
Abstract
Girls in Western countries are often sent to therapy to better manage their behaviour. Once in the therapy room, children often rely on nonverbal means to express their thoughts or feelings in therapy interactions. Children demonstrate their understandings of their mental health and awareness of their experiences through bodily postures. Yet there is limited literature that critically examines girls’ body language in therapy. The current study uses a critical discourse analysis to investigate reoccurring patterns of postures across two girls’ discursive therapy sessions. A Foucauldian power analysis illustrates girls’ body language is a form of everyday resistance to deficit-focused interactions. It shows how the girls were identified in problematic ways at times, and how they used their bodies to actively resist and reposition themselves in the therapeutic encounter by using the physical space around them. Findings demonstrate the need for professionals working in therapy contexts to critically examine the meaning of girls’ body language to avoid inadvertently positioning them as gendered docile bodies in need of modification and self-management.
Where there is power, there is resistance. (Foucault, 1979, p. 95)
In the current neoliberal regime, girls are expected to self-regulate intense feelings and behaviours irrespective of the intersecting forms of oppression they may experience (Dhar, 2020). Caregivers, particularly mothers, are under increased scrutiny to raise daughters to be productive citizens, independent and self-contained (Callaghan et al., 2017; Füredi, 2002). Such neoliberal expectations increase the pressure on mothers to seek professional support for their daughters who may express intense emotions (Füredi, 2002). Individualised therapy approaches can decontextualise and depoliticise the challenges parents, particularly mothers, currently face (Kilty & Dej, 2012) having to balance increased workforce participation with caregiving responsibilities (Autret et al., 2024). Such approaches frequently overlook the oppressive structures, such as poverty, gendered violence, racism and ableism, that cause and perpetuate girls’ distress (Brown, 2021).
In institutional contexts such as the therapy room, power relations are present, with girls having to negotiate their access to the conversational floor via verbal and nonverbal means (Avdi, 2015; Reid & Brough, 2023). Power operates in therapeutic conversations with caregivers who, at times, are given the opportunity to retell a deficit-focused problem-saturated story about their child (Reid, 2024). Such stories identify the child as ‘the problem’, with the child being expected to address their problematic behaviours via therapy. As Paré (2014) argues, ‘identities are not merely “shared” in therapy but also forged there’ (p. 209). Power relations are reflected in adult-centric expectations of how children could and should participate with their minds and bodies in therapy sessions (M. O’Reilly & Parker, 2013). Girls can be expected to sit still and listen to the therapist and/or their caregiver, speaking only at designated pauses in the therapeutic interaction. In therapy, certain bodily movements can be seen as inappropriate participation in the session. Kallio and Honkatukia (2022) refer to these expectations as ‘institutional bodily control’, which can reinforce problematic identity conclusions (p. 114). Such forms of institutional bodily control can unintentionally inform therapy with girls and, therefore, cannot be ignored.
Children's communication is multimodal, using their voice, bodies and objects around them to express themselves in everyday relational contexts (Taylor, 2012), including the therapy room. Children utilise body language to convey their thoughts, emotions and responses to their therapists and caregiver(s). Although there has been a pseudoscientific interest in body language, this work has largely overlooked the matrix of power relations in the child's life and the gendered expectations that operate through the body (McLaren, 2002). This research has employed a superficial approach to interpreting the meaning of postures, gestures and facial expressions (e.g., de Gelder et al., 2015) and children's bodily signals within an attachment relationship (e.g., Tsur, 2020). Therapy is represented as a ‘speaking’ profession, but there is limited research investigating therapeutic practice with girls using nonverbal forms of communication and their bodies to resist oppressive power relations.
Discursive therapies espouse collaborative ways of working with children and their families (White & Morgan, 2006). Discursive therapy includes solution-focused, collaborative and narrative therapies (Strong, 2016), and is characterised by the therapist being curious and suspending what they may know so they ‘can enter the world of the child’ (Gehart, 2007, p. 187). Discursive therapy literature underscores the importance of understanding children's nonverbal communication (Marsten et al., 2016). While discursive therapy espouses child-centred practice (Gehart, 2007; Marsten et al., 2016) and underscores the importance of exploring children's acts of resistance to oppression (Wade, 1997), there are messy realities when working with children and their caregivers, who may have conflicting versions of the presenting concern(s). Consequently, it is important to examine if and how discursive therapy is enacted in a power astute way.
Although research has focused on child-centred and age-appropriate ways therapists can engage with children (e.g., L. O’Reilly & Dolan, 2016), limited attention has been paid to their body language in therapy involving their caregiver(s). Furthermore, research has focused on how the therapist positions themself, with little account of how children physically respond within the context of the caregiver–child dyad. Research by Hung et al. (2019) examines both children's and practitioners’ spoken language and some gestures in therapy but does not fully examine children's unspoken forms of communication and what these might mean for power relations within therapy. Avdi (2015) has considered how discourse reinforces unequal power relations that impact children's participation in therapy when their caregivers and other family members are present. Yet the ‘girl body’ as a social entity within a sociocultural and physical context is often overlooked in therapy literature (Cameron & McDermott, 2007). This is of concern given the additional layers of sexist and gendered norms that girls and women are subject to.
