
Abstract
This study deals with the health effects within a child population, neighbouring a landfill. After detecting metals in soil and air samples collected in the surroundings of the landfill and in a control site, we have studied: (i) levels of lead (Pb) and exposure biomarkers in blood and urine, (ii) oxidative stress biomarkers and (iii) renal injury by applying a set of early effect biomarkers. Levels of Pb were higher in the exposed site (i.e. 1129 mg/kg and 640 ng/m3 in soil and air samples, respectively) versus those in the control site (i.e. 14.3 mg/kg and 9.3 ng/m3 in soil and air samples, respectively). Pb impregnation and levels of delta-aminolevulinic acid in urine were influenced by the living site that shows the prevailingly alarming situation in the Mbeubeuss landfill. Malondialdehyde changes indicated Pb-induced excessive production of reactive oxygen species. Lactate dehydrogenase activities and proteinuria were found to be higher in the children living in the exposed site. These evidences may reveal the usefulness of these two effect biomarkers to monitor the kidney injury entailed by relatively low-environmental exposure to Pb. Overall, these results show that the Mbeubeuss landfill constitutes a real source of environmental and health risk, be it living or working on site, of the surrounding population, predominantly for children.
Introduction
Air pollution is a growing public health problem worldwide, and emerging in African countries. However, the potential significant risks of the environment and of human health generated through accelerating industrialization, urbanization and traffic density in developing countries have only recently attracted attention. According to the World Health Organization (WHO), most of the inhabitants of developing countries are chronically exposed to health risks, notably those associated with continuously increasing untreated domestic waste. Taking into consideration both the health and the environment in the context of urban development and challenges to waste management are of the major concerns worldwide. 1 Open landfills inexorably threaten the health and the quality of life in surrounding populations. The menace of pollution from waste is particularly alarming in developing countries, due to the lack of appropriate infrastructures and, more generally, of appropriate management policies and strategies. 2 If dumped indiscriminately, hazardous waste may have both short- and long-term adverse human effects.
Waste produced in the City of Dakar, the capital of Senegal, is dumped in Mbeubeuss, an open air landfill outskirts of the urban zone. The breakdown of this waste has been found to be 45% fine waste, 20.2% organic waste, 8% plastics, 7.3% papers and cardboards and 2.7% metals. 3 These wastes also contain heavy metals, mainly due to their prior use in industrial production (e.g. batteries, aerosols, kitchen utensils, paint, ink and electronics components) or in various types of packaging (e.g. cans, juice or milk boxes, paper, cardboard and plastics). 4 The major environmental risk linked to heavy metals is due to the incineration of waste in dump sites. This leads in the emission of dust particles containing heavy metal such as lead (Pb) into the atmosphere.5 –7
The environmental and health risks of Pb, heavy metal well-known to be toxic even at relatively low-concentrations, are exacerbated by its particularly long half-life in the environment.8,4 Exposure to Pb is ubiquitous, with the highest levels found in some environmental exposures that have been associated with a number of serious systemic adverse effects involving the nervous system, blood-forming organs, lungs and kidneys. 9 Pb is also one of the most prevalent and nephrotoxic metal to human. 10 Chronic massive exposure to Pb produces renal adverse effects; notably progressive tubulointerstitial nephropathy that develops insidiously leads, therefore, to kidney failure. 11 To better define the exposure level without Pb-related early adverse renal effects, a large number of cross-sectional studies conducted during the last two decades, involving a renal biomarker battery, disclosed a lack of association between the urinary excretion of renal biomarkers of tubular or glomerular toxicity and levels of exposure to Pb.7,12 Pb-induced proteinuria is, therefore, characterized by the predominance of low molecular-weight (LMW) proteins derived from plasma, owing to the failure of proximal tubule to reabsorb proteins filtered through the glomeruli. 7 In adults, such urinary biomarkers (e.g. α-glutathione S-transferase (α-GST), clara cell protein (CC16) and retinol binding protein (RBP)) are the major constituents of LMW proteinuria related to the function or integrity of different nephron segments, which were found to be useful for detecting early adverse health effects of Pb.12 –16 Moreover, the underlying oxidative mechanisms involved in Pb-induced adverse health effects are now well documented. 17 Indeed, Pb induces oxidative stress conditions in specific organ targets not only by generating reactive oxygen species (ROS) but also by reducing cellular antioxidant defenses.17 –20
Exposure to Pb hazards could still be a serious health concern for inner-city children in developing countries like Senegal. Targeted community-specific prevention of childhood Pb poisoning requires much effort to complete the knowledge of local Pb emission sources and their relative contribution to the body burden. There is also a need for concerted efforts from African governments, health administrators and scientists to ensure that necessary attention is given to research on the subject so that meaningful control actions can be planned, thereby ensuring a suitable environment to live in. A few years ago, it was somewhat critical to undertake a pilot study, given the lack of relevant data from African developing countries. Subsequently, a cross-sectional study was carried out dealing with Pb exposure and its relationship to traffic density among Senegalese children living in the City of Dakar (Senegal).21,22 Now, as a part of the baseline evaluation for a community-based cross-sectional study, we sought to investigate the Pb impregnation levels in the Senegalese children living in Diamalaye II, near the Mbeubeuss landfill (Dakar, Senegal). Children have been considered a special risk group for Pb exposure, as they absorb the metals more readily than adults. The biomarkers of exposure to Pb among the children of Diamalaye II will be compared with those from the children residing in a different neighbourhood of Dakar (i.e. Darou Salam 6 Nder), sharing similar sociodemographic characteristics, but not exposed to the landfill.
