
Abstract
The synthetic catecholamine isoprenaline (ISO) has been used as an inductor in the acute myocardial infarction model for more than a half century. Despite the fact that many articles were published on this topic, precise early haemodynamic pathology remains unknown. Acute haemodynamic changes were measured in rats; first, in preliminary experiments by the thermodilution method; and second, in main experiments continuously for 2 h using a Millar catheter. Animals received saline or ISO in the cardiotoxic dose (100 mg/kg, subcutaneously). Also, additional experiments were performed with salbutamol in order to evaluate the role of β2-receptors. ISO caused a rapid, within 1 min, approximately 40% decrease in arterial blood pressures, 30% increase in the heart rate, and 30% decrease in the stroke volume. Within the first 2 min, the changes were followed by decreases in afterload (−40%), preload (−10%), diastolic relaxation (−50%), diastolic filling (−40%), and a marked, but short-term, increase in the left ventricle contractility (+100%). Ejection fraction did not significantly change, suggesting diastolic dysfunction. Salbutamol, with the exception of diastolic pressure and afterload, did not substantially influence other parameters. In conclusion, this study demonstrated that diastolic dysfunction precedes systolic dysfunction and β2-receptor stimulation alone is not sufficient for an early induction of diastolic dysfunction.
Introduction
Endogenous catecholamines, adrenaline and noradrenaline, are the essential components of the sympathetic nervous system, which are responsible for maintaining the cardiovascular homeostasis. However, catecholamines are cardiotoxic under certain circumstances and thus may contribute to additional cardiac impairments. The known examples are chronic heart failure, stress cardiomyopathy, arrhythmias, and acute myocardial infarction (AMI). 1 –4 Infarctions may be triggered by catecholamines themselves, and it is the base for the experimental use of catecholamines as a model of AMI. 5,6 Interestingly, a synthetic catecholamine isoprenaline (ISO) with nonselective β-adrenergic agonistic activity has demonstrated a superior activity in mimicking the AMI in laboratory animals in comparison with that of endogenous catecholamines. 5 Although the haemodynamic effects of therapeutic doses of ISO are well known, the precise pathophysiology of the ISO model of AMI, in which doses of ISO are much larger, is not known. This model has been used for more than a half century notwithstanding. Additionally, the reason for ISO superiority in the induction of AMI over the endogenous catecholamines is also unknown.
Current knowledge emphasizes that both β-adrenergic receptor and catecholamines redox cycling (including the production of a row of their oxidation products and production of reactive oxygen species) are involved in the pathophysiology of catecholamine-induced cardiac impairment. 4,7,8 Although oxidative stress is important, the first event in the pathophysiology represents the overstimulation of both β-adrenergic receptors in the cardiovascular system. It leads to marked stimulation of the myocardium having positive inotropic, chronotropic, and dromotropic effects due to the activation β1-receptors. Also, it causes a decrease in total peripheral resistance (TPR) as a consequence of the stimulation of β2-receptors. In the therapeutic doses of ISO, the stimulation of β-receptors leads to an increase in cardiac output together with the reinforcement of myocardial contractility and improvement in the myocardial relaxation. 9,10 Interestingly, the consequences of the cardiotoxic doses are quite the opposite, that is they cause decreases in cardiac output and stroke volume. The decreases are associated with impaired systolic and diastolic functions. 11 –13 Although lots of data have been published on the biochemical and histological findings regarding the cardiotoxic doses of ISO, the early haemodynamic processes in the cardiovascular system, which cause a drop in the stroke volume remain unclear. Therefore, this study was aimed at detailed analysis of haemodynamic changes, in particular contractility and diastolic function, after the administration of cardiotoxic doses of ISO. Additionally, we investigated the involvement of β2-receptors in the cardiac injury.