The current paper foregrounds power and critically examines the role of girls’ bodies and their body language in the dyadic therapy encounter. Our intention is not to critique the therapy interaction, but to explore how and when girls communicate nonverbally using their bodies. Transcript excerpts from several video-recorded discursive therapy sessions are analysed. The discursive therapy sessions included two 9-year-old girls, Emily and Isla (pseudonyms), their caregivers and therapist in a private practice context. By employing critical discourse analysis (CDA), the reoccurring pattern of girls’ postures in therapy interactions is examined. This paper offers a needed contribution to poststructural feminist scholarship to investigate how power operates in therapy and how girls may be discursively (re)shaped by the encounter, but also to recognise and honour everyday forms of resistance.
Girls as neoliberal subjects and docile bodies
Feminist scholars have critiqued how girls are socially constructed as ‘ideal neoliberal subjects’ who are autonomous and empowered to self-improve (Rutherford, 2018; Scharff, 2016). Scharff (2016) demonstrates how societal discourses represent girls and young women as agentic subjects ‘who can lead responsibilized and self-managed lives through self-application and self-transformation’ (p. 217). While this empowered positioning focuses on girls’ agency, it also obscures ‘intensifying forms of governmentality’ of girls’ bodies (Scharff, 2016, p. 218). Moreover, increasing global inequality further reduces opportunities for many girls. Poststructural feminism has argued that inequality is not experienced the same by all girls, pointing to the need to explore different types of oppression which impact ‘in particular, women of colour, disabled women and queer women’ (Tseris, 2019, p. 30) .
Power is exercised through the female body via professional knowledge that enables the institutional regulation of girls via therapeutic intervention (Foucault, 1979; Hook, 2003). Tseris (2019), offering a feminist analysis of patriarchal expectations, illustrates how women who ‘act out femininity are given psychiatric diagnosis’, and those who ‘reject a conventional role’ are almost guaranteed a diagnostic label (p. 23). Therapy is an institutional site where gendered norms are inscribed onto girls and their bodies. In this patriarchal and neoliberal regime, girls who are deemed to be misbehaving and/or expressing intense feelings due to the distress they are experiencing are sent to therapy and positioned as ‘therapeutic subjects’ in need of behavioural modification, regulation and discipline (Foucault, 1979). Therapy, from this perspective, can be seen as an apparatus of disciplinary power (Hook, 2003) that inducts girls to be therapeutic subjects who self-surveil their emotions and bodies, reinforcing their positioning within the power–knowledge relations inherent in therapeutic practices (Roberts, 2005). Within the therapy room, biopower operates whereby girls become ‘docile bodies’ who are encouraged to comply with these gendered expectations, to self-discipline and self-regulate (Foucault, 1979). Hook (2003) argues that any therapy modality is a means for the client to engrave within themselves ‘a power relation in which they are the principle of their own subjection’ (p. 613). By ensuring girls’ compliance with such gendered norms, patriarchal and capitalist structures beyond the therapy room can be maintained. Applying a Foucauldian analysis, some feminist scholars point to these societal expectations and how they (re)produce docile bodies as well as pointing to ‘a locus of resistance’ (McLaren, 2002, p.86). Poststructural feminism argues that girls and women are constituted by psychological/psychiatric and neoliberal discourses and are, at times, able to negotiate and resist them (Tseris, 2019).
Girls’ body movement as everyday resistance
Girls’ body language and movement can be seen as a form of power and bodily resistance. There has been a growing interest in studying everyday resistance in sociology (Hollander & Einwohner, 2004) and other disciplines. Hollander and Einwohner's (2004) study of the typology of resistance identified that ‘authors seem to agree that resistance is not a quality of an actor or a state of being, but involves some active behaviour, whether verbal, cognitive, or physical’ (p. 538). Traditionally, resistance has been understood as collective and/or organised forms of political resistance to oppressive regimes (Hollander & Einwohner, 2004). Such acts of resistance, such as public campaigns, rallies or other forms of political protest, are easily visible. Similarly to Johansson and Vinthagen (2019), we define everyday resistance as ‘how people [in this case, girls] act in their everyday lives in ways that undermine power’ (p. 16). For Scott (1985), these forms of everyday resistance may not be initially visible to others but may be noticeable to those who are culturally and socially discerning. In fact, Scott (1985) refers to everyday resistance as infrapolitics, which means politics that are invisible. This highlights the importance of critically exploring girls’ body language in therapy as a potential example of everyday resistance.
While there has been some theoretical development in understanding children's physical interaction with their relational and physical spaces, therapeutic interactions with girls and their caregivers remain complex, with competing perspectives and enduring power relations within and beyond the therapy room. Practitioners offering therapy to girls face additional challenges when the caregiver arrives at the therapy room with a problem-saturated story about their child (Marsten et al., 2016; Reid & Brough, 2023). This paper makes a new contribution to the literature by proposing girls’ body language – specifically, their postures, gestures and movement – may be a form of everyday bodily resistance within the physical and relational space of therapy. This is distinct from previous research that has only understood children's body language as a form of communication. The question guiding our study is, ‘How might girls use body language as everyday resistance in therapeutic interactions when their caregivers are present?’
