
Abstract
Brucellosis is a zoonotic disease caused by a kind of Brucella bacteria, which commonly appears in humans and rarely causes mortality. In our study, five cases, who were diagnosed by evaluation of clinical findings and serological tests, they also had very high ferritin levels, were reported. Ages of the patients were 16, 12, 10, 16 and 8 years, respectively. Serum ferritin levels were 1200, 985, 886, 748 and 435 ng/ml, respectively. We observed that complaints of the patients reduced after the treatment and ferritin levels returned to its normal range. In the situations of extremely evaluated serum ferritin which is an acute-phase reactant, its levels are able to raise in brucellosis, without existing hemochromatosis and Still’s disease
Introduction
Since the time of Hippocrates, brucellosis is a well-known multisystem disease that contains many different clinical features and complications.1,2 This is the most common zoonosis in the world. Brucellosis is endemic in Turkey. Approximately 18,000 new patients with brucellosis are determined annually in Turkey. 3 The main ways of transmission have been reported as infected milk and milk products via dietary intake, inhalation of stable powders from the habitat of infected animals or skin contact with infected animals and animal products. The main common clinical symptoms and findings in most patients are high fever, muscle–joint pain, fatigue and anorexia. 4 Diagnosis is usually confirmed via result of clinical features, serology or culture. 5 In an organism, a systemic response begins within hours or days. The condition is likely to cause an inflammatory process and this response is defined as an acute phase response. 6 Because brucellosis is an infectious disease, it increases acute phase reactants such as C-reactive protein (CRP) and ferritin. 7 In this study we present five patients diagnosed with brucellosis with very high ferritin levels.
Case 1
A 16-year-old male patient was admitted to a health institution 20 days before due to fever and joint pain. Various treatments were given in the institutions where the patient had been presented initially. The patient's symptoms did not diminish, and so he was admitted to our emergency department. Other findings of patient were normal except pallor and weakness in his physical examination. Laboratory results were detected as abnormal, as follows: brucella agglutination test: 1/1280, ferritin: 1200 ng/ml, lactate dehydrogenase (LDH): 846 U/L and Hb: 11.5 g/dl. Complaints of the patient decreased after implementation of binary antibiotic (doxycycline and rifampin) therapy for 6 weeks and the patient’s general condition improved. Control tests gauged are as follows: hemoglobin 13 g/dl, ferritin: 118 ng/ml and LDH: 320 U/L.
Case 2
A 12-year-old male patient presented to our hospital with complaints of fever, joint pain and cold chills, he had these symptoms for approximately 40 days before he came to the hospital. Upon physical examination, the spleen was palpable 3 cm. Results of laboratory analysis were as follows: ferritin: 985 ng/ml, LDH: 724 U/L, sedimentation: 48 mm/h, CRP: 96 mg/L and brucella tube agglutination test: 1/1280. We started triple antibiotic (doxycycline, rifampicin and streptomycin) therapy. The patient’s symptoms and signs disappeared within 2 weeks after the onset of treatment. Subsequent control investigations were as follows: ferritin: 146 ng/ml, sedimentation: 32 mm/h, CRP: 8 mg/L and LDH: 211 U/L.
Case 3
A 10-year-old female patient presented to our clinic with complaints of joint pain, weight loss and perspiration since a month. There were no pathological findings except splenomegaly (3 cm below the rib) on physical examination. Laboratory results of patient were as follows: ferritin: 886 ng/ml, alanine transaminase (ALT): 87 U/L, aspartate aminotransferase (AST): 90 U/L, LDH: 773 U/L and γ-glutamyl transpeptidase (GGT): 68 U/L, alkaline phosphatase (ALP): 420 U/L, CRP: 21 mg/L, total bilirubin: 2.60 mg/dl, direct bilirubin: 1.68 mg/dl and brucella tube agglutination: 1/1280. Gentamicin (for 10 days) and doxycycline (for 6 weeks) combined therapy was initiated. General condition of the patient improved and her complaints regressed significantly after 3 weeks since the start of therapy. Results of control analyses were as follows; ferritin: 146 ng/ml, sedimentation: 32 mm/h, CRP: 8 mg/L and LDH: 211 U/L.
Case 4
A 16-year-old male patient with complaints of cold chills, joint pain and abdominal pain lasting for 3 weeks before he was presented to our clinic. This patient had a history of eating cheese and fresh herbs. The physical examination was normal except pallor and fatigue. Brucella agglutination test: 1/1280, ferritin: 748 ng/ml and LDH: 850 U/L were detected after laboratory analysis. His complaints resolved after treatment with dual antibiotic therapy using doxycycline and rifampicin for 6 weeks. Results of the control analyses were as follows: ferritin: 145 ng/ml and LDH: 164 U/L.