Materials and methods
Animals
Totally 35 Wistar:Han male rats were obtained from Biotest s.r.o. (Czech Republic). The rats were housed in cages located in a special air-conditioned room with a periodic light–dark cycle for 2 weeks. During this period, the rats were provided with free access to tap water and standard pellet diet for rodents. After the acclimatization period, the healthy rats weighing approximately 370 g were used for the experiments described below.
The study was performed under the supervision of the Ethical Committee of Charles University in Prague, Faculty of Pharmacy in Hradec Králové, and it conforms to The Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85-23, revised 1996).
Anaesthesia
After 12 h of fasting, the rats were anaesthetized with intraperitoneal injection containing aqueous solution of urethane (Sigma-Aldrich, USA) at a dose of 1.2 g/kg.
Haemodynamic study by thermodilution method
A polyethylene catheter (0.5/1.0 mm filled with heparinised saline 50 IU/ml) was inserted into the right internal jugular vein for injection of the indicator (saline). Its temperature was approximately 10°C. A thermocatheter (outer diameter 0.8 mm) was introduced through the common left carotid artery into the aortic arch. Another polyethylene catheter filled with heparinised saline was inserted into the left common iliac artery. The catheter was connected to the blood pressure transducer BPR-01. Both the transducer and thermocatheter were linked to the apparatus for the measurement of haemodynamic variables Cardiosys equipped with Cardiosys 1.1. software (Experimetria Ltd, Hungary) using a thermodilution transpulmonary method according to the Stewart-Hamilton principle. 14
Haemodynamic study by pressure–volume recording using a micromanometer catheter
The left common iliac artery was connected to a pressure transducer MLT0380/D (AdInstruments, Australia) via a polyethylene catheter (0.5/1.0 mm filled with heparinised saline 50 IU/ml). A high-fidelity pressure–volume micromanometer catheter (Millar pressure–volume catheter SPR-838 2F, 4E, 9 mm, Millar Instruments Inc., USA) was inserted into the left heart ventricle through the right common carotid artery. Both pressure transducer and Millar pressure–volume catheter with the subcutaneous electrodes of the electrocardiography (ECG) standard limb lead II MLA1215 (AdInstruments, Australia) were connected to PowerLab with LabChart 7 software (AdInstruments, Australia).
Drug administration and measurement
The healthy Wistar:Han male rats were randomly divided into groups. All of them were of statistically similar average weight.
Thermodilution method
Following 15 min of equilibration, 10 rats received isoprenaline (Sigma-Aldrich, USA) in the dose equal to 100 mg/kg subcutaneously (sc). Cardiac output and derived parameters were measured by the administration of 100 μl of cold saline 14 in the following time intervals—0 (baseline level), 5, 10, 15, 20, 25, 30, 40, 50, 60, 75, 90, 105, 120, 150, 180, and 240 min.
Pressure–volume recording using a micromanometer catheter
Following 15-min of equilibration, the calibration of parallel volume necessary for the estimation of real blood volume in the left ventricle was performed using 20 µl of 25% w/w natrium chloride solution with 900 IU/ml of heparin—the hypertonic saline calibration. 15 Five minutes after calibration, 15 rats received ISO (100 mg/kg sc—the same dose as in the previous setting) or salbutamol hemisulphate sc (5 rats, Sigma-Aldrich, USA) in the equimolar dose of ISO (116 mg/kg sc) or the solvent—control group (5 rats, 2 ml/kg of saline sc, Braun, Germany). Haemodynamic as well as ECG monitoring continued for 2 h after the administration of drug/drugs. After 2 h, an additional hypertonic saline calibration was performed. At the end of the experiment, a blood sample was collected from the abdominal aorta into the heparinised test tube (170 IU/10 ml) and conductance signal was calibrated using cuvettes of known volumes. 16
Following the experiment, all surviving animals were killed painlessly using intravenous administration of 1 ml 1 M aqueous solution of potassium chloride (Sigma-Aldrich, USA).
