
Abstract
Occupational exposure to lead may cause an increase in blood pressure. The aim of the study was to estimate the effect of occupational exposure to lead on selected parameters of ambulatory blood pressure monitoring (ABPM) and structural changes in carotid arteries. The study included 33 normotensive men occupationally exposed to lead and 39 unexposed men employed in administration of the foundry. All of the men underwent 24-hour ambulatory blood pressure monitoring and high-resolution B-mode ultrasonography to determine intima-media thickness (IMT). The group of men occupationally exposed to lead manifested significantly higher mean systolic blood pressure (MSBP), mean diastolic blood pressure (MDBP), mean blood pressure (MBP), pulse pressure (PP), variability of diastolic blood pressure (VDBP), and IMT than the unexposed group. The studied groups did not differ in mean values of variability of systolic blood pressure (VSBP). As compared to the unexposed group, in men exposed to lead, atherosclerotic plaques were significantly more common. In the group of persons exposed to lead the Pearson’s correlation coefficient analysis revealed significant linear positive correlations between MSBP and IMT, between lead level and the number of atherosclerotic plaques, and between lead level and PP. Multivariate stepwise regression analysis demonstrated that higher lead level in blood and higher triglyceride concentration in blood represent independent risk factors of an increased pulse pressure in the group of individuals occupationally exposed to lead. Occupational exposure to lead can be associated with increased blood pressure and accelerated progression of atherosclerosis.
Introduction
The relationship between occupational exposure to lead and abnormalities in human circulatory system still seems to be insufficiently recognised. Although several publications are available which deal with in vitro and experimental studies on laboratory animals and examine various aspects of lead effects on cardiovascular system, their analysis provides no unequivocal proof of the extent to which lead and its compounds may affect blood pressure, development of arterial hypertension, and atherosclerosis. The available experimental and epidemiological data permit to conclude that occupational exposure to lead may result in an increased blood pressure. 1-3 However, it seems indispensable to confirm or to verify the existing assumptions and to pinpoint the site occupied by lead among other factors that play a role in the pathogenesis of arterial hypertension, including angiotensin II, aldosterone, increased sympathetic activity, decreased concentration of atrial natriuretic peptide and B-type natriuretic peptide, the decrease in nitric oxide, higher concentration of endothelins, high salt intake, low physical activity, abdominal obesity mainly of androgenic type, and mental stress. In view of the existing doubts, it seems significant to apply more reliable investigative methods than those that have been applied till now.
Values of blood pressure parameters obtained in 24-hour ambulatory blood pressure monitoring (ABPM) manifest greater reproducibility than blood pressure measurements obtained in medical offices or at home measurements, performed by patients themselves. 4,5 Despite numerous data pointing to its usefulness, ABPM still remains an approach that is not sufficiently exploited. 6
The carotid artery intima-media thickness (IMT) represents an early marker of atherosclerotic plaques. Increased values of IMT in the common carotid artery are generally recognized to represent an independent risk factor of cardiovascular incidents. 7,8
The aim of the study was to estimate the effect of occupational exposure to lead on selected parameters of ambulatory blood pressure monitoring and structural changes in carotid arteries.
Methods
The study included 33 male employees of a copper foundry who were occupationally exposed to lead and who worked in the metallurgical section and preparation of charge as metal smelters, refiners or converter workers (group I). The group was compared to 39 unexposed men employed in administration of the foundry (group II). The magnitude and quality of the environmental exposure for all of the men included in the study was similar. All persons inhabited the same region at similar distances to the car traffic. For the study group, we included only subjects who inhabited the region for at least 10 years. Persons who were on a special diet (e.g. vegetarians) were excluded from the study. Concentrations of lead dust at the workplaces of group I participants of the study ranged from 0.55 to 4.48 of maximum admissible concentration (MAC) established in Poland (0.05 mg/m3). Persons working at the workplaces with exposure to compounds other then lead exceeding 0.2 of MAC were excluded. Clinical characteristics and characteristics of occupational exposure to lead of the studied groups are presented in Table 1 .
Clinical characteristics and occupational exposure to lead of studied groups (group I: men occupationally exposed to lead; group II: healthy men, the unexposed group)

Abbreviations: ALA-U: concentration of deltaaminolevulinic acid in urine, BMI: body mass index, FEP: concentration of free erythrocyte protoporphyrins, Pb-B: lead concentration in whole blood.
