
Abstract
This study was conducted to evaluate the possible genotoxic effects of waste anesthetic gases. Comet assay was performed on peripheral blood lymphocytes of 60 volunteers: 20 healthy unexposed office workers and 40 operation room (OR) personnel at Tanta University Hospital (Egypt). The exposed personnel were anesthetists (6 females and 7 males), surgeons (10 males), nurses (9 females), and technicians (8 males). The study revealed significantly increased comet parameters (mean comet tail length and mean percentage of DNA in the tail) in peripheral blood lymphocytes of OR personnel in comparison with control individuals. The maximum DNA damage was observed in anesthesia technicians, whereas the nurses showed the least DNA damage. Furthermore, significant difference was observed between smoker and nonsmokerOR personnel in relation to mean comet tail length. However, no significant difference was seen due to age, gender, or duration of exposure. Also, significant increase in mean percentage of tail DNA was observed in smoker individuals of both exposed and control groups. As a conclusion, this study points to the risk of DNA damage in personnel who are exposed to waste anesthetic gases.
Introduction
Contamination of operating theaters with anesthetic gases is inevitable due to the probability of leakage from anesthesia systems and release of gases through patients’ expiration. Anesthesia induction with masks besides the use of uncuffed endotracheal tubes and semiclosed anesthesia circuits are added causes in pediatric patients. 1,2 A great concern has been raised about the operation room (OR) personnel who work in places with inadequate waste gas scavenging and air conditioning systems and might thus be exposed to health risks from anesthetic agents. 3,4
During recent decades, the possibility of health hazards resulting from the exposure to anesthetic gases has been discussed extensively. 3 –8 Some studies have suggested that chronic exposure to trace levels of anesthetic gases may cause immunologic problems and genotoxicity. 9,10
Assessment of genotoxicity can be performed using different genetic markers such as chromosomal aberrations, sister chromatid exchanges, micronucleus test, and alkaline comet assay. 11 As a rapid, simple, sensitive, and versatile technique, the alkaline comet assay (syn: single-cell gel electrophoresis assay) has been increasingly used in diverse areas of genotoxicity studies. 12 This technique is capable of detecting a wide range of genetic damage such as DNA single-strand breaks, double-strand breaks, base damage, and alkali labile sites in individual cells. 13
Human epidemiologic studies assessing the genotoxicity risk arising from the exposure to anesthetic gases have revealed both positive 10,14 –16 and negative findings. 17 The contradictory results obtained in the genetic biomonitoring of individuals chronically exposed to anesthetics could be due to differences in the anesthetic agents used or the cytogenetic biomarker evaluated. Other factors such as the duration and intensity of exposure could be considered as well.
It is understandable that data from one study in one particular occupational setting cannot be used to judge the genetic risk in another occupational setting. This makes this study rational, despite the availability in the literature of similar investigations but on different populations or under different conditions of exposure. A survey of literature on the genotoxicity resulting from the exposure of health professionals to waste anesthetic gases revealed no studies from Egypt. Hence, the present work was initiated to assess the genome damage in OR personnel in one of the Egyptian hospitals. The results of this study should contribute to the proper implementation of intervention measures aimed to eliminate or significantly reduce worker exposure and prevent untoward biological effects, besides addressing the need of regular biomonitoring of exposed personnel.
Methods
The study was approved by our local ethics committee. All participants received detailed information concerning the aims of this research work, and informed consent was obtained from each of them prior to the beginning of the study.
Study population
A total of 60 blood donors, 20 healthy unexposed office workers, and 40 OR personnel participated in the study. The control group included 20 individuals (12 males and seven smokers) aged from 27 to 55. They were selected from the same hospital population, but with no history of occupational exposure to anesthetic agents.
The exposed personnel were anesthetists (6 females and 7 males), surgeons (10 males), nurses (9 females), and technicians (8 males). All the females were nonsmokers and 14 males were smokers. The anesthetists, nurses, and technicians spend about 8 hours per day in the operation theater for 6 days per week, whereas surgeons spend about 8 hours per day for only 2 days per week. The age of the exposed personnel ranged from 26 to 56 years, and the average duration of their employment ranged between 1 and 35 years. During work, all subjects were exposed to a complex mixture of anesthetic agents. The most commonly used anesthetics were New-Flotan® (halothane stabilized with thymol 0.01%), Isoflurane® (isoflurane with no additives or stabilizers), Ultane® (sevoflurane containing no additives), and nitrous oxide (as pure, liquefied compressed, medical grade nitrous oxide gas). The ORs had air conditioning systems but not central high-flow scavenging systems.
