
Abstract
Several experimental, pathological, epidemiological, and clinical studies have clearly depicted that diabetes mellitus results in cardiac functional and structural changes. Diabetic cardiomyopathy results in both structural and functional alterations in the myocardium. Several mechanisms have been implicated in the pathophysiology of diabetic cardiomyopathy. Of these, metabolic disturbances, myocardial fibrosis, small vessel disease, and cardiac autonomic neuropathy are the major players in the pathophysiology of diabetic cardiomyopathy. This review is intended to discuss various such pathophysiological mechanisms of diabetic cardiomyopathy. We have also described the systolic and diastolic dysfunctioning and its corelation to structural changes in diabetes.
Keywords
Introduction
As per World Health Organization factsheet, diabetes increases the risk of heart disease and 50% of people with diabetes die of cardiovascular disease. 1 The epidemic of obesity and sedentary lifestyle is projected to result in over 300 million people with diabetes mellitus by 2025. 2 Developing nations will bear a disproportionate burden of this increase, with an expected 170% rise from 84 million to 228 million affected individuals. This trend is particularly ominous, as those in the developing nations tend to develop diabetes earlier in life (at an age of 40–64 years) than their counterparts in the developed world (at an age of 65 years or older), implying a longer duration of exposure during the most productive years and, therefore, a potentially greater risk of diabetes-associated morbidity and mortality. 2
In early 1970s, diabetic cardiomyopathy was originally described when four diabetic patients presented with heart failure without the evidence of hypertension, coronary artery disease (CAD), valvular, or congenital heart disease. 3 Thereafter, large number of molecular, epidemiological, and diagnostic studies have been carried out in relation with diabetic cardiomyopathy. Accumulating data from experimental, pathological, epidemiological, and clinical studies have shown that diabetes mellitus results in cardiac functional and structural changes. 4 In one of the largest epidemiologic studies, involving over 800,000 patients, diabetes was found to be independently associated with the occurrence of congestive heart failure after adjusting for left ventricle (LV) hypertrophy, hypertension, CAD, and atrial fibrillation. 5 Once clinical cardiovascular disease develops, these patients have a poorer prognosis than normoglycemic patients. However, on the functional level, cardiovascular dysfunction during dysregulated metabolism occurs soon after the onset of metabolic abnormalities, long before the appearance of histopathological changes, and such dysfunction is regulated by dynamic and complex mechanisms on the cellular and molecular levels. This gives hope that the intervention with preventive therapies is possible at a stage before atherosclerosis and heart failure are manifested. The present review article shall familiarize the readers with the structural and functional changes in diabetic cardiomyopathy and the related pathophysiology.
Pathophysiology of diabetic cardiomyopathy
There are three major stages of diabetic cardiomyopathy, that is, early stage, middle stage, and the late stage (Table 1). 4 Several factors such as metabolic disturbances, myocardial fibrosis, small vessel disease, autonomic dysfunction, and insulin resistance have been implicated as putative mechanisms leading to diabetic cardiomyopathy.
Three stages of diabetic cardiomyopathy

GLUT4: glucose transporter 4; FFA: free fatty acids; LV: left ventricle; IGF-I: insulin-like growth factor-I; TGF-β1: transforming growth factor-β1; AT II: angiotensin II; CAN: cardiac autonomic neuropathy; CAD: coronary artery disease.
Metabolic disturbances
Normally, the heart utilizes free fatty acids (FFAs) as its primary energy source during aerobic perfusion at normal workloads and increasingly relies on glycolysis and pyruvate oxidation during periods of ischaemia or increased work. 6
Alterations in substrate supply and utilization
Hyperglycaemia triggers metabolic changes in diabetes directly. Diabetic hearts have primary defect in the stimulation of glycolysis and glucose oxidation. 7 Altered substrate supply and utilization by cardiac myocytes could be the primary injury in the pathogenesis of diabetic cardiomyopathy. 8 A major restriction to glucose utilization in the diabetic heart is the slow rate of glucose transport across the sarcolemmal membrane into the myocardium, due to cellular depletion of glucose transporters (GLUTs) 1 and 4. 9 Another mechanism of reduced glucose oxidation is via the inhibitory effect of fatty acid oxidation on pyruvate dehydrogenase complex due to high circulating FFA and the net effect is reduced availability of ATP. 10
In perfused hearts obtained from genetically diabetic mice, substrate metabolism affecting contractile function in diabetes has been characterized. 11 Contractile dysfunction was evident in the genetically diabetic hearts, with increased LV end-diastolic pressure and reduced LV developed pressure, cardiac output, and cardiac power. The rate of glycolysis from exogenous glucose in diabetic hearts was 48% of control, whereas glucose oxidation was depressed to 16% of control, and palmitate oxidation was increased twofold. Overexpression of GLUT4 in perfused hearts from the genetically diabetic mice normalized both cardiac metabolism and contractile function supporting a causative role of impaired glucose metabolism in the cardiomyopathy observed in genetically diabetic hearts. 12 An echocardiographic study was carried out to determine whether contractile function in diabetic db/db mice was reduced in vivo and restored in mice where the transgenic db/db-human GLUT4 had been added to normalize cardiac metabolism. Results depicted that both systolic and diastolic functions were unchanged in 6-week-old db/db mice, but fractional shortening and velocity of circumferential fiber shortening and the ratio of E and A transmitral flows were reduced in 12-week-old db/db mice, indicating the development of a cardiomyopathy. These cardiac functional changes were normalized in transgenic db/db-human GLUT4 mice, 13 confirming that the in vitro findings that altered cardiac metabolism can cause contractile dysfunction in db/db hearts and that the process is associated with substrate supply and utilization. However, the major derangement in carbohydrate metabolism in diabetic myocardium was not in glycolysis but in pyruvate oxidation. 14,15
