as well as the number of cases who sought treatment and died in hospitals (17 in 2004 to 4 in 2009) have declined in recent years. This decline in alcohol poisonings and the rise in those with drugs were significant (p < 0.001). These numbers are seen in Table 2 with the numbers of suicides given in parentheses.
Fatal drug and alcohol poisonings in Finland during the years 2004–2009a

aNumbers of suicides are indicated in parentheses.
The main agents involved in fatal poisonings in 2004–2009 are listed in Table 3, with the number of suicides given in parentheses. Antidepressants and opioids were the most common medicinal substances involved in fatal accidents every year. Tricyclic antidepressants such as amitriptyline and doxepin continued to dominate in such cases, even though newer agents were also common. Levomepromazine is present in almost half of the cases involving antipsychotics. The proportion of fatal poisonings attributable to cardiovascular agents was fairly constant, mostly due to β-blocking agents, although verapamil must be noted as a single substance that causes many poisonings, some of which are also fatal. Other agents are involved less frequently, although the rise in the use of pregabalin is evident in death statistics from 2009.
The main agents detected in fatal poisonings in Finland in overall and in deaths in hospitalsa

aNumbers of suicides are in brackets.
The same trends were also evident in those fatal poisonings where the patients were brought to the hospital (Table 3). Antidepressants and opioids were again prominent in these patients, but cardiovascular agents and antipsychotics were detected nearly as often. The number of substances found varied from one to three per case, depending on the importance of the finding.
Children and adolescents
No fatal poisonings occurred among the children younger than 10 years between 2004 and 2009, and the only fatal poisoning that concerned a child (age range 10–14 years) occurred in 2005, when one girl committed suicide using drugs. All fatal poisonings in the age group of 15–19 years occurred outside the hospital, and the most common toxic agents were alcohol and drugs together. The number of these cases was stable from year to year, as were the numbers of both unintentional deaths and suicides. The drugs involved in these cases were mainly morphine derivatives or psychotropic drugs such as quetiapine. Ethanol was taken together with drugs, but in only four cases, the ethanol was found to be the primary cause of death; and in every case, the blood ethanol level exceeded 2 mg/g, the highest value being 4.2 mg/g. Each year, the unintentional fatal poisonings were more common than suicides (Table 4). All adolescents who abused the drugs were found dead, and the healthcare personnel had no opportunity to save their lives.
Fatal poisonings among children between 15 and 19 years of age in Finland during the years 2004–2009a
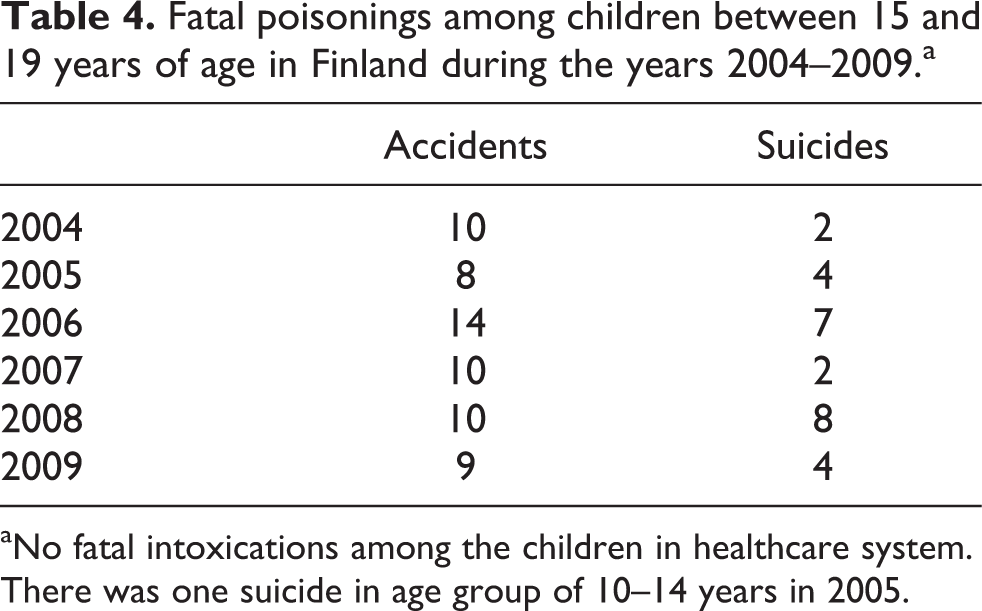
aNo fatal intoxications among the children in healthcare system. There was one suicide in age group of 10–14 years in 2005.
Discussion
Studies concentrating on hospitalised patients who die due to poisoning are not numerous and are usually limited to case studies or focus on management. 10 –12 Furthermore, the number of such patients is small, and previous studies have shown that most fatal poisonings occur outside hospitals, a finding of which our study confirmed. In addition, most fatal poisonings in hospitals involved suicidal people. Thus, the increase in the effectiveness of the treatment will probably not greatly diminish the number of the fatal poisonings, while prevention of poisoning being the most effective means.
The number of deaths was higher among men than women, which is exactly the opposite of a previous finding that women are more often hospitalised due to poisoning. 13 Our study did not investigate morbidity, but it is possible that the cases of poisoning are more numerous among women, whereas those among men are more serious. As previous studies have shown, mortality due to poisoning among children in Finland is very low. 4 During the study years, no victim younger than 19 years died from poisoning in the healthcare system, and the fatal poisonings outside the hospitals were few.
The total number of fatal poisonings was fairly stable during the study period, although the agents causing these poisonings changed. In unintentional poisonings, drugs became increasingly common year after year, whereas ethanol as a cause of death either remained steady (death outside hospital) or even decreased (death inside hospital). High consumption of ethanol is a common problem in many northern European countries and is a leading cause of monointoxications in many countries. 14 The high prevalence of fatal ethanol poisonings in Finland and Sweden has probably been not only due to the heavy drinking habits but also due to the higher rate of postmortem investigations and different established practices in determining the cause of death than in other countries. 15
In the present study, the patients were divided into two groups according to their place of death: outside hospital or inside hospital. The latter group was not as homogenous as the former, but it did include those patients who were already in terminal condition when first seen by the healthcare personnel. However, if there were no secondary signs of death, like rigor or livor mortis, they were resuscitated and brought to the hospital where a medical doctor finally confirmed the death. The two study groups showed neither clear differences in terms of gender and age nor there were any specific products found that could have posed a particular difference between the groups.
Suicides, however, seem to be committed mostly with medicinal substances every year, which was also noted in previous studies. 16 A significant reduction in suicide rates poses a challenge, but unintentional poisonings could serve as a focus, and the rise in drug poisonings should evoke concern. In particular, the number of deaths due to opioids is rising, while other analgesic agents such as paracetamol still play a minimal role in Finland. This rise in unintentional drug overdose mortality due to opioids has also occurred elsewhere. 17,18 In the United States, medical guidelines in 1997 stated a clear preference for opioids as pain medication, and since then their use has expanded. 17 Our study showed that this rise has also occurred in Finland in recent years.
Limitations
The classification of cases to accidental and intentional ones may include some weaknesses. Only confirmed suicides are included in the intentional group, while unclear cases are included in the accidental group. The classification was based on the judgement of the specialist of the forensic medicine who had signed the death certificate and one of the writers. If their opinions differed and if the case was unclear, then it was not included in the intentional group but was included in the accidental group.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.