Personal data concerning health status of all the participants of the study were obtained on the basis of anamnesis, physical examination, and basic laboratory tests. From the study, we excluded persons with formerly diagnosed or suspected arterial hypertension, diabetes, coronary artery disease, heart failure, peripheral artery disease, renal failure, hypercholesterolemia, hypertriglyceridemia, and other metabolic diseases that could confound the results.
From every examined man, blood samples were taken from the cubital vein, around 12 h after the last meal. Part of the blood was allowed to clot and the other part was mixed with ethylenediaminetetraacetic acid (EDTA), spun at 10,000 rpm, then the plasma was collected and kept frozen at the temperature of –70°C. The blood sampling was preceded by informing the examined men on aims of the project and obtaining their written consent for participation in the study.
Total cholesterol, high density lipoproteins (HDL cholesterol) and triglycerides (TG) concentrations in serum were determined using kits of Spinreact Company. Low-density lipoproteins (LDL cholesterol) level was calculated using the formula of Friedewald: LDL cholesterol = total cholesterol – (HDL cholesterol + TG/5), when triglyceride content was <400 mg/dL. If TG concentration exceeded 400 mg/dL, both LDL and HDL cholesterol levels were determined using a uniform colorimetric technique. Blood pressure was measured using a mercury manometer.
Concentration of lead in blood (Pb-B) was estimated by a flameless technique, in a graphite cuvette using the atomic absorption spectrometer, SOLAAR M6 (Thermo Elemental). The estimations were performed in the Atomic Absorption Laboratory, subjected to the inter-laboratory quality control of estimations.
Levels of delta-aminolevulinic acid in urine (ALA-U) were estimated by spectrophotometry. 9 Free erythrocyte protoporphyrins (FEP) were estimated according to Piomelli et al., by a fluorimetric technique, in a Perkin-Elmer fluorimeter. 10
All of the men underwent 24-hour ambulatory blood pressure monitoring. ABPM was performed by using Welch Allyn ABPM 6100 (Welch Allyn UK, Aston Abbotts, Buckinghamshire). A mean blood pressure (MBP), mean systolic blood pressure (MSBP), mean diastolic blood pressure (MDBP), variability of systolic blood pressure (VSBP), variability of diastolic blood pressure (VDBP), and pulse pressure (PP) were estimated. Pulse pressure was calculated using the formula of PP = MSBP – MDBP. VSBP represented standard deviation (SD) of all systolic blood pressure measurements in 30-min intervals and VDBP was represented by standard deviation of all measurements of a diastolic blood pressure in 30-min intervals.
High-resolution B-mode ultrasound images obtained with the ALOKA ProSound SSD-5500 SV system (Aloka Inc, Tokyo, Japan) were used to determine IMT, while both carotid arteries were measured with a linear array transducer 5-10 MHz. Measurements of IMT were taken on the distal 10 mm of both right and left common carotid artery in the far wall. Five determinations were done on each side and the average measurement was used as the IMT. With the concomitant use of duplex Doppler, atherosclerotic plaques were evaluated.
All statistical analyses employed the Statistica PL 6.0 software (StatSoft, Poland). We analyzed the basic parameters of ABPM (MSBP, MDBP, MBP, PP, VSBP, VDBP), IMT and the incidence of the atherosclerotic changes within the carotid arteries. In the analysis, the factors possibly confounding the results were considered: anthropometric data, parameters of lipid metabolism, the frequency and intensity of smoking habit, and the frequency and amount of alcohol consumption. For quantitative variables, arithmetic means and standard deviations of the parameters were calculated in the studied groups. Distribution of variables was tested using the Shapiro and Wilk W test. In the case of quantitative independent variables of a normal distribution, statistical analysis took advantage of the t test for independent variables. In the case of independent quantitative variables manifesting a distribution distinct from the normal one, the Mann-Whitney U test was used. Results for categorical and binary variables were expressed in percents. The subsequent statistical analysis of independent qualitative variables took advantage of the chi-square test (maximum likelihood method). Relationships between examined variables were determined using analysis of correlation and regression. Significance of differences and relationships was established at the level of p < 0.05.
Results
Comparing the group of occupationally lead-exposed individuals with those of the unexposed group, no significant differences were detected in parameters of lipid metabolism or blood pressure (Table 2).
Parameters of lipid metabolism, arterial blood pressure, frequency of cigarette smoking and alcohol consumption in the studied groups (group I: men occupationally exposed to lead, group II: men representing the unexposed group)

Abbreviation: TG: triglycerides.