FFA metabolism
Elevated FFA levels are believed to be one of the major contributing factors in the pathogenesis of diabetes. Independent of the effects of hyperlipidaemia on coronary artery endothelial function, the increase in and dependence of diabetic myocardium on fatty acid supply result in several major cellular metabolic perturbations (Figure 1). 16 FFAs enhance peripheral insulin resistance and trigger cell death. Disturbances of FFA metabolism may be an important contributor to abnormal myocardial function in diabetes. These changes are characterized by the elevation of circulating FFAs caused by enhanced adipose tissue lipolysis as well as by high tissue FFAs caused by hydrolysis of augmented myocardial triglyceride stores. Moreover, in addition to the FFA-induced inhibition of glucose oxidation (which may contribute to the above effects by limiting the entry of glucose into the cell), high circulating and cellular FFA levels may result in abnormally high oxygen requirements during FFA metabolism and the intracellular accumulation of potentially toxic intermediates of FFA, all of which lead to impaired myocardial performance and severe morphological changes. 8,17 Abnormalities in FFA metabolism have been demonstrated in idiopathic dilated cardiomyopathy in which the rate of FFA uptake by myocardium is inversely proportional to the severity of the myocardial dysfunction. 18 It is possible that similar defects contribute to the development of diabetic cardiomyopathy. There is increased β-oxidation and mitochondrial accumulation of long-chain acyl carnitines, leading to uncoupling of oxidative phosphorylation. 19 Enhanced fatty acid oxidation decreases glucose and pyruvate utilization by inhibiting pyruvate dehydrogenase. Pyruvate oxidation is reduced further by pdk4 and activated by peroxisome proliferator-activated receptor (PPAR). The net result is an excess of glycolytic intermediates and increased synthesis of ceramide leading to apoptosis, which can be prevented by the PPAR-α and -γ agonist troglitazone. 20 Thus, impaired glycolysis, pyruvate oxidation, lactate uptake, and a greater dependence on fatty acids as a source of acetyl coenzyme A leads to a perturbation of myocardial bioenergetics and contraction/relaxation coupling. 8 The FFA-induced impairment in glucose oxidation may be a major factor in the development of diabetic cardiomyopathy and would explain why cardiac function tends to improve upon metabolic improvement. Furthermore, the availability of carnitine, an essential substance for myocardial FFA metabolism, is usually reduced in diabetes. Evidence of cardiomyopathy in streptozotocin-induced diabetic rats with no evidence of coronary vascular occlusion and normal serum cholesterol correlates with reduced serum and myocardial carnitine levels and abnormal-appearing mitochondria, consistent with carnitine deficiency. 21

Alterations in FFA metabolism and related pathophysiologic mechanisms of diabetic cardiomyopthy. FFA: free fatty acid; ↑: increase; ↓: decrease.
Abnormality in calcium homeostasis
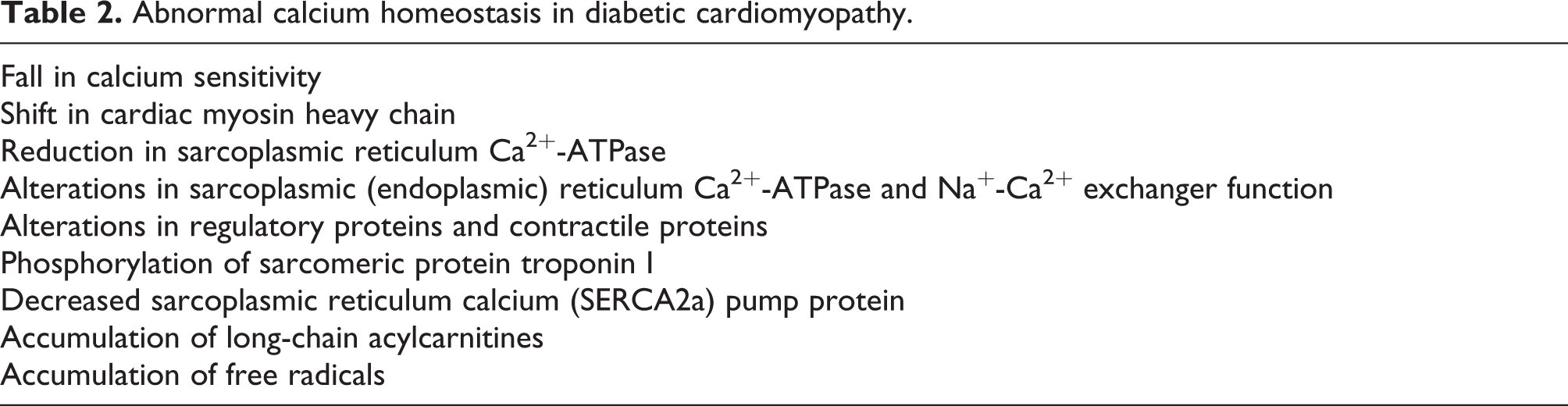
Abnormal calcium homeostasis occurs due to several reasons contributing significantly to diabetic cardiomyopathy (Table 2). Oxidative stress caused by toxic molecules may play a critical role in subcellular remodelling and abnormalities of calcium handling that lead to subsequent diabetic cardiomyopathy. A fall in calcium sensitivity, shift in cardiac myosin heavy chain (MHC), 22 reduction in sarcoplasmic reticulum Ca2+-ATPase, and decreased sarcoplasmic reticulum calcium (SERCA2a) pump protein may all contribute to impaired LV function. 23 The important contributors to abnormal myocardial carbohydrate and lipid metabolism in diabetes are alterations in regulatory proteins and contractile proteins, sarcoplasmic (endoplasmic) reticulum Ca2+-ATPase, and Na+–Ca2+ exchanger function. These changes likely result from the accumulation of toxic molecules such as long-chain acylcarnitines, free radicals, and abnormal membrane lipid content. The consequences of these changes include alterations to the calcium sensitivity of regulatory proteins involved in the regulation of the cardiac actomyosin system, possibly due to phosphorylation of sarcomeric protein troponin I. 24 Indeed, abnormal systolic and diastolic functions normalize after overexpression of SERCA2a in streptozotocin-induced diabetic rat hearts. 25 Similarly, investigation of steady state and transient changes in stimulus frequency on the intracellular Ca2+ transient and cell shortening shows a slower decay of the Ca2+ transient and longer times for maximum cell shortening and relengthening and an accompanying reduction in Ca2+ efflux from the cell, due to either depressed Na+/Ca2+ exchanger activity or an elevation in intracellular Na+ levels is the most likely reason for the same. 26 Other changes that have been demonstrated to contribute to the development of myofibrillar remodelling in the diabetic heart are alterations in the expression of myosin isoenzymes and regulatory proteins as well as myosin phosphorylation. 27
Abnormal calcium homeostasis in diabetic cardiomyopathy
Accumulation of AGEs
The hyperglycaemia leads to nonenzymatic glycation of macromolecules. The sugars linked to macromolecules are condensed into large heterocyclic derivatives by complex reaction and they are labelled as advanced glycation end products (AGEs). These AGEs accumulate in tissues and are implicated in morphological changes that occur in the diabetic heart. Inelasticity of the vessel wall occurs due to the accumulation of AGE-modified extracellular matrix and this results in the interference of the myocardial function. It is reported that in diabetes, prolongation of isovolumic relaxation time, as assessed by Doppler echography, correlated with serum levels of AGEs after adjustment for age, diabetes duration, renal function, blood pressure, and autonomic function parameters. 28
Activation of PKC