After the determination of metal levels in soil and air samples collected in the immediate surroundings of the landfill, we focused our attention on determining (i) levels of Pb in blood and urine and the subsequent changes in biomarkers of haemoglobin (Hb) synthesis among the two groups of children, (ii) oxidative stress biomarkers and (iii) the evaluation of renal function by applying a set of early urinary biomarkers.
Materials and methods
Site description
Exposed site
Mbeubeuss is the name of a landfill located near Dakar (14°48′N/17°19′W), the capital of Senegal, in the territory of Pikine City (Diamalaye II; Figure 1). The landfill is located approximately 2 km north of the village of Keur Massar and 2 km east of the village of Malika. Mbeubeuss covers 600 ha and receives more than 395,000 tons per year of household solid wastes. This amount represents 86.43% of the 457,000 tons per year put in this landfill, 13.57% being industrial and hospital wastes (e.g. motor oil, plastic, iron, cardboard as well as electrical and electronic waste), 2 thereby constituting a real ecological bomb.

Map of the urban community of Dakar and the Mbeubeuss landfill situation.
The garbage is not covered with inert material and the landfill is not closed, which facilitates access to the site for both people and children. Moreover, the only known form of exploitation of the landfill remains the simple moving of the waste deposited by trucks. 23 In fact, the discharge receives daily about 3500 people, whose job is to recover and sort the marketable materials (e.g. plastics and metals), with a strong presence of women and children.
Control site
The control site named ‘Darou Salam 6 Nder’ is about 3.5 km far from the Mbeubeuss landfill. This site was selected to be far enough from the landfill, for not being under its pollution influence, but for sufficiently close from it to keep the same sociodemographic and economic properties in the population.
Ethics approval
The present epidemiological study was approved by the National Biomedical Ethics Committee of the Department of Health and Preventive Medicine of Dakar (Senegal).
Study population
The purpose and risks of the study protocol were explained to parents, and their written consent was obtained prior to the collection of samples and the questionnaire administration. Through individual detailed interviews, the basic demographic data and medical history of each child was determined. In order to be included in the final data analysis, children had to fulfil the following criteria: (i) live in their area of residence since their birth (i.e. control site: Darou Salam 6 Nder versus exposed site: Diamalaye II near the Mbeubeuss landfill), (ii) no family history of renal/urological diseases and (iii) no intake of potentially or suspected nephrotoxics. For the final analysis, children aged from 1 to 16 years were included: 26 children living in the exposed site and 32 socioeconomic status children on the control site.
Soil and air sampling and metal level determination
Soil sampling and metal level determination
For soil sampling, most of the current guidelines require the collection of composite samples. 24 Accordingly, composite samples were collected by taking 500 g of top soil (0–5 cm depth) in the control site (i.e. Darou Salam 6 Nder) and the exposed site (i.e. Diamalaye II near the Mbeubeuss landfill). Soil samples were sieved to remove all elements bigger than 4 mm and immediately stored at 4°C until analyses. Metal levels in soil samples were determined after microwave digestion (CEM Mars Express). According to Dudka et al., 25 sieved soils were digested in a mixture of nitric acid (HNO3) and perchloric acid (HClO4) in 1:2 (v/v) ratio. The resulting solutions were filtered and their volumes were adjusted to 25 mL with ultrapure water. Metal levels were determined using inductively coupled plasma-mass spectrometry (ICP-MS). 26 For ICP-MS calibration, standard solutions were prepared by diluting a commercial 10 ppm multielement standard (SCP33MS, SCP Science-Quebec, Quebec, Canada).