Each participant was asked to complete a questionnaire that included standard demographic data (age, gender, address, and marital state), medical history (acute and chronic diseases, radiotherapy and chemotherapy, vaccinations, contraception, and medication), and lifestyle (smoking, tea, and coffee). It was ensured that both exposed and control subjects neither took any vaccinations nor were exposed to any kind of radiation or chemotherapy for 12 months before sample collection.
The subjects who smoked more than five cigarettes per day for at least 1 year were considered as smokers. Table 1 shows the main characteristics of both groups.
Demographic characteristics of control and exposed subjects
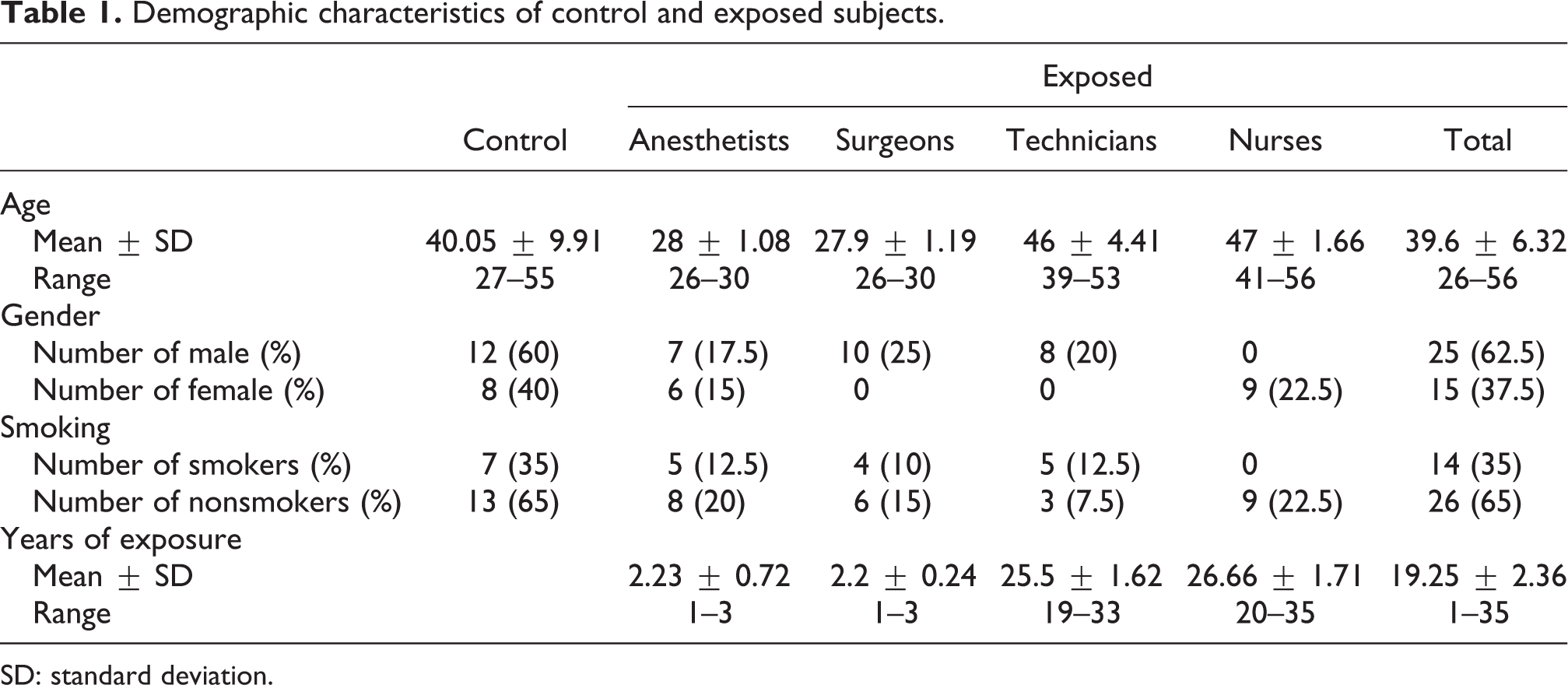
SD: standard deviation.