However, the group of persons occupationally exposed to lead manifested significantly higher mean values of MSBP, MDBP, MBP, PP, VDBP, and IMT in comparison to unexposed subjects. The studied groups did not differ in mean values of VSBP. As compared to the unexposed group, in men exposed to lead, atherosclerotic plaques were significantly more common (Table 3).
Parameters of ABPM, IMT, and percent of subjects with atheroslerotic plaques in the studied groups (group I: men occupationally exposed to lead, group II: men composing the unexposed group)
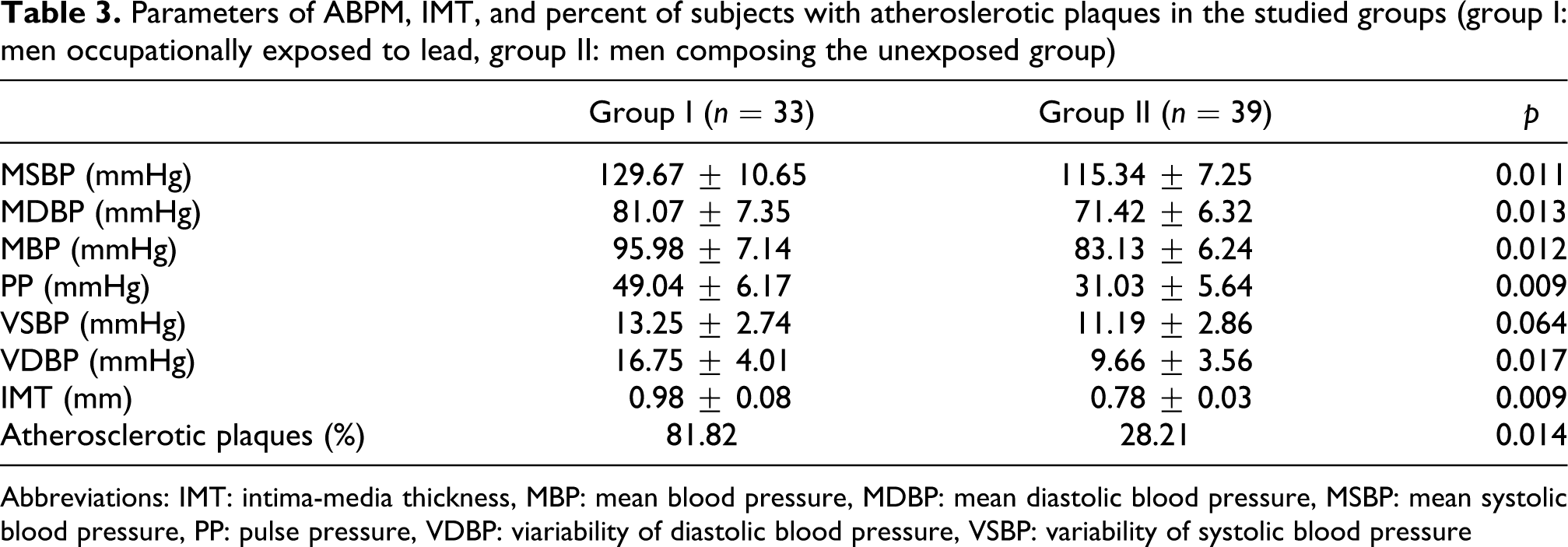
Abbreviations: IMT: intima-media thickness, MBP: mean blood pressure, MDBP: mean diastolic blood pressure, MSBP: mean systolic blood pressure, PP: pulse pressure, VDBP: viariability of diastolic blood pressure, VSBP: variability of systolic blood pressure
In the group of persons exposed to lead, the Pearson’s correlation coefficient analysis revealed significant linear positive correlations between MSBP and IMT (r = 0.50; p < 0.01), between lead level and the number of atherosclerotic plaques (r = 0.44; p < 0.05), and between lead level and PP (r = 0.63; p < 0.05).