Methodology
This study adopted a poststructural methodology using a Foucauldian definition of power, which allowed a nuanced analysis of the ‘micro-physics’ (Foucault, 1979, p. x) of power relations in the microinstances of therapeutic interactions with children. Foucault (1991) argued that discourse is constituted by ‘the difference between what one could say correctly at one period (under the rules of grammar and logic) and what is actually said’ (p. 63). He points our attention to ‘what is possible to speak of’ within a specific time and place (Foucault, 1991, p. 59). These understandings of power and discourse are crucial for comprehending what girls are permitted to say in the microinstance of therapy. A Foucauldian analysis extends our understanding of how power can operate in our interactions with girls moving beyond a top-down hierarchical power relationship; instead, power is understood as ‘exercised through a net-like organisation’ (Foucault, 1980, p. 98). This framework enables the observation of power to recognise how children may use their bodies as a form of resistance to dominant discourses in therapy.
Fairclough's CDA (1989, 2003) is informed by Foucault's notions of discourse, power and knowledge. Fairclough (2003) provides analytical tools to examine discourse, not only the words spoken in the therapy interaction but also nonverbal forms of communication. According to Fairclough (2003), discourse operates in three significant ways through everyday social practices:
Discourses – how ideas, individuals, processes and objects are represented; Styles – the ways people perform preferred ways of being and epistemic truths; Genres – the ways people act and interact with one another through texts. (p. 26)
These elements combine to form interconnected meaning-making possibilities via spoken, written and nonverbal forms of communication in therapy. Styles, as an analytical tool, was of particular importance to the current study as the way we speak, gesture or position our bodies is a ‘discoursal aspect of ways of being’ in which identities are formed (Fairclough, 2003, p. 159). For Fairclough (2003), verbal and nonverbal forms of communication are ‘a matter of embodiment’ through which children and adults in the therapy room identify themselves and others (p. 159).
The sequence and repetition of utterances alongside gestures were investigated across the sessions. Both children’s recurrent gestures that had a ‘stable form meaning unit’ and that reoccurred across separate counselling contexts were identified (Ladewig, 2014, p. 1559). Girls’ body language was analysed in terms of its symbolic quality, the function it served within therapy and its ideological significance (Harrison, 2018; Kendon, 2004).
Method
A qualitative critical case study approach was enacted to investigate and richly describe ‘the exercise of power in culturally specific yet socially reproductive processes’ (Lather, 2001, p. 478). This case study allowed for nuanced observations of moment-to-moment interactions of all participants, rather than relying on adults providing their interpretations of the event via interviewing methods. In keeping with qualitative approaches, which favour depth of analysis over sample size (Patton, 2002), an intentionally small sample of two therapists enabled a fine-grained analysis. Purposeful sampling was used, via professional networks, to recruit practitioners who identified as offering discursive therapy to children and their families in Queensland, Australia. Practitioners were invited to participate based on their prior postgraduate training and professional supervision in discursive therapies, which included narrative, solution-focused and/or collaborative therapies. QUT Human Research Ethics Committee approval was obtained (Approval No. 1800001132). Two therapists volunteered: one therapist was based in a metropolitan area, and the other worked in a regional area. Both practitioners worked in private practices, held postgraduate qualifications, had extensive experience in working therapeutically with children and their families and provided supervision and discursive therapy training to other practitioners in the field. Both therapists mostly drew on narrative therapy in their work with children.
Recruited practitioners were asked to identify any child aged between 8 and 12 years who was a current client and was referred to them due to identified ‘mental health issues’ or ‘behavioural’ and/or ‘emotional concerns’. Information and consent procedures were used to invite, first, the caregiver's or legal guardian's consent to participate on behalf of the child, and second, the child's assent to participate. Each child assented before any research activities began. Everyday language was used in the consent forms. The two girls who participated in the study were both, coincidentally, 9-year-olds. In both cases, the caregiver was their biological mother, who had arranged counselling for them and attended the sessions with them. Kate, Emily's mother, arranged counselling for her due to behavioural concerns, including ‘whinging’, ‘crying’ and self-hatred. Sally, Isla's mother, organised counselling due to concerns regarding her ‘anger’, ‘screaming’ and negative self-talk.
Three or four therapy sessions with each girl were video recorded using an iPad installed in the counselling room prior to the commencement of each session. Seven sessions in total were featured in the study. For Emily, the three recorded sessions were her first three ones, whereas for Isla, the four recorded sessions occurred after she had already had three individual sessions without her caregiver being present. Each recorded session lasted approximately 1 hour. These recordings were subsequently transcribed, and the transcripts became the corpus for this study. Transcripts were de-identified to ensure the confidentiality of participants. Although Jeffersonian transcription conventions include descriptions of specific body language as it appears during interactions (Wetherell et al., 2001), an illustrator was commissioned to visually depict key postures observed throughout the sessions.