Increased activation of the diacylglycerol (DAG)-activated protein kinase C (PKC) signal transduction pathway has been identified in vascular tissues from diabetic animals and in vascular cells exposed to elevated glucose. 29 Hyperglycaemia-induced upregulation of PKC by DAG has been proposed as a mechanism in the development of vascular complications in diabetes. 30 This has been shown to induce many of the changes in diabetic cardiomyopathy, which include a reduction in tissue blood flow, enhanced extracellular matrix deposition, capillary basement membrane thickening, and increased vascular permeability with alterations in neovascularization. PKC interferes with the contraction proteins troponin-T, troponin-I, and troponin–tropomyosin complex. 30 Increased PKC activity influences nuclear gene transcription by way of the mitogen-activated protein kinase (MAPK) cascade to induce the immediate early gene programme with subsequent stimulation of late genes that increase the production of angiotensin converting enzyme (ACE), α-MHC, and skeletal α-actin. 31 ACE, in particular, may account for the development of abnormalities that contribute to the development of diabetic cardiomyopathy. 32
In cultured cardiomyocytes, incubation with high-glucose promotes Nuclear Factor-kB (NF-κB) activation through the DAG-PKC signal transduction pathway. This route increased PKCα and PKCβ2, which phosphorylated MAPK and lately IκB. 33 Also they lead to the release of vasoactive peptides and growth factors from the circulating and local cells. 34
Myocardial fibrosis
Myocardial fibrosis and myocyte hypertrophy are the most frequently proposed mechanisms to explain cardiac changes in diabetic cardiomyopathy. Several studies have shown that diabetes causes defects in cellular calcium transport, 35 defects in myocardial contractile proteins, 36 and an increase in collagen formation, 37 which result in anatomic and physiological changes in the myocardium.
Myocyte cell death
Myocyte cell death may be caused by apoptosis or necrosis or both. Apoptosis is programmed cell death involving genetically controlled process that removes unwanted or damaged cells, whereas myocyte necrosis refers to myocyte cell death due to biochemical damage. Identification of double-stranded DNA cleavage with single base or longer 3′ overhangs is the measure for the evaluation of apoptosis, while myocyte necrosis can be assessed by the detection of DNA damage with blunt end fragments. 38 Apoptosis does not cause scar formation or significant interstitial collagen accumulation, 39 with nuclear fragmentation and cell shrinkage being replaced by the surrounding cells. 40,41 Conversely, myocyte necrosis results in widening of the extracellular compartments among myocytes and increased deposition of collagen in a diffuse or scattered manner, 42,43 resulting from both replacement fibrosis due to myocyte necrosis and connective tissue cell proliferation. 44 In diabetic heart disease, both apoptosis and necrosis are involved. Frustaci et al. 45 reported that myocyte necrosis was 1.4-fold more prevalent in patients with diabetes and hypertension than with diabetes alone, whereas myocyte apoptosis was not affected by the addition of hypertension.
Process of myocardial fibrosis
Hyperglycemia also results in the production of reactive oxygen and nitrogen species, which increases oxidative stress and causes abnormal gene expression, alters signal transduction, and activates the pathways leading to programmed myocardial cell death or apoptosis. This process is associated with the glycosylation of p53 resulting in an increment in angiotensin II (AT II) synthesis, which leads to p53 phosphorylation, increased Bax expression, and also myocyte apoptosis. Collagen accumulation in the diabetic myocardium may be due in part to impaired collagen degradation resulting from glycosylation of the lysine residues on collagen. 4 It is reported by Fiordaliso et al. 46 that the inhibition of p53 glycosylation prevents the initial synthesis of AT II and consequent p53 activation and apoptosis. Furthermore, it is also reported that hyperglycemia triggers generation of reactive oxygen species and this directly induces apoptotic cell death and myocyte necrosis in the myocardium. 47 A similar study reports that cardiomyocytes incubated for 3 days with medium containing 25 mM glucose showed less hypoxia-induced apoptosis and necrosis than cells exposed to medium containing 5 mM glucose, suggesting that glucose treatment renders the cardiomyocytes resistant to hypoxia-induced apoptosis and necrosis. 48
Alterations in endothelin-1 and its receptors were associated with increased focal fibrous scarring with apoptotic cardiomyocytes in diabetic rats, and the fibrotic process was completely prevented by treatment with bosentan. This suggests that hyperglycemia-induced upregulation of the endothelin system in the diabetic heart may play an important role in myocardial fibrosis. 49 An in vivo study in streptozotocin-induced diabetic rats showed an increased AT II and angiotensin receptor levels and changes in AT II quantity, the fraction of AT II positive cells, and the number of AT II receptor sites per myocyte paralleled the change in myocyte death. 50 The change in AT II and AT II receptors in diabetic hearts appears to be local and independent of the circulating renin–angiotensin system. 51,52 This upregulation of the local renin–angiotensin system in diabetes may enhance oxidative damage, activating cardiac cell apoptosis, and necrosis. 45 Thus, either increased AT II or increased AT II receptor density enhances the effect of AT II, and this AT II has dose-dependent effects on collagen secretion and production in rat adult cardiac fibroblasts. 53
Insulin-like growth factor-I (IGF-I), a key factor for cardiac growth and function, modulated the local AT II effects. Cardiomyocytes generate AT II and IGF-I, and it exerts pleiotropic effects in an autocrine/paracrine fashion. IGF-I reduces both AT II and apoptosis. IGF-I also plays an important role in myocardial fibrosis and development of diabetic cardiomyopathy. IGF-I is decreased in diabetes, and exogenous IGF-I treatment has been shown to ameliorate contractile disturbances in cardiomyocytes from diabetic animals. 4 In an experimental model of streptozotocin-induced diabetic mice, diabetes progressively depressed ventricular performance but had no haemodynamic effect on those with IGF-I overexpression. Myocyte apoptosis measured at 7 and 30 days after the onset of diabetes was twofold higher in diabetic mice without IGF-I than with IGF-I overexpression. Myocyte necrosis was apparent only at 30 days and was more severe in diabetic nontransgenic mice, which lost 24% of their ventricular myocytes and showed 28% myocyte hypertrophy, both of which were prevented by IGF-I. 54 Therefore, resistance to actions of IGF-I and insulin could explain the abnormalities of both diastolic and systolic function and LV hypertrophy.