Air sampling of atmospheric particulate matter and metal level determination
The method used to collect the atmospheric particulate matter is total filtration on cellulose filter (Whatman 41, diameter: 110 mm and porosity: 0.4 µm) using a high volume sampling pump (Staplex TFIA-1 model) with a constant flow rate of 80 m3/h. During sampling, the pumps were placed at about 1.50 m high. After collection, filters were stored at 4°C in sterile Petri dishes. Metal levels were determined by ICP-MS after microwave digestion of the filter, as published elsewhere. 27
Biological sample collection, impregnation levels and biomarker study
Biological sample collection
Blood and spot urine (i.e. second morning void) were collected with disposable collection material certified for trace metal determination. Venous blood samples were obtained by venipuncture either into EDTA, heparized, citrate, and serum tubes. EDTA tubes were used for the determination of the levels of Pb (B-Pb), zinc protoporphyrin (ZPP) and glutathione status (GSSG/GSH). Whereas hemoglobin (Hb) and malondialdehyde (MDA) levels were analysed using heparized and citrate tubes respectively. Finally, serum tubes were used for the analysis of albumin (S-Alb), creatinine (S-Crea) and CC16 (S-CC16). Blood collection tubes were quickly placed in a cooling box at 4°C and transported to the laboratory where they were divided into aliquots and stored at −80°C until further analyses. Spot urine samples were collected in polyethylene tubes and transferred in a cooling box at 4°C to the laboratory where they were divided into aliquots and stored at −80°C until the determination of levels of Pb (U-Pb), RBP, CC16 (U-CC16), α-GST, delta-aminolevulinic acid (U-ALA), lactate dehydrogenase (U-LDH), creatinine (U-Crea), albumin (U-Alb), and total protein (U-Prot) in urine.
Impregnation levels and biomarker study
Samples from both the control and the exposed subjects were studied within the same runs of the analysis. The laboratory performing the metal analysis takes part in the quality control programs and is also approved by the French Ministry of Work and Solidarity. Level of Pb in blood (i.e. B-Pb) 28 and in urine (i.e. U-Pb) 29 was determined using ICP-MS. ZPP levels were determined in blood samples using a hematofluorometer and values were related to Hb. 30 ALA levels were determined in urine samples by spectrophotometry and values were related to creatinine. 31 MDA levels in plasma and glutathione status in whole blood (i.e. GSSG/GSH) were studied using high-performance liquid chromatography methods.15,32,33 The methemoglobin cyanide method was used to determine Hb contents in whole blood. 34 Levels of RBP, α-GST, CC16 and albumin in serum and/or urine samples were determined using commercially available immunoassays according to the manufacturer’s recommendations (i.e. RBP enzyme-linked immunosorbent assay, Randox Laboratories Ltd, Crumlin, UK; Biotrin Nephkit-Alpha human GST-α EIA, Biotrin International SARL, Lyon, France; CC16 Elisa Human Kit, Euromedex, Souffelweyersheim, France and BCG Albumin Assay Kit, Gentaur, Bruxelles, Belgium). LDH activity in urine samples was determined using the Cytotoxicity Detection Kit LDH (Roche Diagnostics, Neuilly-sur-Seine, France). Total protein contents in whole blood, plasma, serum and/or urine samples were determined using the bicinchoninic acid protein assay kit (Sigma-Aldrich, Saint-Quentin Fallavier, France). 35 Values of urinary markers were related to those of creatinine, as evaluated with the modified Jaffé reaction. 30
Statistical analysis
Excretion of urinary biomarkers was related to urinary creatinine to compensate for the influence of urine flow rate on excretion rates. Group general characteristics, levels of exposure to Pb and level of biomarker in blood and urine were expressed as mean ± SD and range (min; max). Comparisons were carried out between the control and the exposed subjects (Mann-Whitney U test). Thereafter, we looked for the blood or urinary biomarkers that are significantly associated with the levels of exposure to Pb using single linear regression models (Pearson test). SPSS for Windows (SPSS, Paris, France) was used to perform statistical analyses. Statistically significant differences were reported with the p < 0.05.