Using CDA, transcript excerpts across the seven sessions were selected for examination. Fairclough's three-tiered analytical process (1989) was employed to analyse the transcripts. The first stage, description, involved identifying the linguistic choices made by all participants, including how words were spoken and accompanying body language. The second stage, interpretation, deconstructed the social meanings of verbal and nonverbal cues within therapy, locating them in the wider sociocultural context. The final stage, explanation, drew on key theoretical perspectives to analyse participants’ verbal and nonverbal language choices, with a predominant focus on girls’ body language. To enable analytical rigour, one researcher undertook an initial analysis, which was then reviewed by a second researcher.
Throughout the process, we maintained a critically reflexive stance, recognising the importance of situating ourselves within the meaning-making and production of knowledge process (Brough et al., 2020, p. 513). We acknowledge that no data analysis is objective or neutral. As adult researchers (two social work and one psychology trained) wielding epistemological power, our interpretations may be complicit in shoring up the expertise of adults about children without the direct input of children themselves. Although the children in this study cannot confirm our analysis, we all bring a commitment to investigating the politics of therapy involving children.
Analysis
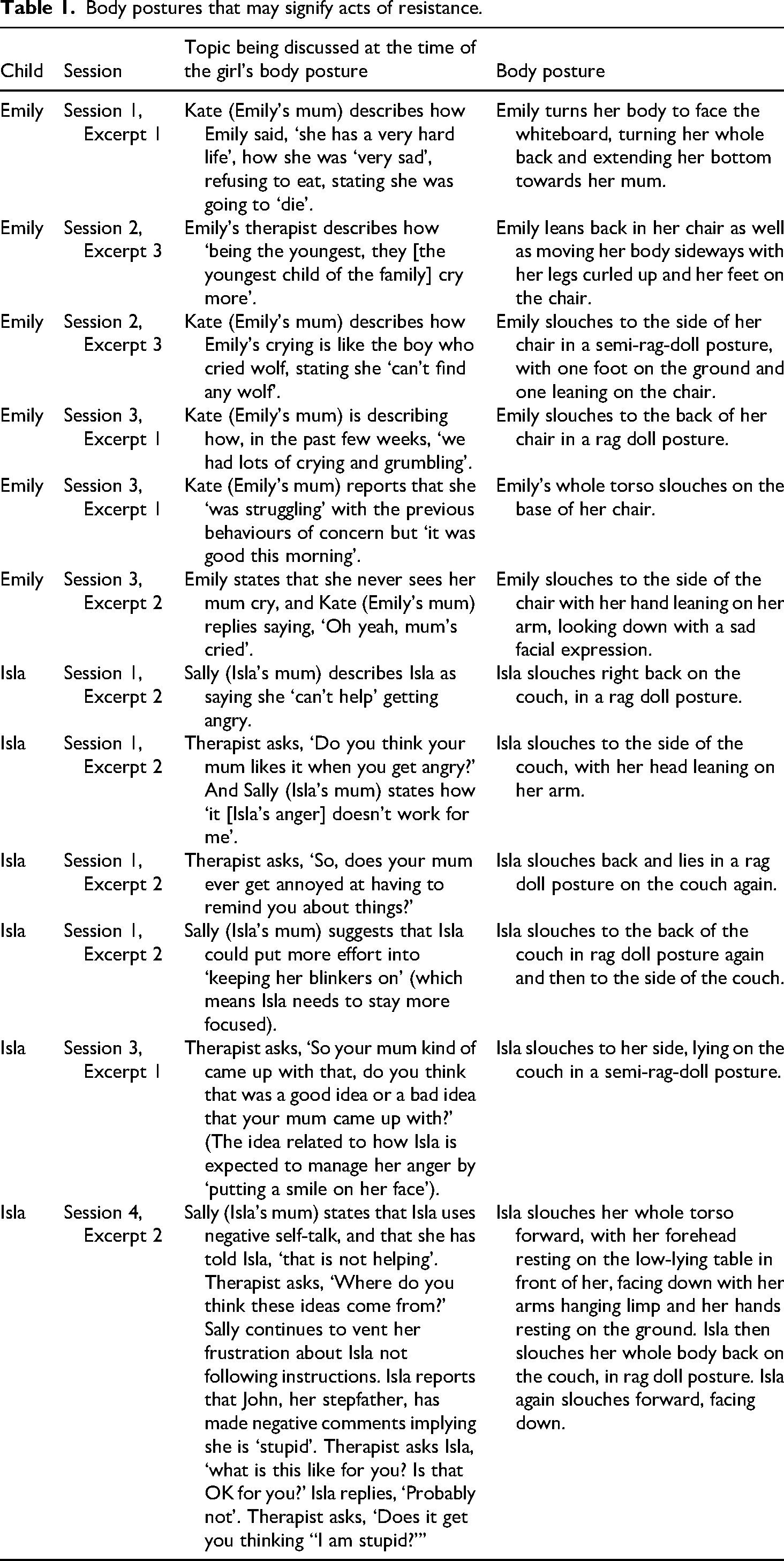
Our current findings show that girls’ body language can be understood as a corporal response to what caregivers and therapist have said, and to the topics being discussed. Table 1 illustrates Emily's and Isla's body postures that occurred in response to a variety of challenging topics being discussed in the therapy room, which may have negatively represented them, their behaviour and, consequently, their identity. It is important to note, however, that within the larger study conducted, there were a range of other findings that illustrate contrasting patterns of girls’ body language. There were, for example, instances of collaborative practice, with the child being positioned as an ‘informer’ and occasionally as a ‘knower’, and with the therapist asking questions in such a way as to consult the child regarding their understandings of what was occurring for them. In these interactions, both girls actively responded with their bodies, for example, by sitting up and picking up objects from the room, such as a whiteboard marker, to enact their agency and further voice their perspectives.