Tail length (in µm) and tail DNA percentage in control and exposed subjects

SD: standard deviation.
a Significantly different from control (p < 0.05) as determined by Student’s t test.
Blood sample collection
All subjects contributed to the study with a single blood donation. Venous blood samples (approximately 5 ml) were drawn from each subject into heparinized tubes. Samples were coded, transmitted on ice to the laboratory, and processed within 2 hours. Genotoxic effects were evaluated through the alkaline comet assay.
Alkaline comet assay
The alkaline comet assay was conducted as described by Singh et al. 18 Lymphocytes were separated from the heparinized peripheral blood and washed with RPMI-1640 culture medium supplemented with 10% fetal calf serum. Cell pellets were mixed with 70 μl of 0.7% low-melting point agarose at 37°C and then placed on microscope slides precoated with a thin layer of 0.5% normal melting agarose. After cooling at 4°C for 5 min, slides were covered with another layer of low-melting agarose. After solidification at 4°C for 5 min, slides were immersed in a cold, freshly prepared lysing solution for 60 min. After that, the slides were removed and placed close together in a horizontal gel electrophoresis tank filled with fresh alkaline buffer (1 mM disodium EDTA and 300 mM NaOH, pH 13) for 20 min at 4°C to allow DNA to unwind and to show the alkali-labile sites. Electrophoresis was conducted at 4°C with 25 V and 300 mA for 20 min. Then the slides were taken out, washed in distilled water, and Tris buffer (0.4 M Tris, pH 7.5) was added to neutralize excess alkali. After washing, the slides were allowed to dry at room temperature prior to staining with ethidium bromide. The whole procedure was carried out in dim light to prevent additional DNA damage.
Per each individual, 100 cells were analyzed at ×400 objective of an Olympus fluorescent microscope equipped with an excitation filter of 515–560 nm and a barrier filter of 590 nm. Two comet parameters were measured, that is, tail length and percentage of DNA in the tail. The length of DNA migration (comet tail length) was measured in micrometers from the nucleus center to the tail end. The percentage of DNA in the tail was determined by measuring the total intensity of ethidium bromide fluorescence in the cells (considered as 100%) and determining the percentage of the intensity measured only in the tail. Computerized image analysis system was used for this purpose.
Statistical analysis
The results of the study were recorded as mean and standard deviation for each group and then statistically analyzed using Student’s t test. Results were considered significant when p < 0.05. The SPSS for Windows (version 16) software package was used (SPSS Inc., Chicago, IL, USA).
Results
The two studied groups had comparable demographic characteristics. Within the exposed group, individuals were divided into subgroups by profession. It was not possible to match all studied variables in subgroups, as all nurses were women and all surgeons and technicians were men. The distribution of subjects with respect to age, gender, smoking, and years of exposure was demonstrated in Table 1.
Fluorescent microscopic examination of peripheral blood lymphocyte of control subjects revealed prominence of fluorescent spheres without tail (Figure 1). On the other hand, peripheral blood lymphocytes of OR personnel displayed many damaged cells with fluorescent heads and tails (Figures 2 and 3). These morphological findings were confirmed by statistical analysis, which showed significantly increased comet parameters (mean comet tail length and percentage of DNA in the tail) in OR personnel when compared with the control subjects. Among the OR personnel, the maximum DNA damage was observed in anesthesia technicians, whereas the nurses showed the least damage (Table 2).