In the group of persons exposed to lead, the possible independent risk factors for the pathological changes in the parameters of ABPM were found on the basis of the simple linear regressions between parameters of ABPM (MBP, MSBP, MDBP, VSBP, VDBP, PP) and basic anthropometric data (age, height, body mass, BMI, BSA), mean values of blood pressure, lipid metabolism parameters (total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides), and toxicological parameters (Pb-B, FEP, ALA-U). The simple linear regressions were performed because of a relatively small number of the examined group of persons exposed to lead. As the next step, with the use of multivariate stepwise regression analysis the final models were obtained for the specific ABPM parameters, taking statistically significant variables of simple linear regressions: age, TG, Pb-B and FEP into account. The model PP = 32.83 + 0.02 Pb-B + 0.07 TG ± 4.76 was characterized by the highest value of the determination coefficient (R 2 = 79.13%) and the lowest p value (p < 0.01). The obtained model permitted to demonstrate that higher blood lead levels and higher blood triglycerides concentrations represent independent risk factors of an increased pulse pressure in the group of individuals occupationally exposed to lead (Table 4).
Results for the final model obtained in multivariate stepwise linear regression analysis

Abbreviations: Pb-B: concentration of lead in whole blood, PP: pulse pressure, SEM of Rc: standard error of the regression coefficient, TG: triglycerides.
Discussion
Lead and its compounds belong to the most harmful substances among those to which workers of non-ferrous metal foundries are exposed. In 1990−1996, emission of lead compounds was reduced in 41 European countries by 1% to 61% per year, as compared to the preceding year. 11 As a result, the number of acute intoxications with lead became reduced within the last 15 years. Nevertheless, occupational exposure to lead continues to pose a significant health problem. 12 Numerous population studies point to an increased general mortality (the total number of deaths in the population in a period of time due to various causes) due to occupational exposure to lead compounds. 13,14 The health-endangering concentration of lead in blood is thought to involve levels exceeding 15.3 µg/dL according to the British Regional Heart Study, 10 µg/dL according to NHANES II study and 2 µg/dL according to NHANES III study. 15-17
Effect of lead on circulatory system has provided topic of scientific studies for over 80 years. The first observations of the cause-effect relationship between exposure to lead and manifestation of arterial hypertension appeared in reports of Harris and Mayer, originating from the years of, respectively, 1918 and 1927. 1 The first epidemiological evidence for the relationship between lead and arterial hypertension was provided by Vigodortlchik in 1935. However, studies that failed to demonstrate the relationship or even excluding it appeared in parallel. 18,19 Also, experiments on animal models provided no unequivocal evidence. According to the current knowledge, an effect of lead on blood pressure depends on the dose of lead to which somebody is exposed and duration of the exposure. A single exposure to a low dose of lead causes a transient hypertensive effect. On the other hand, high doses of lead, which induce acute intoxication, cause a decrease in blood pressure. 1-3 In animals, low doses of lead systematically administered for a long time cause arterial hypertension. 12
Despite formulation of the above conclusions by investigators, the role of lead in the pathogenesis of arterial hypertension remains unsolved. Moreover, contradictory reports on the subject continue to appear. This reflects difficulties of interpreting the relationships between exposure to lead and development of circulatory pathology in humans. Development of diseases in the cardiovascular system may be determined by co-existing exposure to metals and of other pathogenetic factors, such as consumption of alcohol, cigarette smoking, and other metabolic or systemic diseases. Moreover, drawing conclusions as to the role of a single metal in the pathogenesis of diseases of circulatory system may be hampered by a parallel exposure to other metals. 20 Therefore, analysis of results obtained in the exposed group requires a comparison to an appropriately selected unexposed group of similar principal anthropometric parameters, environmental exposure to metals, use of condiments, spices, and certain beverages, which might significantly bias the obtained results or manifestation of other systemic or metabolic diseases. 21 Planning to interpret effect of a single metal on body functioning, one has to consider first selection of the group which, with high probability, could be defined as a group with isolated exposure to a given metal. This is linked to the necessity of using complex statistical techniques that permit to define the so-called independent risk factors. Moreover, an appropriate technique should be selected for measurement of studied parameter, in this case blood pressure and structural lesions in carotid arteries. The most suitable technique seems to involve the technique warranting the highest sensitivity and specificity of evaluation, yielding in parallel reproducible and credible results of measurements.
In the author’s opinion, due to introducing the specific inclusion and exclusion criteria, a good comparability of the group exposed with the not exposed was gained. The compared groups did not significantly differ in anthropological parameters. The magnitude and quality of the environmental exposure for all of the men included into the study was similar. All persons inhabited the same region at similar distances to the car traffic. For the study group, we included only subjects who inhabited the region for at least 10 years. Persons who were on a special diet (e.g. vegetarians) were excluded from the study. Individuals who provided in anamnesis, physical examination, and basic laboratory tests a diagnosis of arterial hypertension, diabetes, ischemic heart disease, heart failure, peripheral artery disease, renal insufficiency, hypercholesterolemia, hypertriglyceridemia, or other metabolic and systemic diseases that might significantly affect results of the study were excluded.