Body postures that may signify acts of resistance.
Bodily responses to deficit-focused stories about the child
Our study found that body language was a crucial semiotic resource used by the two girls to respond to problem-saturated stories retold about them by their caregivers in the therapeutic interaction. When caregivers were provided access to the conversational floor and spoke in a deficit-focused way about key events involving their daughters, and represented their behaviour in problematic ways, there was a clear pattern to Emily's and Isla's postures and gestures. These patterns involved both girls slouching back into the chair or leaning their body to the side of it. This posture was reminiscent of a rag doll due to their arms being limp at their sides, their neck partially tilted backwards and their gaze looking up to the ceiling or the side of the room. Figures 1 and 2 are key examples of this bodily response. In these moments of ‘rag doll posturing’, the adults were often in more upright and actively engaged postures, while the child was positioned as an observer to the conversation at hand.

Rag doll posture of the child.
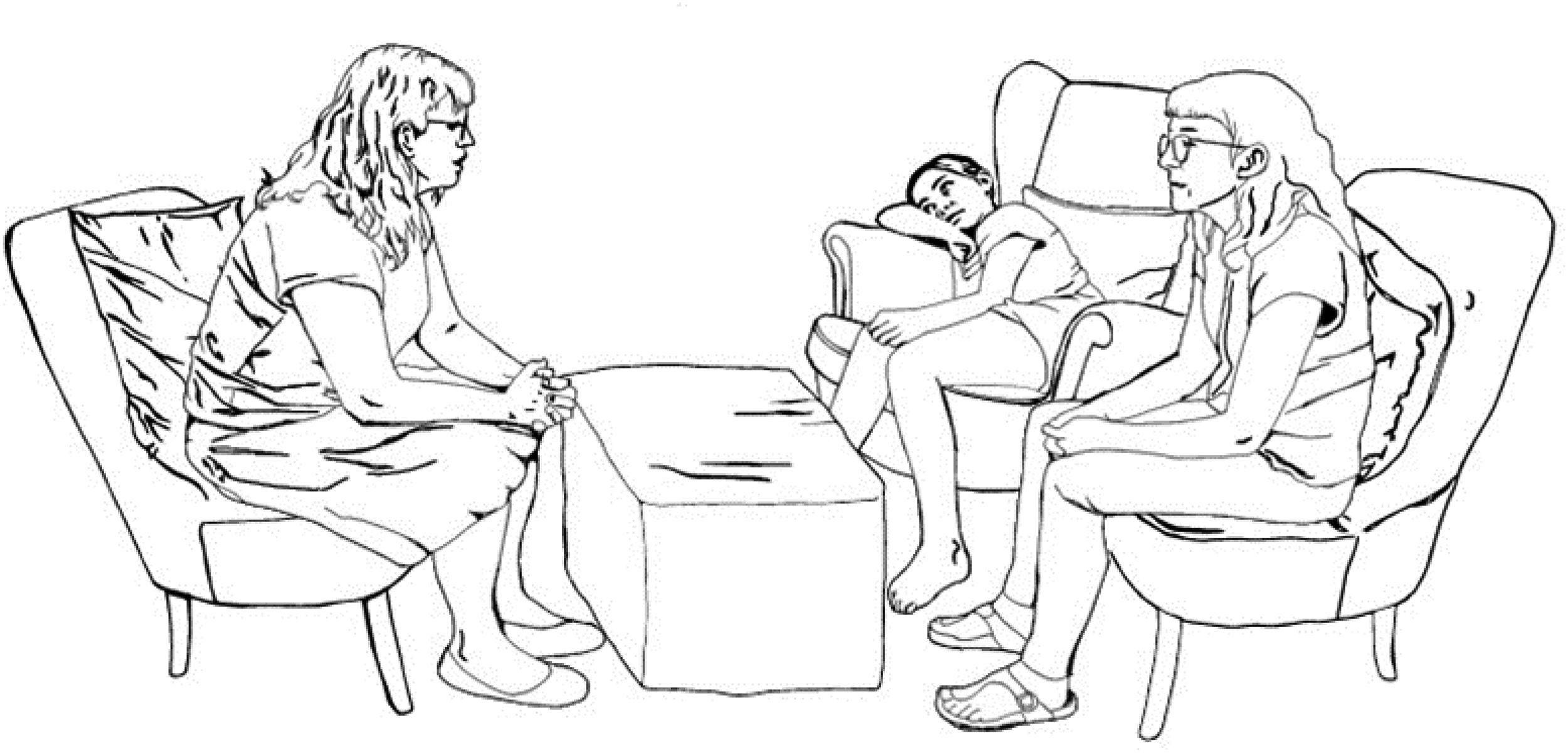
Semi-rag-doll posture of the child.