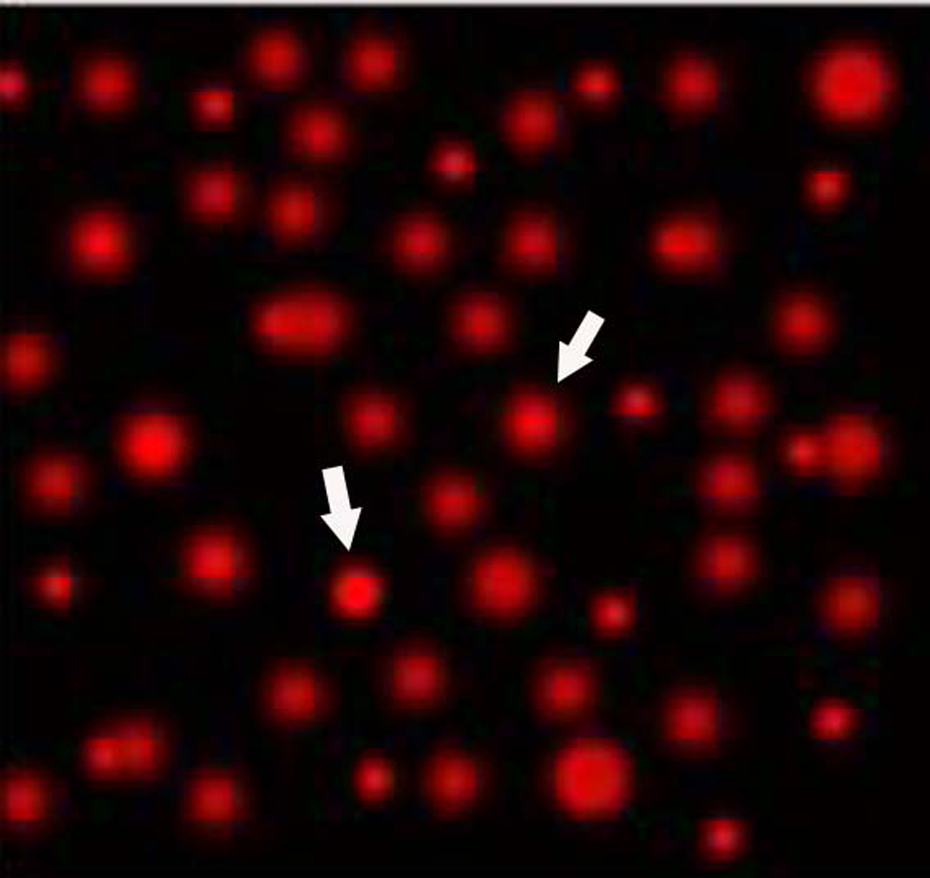
A photomicrograph of peripheral blood of control group, showing fluorescent spheres without tail (arrow; ethedium bromide stain; microscopic magnification ×400).
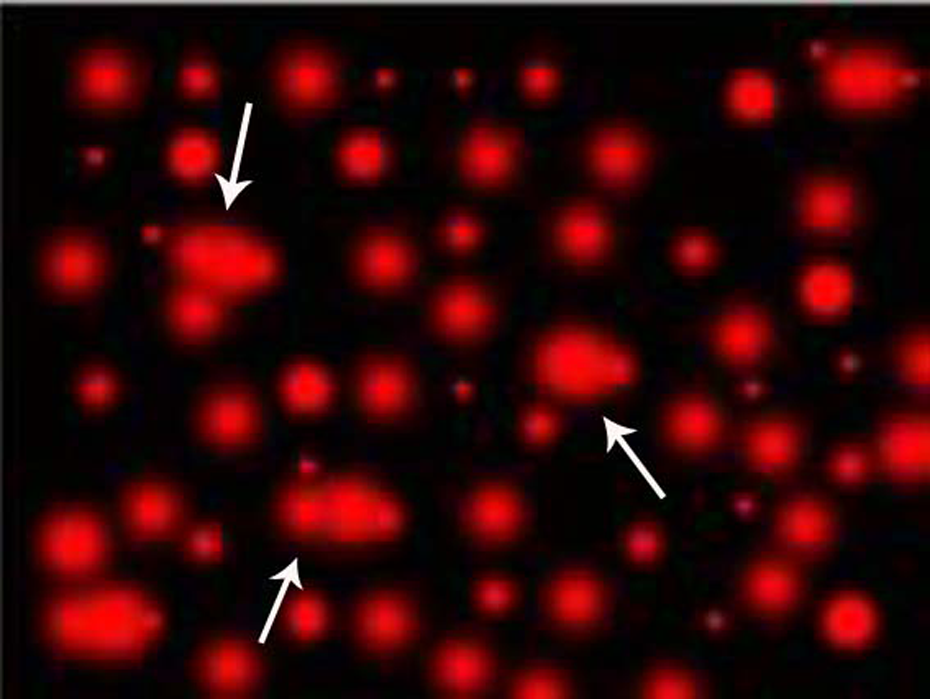
A photomicrograph of peripheral blood lymphocytes of operating room personnel, showing many fluorescent heads with tails (arrow; ethedium bromide stain; microscopic magnification ×400).