Results
Metal levels in soil and air samples
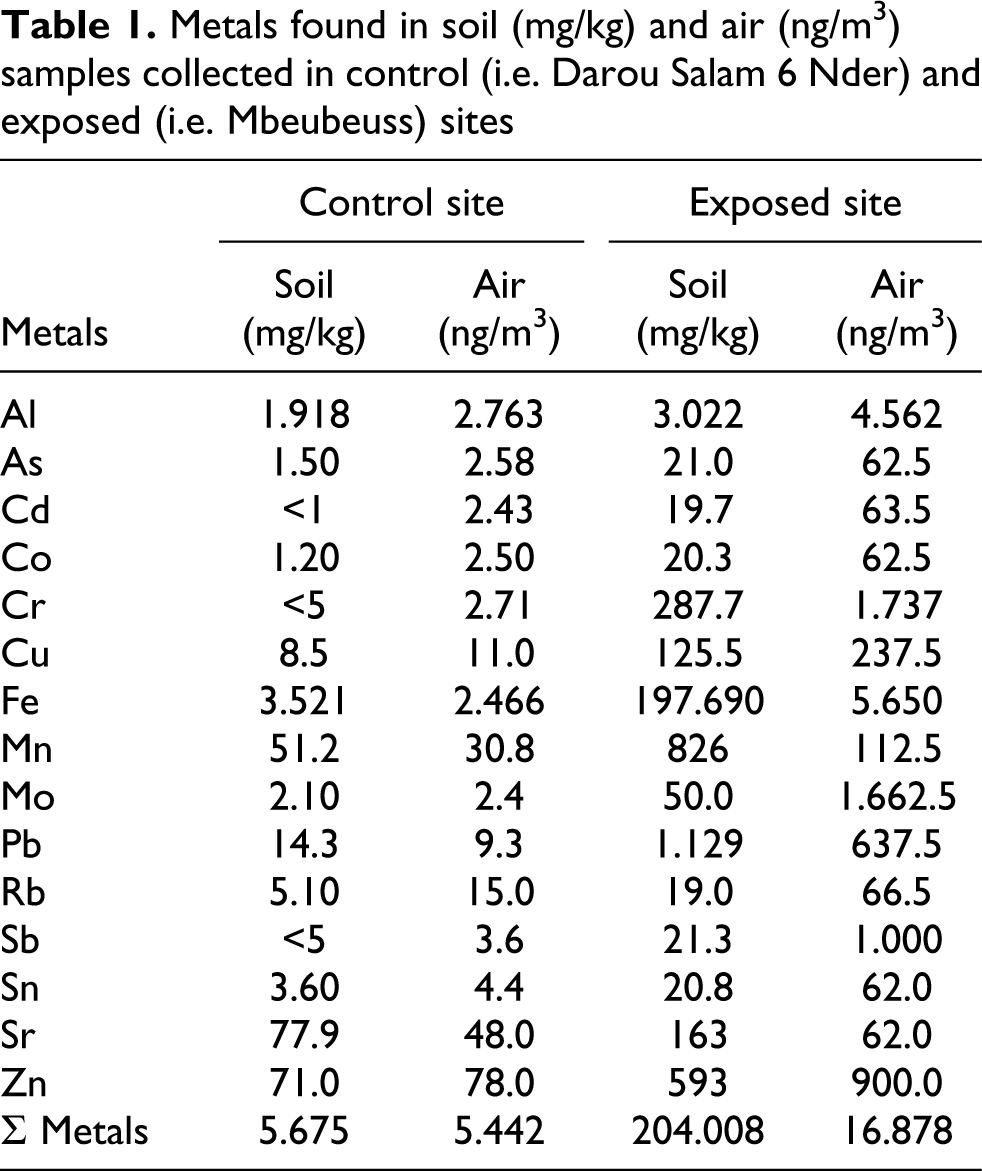
Table 1 shows the metals found in soil and air samples collected in the control site (i.e. Darou Salam 6 Nder) and the exposed site (i.e. Diamalaye II near the Mbeubeuss landfill). Similar patterns of metal levels were observed in both the soil and the air samples of the control or the exposed site. Indeed, there are few inorganic elements usually associated with the natural environment (e.g. Na, Mg and Ca), but, in contrast, there are a lot of anthropogenic elements (e.g. Al, Ba, Cd, Cr, Cu, Fe, Mn, Mo, Pb, Sb and Zn) that are also associated. The major metals in soil and air samples were also Al and Fe in the control site, and Al, Cr, Fe, Mo, Pb, Sb and Zn in the exposed site. Each metal was found at a higher level (i.e. sevenfold higher in soil sample and threefold higher in air sample) in the exposed site versus the control site. Furthermore, the heavy metal of interest, Pb, was detected at the highest levels in the soil and air samples collected in the exposed site (70- and 80-fold highest for Pb levels in soil and air samples, respectively).
Metals found in soil (mg/kg) and air (ng/m3) samples collected in control (i.e. Darou Salam 6 Nder) and exposed (i.e. Mbeubeuss) sites
General characteristics of the child population, impregnation levels and biomarker study
General characteristics of the child population
Basic demographic data (i.e. sex breakdown, age, height, weight and body mass index) of the children in the control site (i.e. Darou Salam 6 Nder) and the exposed site (i.e. Diamalaye II near the Mbeubeuss landfill) did not differ significantly (Table 2).