Both girls exhibited these rag doll and semi-rag-doll postures across all sessions. Although these postures may not be recognised as universal or ‘emblematic gestures’ (Harrison, 2018, p. 1) by the general public, such as a thumbs up or a wave might be, their significance and function cannot be underestimated within the therapy context. A recurrent gesture is defined by Ladewig (2014) as a ‘stable form-meaning unit [that] recurs in different contexts of use over different speakers in a particular speech community’ (pp. 1559–1560). These rag doll postures became prominent across the sessions because they ‘exhibit regularity in their form, organisation and function’ (Harrison, 2018, p. 1). It is noteworthy that when Emily and Isla resorted to these postures, neither girl spoke or verbalised any sound. Yet these silent postures may have served as significant communicative acts in response to deficit-focused narratives being retold about them by their caregivers. For example, Table 1 demonstrates how both Emily and Isla assumed a rag doll or semi-rag-doll posture by slouching back or to the side immediately after their caregiver made negative comments about their behaviour. This occurred in four out of the six examples of Emily's sessions, and three out of six examples involving Isla.
Girls’ gestures of negation
On initial inspection, these rag doll postures could be seen as children being positioned and positioning themselves as ‘docile bodies’, with Emily and Isla going limp, surrendering under the weight of the problem-saturated narrative. Such narratives were told by the caregivers in such a way as to identify the girls’ behaviour as needing to be modified, defining the girls as therapeutic subjects. Each postural example featured in Table 1 coincided with a dominant, deficit-fuelled story that constructed and reinforced negative identity conclusions about the girl and their purported behaviours of concern. In such moments during therapeutic interactions, both Emily and Isla bore witness to the negative accounts being told about them. These slouching postures could indicate Emily and Isla actively assuming the therapeutic subject position. Such a silent and passive positioning could also, however, be interpreted as an act of negation.
Gestures of negation can be defined as any posture or gesture that serves as semiotic resource to actively dismiss or reject the previous ideas presented in the interaction (Bressem, 2014). The function of these gestures or postures is to enable the child to disagree with what has been said. In responding in this way, the argument as such, is negated without directly opposing it. Gestures of negation are usually explicit. For example, a head shake is an easily recognised, conventional gesture of negation (Harrison, 2018). While practitioners drawing on discursive therapy may seek to consult children about their views and what matters to them (Marsten et al., 2016), children may not be afforded the conversational right or the discursive authority by their caregiver to explicitly disagree with authoritative statements asserted by them. Gestural research has demonstrated the connection between postures and utterances of negation, with acts of speech supporting the person's body language (Harrison, 2018; Kendon, 2004). In the current instance, though, the gesture alone speaks clearly of the girls’ active withdrawal from the therapeutic interaction. Such rag doll postures served a significant negating function and potentially called into question the ‘truth’ of the female caregiver’s statements. By physically withdrawing, the girls may be refusing to be complicit in such negative accounts being told about them.
Girls’ postures of protest
Another prominent reoccurring posture pattern was enacted by Isla in instances where the therapist asked questions in a way that inferred she was responsible for her problematic behaviour and its impacts. For example, Table 1 shows that five of the six examples featuring Isla assuming either a full rag doll or a semi-rag-doll posture directly after the therapist's question. Isla's full rag doll posture was observed in Session 1, Excerpt 2, when the therapist asks a question to invite Isla to consider how her behaviour is impacting Sally, her mother. This question appears to reinforce the dominant story that has been told about Isla and her ‘behaviours of concern’, including the potential inference that Isla herself is ‘the problem’. It appears Isla is slumping under the weight of this inferred negative identity construction. It is interesting to note that once such a deficit focus ceases in the interaction, Isla resumes her seated postures.
Isla seems to actively use her body to resist and even protest the idea that she is solely responsible for the situation. In Session 3, Isla again resorts to a semi-rag-doll posture, this time lying on her side when the therapist asks her to evaluate her mother's suggestion that she can manage her anger by ‘putting a smile on her face’. Despite the therapist trying to consult Isla about her mother's suggestion, Isla is identified as having an ‘anger problem’ in this therapeutic sequence. Isla's semi-rag-doll posture can be understood as an act of resistance, refusing to be solely responsible for her response to challenging events. Spiess (2016) states that ‘the linguistic utterance of protest manifests itself in different ways, and it can have diverse functions’, such as public protests, sit-ins or strikes (p. 344). The function of Isla's nonverbal ‘protest communication’ here can be likened to a strike, where one refuses to undertake one's usual conversational duties in the therapeutic interaction (Spiess, 2016, p. 343). Isla's refusal is also demonstrated by her absence of eye contact, by looking elsewhere in the room. Such a reoccurring pattern can be recognised as ‘postures of protest’, silently, yet symbolically, resisting being identified as the therapeutic subject.