A photomicrograph of peripheral blood lymphocytes of operating room personnel, showing many fluorescent heads with tails (arrow; ethedium bromide stain; microscopic magnification ×400).
In operating theater personnel, a significant difference was observed between smokers and nonsmokers in relation to mean tail length. However, no significant difference was seen due to age, gender, or duration of exposure (Table 3).
Tail length (in µm) by age, gender, smoking, and duration of exposure in control and exposed subjects

SD: standard deviation.
aSignificant.
A significant increase in the percentage of DNA in tail was observed in all participants with smoking exposure. In addition, significant difference was observed between male and female exposed subjects. However, the percentage of DNA in the tail showed no association with age or years of exposure (Table 4).
Percentage of DNA in the Tail by age, gender, smoking, and duration of exposure in control and exposed subjects

SD: standard deviation.
aSignificant.
Discussion
Over the years, there have been significant improvements in the control of anesthetic gas pollution in health care facilities. However, occupational exposure to waste anesthetic gases still occurs. 11 Hence, this study was conducted to evaluate the genetic damage in OR personnel (anesthetists, surgeons, nurse anesthetists, and technicians) at Tanta University Hospital. DNA injuries caused by different anesthetic agents have been studied by different methods of detection. Being highly sensitive and specific, the comet assay proved to be a useful tool to evaluate the degree of DNA damage. 19,20
Although the exposure levels to anesthetic gases were not evaluated, the present study points to an increase in DNA damage in the OR personnel. Using the alkaline comet assay, the current study revealed significant increase in both comet tail length and percentage of DNA in the tail in the lymphocytes of exposed subjects compared with the controls. These results indicate that the level of exposure in the workplace is sufficiently high.
Although the DNA damage was higher in the anesthesia technicians, the differences between the exposed subgroups were not statistically significant. Recently, a study on a group of 17 nurse anesthetists exposed to waste anesthetic gases showed significant differences in comet parameters between the control and exposed groups. 8 Furthermore, an earlier study, 21 using the comet assay, demonstrated an elevated grade of DNA damage in OR personnel exposed to waste anesthetic gases in Ankara. However, Szyfter et al. 17 did not observe such a genotoxic effect using the same technique.
The studies using comet assay to determine the risk of genotoxicity provided conflicting results and were reviewed by many authors. 19 The mechanisms explaining the lack of DNA damage reported in some studies are still under debate. However, it was claimed that peripheral lymphocytes are not the proper cells to examine the genotoxicity of anesthetics, as adaptive response might emerge at prolonged exposure. In addition, during monitoring of working population, it is rather difficult to achieve entirely equal conditions of exposure. Interindividual differences in sensitivity to studied agents are also considered. 20,22
In the current study, smoking was associated with a significant effect in relation to DNA damage. This effect was noticed by other investigators as well. 11 This finding is not surprising in light of the presence of free radical generating nicotine and N-nitrosamines in tobacco smoke. 23 However, the majority of previously published human biomonitoring studies failed to show an effect of smoking on DNA migration in the comet assay. Various explanations for the reported discrepancies have been proposed, including the power of the statistical analysis, differences in the brand and number of cigarettes smoked per day, and the amount of tar contained in tobacco. Passive smoking, which is usually overlooked, is another contributing factor to the inconsistency of the results. 8,19
DNA damage showed no association with age or years of employment, but a significantly increased percentage of DNA in the tail was observed in male subjects of the exposed group. However, the significance of male gender in relation to comet assay results was denied by Chandrasekhar et al. 11 Surprisingly, the latter study showed the significance of age, gender, and duration of exposure using a different assessment technique, that is, the micronucleus assay. Based on the fact that DNA damage repair capacity is impaired with age, it seems reasonable to speculate that comet parameters could increase in older subjects when compared with younger ones. However, not much reports support this assumption. This can be attributed to the intensive physical exercise among the young study subjects, which was unaccounted for, but probably can increase the level of basal DNA damage, thus masking the age-related variation between the old and the young. 19
In the present research work, for clinical relevance, we described the genotoxic effects of the authentic inhalation anesthetics used in our ORs. Isoflurane, sevoflurane, and nitrous oxide contain no additives or stabilizers. Halothane is stabilized with thymol 0.01% (w/w).