Calculation of parameters
The Millar catheter records two electrical signals: the first one for pressure and the second one for conductance/volume. The pressure electrical output signal varies proportionally with changes in pressure; therefore, a simple internal calibration was performed in each experiment in order to obtain the precise intraventricular pressure values. However, the conductance signal is not directly transformable in the intraventricular blood volume. It depends on more factors (equation (1))
15
:

where G(t) is the measured conductivity, α is the dimensionless constant, σ b is the specific blood conductivity, L is the distance between electrodes, V t is the actual blood volume in the left ventricle and G p is the so-called parallel conductance, which reflects the electrical field of the surrounding tissues (e.g. left ventricular wall, right ventricle, and lung tissue). Therefore, two calibrations are necessary in order to obtain the precise volume of blood in the left ventricle, the first one is the above mentioned hypertonic saline calibration (for the assessment of parallel conductance) and the second one is the cuvette calibration (for the assessment of σ b). Details can be found in references 15 and 16 . Thus, the conductance signal without repeated calibrations can be very easily influenced by many factors. In particular, changes in blood viscosity and parallel tissue conductivity were relevant in our experiments. Therefore, the volume signal was calibrated at the beginning and end of each experiment, and stroke volume and related parameters data were reliable during the first 15 min of the experiment. Changes at the end of the experiment (2 h) were only approximate because it was not possible to carry out the cuvette calibration during this experiment.
TPR was calculated as mean arterial blood pressure divided by the cardiac output. Left ventricular dP/dt max (maximal pressure rise in the isovolumic phase in the left ventricle) divided by left ventricular end-diastolic volume (LVEDV) was designated as (dP/dt max)/V and dP/dt max divided by instantaneous pressure at this maximum as (dP/dt max)/p. Other parameters had the common meaning. Tau (the time constant of left ventricular isovolumic pressure decay) was calculated by Weiss method. 17
Data analysis
Data are expressed as means ± SEM. In the case of thermodilution method, differences versus baseline values (i.e. before drug administration) were compared by means of Student’s paired T test. Differences between groups (pressure–volume recording) were analysed by one-way analysis of variance (ANOVA) followed by Bonferroni’s multiple comparison test. Outliers were excluded by Grubb’s test. Statistical software GraphPad Prism 5 for Windows (GraphPad Software, USA) was used for all statistical analysis. Differences between groups were considered significant at p ≤ 0.05, unless otherwise indicated.
Results
Thermodilution method
ISO as a nonselective β-receptor agonist is expected to cause vasodilation and acceleration in the heart rate. Indeed, a rapid increase in the heart rate and a decrease in both systolic and diastolic blood pressures were documented after ISO administration. 18 We observed similar changes in the heart rate and blood pressure (for details see Supplementary Figure S1). These changes were accompanied by decreases in stroke volume and TPR (Figure 1). All mentioned variables changed at the first stroke volume measurement (5 min after ISO administration) and remained mostly at the same level during the whole experiment (4 h). Of the 10 animals, 4 died within the first 70 min and were not included in the analysis.

Arterial blood pressures (A) and the heart rate (B) after subcutaneous (sc) administration of 100 mg/kg isoprenaline (ISO) measured by the thermodilution method. Changes and statistical significance were calculated versus baseline levels before ISO administration. Changes in heart rate were significant at p < 0.01 from the first measurement at fifth minute and blood pressures were significant at p < 0.001 from the first measurement at the fifth minute.

The stroke volume (a) and total peripheral resistance (b) after subcutaneous (sc) administration of 100 mg/kg isoprenaline (ISO) measured by the thermodilution method. Changes in the measured parameters and statistical significance were calculated versus baseline levels (at time 0, i.e. before ISO administration); *p < 0.05.
Pressure–volume recording
In order to characterize the ISO-induced cardiovascular effects in detail, we continuously analysed the ISO-treated animals using the Millar catheter. This approach enables continuous measurements in contrast to the thermodilution method, but (1) it is more invasive and therefore it enables only shorter experiments (in case of ISO up to 2 h); (2) it requires repeated calibration in pathologically changing myocardium for a precise measurement of intraventricular blood volume and derived parameters (for more details see ‘Parameters calculation’ and ‘Discussion’ sections).