General characteristics and biomarkers of the control and the exposed subjects under studya

B-Pb: level of lead in blood; U-Pb: level of lead in urine; ZPP: zinc protoporphyrin; U-ALA: delta-aminolevulinic acid in urine; MDA: malondialdehyde; GSH: reduce glutathione; GSSG: oxidized glutathione; CC16: clara cell protein; RBP: retinol binding protein; α-GST: α-glutathione S-transferase; LDH: lactate dehydrogenase; U/S: urine/serum concentration ratio; NS: not significant.
aGeneral characteristics are expressed either as number or as mean ± SD and range (min; max). Level of lead in blood and urine (i.e. B-Pb and U-Pb, respectively), levels of biological markers in blood (i.e. ZPP, MDA, GSH, GSSG and creatinine), levels of biological markers in serum (i.e., S-CC16, S-albumin and S-creatinine) and levels of biological markers in urine (i.e. RBP, αGST, U-CC16, LDH, albumin and proteins) are expressed as mean ± SD and range (min; max).
b p < 0.001, Mann-Whitney U test.
c p < 0.05, Mann-Whitney U test.
d p < 0.01, Mann-Whitney U test.
Impregnation levels
Table 2 shows the levels of Pb in blood and urine, in both the control and the exposed subjects. B-Pb levels in all the children under study were relatively low: no subject had a B-Pb level >150 μg Pb/L in the control site and no children had a B-Pb level >400 μg Pb/L in the exposed site. Moreover, B-Pb levels were statistically influenced by living sites (i.e. mean B-Pb level was 82.2 µg Pb/L in control children versus 149.7 µg Pb/L in exposed children) but not by gender (Figure 2(a)). Similar observations were made for U-Pb levels (i.e. 0.7 µg Pb/g creatinine in control children versus 6.0 µg Pb/g creatinine in exposed children; Figure 2(b)). It is noteworthy that, in the child population under study, 42% of children (i.e. 13 children) had B-Pb levels >100 μg Pb/L and 13% of children (i.e. 4 children) had B-Pb levels >300 μg Pb/L. Only 6% and 3% of the children (i.e. 2 and 1 children, respectively) had U-Pb levels >20 μg Pb/g creatinine. Overall, of the 58 children under study, 10% of them (i.e. 6 children) had U-Pb levels >5 μg Pb/L. There were also positive relationships between B-Pb and U-Pb levels (i.e. r 2 < 0.752; p < 0.01), as shown in Table 3. Moreover, B-Pb and U-Pb levels were statistically significantly higher for the exposed boys (i.e. B-Pb: p < 0.01 and U-Pb: p < 0.05) and the exposed girls (i.e. B-Pb: p < 0.05 and U-Pb: p < 0.05) compared with the control boys and control girls, respectively. There were also positive relationships between B-Pb and U-Pb levels not only in boys (i.e. r 2 < 0.715; p < 0.01) but also in girls (i.e. r 2 < 0.876; p < 0.01; Table 4). As shown in Table 2, no significant change in ZPP levels was reported in the child population under study. There were positive relationships between B-Pb and ZPP levels (i.e. r 2 < 0.665; p < 0.01), on one hand, and U-Pb and ZPP levels (i.e. r 2 < 0.378; p < 0.01), on the other hand (Table 3). Moreover, positive relationships were also reported between B-Pb and ZPP levels not only in boys (i.e. r 2 < 0.627; p < 0.01) but also in girls (i.e. r 2 < 0.881; p < 0.01) and between U-Pb and ZPP levels only in girls (i.e. r 2 < 0.663; p < 0.01; Table 4). Moreover, U-ALA levels were statistically influenced by living sites but not by gender (Table 2 and Figure 2(c)). Table 4 shows a positive relationship between B-Pb and U-ALA levels (i.e. r 2 < 0.615; p < 0.05) only for the girl population.

Box plots of exposure and effect of biomarkers in blood, serum and urine (between control and exposed girls and boys) illustrated by the median, the upper and lower quartiles, the range and the outliers (°). Significant differences between control and exposed girls or boys are shown as follow: *p < 0.05; **p < 0.01; ***p < 0.001; Mann-Whitney U test. (a) Levels of B-Pb, (b) U-Pb, (c) U-ALA, (d) MDA and (e) α-GST, (f) urinary/serum CC16 ratio, (g) LDH activity and (h) level of protein in urine. CG: Control girls; EG: exposed girls; CB: control boys; EB: exposed boys; B-Pb: lead in blood; U-Pb: lead in urine; U-ALA: delta-aminolevulinic acid in urine; MDA: malondialdehyde; α-GST: α-glutathione S-transferase; LDH: lactate dehydrogenase; CC16: clara cell protein.