Transforming growth factor-β1 (TGF-β1) also promotes the effects of AT II. 55,56 TGF-β1 plays a critical role in organ morphogenesis, development, growth regulation, cellular differentiation, gene expression, and tissue remodelling. Metabolic abnormalities such as chronic postprandial hyperglycemia, hyperinsulinemia, and insulin resistance induce TGF-β1, and this is implicated in the development of diabetic cardiomyopathy. In the heart of rat, TGF-β increases fibrous tissue formation and upregulates collagen expression during tissue repair by binding to TGF-β type-II receptor. Expression of TGF-β1 type-II receptor has been shown to be significantly increased in the LV of Otsuka Long-Evans Tokushima fatty (OLETF; type-2 diabetes model) rats, and the ratio of collagen content/dry weight of the LV was significantly higher in OLETF rats than in control rats at 15 weeks of age. 57
Overexpression of core 2 GlcNAc-T may contribute to the cardiac abnormalities similar to those observed in experimental animals and patients with diabetes. Koya et al. 58 produced transgenic mice overexpressing core 2 GlcNAc-T and reported that elevations of core 2 GlcNAc-T activities contributed to cardiac hypertrophy and increased c-fos/gene expression and AP1 activity. The mechanisms of action of core 2 GlcNAc-T were explored further and it was found that core 2 GlcNAc-T overexpression also induced c-fos expression, AP1 activation, altered glycosylation, and signalling threshold of Trk receptors. 58 Moreover, development of diabetic cardiomyopathy is accelerated after the disruption of 14-3-3 protein function, in part through enhancement of the Ask1 signalling pathway. This process subsequently contributes to myocardial remodelling events like hypertrophy, interstitial fibrosis, and endothelial dysfunction. 59
Consequences of myocardial fibrosis
Fibrosis is attributed to replacement fibrosis caused by focal myocyte necrosis 60,61 and increased interstitial fibrosis, in part due to the reaction of connective tissue cells to pathological loads. 44 Nunoda et al. 62 carried out a biopsy study in patients with diabetes mellitus and showed that hypertrophy of myocardial cells and interstitial fibrosis of the myocardium are present in mild diabetes mellitus. In a longitudinal study of cardiac performance in streptozotocin-induced type-1 diabetic rats for 56 days using noninvasive echocardiographic techniques, significant reductions in diastolic performance (transmitral flow velocities and slopes) and systolic dysfunction (LV fractional shortening and cardiac output) developed in the absence of fibrosis. 63 This suggests that abnormal heart function in this model may be of metabolic rather than structural origin. A similar study was carried out to investigate the chronic effects of streptozotocin-induced diabetes on contraction in rat ventricular myocytes, which showed that time to peak contraction was significantly longer at 2 months but appeared to normalize at 10 months, and the time to half-relaxation of contraction was not significantly different after 2 months but was significantly reduced at 10 months. There was no alteration in the ultrastructure of cardiac muscle and sarcomere lengths after streptozotocin treatment, indicating that morphological defects in contractile myofilaments and associated structures do not explain contractile dysfunction seen in this model. 64 Diabetic heart disease may simply reflect increased interstitial fibrosis in the heart, because collagen accumulation occurs mainly as a result of an increase in type-III collagen in the diabetic heart. 65 Several studies have shown decreased LV function without vascular lesions 66 and no increment in abnormal function after dobutamine stress. 67 The upregulation of the local renin–angiotensin system suggests that cardiac structural and functional changes in diabetes are not the result of change in the circulating renin–angiotensin system, but are relatively specific to the heart, leading to a specific diabetic cardiomyopathy. 4
Small vessel disease
Structural abnormalities of vessels
Microangiopathy involving arterioles, capillaries, and venules and hyaline arteriosclerosis are the characteristic morphological changes in small vessels seen in diabetic myocardium. There occurs basement membrane thickening, arteriolar thickening, capillary microaneurysms, and reduced capillary density, which may be the results of periarterial fibrosis and focal subendothelial proliferation and fibrosis, possibly due to abnormal permeability of diabetic capillaries. Examination of the myocardium in diabetic animals shows that the volume of extracellular components is increased threefold and the volume of capillaries is reduced. The surface density and total surface area of capillaries were reduced, and the oxygen diffusion distance to myocyte mitochondria increased. 68 An in vivo animal study of diabetic rats also revealed numerous areas of microvascular tortuosity, focal constrictions, and microaneurysm formation, although these changes were most prominent in rats with both hypertension and diabetes. 69 The association of microvascular disease with diabetic cardiomyopathy is supported by a study in two models of congestive cardiomyopathy including the hereditary cardiomyopathic Syrian hamster and the hypertensive-diabetic rat. Histopathological study revealed microvascular spasm in both the genetic and the acquired disease models early in the disease associated with small areas of myocytolytic necrosis that undergo subsequent fibrosis. The combination of cell loss and slowly decreasing contractility resulting from the reactive hypertrophy due to a compensatory response to myocellular necrosis culminates in a cardiomyopathy. 70 Kawaguchi et al. 71 carried out a biopsy study and reported that diabetic patients had nearly normal or mildly depressed systolic LV function but significantly greater thickening of the capillary basement membrane, accumulation of toluidine blue-positive materials (i.e. materials showing metachromasia), interstitial fibrosis, and smaller myocytes (cell atrophy) compared with the control subjects, and the presence of hypertension was synergistic for these changes. This suggests that alterations in capillaries due to diabetes may lead to myocardial cell injury and interstitial fibrosis and, ultimately, to diabetic cardiomyopathy. All these features have been described in diabetic hearts, suggesting a similar disease process in the cardiac microcirculation and the presence of diffuse myocardial small vessel disease in diabetes.