Changes in the heart rate and blood pressures after ISO administration shown in the preceding section were confirmed. In addition, the changes were rapid and significant already 30 s after sc administration of ISO (Figure 2(a) and (b)). Diastolic and systolic blood pressures followed the same pattern. Stroke volume decreased as well, but the decrease started approximately 5–10 s after changes occurred in the blood pressure and the heart rate (see Supplementary Figure S2).

Arterial diastolic (A), systolic (B) blood pressures, (C) and stroke volume after the application of 100 mg/kg isoprenaline (ISO; red), salbutamol (green) and saline (blue)—the Millar catheter-based method. Statistical significance: is: ISO versus salbutamol at p < 0.05; ic: ISO versus control at p < 0.05; cs: salbutamol versus control at p < 0.05.

Basic haemodynamic parameters. The mean arterial blood pressure (a), the heart rate (b), and the ejection fraction (c) after the administration of isoprenaline (ISO; black), salbutamol (dark grey), and saline (grey). Statistical significance at p < 0.05: is: ISO versus salbutamol; ic: ISO versus control; cs: salbutamol versus control.
To investigate the cause of the fall in stroke volume, we analysed ejection fraction, parameters of loading conditions (preload and afterload), and systolic and diastolic functions. There was no significant change in ejection fraction (Figure 2(c)) between controls and ISO-treated group; ISO tended to increase ejection fraction, suggesting that the responsible factor may be an impaired diastolic function.
As loading conditions may influence the assessment of systolic and diastolic functions, we first determined the loading condition parameters. The extent of preload can be deduced from the left ventricular end-diastolic pressure (LVEDP). 19 ISO caused a rapid, but relatively mild (10%) and short-term, decrease in this parameter (Figure 3(a)). After 5 min, the differences were not significant. The assessment of afterload was accomplished by the assessment of TPR. A marked 40% drop in TPR was found after the administration of ISO (Figure 3(b)).

Parameters of preload, afterload and contractility. The left ventricular end-diastolic pressure (a), the total peripheral resistance (b), and the parameter dP/dt max (c) after administration of isoprenaline (ISO; black), salbutamol (dark grey), and saline (grey). Statistical significance at p < 0.05: is: ISO versus salbutamol; ic: ISO versus control; cs: salbutamol versus control.
As loading conditions were apparently changing, the sensitivity of contractility (systolic) parameters were enhanced by minimizing the preload influences ((dP/dt max)/V) or by reducing afterload influences ((dP/dt max)/p). 20 Nevertheless, both the derived parameters showed qualitatively similar kinetics as the nonderived dP/dt max (Figure 3(c) and Supplementary data Figure S3). It suggests that the loading conditions could not be considered as the main factor of contractility changes. Contractility increased approximately to 100% of baseline value at 25 s after ISO administration. Although this contractility peak was only transitive, dP/dt max remained rather elevated for the rest of the experiment.
Diastole has two distinctive phases, the isovolumetric relaxation and the filling phase. The former one can be characterized by peak negative dP/dt. As this parameter is also influenced by loading conditions, we verified these results by the assessment of tau which is less affected by these parameters. 17,21 Both parameters gave similar outcome; however, the tau interindividual and intraindividual variability in the ISO group was very high and some cardiac cycles could not be quantified by use of the tau (data not shown). Hence, we present the relaxation data as peak negative dP/dt (Figure 4(a)). Relaxation indicated marked 50% depression of the baseline value within the first minute of ISO administration. It remained there for the whole 2 h of the experiment. The filling phase can be characterized by maximal volume rise dV/dt max (Figure 4(b)). Once again, this phase appeared to be depressed and it reached its maximal decrease (40%) within the first 2 min. After the initial decrease, marked variability in the parameter was observed.