Girls’ postures of protection
Unlike the recurrent gestures (Ladewig, 2014) of the semi-rag-doll or the full rag doll, Isla also demonstrated a ‘posture of protection’, particularly in Session 4, Excerpt 1. Figure 3 shows Isla sagging her whole body forward, with her arms again limp like a rag doll and her head facing the floor. This posture appears to offer Isla physical protection from discussing the negative comments her male step-caregiver has previously made about her. This posture is emblematic of a partial foetal position, which is universally recognised as the ‘bodily gesture of folding into oneself’ and understood as a means to seek comfort and security (Geurts, 2003, p. 365). Isla appears to be physically closing herself off from such hurtful things being retold, as an attempt to comfort herself. This posture, unlike other ones, also featured some speech acts of polite negation (Harrison, 2018). For example, when her therapist asks her, ‘What is this like for you? Is that OK for you?’ Isla replies, ‘Probably not’. The use of the word ‘probably’ demonstrated tentative modality to politely reevaluate yet not directly oppose her male step-caregiver's actions towards her. The partial foetal posture involves a total absence of eye contact and facial expression and appears to enable Isla to make visible how hurt she feels when she is spoken to in a way that infers she is ‘stupid’. Although Isla's actions are mostly silent in nature, this posture sent a powerful message to the adults in the room – that this way of being treated is not ok. Isla's mother responded by putting her hand on her back to console her. Despite the enduring power relations in the girls’ lives, there was a clear pattern of both girls engaging in postures to negate authoritative statements or questions made by adults to potentially protest and protect themselves from such deficit-focused discourses.

Isla's posture of protection.
Discussion
Discourse constitutes our everyday interactions, shaping what girls, in this case, are permitted to speak about in therapy (Foucault, 1991). This study's analysis brings attention to the complex typology of power relationships and the associated infrapolitics in therapy, in girls’ lives and beyond the walls of the therapy room. It shows how working with girls and their female caregivers is complicated, with competing tensions at work (Avdi, 2015). While discursive therapy modalities, such as narrative therapy, espouse collaborative approaches when working with children and their families (Marsten et al., 2016), therapists offering girls’ access to the conversational floor is not enough to respond to these largely invisible power relations within the family context. Despite the therapists’ attempts to work collaboratively and invite their voices, it was evident that the girls, in these moments, were not authorised to directly call into question their caregivers’ version of the ‘truth’. This aligns with Scott's work (1985) that explains that open defiance is not possible for many individuals, especially for girls and women, where disagreement could be easily interpreted as unacceptable defiance, leading to negative repercussions (Tseris, 2019).
Consequently, it appears that the girls utilised their bodies as a discoursal resource to engage in silent forms of everyday resistance, to negate and resist the deficit-fuelled stories told by their caregivers, to challenge the status quo and associated power relations (Kallio & Honkatukia, 2022). While we did not have access to the girls’ internal world, it would appear that they subtly, yet influentially, resisted institutional practices such as therapeutic questioning that, at times, reinforced girls’ problematic identities. Foucault explains, ‘(t)here is not one but many silences, and they are an integral part of the strategies that underlie and permeate discourses’ (Foucault, 1979, p. 27). Girls’ body language in the current study, however, is recognised as powerful acts of everyday bodily resistance to dominant discourses, with key postures of negation, protest and protection silently speaking the unspeakable.
Foucault (1991) explored how docile bodies learn to self-manage their behaviours, yet in this process of ‘self-mastery’ of their identified behaviours of concern, the individual loses control by adhering to societal expectations. After closer observational analysis of reoccurring patterns of posture across all sessions, the two girls can be seen as social agents, as rebels who used their bodies to communicate matters of concern. Such postures inadvertently contested ‘objectionable talk’ (Strong & Tomm, 2007) and specific ideologies, such as the notion that girls need to self-regulate their emotions regardless of their potentially oppressive sociocultural circumstances (Reid, 2024; Reid & Tseris, 2025). By closely observing the body language in the therapy room, each girl's postures in response to deficit-fuelled interactions exposed the infrapolitics at work in the therapy room.
As Scott (1985) notes, the nuance of such infrapolitics can, however, be invisible to some and therefore, easily disregarded given that both girls did not explicitly or directly opposed the adults in the room with acts of verbal protest. The absence of such visible and confrontational forms of protest points to the constraining social, relational and cultural realities and associated power imbalances that girls are constantly navigating. In seeking to understand the infrapolitics of girls’ bodily resistance, we recognised that their gestures may have communicated a political stand on important issues that impact their mental health. While not collective and coordinated, like public rallies or political protests (Hollander & Einwohner, 2004), these individual acts of nonverbal protest served as signifiers (somewhat like a placard), silently stating their personal ethics and counter-political slogans in the face of powerful individualising discourses. Further recognition of girls’ bodily resistance to neoliberal and psychologising discourses that position them as docile bodies is needed.