In an autopsy study of three diabetic patients, both endothelial and subendothelial proliferations with fibrosis were observed in small coronary arteries. 72 A further support is given by Blumenthal et al., 73 who reported a postmortem study of intramural coronary arteries in 116 diabetic patients compared with 105 nondiabetic patients. The results showed that endothelial proliferation with interspersed peroxidase acid Schiff material was found more commonly in vessels of all sizes in diabetic patients than in those of nondiabetic patients. Small arteries and arterioles displayed hyaline thickening in 50% of diabetic patients compared with 21% of nondiabetic patients. These changes were not related to systolic hypertension. Furthermore, a biopsy study during coronary bypass surgery found capillary basement membrane thickening in diabetic patients, which was quantitatively greater in patients with overt diabetes compared with those with only glucose intolerance. 73 Despite these findings, it has been proposed that such focal changes in microvessels are insufficient to account for the diffuse myocardial degeneration with interstitial fibrosis in diabetic cardiomyopathy. Another substantial argument against the contribution of microangiopathy was shown in a study of patients with diabetes compared with control patients with hypertension, both hypertension and diabetes mellitus, and neither hypertension nor diabetes mellitus. Using vascular perfusion fixation and sampling tissue blocks in three different planes, Sunni et al. 74 showed no significant differences in the extent of small vessel disease or the density distribution of vessels of various size categories between the groups. There was no significant difference in intramyocardial arteries in diabetic cardiomyopathy and arterial lesions of diabetes compared with controls. Although most of these patients with diabetes mellitus also had myocardial infarction and the effects of large vessel ischemia may have affected any difference between the groups, there is no direct proof that microvasculopathy is an underlying cause of diabetic cardiomyopathy. In a similar study, comparing endomyocardial biopsies from seven symptom-free type-1 diabetic patients with biopsies from seven age- and sex-matched nondiabetic subjects, arteriolar hyalinization was found in three patients and arteriolar thickening was observed in five patients. Morphometry performed on electron micrographs showed no significant difference in the thickness of the capillary basal lamina between diabetic patients and controls. These findings further indicate that the abnormality of cardiac function described in diabetes is not associated with thickening of the myocardial capillary basal lamina. 66
Functional abnormalities of vessels
In both dilated cardiomyopathy and diabetes mellitus, abnormalities in coronary small vessel function occur, maximal pharmacological coronary flow reserve is reduced, and endothelium-dependent coronary vasodilation is impaired. 75 –78 Metabolic substrates or products such as adenosine play an important role in regulating microvascular tone to maintain constant coronary blood flow for a given level of metabolic demand. There was a reduction in increase in coronary blood flow induced either by pacing or inotropic agents, (to increase myocardial oxygen demand) in spontaneously diabetic rats compared with nondiabetic rats. 79 Reduced coronary flow reserve may lower the threshold for myocardial ischemia, particularly when coronary stenoses are present. Repeated episodes of myocardial ischemia, resulting from both structural and functional abnormalities in small vessels during increased myocardial demand or from microvascular spasm due to changes in calcium distribution, results in diabetic cardiomyopathy. Such a process would lead to focal cell loss due to microvascular spasm and reperfusion injury, with the subsequent development of focal fibrosis and reactive hypertrophy in response to the myocardial necrosis.
Strauer et al. 77 carried out a study using dipyridamole in diabetic patients with normal global systolic function and impaired diastolic function. They reported that maximal coronary flow to be significantly reduced and minimal coronary resistance to be increased, although there was no difference in myocardial oxygen consumption compared with controls. Another study in normotensive type-2 diabetes demonstrated that myocardial blood flow was not only significantly reduced in diabetic patients but also correlated significantly with average fasting glucose concentration and average HbA1c. 80 Similarly, in type-1 young adult diabetic patients with no or minimal microvascular complications and without any evidence of coronary heart disease, 29% reduction in myocardial blood flow and significant increase in total coronary resistance during hyperemia and consequent impairment in coronary flow reserve have been reported. 81 Another study confirmed reduction in flow reserve, which was ascribed to a significantly higher resting myocardial blood flow. 82 During atrial pacing, diabetic patients did not exhibit lactate production. 83,84 A number of other studies report that there is an association of diabetic cardiomyopathy with stenosis of small coronary arteries. 66 Apart from these, myocyte alterations have been shown to develop before the detection of vascular lesions in genetically diabetic mice. 36
Endothelial dysfunction
Commonly, in coronary vasculature of the diabetic patients, endothelial dysfunction occurs, leading to abnormal control of blood flow, and there is impairment in endothelium-dependent responses of both small and large vessels in diabetic rats. 85,86 Diabetic patients with an otherwise low likelihood of atherosclerosis also have impaired endothelium-dependent dilatation in the epicardial coronary arteries 76 and in forearm arteries. 87 Several mechanisms have been implicated in the abnormal endothelium-dependent vasodilation in diabetes. There is an increase in PKC activity in hyperglycemia, which may also play a role in the development of endothelial dysfunction in diabetes. 88 PKC activation is associated with abnormal retinal and renal haemodynamics in diabetic animals, and overexpression of the β-isoform in myocardium is associated with cardiac hypertrophy and failure, 89 implying that this may play a role in the development of diabetic cardiomyopathy by affecting vascular cells. The nitric oxide activity is reduced partly due to the accumulation of glycosylation end products 90 and partly due to increased oxidative stress. 91 –94 Tesfamariam et al. 95 have reported that the synthesis of vasoconstrictor prostanoids by the endothelium increases, and hence the vasoconstriction is enhanced in diabetic subjects.