Relationships between the biological markers of exposure or effects of the subjects under study (i.e. levels of lead in blood and urine (B-Pb and U-Pb, respectively))

Relationships between the biological markers of exposure or effects of the boys or girls under study (i.e. levels of lead in blood and urine (B-Pb and U-Pb, respectively))

Biomarker study
In contrast to glutathione status, statistically significant changes in MDA levels were found in children living in the exposed site versus the control site (Table 2). Indeed, MDA levels were not influenced by gender (Figure 2(d)). Moreover, MDA levels, as an indicator of lipid peroxidation, were found to be positively correlated with B-Pb levels (i.e. r 2 < 0.392; p < 0.01), U-Pb levels (i.e. r 2 < 0.416; p < 0.01) and ZPP levels (i.e. r 2 < 0.375; p < 0.01; Table 3). Similar relationships were also observed in the boys but not in the girls (Table 4). With regards to the systemic biomarkers under study (i.e. S-CC16, S-creatinine and S-albumin), no statistically significant difference was reported between the children living in the exposed site versus the control site (Table 2). Nephron segment specific urine biomarker levels are summarized in Table 2. Indeed, the levels of RBP, αGST, CC16 and albumin in urine were not significantly modified between the two populations of children. Nevertheless, some significant changes in α-GST and CC16 levels were significantly influenced by living site and/or gender (Figure 2(e) and (f)). There were also negative correlation between RBP and U-ALA levels in the overall population (i.e. r 2 < −0.402; p < 0.01), and notably in the boys (i.e. r 2 < −0.369; p < 0.01). Moreover, positive relationships were found between U-CC16 and B-Pb levels (i.e. r 2 < 0.462; p < 0.01), ZPP levels (i.e. r 2 < 0.569; p < 0.01), MDA levels (i.e. r 2 < 0.400; p < 0.01) and RBP levels (i.e. r 2 < 0.420; p < 0.01); such positive relationships were also seen in the boys, and to a lesser extent in the girls (Tables 3 and 4). Moreover, αGST levels were positively correlated with U-Pb levels (i.e. r 2 < 0.538; p < 0.05) only in the girl population (Table 4). Finally, U-LDH activities and protein levels were significantly higher for the children living in the exposed site versus the control site (Table 2; Figure 2(g) and (h)). Positive relationships were also found between protein levels and U-Pb levels (i.e. r 2 < 0.286; p < 0.05), on one hand, and between U-LDH activities and U-Pb levels (i.e. r 2 < 0.330; p < 0.05), U-ALA (i.e. r 2 < 0.380; p < 0.01) and protein levels (i.e. r 2 < 0.491; p < 0.01), on the other hand; such positive relationships were also seen in the boys, and to a lesser extent in the girls (Tables 3 and 4).
Discussion
Nowadays, heavy metal impregnation has declined significantly among children in most developed countries. Yet, the extent and real magnitude of the problem has only been partially recognized nor assessed in most African developing countries, as in Senegal, where environmental and health situations of serious concern still remain. According to the high diversity of the encountered wastes (e.g. food scraps, domestic waste as well as industrial and hospital wastes) and the nonappropriate storage conditions (e.g. uncovered garbage and unregulated access), the Mbeubeuss landfill, located near Dakar (Senegal), constitutes a real source of environmental and health risks of the surrounding population, especially for children, living and/or working within it. Targeted community-specific prevention of childhood Pb poisoning requires much effort to complete the knowledge of local Pb emission sources and their relative contribution to the body burden. Hence, in order to contribute to a greater insight of the environment and health dangerousness of the Mbeubeuss landfill, a cross-sectional study was undertaken to evaluate (i) soil and air contamination levels of Pb, (ii) Pb impregnation levels of the surrounding population of children and (iii) helpfulness of the potential relationship between the levels of exposure to Pb in the landfill and the changes in biomarkers of haem biosynthesis, oxidative stress and/or nephrotoxicity in the sensitive child population under study.
The study of the metals present in the soil and air samples collected in the Mbeubeuss landfill revealed high Pb levels in the exposed site (i.e. Diamalaye II near the Mbeubeuss landfill: 1129 mg/kg and 640 ng/m3 in soil and air samples, respectively) versus those in the control site (i.e. Darou Salam 6 Nder: 14.3 mg/kg and 9.3 ng/m3 in soil and air samples, respectively). Pb levels found in the Mbeubeuss landfill soil were almost 80-fold higher than those in the control site, and threefold higher than those of Impact Statement set by WHO (i.e. 400 mg/kg). It is noteworthy that the Pb levels in air samples collected in the Mbeubeuss landfill were clearly higher than those reported by Dieme et al., 36 in two collection urban sites in Dakar (i.e. 7 and 20 ng/m3 in Fann and Faidherbe, respectively). Non-negligible Cd levels were found in the exposed site (i.e. 19.7 mg/kg and 63.5 ng/m3 in soil and air samples, respectively) versus those in the control site (i.e. <1 mg/kg and 2.43 ng/m3 in soil and air samples, respectively). Nevertheless, Dieme et al. 36 did not detect any Cd in the air samples they collected in Dakar.