Although our results revealed an association between occupational exposure of health professionals to anesthetic agents and the induction of genotoxicity, the dose dependency of genotoxic effects was not established. Current knowledge regarding the association between genotoxicity of waste anesthetic gases and occupational exposure limit is obscure due to lack of environmental monitoring of anesthetic concentrations in most of previous genotoxicity studies. Assessment of the extent of genetic material damage in relation to the actual magnitude of exposure was demonstrated in only a few studies. Wiesner and colleagues 10 proved that exposure to inhaled anesthetics above the limits recommended by The National Institute for Occupational Safety and Health (NIOSH) 24 was associated with genotoxicity, as they observed a significant increase in the micronucleus frequency in a group of anesthetists exposed to high levels of anesthetics (about 170 ppm nitrous oxide and 4 ppm of halothane and isoflurane) but not to low levels (12 ppm nitrous oxide and less than 0.5 ppm of the volatile anesthetics isoflurane, sevoflurane, and desflurane). Also, an earlier study demonstrated that the number of micronucleated lymphocytes was higher in veterinary surgeons exposed to waste anesthetic gases (5.3 ppm isoflurane and 12.3 ppm nitrous oxide) than in nonexposed subjects, although the difference was statistically nonsignificant. 25 Using a different cytogenetic biomarker (sister chromatid exchange), induction of genotoxicity was demonstrated in a group of OR personnel exposed to waste anesthetic gases within the exposure limits of NIOSH (11.8 ppm nitrous oxide and 0.5 ppm isoflurane). 3 Occurrence of genotoxic effects has been reported in health professionals exposed to anesthetic concentrations above and within the exposure limits of NIOSH. These discrepant results might be explained by a number of factors such as employing too small study groups that are simultaneously exposed to several anesthetic agents, using different cytogenetic end points, as well as insufficient matching for age, gender, and smoking habits.
The results of this study indicated that occupational exposure to a mixture of anesthetic agents induced a significant increase in the level of genotoxicity. Although these results do not allow us to draw conclusions regarding a possible mechanism of the genotoxic action of the studied anesthetics, several mechanisms have been suggested. It was proposed that inhalation anesthetics may undergo a residual metabolic oxidation or reduction, giving rise to reactive products. Sevoflurane can undergo dehydrofluorination by soda lime and barium hydroxide lime in the anesthesia apparatus, releasing several degradation products including fluoromethyl 2,2-difluoro-1-(trifluoromethy) vinyl ether (compound A). 26,27 Compound A is an alkylating agent that demonstrated genotoxic effect in Chinese hamster ovary cells, using sister chromatid exchange technique. 28 Similarly, halothane may undergo reductive defluorination producing 1-bromo-1-chloro-2,2-difluoroethylene, an alkylating agent, which is potentially genotoxic. Also, direct reaction with DNA may occur with halothane or isoflurane and the most feasible alkali-labile modification may be alkylation at the N7 position of purines. 29 The capacity of inhalational anesthetics to cause DNA damage was observed in lymphocytes of patients anesthetized by sevoflurane or isoflurane using comet assay, which detects DNA damage including strand breaks and alkali-labile sites. 30 DNA strand breaks were also detected in peripheral blood lymphocytes of patients anesthetized with isoflurane–nitrous oxide–oxygen mixture. 31 Besides, DNA single-strand breaks with oxidized purine and pyrimidine bases were detected in lymphocytes of patients receiving sevoflurane anesthesia. This could explain DNA damaging potential of sevoflurane, since accumulation of oxidized bases has been considered a pathogenic event in cancer. 32 In addition, oxidative DNA damage was shown in OR personnel, and it was related to insufficient antioxidant capacity and excessive generation of reactive oxygen species. 33 Disturbance of the pro-oxidant/antioxidant balance is considered to be a causative factor underlying the oxidative damage to cellular molecules such as DNA. 34
The comparison between occupational studies is difficult since the level and type of exposure, biological factors, and protective measures vary among different studies. The outcome of this study indicates the danger of exposure to waste anesthetic agents in the hospital under study, suggesting the need for further minimizing the exposure. The waste anesthetic gas scavenger and air conditioning equipment should be checked frequently and sufficient ventilation should be provided.
Conclusions
This study points to the potential risk of DNA damage in the health care workers who are exposed to waste anesthetic gases and recommends minimizing exposure in the studied hospital. Precautions will help to reduce health risks in the exposed hospital personnel. Further studies should include a better design using larger study groups with measurement of hazardous agents’ concentrations.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.