Cardiac autonomic neuropathy
Diabetic cardiomyopathy is also associated with CAN. There is a change in sympathetic innervation in the diabetic heart leading to alterations in catecholamine levels and adrenergic receptors in the myocardium. There is a significantly increased cardiac norepinephrine content and β-adrenergic receptor density in short-term diabetic patients and these changes precede both the development of cardiac hypertrophy and the enhanced adenyl cyclase activity. However, as the diabetic state develops, cardiac norepinephrine content, β-adrenergic receptor density, and adenylyl cyclase activity returned to control levels. 96 In streptozotocin-induced diabetic rats, ventricular norepinephrine levels were increased after 1 and 2 months of diabetes, but were at or below control levels after 4 months of diabetes. Histofluorescence studies demonstrated that the density of noradrenergic varicosities in diabetic rat hearts appeared to be increased, with abundant branched profiles after 1 month of diabetes. 97 The reason for the increased norepinephrine in the early stages of diabetes can attributed to increased bradykinin-induced release of norepinephrine, which has been shown to be four times greater in diabetic than in normal preparations, 98 as well as the acute effects of high glucose levels on sympathetic activity. 99 Furthermore, it is reported in several studies that the plasma noradrenaline level is reduced in diabetic patients. Kondo et al. 100 carried out a study in 10 type-2 diabetic and eight control inpatients, in which blood for catecholamine measurement was collected every 4 hours, and the mean obtained for 24-hours. The plasma noradrenaline level in diabetic patients was significantly lower than that in controls. In contrast, no significant difference in adrenaline levels was observed. A similar study in diabetic subjects showed lower arterial levels of noradrenaline in diabetic subjects compared with control subjects during exercise but similar disappearance rates after exercise, indicating lower release of noradrenaline in diabetic patients. 101 These data suggest that alterations in cardiac sympathetic activity during the early stage of diabetes enhance the cardiac β-adrenergic system, which may induce toxic effects on the heart. Norepinephrine has been shown to induce apoptosis in cultured neonatal rat myocytes 102 –104 via the formation of reactive oxygen species, 105 –107 despite a decrease in the severity of the cardiac necrosis induced by the administration of isoproterenol in diabetes. 108 Similar results were also demonstrated in ferrets receiving chronic norepinephrine. 109 However, the activation of apoptosis is dependent on the type of adrenergic receptors stimulated. In vitro pharmacological studies of cardiac myocytes demonstrate that stimulation of β1-adrenergic receptor induces apoptosis that is cyclic adenosine monophosphate-dependent and involves the voltage-dependent calcium influx channel. Overexpression of β1-adrenergic receptors causes marked myocyte hypertrophy, interstitial fibrosis, and reduced contractile function, which was accompanied by increased myocyte apoptosis. 110 On the contrary, an antiapoptotic effect is exerted by the stimulation of β2-adrenergic receptor, which appears to be mediated by a pertussis toxin-sensitive G-protein. Stimulation of α1-adrenergic receptors causes myocyte hypertrophy and may exert an antiapoptotic action. 111 A study, by Irlbeck and Zimmer 112 using phenylephrine or isoproterenol in streptozotocin-induced diabetic rats has demonstrated that the in vivo response to β-adrenoceptor stimulation is well preserved, whereas the effects of α-stimulation are markedly reduced, especially in the LV and systemic circulation, suggesting that the antiapoptotic effect may be also reduced in diabetes.
There is an association of autonomic dysfunction with abnormal cardiac function in diabetes. In the study by Erbas et al., 113 20 type-1 diabetic patients who were clinically free of cardiovascular disease and had normal LV systolic function, ratio of mean peak velocity of early and late atrial mitral flow of diabetic patients with CAN and without CAN were significantly lower than those of controls, and the CAN score correlated with worsening LV relaxation. In another study of 38 type-1 diabetes patients, 56% of patients were found to have CAN and 12% had LV diastolic dysfunction; none had LV systolic dysfunction. All diabetic patients with LV diastolic dysfunction had evidence of CAN, and there was no correlation between LV dysfunction and microvascular complications of diabetes mellitus. 114 A similar correlation of indices of LV diastolic filling to CAN was shown by Kahn et al. 115 in 28 patients with type-1 diabetes without the evidence of ischemic heart disease. In several different studies of diabetic patients, myocardial contractility responses to stress have also been shown to be affected by CAN. Erbas et al. 116 demonstrated the effect of autonomic dysfunction on both LV systolic and diastolic dysfunctions using radionuclide ventriculography in a study of 20 diabetic patients at rest and during handgrip exercise. The results showed that diastolic dysfunction was frequently present at rest, and systolic dysfunction became evident during exercise in patients with CAN. 116 In another study, although baseline myocardial contractility was normal, an abnormal response of LV ejection fraction to isometric (9 of 14 patients) or to dynamic (8 of 14 patients) exercise was found in 14 diabetic patients with autonomic dysfunction and without ischemic heart disease based on exercise stress echo and coronary angiography. The abnormal ejection fraction at peak handgrip was completely reversed by postextrasystolic potentiation (a potent inotropic stimulation independent of the integrity of adrenergic cardiac receptors), suggesting that defective inotropic recruitment plays an important role in LV dysfunction in diabetic patients with CAN during exercise. 117 In a study of 24 patients with type-1 diabetes without CAD excluded by 201Tl scintigraphy compared with 10 controls, cardiac innervation was evaluated by both tomographic imaging and cardiovascular reflex tests. LV systolic (ejection fraction) and diastolic (peak filling rate) functions were determined by equilibrium radionuclide angiography at rest and during bicycle exercise. All control and six diabetic patients exhibited a normal myocardial distribution, and 18 diabetic patients had evidence of regional adrenergic denervation. All patients had a normal ejection fraction at rest. However, patients with regional adrenergic denervation showed an impaired response to exercise as indicated by a smaller increase in ejection fraction and a lower peak filling rate, indicating that subclinical LV dysfunction is related to derangements of adrenergic cardiac innervation. 118
A pharmacological stress study has demonstrated the adverse effect of CAN on myocardial perfusion. Dynamic contrast-enhanced magnetic resonance perfusion imaging was performed during baseline conditions and after dipyridamole-induced vasodilatation in nine type-1 diabetic patients with CAN, 10 type-1 diabetic patients without CAN, and 10 healthy control subjects. The study showed that the myocardial perfusion index was significantly lower in the patients with CAN than in the other groups during dipyridamole vasodilatation despite similar baseline myocardial perfusion index in the three groups and blood pressure was found to be significantly decreased in only the patients with CAN. There was a significant correlation between blood pressure response to dipyridamole and myocardial perfusion reserve index. The decreased myocardial perfusion reserve capacity during dipyridamole vasodilatation may be caused by defective myocardial sympathetic function to maintain blood pressure during vasodilatation. 119 Thus, there is a strong relationship between abnormal response to exercise in the early phase of diabetic cardiomyopathy and an impairment of cardiac sympathetic innervation. 120 However, increments in catecholamine level in early diabetes may mask cardiac dysfunction. In such an in vivo longitudinal study, carried out by Hoit et al., 121 the time course of development of cardiac dysfunction in streptozotocin-induced diabetic rats was examined, overt and covert contractile dysfunctions of the myocardium unmasked by isoproterenol began at 5 weeks of diabetes, and the overt LV systolic and diastolic dysfunctions were fully manifest after 6 week of diabetes. An outline of pathophysiological mechanisms of diabetic cardiomyopathy is given in Table 3.
Outline of pathophysiological mechanisms of diabetic cardiomyopathy

RAAS: Renin Angiotensin Aldosterone System; ACE: angiotensin converting enzyme; α-MHC: α-myosin heavy chain; IGF-I: insulin-like growth factor-I; AT II: angiotensin II.