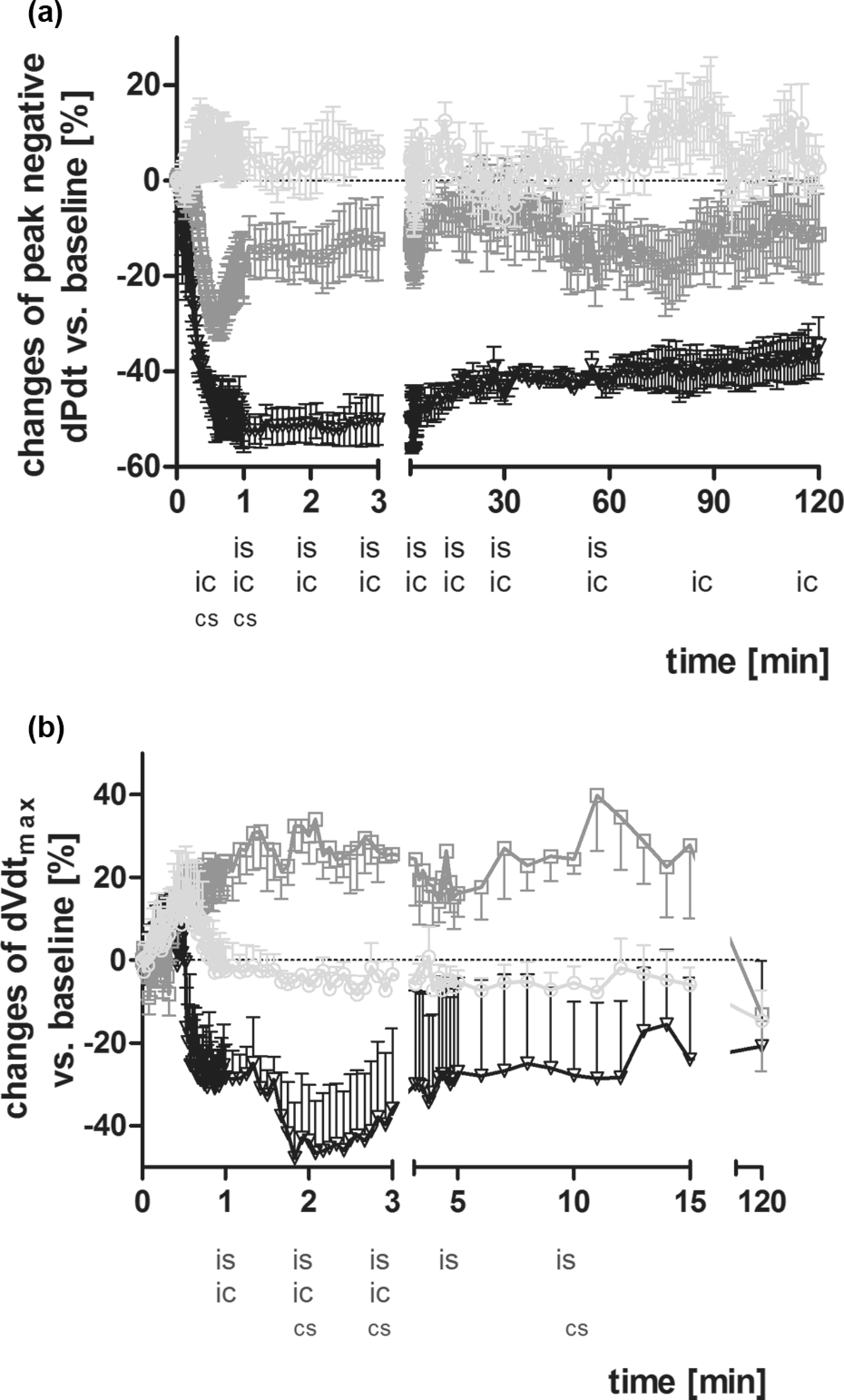
Parameters of left ventricular diastolic function. Peak negative dP/dt (a parameter of left ventricular isovolumetric relaxation) (a) and dV/dt max (maximal volume rise in the left ventricular diastolic filling phase) (b) after administration of isoprenaline (ISO; black), salbutamol (dark grey), and saline (grey). Statistical significance at p < 0.05: is: ISO versus salbutamol; ic: ISO versus control; cs: salbutamol versus control.