In order to get a high credibility of the study, methods recommended by international societies were used: ABPM for the determination of blood pressure and IMT to evaluate structural lesions in carotid arteries. As compared to office measurements, 24-hour ambulatory blood pressure monitoring correlates better with frequency of organ complications associated with high values of blood pressure. 4,5 In European Lacidipine Study on Atherosclerosis (ELSA), such a rule was documented for organ complications such as the number of atherosclerotic plaques and thickness of intima-media complex in carotid arteries. 22,23 Numerous studies demonstrated correlations of IMT with such risk factors as age, male sex, active cigarette smoking, obesity, arterial hypertension, hyperlipidemia, diabetes, elevated levels of C-reactive protein, fibrinogen, or homocystein. 24
Application of the above validated method allowed for a credible evaluation of the effect of lead on blood pressure and structural lesions in carotid arteries. In the present study, it was demonstrated that occasional measurements using a mercury manometer failed to detect higher values of blood pressure in persons occupationally exposed to lead but not suffering from arterial hypertension, as compared to the unexposed group. In the group, an average duration of 26 years of work with lead exposure did not increase either systolic or diastolic blood pressures. Application of ABPM permitted to show that in the group of persons occupationally exposed to lead who did not have arterial hypertension, values of mean systolic blood pressure, mean diastolic blood pressure, mean blood pressure, pulse pressure, variability of systolic blood pressure, and thickness of intima-media complex were significantly higher than in the unexposed group. Moreover, in the group of workers occupationally exposed to lead, there were significantly more individuals with atherosclerotic plaques. In the workers occupationally exposed to lead, mean systolic blood pressure was higher by around 14 mmHg and mean diastolic blood pressure was higher by around 10 mmHg, mean blood pressure was higher by around 12 mmHg, and pulse pressure was higher by 18 mmHg than in the group unexposed to lead. The obtained linear Pearson's correlations between mean systolic blood pressure and thickness of IMT (r = 0.50; p < 0.01), between lead level in blood and the number of atherosclerotic plaques (r = 0.44; p<0.05), and between lead level in blood and pulse pressure (r = 0.63; p < 0.05) seem to confirm a hypertensive and pro-atherosclerotic effect of lead in persons occupationally exposed to this metal.
The performed regression analysis allowed to find out that in the group of persons occupationally exposed to lead, higher lead levels in blood and higher triglyceride levels represented independent risk factors of an increased pulse pressure. Increase in blood lead level above the tolerable limit in Poland of 500 μg/L caused the increase in the mean pulse pressure in the studied group by 10 mmHg, as compared to the value estimated for the specific person without exposure to lead. Increase in blood triglycerides level by 100 mg/dL was linked with the increase in mean pulse pressure in the studied group by 7 mmHg, as compared to the value estimated for the specific person without exposure to lead. As shown by studies performed in recent years, an increase in pulse pressure represents one of independent risk factors for cardiovascular incidents. 25 Darne et al. observed a significantly increased risk of death due to ischemic heart disease in patients with high values of pulse pressure. 26 Hypertension Detection and Follow-up Program study demonstrated that pulse pressure represents a risk factor for cardiac and general mortality but not of cerebrovascular mortality. 27,28 In view of the above quoted data, the demonstration that exposure to lead represents an independent risk factor of increased values of pulse pressure may significantly affect our awareness of the harmful effects of lead compounds on human body.
There are some limitations in our study. The main limitation is the relatively small size of both the lead-exposed and unexposed groups. However, both the lead-exposed and unexposed groups included more than 30 subjects and were fairly comparable. Moreover, statistically significant results were obtained in the study. On the other hand, the number of subjects could be still too small to extrapolate the study findings to general population, although we think our data are suggestive. Also, there are factors possibly confounding comparability of the results obtained from the persons occupationally exposed and unexposed such as the frequency and intensity of smoking habit and alcohol consumption, exposure to compounds other than lead, and the incidence of metabolic diseases. We think we did our best to minimize the influence of factors confounding the results by the use of the precise criteria of qualifying persons for the study. The other limitation of the study is the lack of the determination of lead in bones, one of the markers of chronic, long-lasting exposure to this metal.
Conclusion
Occupational exposure to lead can be associated with increased blood pressure and accelerated progression of atherosclerosis.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not for-profit sectors.