The determination of Pb impregnation levels in the child population under study indicated that the B-Pb levels were closely influenced by the living site but not by gender. Children living in the exposed site have twofold and 10-fold higher B-Pb and U-Pb levels (i.e. 149.7 µg Pb/L and 6.0 µg Pb/g creatinine, respectively) than those living in Darou Salam 6 Nder (i.e. 82.2 µg Pb/L and 0.7 µg Pb/g creatinine, respectively). Overall, it is noteworthy that 42% of children (i.e. 13 subjects) had B-Pb levels >100 μg Pb/L and 13% of children (i.e. 4 subjects) had B-Pb levels >300 μg Pb/L. According to Sakai, 8 B-Pb levels are mostly the representative of soft tissue Pb and most widely used as measures of body burden and internal doses. According to the current literature, B-Pb levels in the child population living in the control site is in agreement with those in the child population living in Dakar (i.e. 99.7 µg Pb/L), noting that, since the phasing-out of leaded-gasoline, B-Pb levels in the Senegalese child population may have declined. 22 A few years ago, Diouf et al. 21 have undertaken a pilot study in order to assess the issue of Pb contamination in the Senegalese children residing on urban site or on rural site. They reported that, during the follow-up, the mean level of B-Pb in all the children (i.e. 83.4 µg Pb/L) was closely influenced by living site and gender. The mean level of B-Pb in urban children (i.e. 106.7 µg Pb/L) was higher than in rural children (i.e. 61 µg Pb/L), and overall, the boys had a higher mean level of B-Pb (i.e. 97.1 µg Pb/L) than the girls (i.e. 71.0 µg Pb/L). Soon after, these results were supported by the cross-sectional study conducted by Diouf et al., 22 in order to study B-Pb levels in Senegalese children and their relationships with changes in biomarkers of haem biosynthesis. They indicated that the mean level of B-Pb in all the children was 87.3 µg Pb/L and confirmed that it was influenced by living site and by genders. Indeed, in rural children, the mean level of B-Pb was relatively low (i.e. 67 µg Pb/L), whereas, in urban children, it was higher (i.e. 105.8 µg Pb/L); B-Pb levels in the boys were higher than in the girls. Taken together, these findings indicated that the child population living near the Mbeubeuss landfill was mainly exposed to Pb, thereby inducing a possible body burden, in agreement with the available data within the Senegalese child population living in rural and/or urban sites.21,22 Although these mean levels of B-Pb were below the current threshold values for which irreversible health effects are observed, the situation prevailing in the Mbeubeuss landfill and to a lesser degree in Senegal in general is quite worrying considering the mean level of B-Pb about 40 µg Pb/L often encountered in the child population in developed countries. 15
Children are particularly susceptible to Pb poisoning because they absorb far more Pb from their environments than adults. 37 Based on the accumulating evidence on the Pb toxicity at relatively low concentrations, Pb poisoning adversely affects children worldwide on the raised hearing threshold. 38 By 1991, the US Centers for Disease Control and Prevention recommended that 100 µg/L of B-Pb level in preschool children as the threshold of Pb poisoning. However, the biochemical changes in the body of children with B-Pb level of around 100 µg/L were poorly understood. 39
Pb is known to adversely affect many organs and systems in humans, where the haematological system is one of the important targets. 7 Indeed, Pb has an inhibitory effect on several enzymes involved in the chain reaction that leads to the formation of haem. 40 In the cross-sectional study, there was no significant change in ZPP level between the control and exposed child populations. However, B-Pb and ZPP levels (i.e. r 2 < 0.665; p < 0.01), on one hand, and U-Pb and ZPP levels (i.e. r 2 < 0.378; p < 0.01), on the other hand, were positively correlated. The final step of synthesis of haem, introducing Fe2+ into protoporphyrin XI, is also affected by Pb; the resulting inhibition of ferrochelatase and Zn2+ chelation induce both the formation and accumulation of ZPP, which could provide an index of disturbance of the final step in the synthesis of haem, and support ZPP as a useful marker of Pb exposure.40 –42 Another important finding was the difference between U-ALA levels in children living in the control and exposed site. Delta-aminolevulinic acid dehydratase (ALAD) is the second enzyme in the biosynthesis pathway of haem, which catalyzes the condensation of two molecules of ALA to a porphobilinogen. 8 ALA is synthesized in the mitochondria from glycine and succinyl-CoA by ALA synthetase (ALAS), which is a rate limiting enzyme in the haem pathway. ALAD possesses thiol groups, which are essential for its activity, and Pb, because of its affinity for thiol groups, is known to inhibit ALAD. 43 The decrease in ALAD activity and the indirect activation of ALAS due to negative feedback regulation by Pb exposure cause an increase in ALA in various tissues and in plasma, as well as its excessive excretion in urine, thereby recommending U-ALA as a measure of Pb effect. 43 Overall, the relevant results about ZPP and U-ALA levels supported the abovementioned results about quiet worrying Pb impregnation levels in the child population under study.