During the course of the experiment, marked ECG modifications were recorded (e.g. ST-elevation/depression, T amplitude rise, and P-R interval prolongation) in ISO-treated animals. Of the 15 ISO-treated animals, 7 died. The deaths were caused by serious dysrhythmias that started by ventricular extrasystoles and in most cases were followed by atrioventricular block of various degrees, polymorphic ventricular tachycardia, and/or ventricular fibrillation, which led to death. No mortality was observed in the controls.
To reveal the role of individual β-adrenergic receptor subtypes in ISO-induced cardiotoxicity, we performed additional experiments with the selective β2-agonist salbutamol. In contrast to ISO, salbutamol caused only a slight and very slow increase in the heart rate and no rapid change in the stroke volume (Figure 2(b), Supplementary data Figure S2). Blood pressures, as in the animals-treated with ISO, dropped very rapidly, but the decrease (around 20%) did not reach the ISO effect (more than 40%) within the first 30 min (Figure 2(a)). After 30 min, there were no significant changes between ISO and salbutamol (about a 40% decrease in both agents). Concordantly to the stroke volume data, salbutamol decreased more diastolic blood pressure than the systolic one (in case of ISO, both pressures dropped in similar manner, see Supplementary data Figure S2). Salbutamol, in contrast to ISO, apparently did not influence preload (Figure 3(a)), but there were mostly no significant differences between ISO and salbutamol in TPR (Figure 3(b)). These results collectively imply that TPR was decreased to a similar extent by both drugs due to the activation of β2-adrenergic receptors.
Concerning the left intrinsic ventricular contractility and relaxation (Figures 3(c) and 4), the influence of salbutamol was rather low and, with exception of (dP/dt max)/p, there were no significant differences between salbutamol-treated group and the controls. On the other hand, differences between ISO and salbutamol were mostly significant. However, it should be mentioned that salbutamol caused short-term but significant decrease in peak negative dP/dt within the first minute after its administration. But this decrease was not associated with the depression in diastolic filling. In addition, salbutamol, in contrast to ISO, rather increased the diastolic filling rate (Figure 4(b)).
No rats died in the salbutamol-treated group during the 2-h experiment.
Discussion
ISO is a synthetic catecholamine with β1- and β2-agonistic activity. ISO is rarely used in pharmacotherapy, at present. Due to its positive dromotropic effect, it could be administered in cases of atrioventricular blockade. Apart from this, its β1 activity in the heart leads to positive chronotropic, ionotropic, and also bathmotropic effects. β2 activity in the vascular system is primarily associated with vasodilation of the blood vessels in skeletal muscles. Therefore, the administration of low ISO doses mimics moderate doses of adrenaline, which stimulates primarily β-receptors and leads to increased cardiac output (e.g. increases in the heart rate and contractility) in line with a decrease in TPR. 10 However, it is in contrast to what we found in our study in which we used cardiotoxic doses of ISO. The volume of the blood ejected from the left ventricle is primarily dependent on systolic (contractility) and diastolic functions of the heart. Both phases are markedly dependent on loading conditions (preload and afterload). While the loading parameters can be reliably determined, 19,22 –24 the precise determination of intrinsic contractility and relaxation has remained unanswered for many decades. Many approaches have been proposed, some of them are new and their validity should be verified or demands some specific processes (e.g. vena cava occlusion) or additional equipment (e.g. echocardiography). 25 –31 In this study, we used a maximal pressure rise in the isovolumic phase (dP/dt max) as a parameter of cardiac contractility. We are aware that dP/dt max is dependent on preload and afterload. Therefore, we modified this parameter in order to attenuate the loading interferences: preload influence can be diminished by division of dP/dt max by LVEDV ((dP/dt max)/V), and afterload by division with instantaneous left ventricular pressure at the dP/dt max ((dP/dt max)/p). 20,22 A parameter of diastolic relaxation peak negative dP/dt also depends on the loading conditions. 17 An additional factor—tau, a time constant of left ventricular isovolumic pressure decay, is less influenced by the loading conditions; but in ischaemic conditions, like in our model, its assessment may be blunted. 17,27 Generally, it appears that profound reduction in peak negative dP/dt is associated with an increase in tau and other relaxation parameters, suggesting relaxation depression. 27 Thus, with respect to marked changes in peak negative dP/dt in this study, this parameter was considered to be a sufficient predictor of diastolic relaxation.