Functional changes in diabetes
Functional changes do occur in diabetic patients independent of hypertension, CAD, or any other known cardiac disease. These alterations can involve either the diastolic or systolic functions of the heart or both. The inter-relationship between diabetes, hypertension, atherosclerosis, and heart failure is given in Figure 2.

Inter-relationship between diabetes, hypertension, atherosclerosis, and heart failure.
Diastolic dysfunction in diabetic patients
Changes in diastolic function have been widely reported in diabetic patients without the evidence of heart disease caused by other factors. 122,123 In experimental diabetes, papillary muscles from animal hearts have shown prolongation of relaxation and considerable slowing in relaxation velocity, 25,124 and isolated perfused hearts from type-2 diabetic rats showed prolonged isovolumic relaxation time and increases in late mitral inflow velocity and LV end-diastolic pressure. 92 In an in vivo animal study with prodromal type-2 diabetes characterized by postprandial hyperglycemia and hyperinsulinemia, 54 OLETF rats with normal average fasting serum glucose and without premature atherosclerosis and hypertension demonstrated prolonged deceleration time and reduced peak velocity of early filling, 59 which represent an early manifestation of abnormal LV diastolic function. A similar study of 30 male diabetic and 30 male control rats showed significant differences in early to late diastolic mitral inflow velocity ratio and isovolumic relaxation time, but not in shortening fraction, deceleration time, and myocardial collagen content. These findings suggest that the presence of diastolic dysfunction in diabetic hearts may relate to uncoupling of the contractile apparatus (which drives early relaxation), without concomitant increases in chamber stiffness (which produces more late diastolic changes). 125 Furthermore, isoproterenol administration into the hearts of 4-week-old diabetic rats reduced the peak rate of relaxation, although the rate of contraction increased normally. 126
The LV ejection time is often reduced, and the length of the pre-ejection period and the ratio of pre-ejection period to LV ejection time are often increased. 4 Diastolic inflow patterns are frequently abnormal, reflecting underlying abnormalities in relaxation, and/or reduced myocardial compliance. In 46 well-controlled type-2 diabetic patients who had no evidence of diabetic complications, hypertension, CAD, CHF, or overt thyroid or renal disease, and no overt systolic dysfunction, LV diastolic dysfunction was present in 28 subjects (60%), of whom 13 (28%) had a pseudonormal filling pattern (reflecting raised filling pressure), and 15 (32%) had impaired relaxation (a milder form of diastolic dysfunction). 127 Echocardiographic examination has made it easier to detect subtle abnormalities in LV diastolic dysfunction before its clinical appearance. Schannwell et al. 128 examined 87 young type-1 diabetic patients and demonstrated reduced early peak mitral velocity, increased late peak mitral velocity, and prolonged deceleration time and isovolumeic relaxation time, despite having normal LV dimensions and systolic function. Newer techniques like tissue doppler imaging have confirmed these findings. 129 Studies suggest that the patients with type-2 diabetes are more likely to have diastolic dysfunction than type-1 diabetic patients. In 20 type-1 and 10 type-2 diabetic patients, ventricular filling was impaired more significantly in the latter group of patients. 130
Systolic dysfunction in diabetic patients
Animal studies have shown diabetes to be associated also with systolic dysfunction. 92,121,131 Similar findings were reported in intact animals; heart rate, systolic blood pressure, and fractional shortening were significantly reduced in diabetic animals compared with control animals. 132 In murine isolated papillary muscle preparations, systolic LV pressure was reduced by 15%, and active force was reduced by 61%. 25 These changes take some time to develop; systolic function was unchanged in 6-week-old db/db mice, but fractional shortening and velocity of circumferential fibre shortening were reduced in 12-week-old db/db mice relative to db/+ control mice. 13 These studies suggest that diabetes is the cause of systolic dysfunction.
Several epidemiological and clinical studies have shown diabetes to be associated with systolic dysfunction also. There is a significant association of idiopathic dilated cardiomyopathy with diabetes mellitus. 133 In a study of 40 type-2 diabetic patients, 22 (55%) patients had systolic dysfunction, but only 3 (7.5%) patients had electrocardiogram changes compatible with cardiac ischaemia; 16 (40%) patients were also found to have LV hypertrophy. 134 Many diabetic patients may have normal LV systolic function at rest with abnormal systolic function only during exercise or dobutamine stress. In 30 diabetic men with normal resting LV ejection fraction and without coronary or any other cardiovascular disease, LV ejection fraction deceased after exercise in 5 of 30 (17%) diabetic patients, remained unchanged in 8 (27%) patients, and increased normally in only 17 patients. 135 Although many studies have shown that diabetic patients have abnormal diastolic dysfunction but preserved systolic function, this may well be due to techniques used for systolic function evaluation. Techniques utilized for systolic function evaluation are less sensitive than those used for the assessment of diastolic dysfunction. The parameters of peak strain, strain rate, and calibrated integrated backscatter were determined echocardiographically in 186 patients who had normal ejection fraction and no evidence of CAD. 63 Forty-eight patients had diabetes mellitus (DM group), 45 patients had LV hypertrophy (LVH group) only, 45 patients had diabetes and LVH (DH group), and there were 48 controls. All patient groups (DM, DH, and LVH groups) showed reduced LV systolic function, compared with controls as evidenced by lower peak strain (p < 0.001) and strain rate (p = 0.005). Calibrated integrated backscatter, which signifies myocardial reflectivity, was greater in each patient group than in controls (p < 0.05). Peak strain and strain rate were significantly lower in the DH group than in the DM (p < 0.03) or LVH (p = 0.01) groups. Diabetic patients who did not have overt heart disease demonstrated evidences of LV systolic dysfunction and increased myocardial reflectivity. Although the changes were similar to those that were caused by LVH, they were independent and incremental to the effects of LVH.