Among the underlying mechanisms involved in Pb-induced adverse health effects, Pb-induced excessive production of ROS in specific organ targets has been cited.22 –24 According to the literature, in the cross-sectional study, MDA levels were significantly higher in the exposed children than in the control children.30,40,44 MDA levels, as an indicator of lipid peroxidation, were found to be positively correlated with internal doses and exposure biomarkers of Pb (i.e. B-Pb, U-Pb and ZPP), supporting the crucial contribution of Pb-induced oxidative damage in Pb toxicity. As ALAD inhibition may result in the accumulation of ALA, which has been shown to be involved in Pb-induced oxidative damage, it is reasonable to speculate that, in the cross-sectional study, the excessive lipid peroxidation in Pb-exposed Senegalese children was triggered by ALA accumulation resulting from Pb-induced ALAD inhibition. 39
Chronic environmental exposure to Pb may produce progressive tubule-interstitial nephropathy that develops insidiously and often leads to kidney failure. 7 There have been many debates on the long-term significance of LMW proteinuria among subjects with chronic low or moderate environmental exposure to Pb. The level of Pb exposure, which may be associated with early adverse renal effects, is, however, uncertain because incipient Pb nephropathy is difficult to detect due to the lack of appropriate blood or urinary biomarkers reflecting an early adverse effect on the kidney. 11 In the cross-sectional study, LDH activities and proteinuria in urine were found to be higher in the children living in the exposed site versus the control site, and positively correlated with Pb impregnation levels and exposure biomarkers. Taken together, these results show the possible usefulness of both these effect biomarkers to monitor the kidney alterations induced by relatively low-environmental exposure to Pb. However, urine levels of the other urine biomarkers under study (i.e. RBP, αGST and U-CC16) were not clear enough to unequivocally point out a possible failure of the proximal tubule in reabsorbing proteins filtered through the glomeruli in Senegalese children exposed to the relatively low-environmental Pb levels within the Mbeubeuss landfill.7,10,15
Conclusion
Overall, the results of this cross-sectional study showed that exposed children, living near the Mbeubeuss landfill, had higher impregnation levels of Pb than control children, thereby supporting that the Mbeubeuss landfill constitutes a real source of environmental and health risk of the surrounding population, especially children, living and/or working within it. Changes in the exposure (i.e. ZPP and U-ALA) and effect (i.e. LDH activity and proteinuria) of biomarkers supported the quite worrying Pb impregnation levels found in the child population living near the Mbeubeuss landfill. Moreover, Pb-induced excessive production of ROS in specific organ targets may be involved in the Pb-induced renal injury. Hence, the environmental exposure to the emissions of Pb, from the landfill Mbeubeuss, is important in the neighbouring population of children. These arguments merit attention and could probably help to place these environmental problems, which are a new challenge for poor countries, at the heart of future development programs.
Footnotes
Funding
The Unité de Chimie Environnementale et Interactions sur le Vivant (UCEIV), EA4492, participates in the Institut de Recherches en ENvironnement Industriel (IRENI), which is financed by the Région Nord-Pas de Calais, the Ministère de l’Enseignement Supérieur et de la Recherche, and the European Regional Development Funds (ERDF). The research described in this article has benefited from grants from the Centre de Recherche pour le Dévelopement International (CRDI) of Dakar (Senegal). The Agence Universitaire de la Francophonie (AUF) provided Mathilde Cabral’s PhD financial support.
Acknowledgements
The authors thank Prof. Michel Lhermitte from the Laboratoire de Toxicologie of the Centre de Biologie-Pathologie, Centre Hospitalier Régional et Universitaire, Lille, France for the skilful technical and scientific assistance in the analysis of metal internal doses and exposure biomarkers as well as Mr Stephen Bones, a native English speaker, from the CUEEP of the Université du Littoral Côte d’Opale for his kind and careful rereading of the article.