In this experiment, the administration of ISO led to rapid decreases in preload, afterload (Figure 3) and myocardial diastolic function within 30 s (Figure 4). On the contrary, the myocardial contractility increased temporarily to 100% of the resting value (Figure 3(c)). This increase was followed by its decrease, but contractility remained elevated for the whole course of the experiment. This initial increase in contractility is in accordance with the haemodynamic action of ISO on β1-adrenergic receptors. This can be confirmed by the administration of selective β2-agonist salbutamol, which caused similar rapid reduction in afterload (Figure 3(b)), however, not a sudden peak in contractility (Figure 3(c)). Therefore, the main cause of the transient contractility peak in ISO group was not the reduced afterload. Salbutamol brought about only a moderate increase in contractility which was probably caused by the activation of the sympathetic nervous system or by the partial activation of β1-adrenergic receptors or by stimulation of presynaptic β2-adrenergic receptors with subsequent endogenous catecholamine release. The latter was documented for another β2-agonist clenbuterol. 32 Tachycardia, which can also elevate dP/dt max, 22 should be considered to be an additional factor. Nevertheless, this fact might not play a significant role in this study because after initial increase in the heart rate, tachycardia, in contrast to dP/dt max curve, remained relatively stable.
The decrease in afterload in the ISO group, confirmed in this study by decreased TPR (Figure 3(b)), may rather improve the stroke volume; therefore, it apparently does not play any role in the decreases in stroke volume. Moreover, as the ejection fraction did not change, it indicates that the decrease in the stroke volume was apparently associated with diastolic dysfunction or decreased preload. The cause of the decrease in preload is not known but generalized vasodilation or/and tachycardia could have played a role. When comparing ISO with salbutamol, it seems that tachycardia may be the main factor because both drugs decreased afterload in a similar manner. This can be explained by the fact that therapeutic doses of ISO caused an increase in preload in clinical studies. 10 The increase in preload was observed in patients with coronary heart disease after the enhancement in heart rate. On the other hand, healthy patients demonstrated a decrease in preload after the same increment of the heart rate, which was similar in this study. 33 Moreover, the relationship between diastolic function/dysfunction and LVEDP, the current marker of preload is not linear. 34 Therefore, it seems that the main factor was the impaired diastolic function. This conclusion may be supported by several findings: (1) tachycardia after sc administration of ISO shortened the diastole and deteriorated diastolic blood supply to the working myocardium. In addition, the same dose reduced the myocardial blood flow in previous studies; (2) a reduced diastolic pressure may be an additional factor in the deterioration of myocardial blood supply; (3) an increase in water content of myocardium after ISO administration, suggesting oedema was very rapid in previous studies; (4) ischaemia which is well described in the myocardium after higher doses of ISO causes relaxation disturbances; (5) the speediness of diastolic dysfunction documented in this study seems to be very rapid, different studies documented very rapid impairment in the myocardial homeostasis, for example some increase in lactate and inorganic phosphate even 30 s after ISO administration; (6) deterioration of the relaxation decreases the stroke volume and cardiac output, notwithstanding the increase in the heart rate. 17,27,34,35 The augment in the heart rate generally causes an opposite increase in dP/dt min, with a decrease in tau. Therefore, it improves the relaxation both in animals and in healthy humans. Nevertheless, the response may differ in patients with coronary heart disease. 17,19,33 Similarly, normal doses of noradrenaline, dobutamine, and ISO or stimulation of the sympathetic nervous system improved ventricular relaxation. 9,17,19,21,36