Structural changes in diabetes
A number of studies have shown structural changes in diabetic hearts in the absence of hypertension, CAD, and valvular heart diseases. The conspicuous histopathological findings are fibrosis, which may be perivascular, interstitial, or both. As the disease progresses, there is increased myocyte loss and replacement fibrosis. In an experimental study with 54 OLETF (type-2) diabetic rats, which show mild obesity, postprandial hyperglycemia, and hyperinsulinemia, low peak velocity of early diastolic transmitral inflow and prolonged deceleration time were associated with extracellular fibrosis and abundant TGF-β1 receptor II in LV myocytes. At 15 weeks of age, the ratio of collagen area/visual field of LV wall in OLETF rats was greater than that in nondiabetic rats, and the collagen content/dry tissue weight ratio of the heart was significantly increased in OLETF rats compared with control rats. 57 These results indicate LV fibrosis in the early stages of type-2 diabetes. In another study using modern stereological techniques to quantify changes in the morphology accompanying streptozotocin-induced diabetes, the results showed that the time to peak tension and relaxation of papillary muscles was prolonged, the heart weight to body weight ratio was increased, and the volume of extracellular components was increased threefold in diabetic rats. At the same time, this study also demonstrated that the volume, surface density, and total surface area of capillaries as well as volume fraction of myocyte mitochondria were reduced, and oxygen diffusion distance to myocyte mitochondria was increased in the diabetic animals. 68 Other studies have identified ultrastructural changes in diabetic hearts. 136,137 More recently, the 2D Haar wavelet decomposition method has been used as a tool to identify textural changes in diabetic rats, which showed increased texture energy compared with controls. These changes were detected before development of echocardiographic structural changes. 138
In a study by Nunoda et al. 62 endomyocardial biopsies were obtained from right ventricular myocardium. The mean diameter of right ventricles myocardial cell has been shown to be significantly larger and the percentage of interstitial fibrosis in diabetic patients is significantly greater than controls. Fibrosis in diabetic hearts has been quantified using new techniques such as the assessment of ultrasonic backscatter, which is directly related to collagen content. In a study of 26 asymptomatic type-1 diabetic patients without hypertension or CAD, Di Bello et al. 139 have shown that integrated backscatter in the septum and posterior wall was significantly higher in diabetic patients than in controls. This increased myocardial acoustic reflectivity is due to augmentation of the connective tissue of the myocardium. Collagen is a primary determinant of echocardiographic scattering in myocardial tissues and there is a linear relationship between collagen deposition and backscatter magnitude. 140 Positive associations have been found between heart weight and total fibrosis with the semiquantitative scale in patients with diabetes alone and with both hypertension and diabetes. 141 The increased myocardial tissue reflectivity in diabetic patients may represent an early marker of diabetic cardiomyopathy. 4
Correlation of structural changes to LV dysfunction
The functional abnormality in diabetic myocardium is considered to be associated with myocardial structural changes, and indeed, these structural changes might play a role in progressive deterioration of cardiac haemodynamics.
Experimental data strongly support the connection between structural changes and heart muscle dysfunction in diabetes. After 2 months of streptozotocin-induced diabetes, in vitro study of myocytes showed a 30% increase in time to peak shortening, which corresponded to a significant reduction in resting sarcomere length and a change in the microtubular cytoskeleton, 142 suggesting that the myocardial structural change may be the basis for cardiac dysfunction. Another study showed that rats with streptozotocin-induced noninsulin-dependent diabetes had prolonged isovolumic relaxation time, elevated LV end-diastolic pressure, and increased chamber stiffness; these functional changes were accompanied with increased LV mass. 92 A similar experimental study in animals also showed that functional changes (e.g. reduced LV compliance) after 1 year of diabetes were associated with increased interstitial connective tissue. 37 A clear relationship between functional and structural changes is indicated by a study showing that diabetic rats exhibited prolonged deceleration time and low peak velocity of early diastolic transmitral flow, which is associated with extracellular fibrosis in LV myocytes, and higher ratio of collagen area/visual field of LV wall and ratio of collagen content/dry heart weight compared with control rats. 57
Abnormal systolic and diastolic function is present in many diabetic patients, particularly in the presence of hypertension and myocardial hypertrophy and fibrosis are commonly present in these patients. A correlation between histological and clinical features in a study of endomyocardial biopsies in 16 diabetic patients, with myocardial changes more pronounced in the symptomatic group and less so in asymptomatic patients has been reported. 143 This suggests that myocardial dysfunction in diabetic patients might be secondary to the accumulation of glycoprotein within the interstitium together with mild interstitial fibrosis. There is increased myocardial fibrosis in diabetic patients, particularly in those with cardiomegaly, suggesting that changes in cardiac interstitial collagen might increase myocardial wall stiffness which is usually associated with functional changes. 144
Systolic dysfunction may be more dependent on the degree of myocyte loss and myocyte injury, which may impair the ability of the myocardium to develop force, and thereby resulting into reduced contractility, decreased pump function, and ejection fraction. Abnormal LV systolic function in diabetic patients may be transient, reversible, and related to changes in diabetic control within a certain range and need not indicate structural myocardial disease. 145 The development of systolic dysfunction during exercise in some patients may reflect loss of contractile reserve related to limited myocyte loss, insufficient to influence resting function.
Diastolic dysfunction is a result of both accumulation of collagen and myocyte injury in the heart, and so there is greater prevalence of diastolic dysfunction in type-2 diabetes. In type-2 diabetes, aging-related increments in cardiac collagen are likely additive, although less satisfactory glycemic control may be an important factor as well. Miric et al. 146 showed that there is reversal of cardiac fibrosis by short-term pirfenidone and spironolactone treatment and attenuation of increased diastolic stiffness without normalizing cardiac contractility in streptozotocin-induced diabetic rats. However, myocyte injury does affect diastolic function and diabetes mellitus can produce a stiff myocardium before the development of myocardial fibrosis due to the formation of advanced glycosylation end products. 147 At an early stage of diabetes, the alterations in myocardial structure are usually small, and these may be mainly related to myocyte injury, which may be reversible or partially reversible. As diabetes progresses, accumulation of collagen becomes obvious and may play a major role in the development of diastolic dysfunction. These chronic alterations are believed to result from repeated acute cardiac responses to suddenly increased glucose levels at the earlier stage of diabetes. 4
Conclusions
Diabetic cardiomyopathy is a distinct clinical entity and patients with diabetes who develop heart failure experience an exceptionally poor prognosis. Diabetic cardiomyopathy encompasses the spectrum from subclinical disease to full-blown syndrome of CHF. Clinically, it presents as systolic or diastolic dysfunction. Traditional cardiac risks such as hypertension, atherosclerosis, and dyslipidemia are common in diabetic patients and further compromise cardiac status. Although the pathophysiological mechanism like metabolic disturbances, interstitial fibrosis, cardiomyocyte loss, small vessel disease, and CAN have been identified, there is lack of consensus on how to diagnose and monitor this condition. Despite this, with the advancements in the molecular technologies, detailed subcellular mechanisms of CV complications of diabetes are being identified. The future holds the promise of providing advanced diagnostic methods and more precise therapeutics to prevent the progression of the disease.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.