Case 5
The patient was 8-year-old and the sibling of the patient from case 4. History of the patient was studied in-depth after diagnoses of case 4. We learned that this patient’s symptoms were similar to those of the sibling (case 4). Brucella agglutination test of case 5 was detected as 1/640. Other test results were as follows; ferritin: 435 ng/ml and Hb: 10.6 g/dl. Evidence for physical examination of the patient was unremarkable. Control results of the patient were as follows: LDH: 182 U/L, ferritin: 161 ng/ml and Hb: 12.8 g/dl after triple combined treatment of trimethoprim, sulfametaksazol and rifampicin for 6 weeks.
Discussion
Brucellosis is a zoonotic disease transmitted from animals to people through direct contact or inappropriate consumption of animal products. In developing countries and Turkey, it is a common disease in regions where raw milk and milk products are consumed and also where cattle-breeding is carried out constantly.
Clinical signs and symptoms of brucellosis may be confused with many other diseases because of its diversity. 8 Anemia, leukopenia, thrombocytopenia, and elevation of ALT, AST and LDH can be seen in case of brucellosis. 9 Brucellosis, being an infectious disease, can lead to elevation of acute-phase reactants such as reactive protein (CRP) and serum ferritin. 7
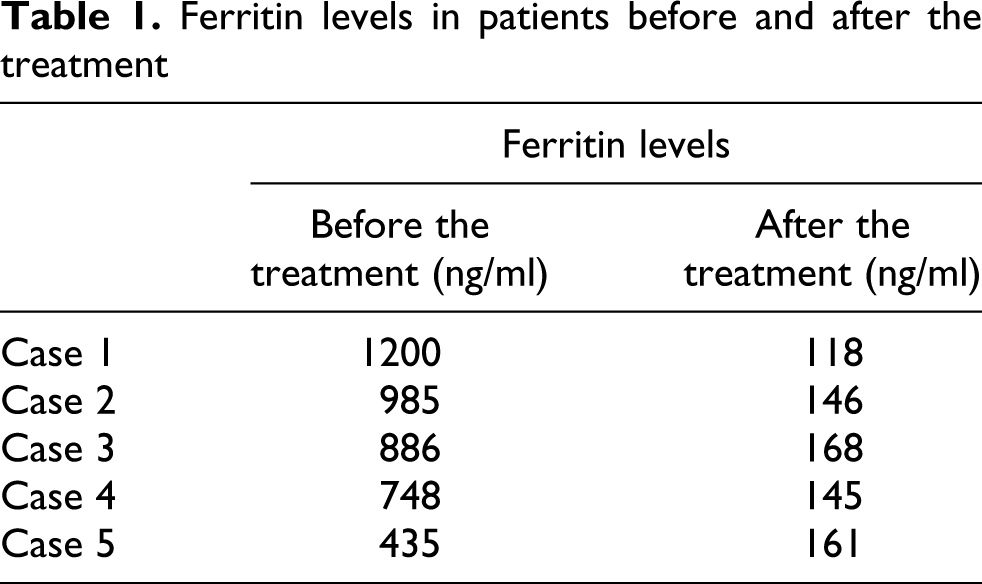
In patients with brucellosis, though the acute-phase reactant ferritin was elevated, very high values of it were not reported. Elevated ferritin levels lead to hemochromatosis and Still’s disease. None of the five cases had hyperpigmentation, previous transfusion history (differential diagnosis of hemochromatosis) and skin lesions (differential diagnosis of Still’s disease). Ferritin levels of cases diagnosed with brucellosis, subsequent to clinical findings and serological tests, were found to be elevated. These values were determined to be a few times higher than the highest value of serum ferritin, which was reported in the literature. In our study, the number of cases and ferritin levels were higher than found in previous studies, our study therefore contributes to previous literature. High ferritin levels of patient returned to its normal range after treatment (Table 1 ).
Ferritin levels in patients before and after the treatment
In our cases, the elevated serum ferritin levels were thought to be due to excessive inflammatory response against bacterial overload. In the literature, elevation of serum ferritin levels was reported as a comorbid condition emerged as a consequence of nonspecific tissue damage, iron metabolism abnormalities and hematopoietic failure.10,11
As a result, all cases demonstrate that brucella infections are able to increase the ferritin levels to match levels found in conditions that are associated with very high levels of serum ferritin, such as hemochromatosis and Still’s disease.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.