Practitioners need to resist arriving too quickly at ‘common sense’ interpretations of girls’ gestural communicative practices, or worse, dismiss these acts as either inconsequential or distractions to the ‘real work’ of therapy. Rather, we need to be curious about girls’ nonverbal gestures and postures and coexplore their potential meaning with them. While it is tempting for practitioners to invite the child to engage in verbal dialogue about the potential meanings of their body language, girls may be unwilling or unable to enter such dialogue. Tension lies in the practitioner's desire for further understanding while also recognising therapy may be unsafe. This fear is not new to women and girls. It is well established that therapy was a tool of repression in the 20th century, albeit there are different forms of therapy, therapy, however, continues, at times, to be harmful for women and girls (Marsden et al., 2021). Regardless of discursive therapies’ commitment to socially just ways of working with children and to distance from the psy-complex, its legacy can unwittingly continue to permeate therapeutic interactions, impacting girls’ sense of safety (Reynolds, 2012). We can, however, start by being cognisant that girls may not feel safe, empowered or positioned to speak in therapy because of the matrix of power operating through therapeutic discourses. Silent gestures, in this context, are not merely a lack of voice but can be understood as a strategic and meaningful form of resistance that disrupts the expectation of verbal expression as the primary mode of communication.
We question – what might be made possible if practitioners drew on this notion of bodily resistance in the therapeutic space with girls? If relating verbally might be unsafe, how might we instead value the body. As Coole (2007) explains, ‘the body’ itself enacts agency to communicate ‘a corporeal mode of knowing … which provides discourse with an ineliminable sub-text’ (p. 416). By drawing on poststructural theory, we as practitioners have an opportunity to interrogate the discursive conditions that make certain forms of expression legible or illegible, and to remain open to the multiplicity of meanings that silent gestures might carry – without imposing a need for verbal confirmation. Practitioners can be allies in the therapy room, working on behalf of girls to both amplify and advocate for often silent acts of resistance against the dominant narrative of the ‘problem child’ that pervades families and society. For example, practitioners could recognise such bodily gestures as a signal to disrupt the current conversation. This would involve practitioners actively facilitating the conversation away from deficit-focused and individualising discourses, to find ways to challenge the taken-for-granted neoliberal and patriarchal expectations regarding girls self-regulating intensive emotions irrespective of oppressive sociocultural forces impacting their lives.
Therapy needs to be a safe place to explore intersecting systemic and structural challenges potentially facing girls globally, including rising social inequality, domestic and family violence and child abuse (Reid, 2024; Reid & Tseris 2025). By noticing potential examples of girls’ everyday forms of resistance, we may work with them to ‘disentangle interlocking systems of power and oppression’ (Bell, 2022, p. 132). This could involve coexploring with girls (where appropriate and safe) how they are responding to such oppressive circumstances in their lives, and to honour and make visible their everyday acts of resistance beyond the therapy room.
Girls, however, need to be provided with a range of therapeutic resources in order to make sense of their challenges and to make visible their everyday forms of resistance. Girls’ nonverbal reflections can be scaffolded in therapeutic interactions by asking contextualising questions, providing images and offering materials that enable them to imagine, draw and write about their politics of experience (Reid, 2024; Reid & Brough, 2023). Girls need to be offered diverse options for how they might prefer to physically interact in a therapy room. These options need to be conveyed to caregivers to avoid the policing of girls who interact with objects in the therapy room and the associated bodily control (Kallio & Honkatukia, 2022). Being discerning and ‘body cognizant’ practitioners (Cameron & McDermott, 2007, p. 87) means we need to deepen our understanding of how girls use their bodies to navigate the matrix of power in their lives, to enable them to continue to enact these acts of everyday resistance. Comfortable furnishings and colourful and playful objects, however, are insufficient to avoid children being corralled into institutional bodily control. If therapists are to do justice to the well-recognised concept of child-centred practice, we need to go beyond superficial understandings of ‘child-friendly’ environments. Recognising and responding to girls’ everyday silent forms of resistance in therapy is, however, inadequate to achieve social justice for them. It is vital for feminist practitioners to be ‘circumspect when articulating the capacity of therapy to address unequal power arrangements rather than assuming its benevolent and empowering role in children's lives’ (Reid & Tseris, 2025, p. 16). Child-centred practice from this perspective also involves respecting that girls may choose not to participate in therapy as the ultimate form of resistance available to them.
Conclusion
Girls in most Western countries are being referred to therapy at increasing rates (Udwin et al., 2021). This study underscores the need for therapists to develop an astute recognition and appreciation of the role that girls’ body language may play in therapeutic interaction, to understand their attempts to call attention to the issues that matter to them. The findings demonstrate how child-centred practice needs to expand to incorporate a nuanced power analysis whereby girls’ everyday acts of resistance can be recognised as potential acts of rebellion against being held individually responsible for the challenges they face. Moreover, we need to recognise that girls’ agency is entangled with their local environments and complex sociopolitical realities. Unless therapists bring an expanded understanding to child-centred practice, recognising the subtle yet influential politics in the therapy encounter, we risk accommodating girls to the oppressive challenges they face, ultimately undermining their emotional well-being. To enable girls a voice on the matters that undermine or support their well-being, therapists need to recognise how girls are finding safe and nonverbal ways to speak the unspeakable using their bodies.
Footnotes
Acknowledgements
The authors would like to acknowledge both Professor Mark Brough from Queensland University of Technology and Alex Olsen for being critical friends and reviewing an earlier draft of this article.
Ethical approval and informed consent statement
This study was approved by QUT Human Research Ethics Committee, and all participants were provided with project information for informed consent or assent (in the case of the two girls who participated).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.