Some questions may arise from the fact that salbutamol produced a decrease in peak negative dP/dt too (Figure 4). A decrease in preload (although it is known that the decreased preload means lower dP/dt min) 17 can be excluded because the preload was normal in salbutamol group and normalized in ISO group, regardless of the fact that peak negative dP/dt remained depressed. The probable cause of peak negative dP/dt decrease in salbutamol group was the very rapid decrease in blood pressure, in particular diastolic blood pressure. It was likely related to lower myocardial perfusion and transient ischaemia associated with a transient diastolic dysfunction. Contrarily, in ISO-treated group, the peak negative dP/dt continued to drop within the first minute and remained depressed through the whole course of the experiment. It indicates persistently impaired diastolic function. In addition, salbutamol, in contrast to ISO, improved diastolic filling phase.
ISO cardiotoxicity is associated with both diastolic and systolic dysfunction in later phases, 12,13 and this study shows that diastolic dysfunction is very rapid and observable prior to systolic dysfunction. The finding that diastolic dysfunction precedes systolic one was documented in humans with coronary heart disease, arterial hypertension, left ventricular hypertrophy, and aging-related myocardial changes. 33,37 Diastolic relaxation is not a passive event, it requires energy, too. Therefore, the drop in ATP content may markedly deteriorate the relaxation as it happened probably in this case. 35,38 Calcium may play an important role in the relaxation and contraction effects. Low doses of ISO accelerate calcium reuptake by sarcoplasmic reticulum, leading first to the improvement in relaxation and in higher doses to an increase in the slow inward calcium current through voltage-gated calcium channels and increase in contractility. Very high doses or prolonged activation led to intracellular ‘calcium overload’ with its known consequences. 9,11,38 –40
This study had some limitations which mostly arise from the used methods. In particular, the precise study of ventricular volumes is dependent on many variable factors. 15,16 Some of them are changing after ISO administration (e.g. blood viscosity due to an increased platelet aggregation and coagulation, oedema of the heart tissue). 5,35,41 Therefore, the ventricular volume changes and their derived parameters cannot be established with precision within the whole course of the 2-h experiment. We used 15 min, implying a relatively short period in which these changes are of minor importance. We did not establish the pharmacokinetics of the administered drugs, but the results indicate that both drugs were rapidly absorbed. Following our previous studies as well as the results of others, the dose of ISO was chosen so that it would be significantly cardiotoxic. 11,35,42
Pharmacological doses of ISO are known to improve left ventricular contraction and relaxation together with the stroke volume and ejection fraction, 10 but the cardiotoxic dose is associated with marked systolic and diastolic dysfunction. In this study, we demonstrated that the cardiotoxic sc dose of 100 mg/kg of ISO produces rapid diastolic dysfunction and on the other hand improves the systolic function of the myocardium. The observed early diastolic dysfunction is primarily associated with the overstimulation of β1-adrenergic receptors, and the stimulation of β2-adrenergic receptors alone is not associated with the early myocardial diastolic dysfunction.
Footnotes
Acknowledgements
The authors wish to thank Mrs Anežka Kunová and Miss Renata Exnarová for their excellent technical assistance. We thank Mrs Ilona Havlíčková, MA for her critical reading and language correction.
Funding
This study was supported by grants from Charles University in Prague—Development Project 75/FaF/2b (2011) and Specific Higher Education Investigation SVV/2011/263-003.
Declaration of Conflicting Interest
The authors declare that they have no conflict of interest.