
Abstract
Between 1983 and 2018, approximately 170,000 people journeyed abroad to access abortions outside Ireland due to Ireland having one of the most restrictive abortion laws in the world. This paper analyses the lived experience of people who made such journeys, contributing to the literature on restricted abortion access and forced abortion travel. Six in-depth interviews were analysed using interpretative phenomenological analysis (IPA). Three master themes were developed. Master Theme 1 speaks to the burden of concealing the experience, and the fear of being discovered and punished that drove the concealment. Master Theme 2 gives insight into overlapping and interwoven challenges of having to leave one's country to access abortion services: lack of access to information, financial burdens, being forced to remain pregnant after making the decision to end that pregnancy, and the impact of all of this against the backdrop of the crisis of unwanted pregnancy. Master Theme 3 speaks to the processing and meaning-making of the journey; how coming into contact with others who had similar stories informed a more compassionate lens on their own stories, and inspired participants, to varying degrees, to become active in the struggle to make Ireland's abortion legislation less restrictive.
Keywords
Abortion is a safe procedure in relation to physical health (Cleland & Smith, 2015) and psychological health. Consistently, when confounding variables are controlled for, the risk of developing psychological difficulties after abortion are no greater than those with delivery of the pregnancy (American Psychological Association Task Force on Mental Health and Abortion, 2008; Charles et al., 2008; Major et al., 2009; National Collaborating Centre for Medical Health, 2011). Nonetheless, abortion is subject to specific regulations in many jurisdictions (e.g., De Costa & Douglas, 2015), and in some is (or has been) severely restricted (e.g., Bloomer & O’Dowd, 2014; Hirvonen, 2017; Ona Singer, 2020). The consequences of restricted abortion access are either self-management without medical supervision (Aiken et al., 2019; Broussard, 2020; Garnsey et al., 2021); unsafe abortions by unqualified providers (e.g., Aiken et al., 2019; Okonofua et al., 1999; Sunil, 2022); or travelling to another jurisdiction, sometimes referred to as abortion “tourism” (e.g., Bloomer & O’Dowd, 2014; De Costa & Douglas, 2015; Gilmartin & White, 2011; Hirvonen, 2017). This term (tourism) is disputed because those who travel for abortion are not actively choosing this option—rather, they are forced to travel (Inhorn & Patrizio, 2009; Kelly & Tuszynski, 2016; Ona Singer, 2020).
Previous research shows that forced abortion travel is associated with financial, logistical, and emotional burdens (Kimport & Rasidjan, 2023). Yet, it tends not to encompass the experience of both unwanted pregnancy and forced travel in combination. In this study, we qualitatively examine the combination of these two experiences in a sample of women who travelled to terminate at a time when abortion was illegal in Ireland except to save the life of the pregnant woman.
Background
Existing research on unwanted pregnancy focuses largely on the conditions that make it unwanted, or unsupported and unsupportable (Macleod, 2016, 2019), for example, bad timing, difficult financial conditions, and wanting to continue with education (Okonofua et al., 1999; Oye-Adeniran et al., 2004). Frequently, relational themes appear in a person's decision not to continue a pregnancy, for example, a partner being unable or unwilling to support the pregnancy, undesirable characteristics in a partner, having a poor or absent relationship, or violence in the relationship (Chibber et al., 2014). A limited amount of research examines the experience of discovering an unwanted pregnancy, particularly in a restricted context (e.g., Tatum et al., 2012), or explores women's accounts of their decision-making in such contexts (e.g., Chiweshe et al., 2017).
Context is highly relevant to considerations of women's experiences, because, as noted above, severe restrictions on abortion may make the only available options self-management of abortion without medical supervision (Aiken et al., 2019); unsafe, clandestine abortions (Aiken et al., 2019; Mohamed et al., 2018; Nara et al., 2019; Okonofua et al., 1999; Sunil, 2022); or forced abortion travel (Kimport, 2022; Kimport & Rasidjan, 2023; Ona Singer, 2020). For the latter, mobility has disproportionate negative effects on those who are already disadvantaged (Bloomer & O’Dowd, 2014; Freeman, 2017), being restricted to those who can afford to travel and indeed are legally allowed to travel (Engle, 2022; Gilmartin & White, 2011).
Even for those who can travel, the experience of having to do so may be difficult. The limited amount of existing research shows that the farther women have to travel (either domestically or internationally) for abortion, the less likely they are to procure one (Sethna & Doull, 2012); that women may be past gestational limits and thus refused the procedure by the time they present to services (Gerdts et al., 2016; Ona Singer, 2020); or that they may require surgical rather than medical abortion because of an inability to return for follow-up appointments (Ona Singer, 2020). Research also shows that there are emotional costs associated with having to travel for abortion care, because of (a) having to disclose the abortion due to the need to travel; (b) being in an unfamiliar place with people unknown; and (c) feelings of shame, exclusion, and being abnormal for having to go outside of one's own state to access abortion care (Kimport & Rasidjan, 2023).
Indeed, restrictions on abortion, which impact who can access it, are an extension of a more general stigma related to abortion (Aiken et al., 2018, 2019; Msetfi et al., 2018; O’Donnell et al., 2018) and voluntary childlessness (Szekeres et al., 2023), and indeed women's sexuality (Mohamed et al., 2018). Stigma refers to the social devaluing of a person based on a specific trait or characteristic (Goffman, 1968). Stigma relating to sexuality and abortion are socially constructed and thus contextual, relying on power disparities and inequalities (Kumar et al., 2009). As such, the context determines not only who is structurally disadvantaged to gaining access to abortion (Katz, 2017) but also who is considered worthy of empathy (Kimport et al., 2016). These aspects are likely to deeply affect women's experiences. Few studies have examined the lived experiences of people who experienced unwanted pregnancy (however, see Nor et al., 2019; Sunil, 2022) and were forced to travel for abortion services, hence the focus of the present study.
The current research
Prior to May 2018, Bunreacht na hÉireann (Constitution of Ireland, 1937) contained an amendment (Eighth Amendment of the Constitution Act, 1983) that granted the equal right to life to mother and the “unborn.” This gave Ireland one of the most restrictive abortion legislations in the world. A further amendment to the Constitution (Thirteenth Amendment of the Constitution Act, 1992) ruled that the 1983 amendment could not prevent people from travelling to access abortion services outside of the State's borders. In the context of this legislation, residents accessed abortions abroad or used abortion medications which they ordered online (Aiken et al., 2018).
Further to another referendum on May 25, 2018, the 36th amendment to the constitution was passed, which removed the eighth amendment, and allowed for provision to be made in law for the termination of pregnancy. The subsequently passed Termination of Pregnancy Act (2018) allows for abortions up until 12 weeks of gestation and, under very limited conditions, permits abortions beyond 12 weeks of gestation. Prior to this, the State prohibited most people from having abortions in Ireland, with the threat of a 14-year prison term (Sheldon, 2016), although people were able to travel to access abortions abroad, thus providing an interesting context in which to study the impact of unwanted pregnancy and forced abortion travel.
To understand women's experiences in such circumstances, we used the power threat meaning framework (Johnstone & Boyle, 2018), focusing on (a) the power structures within which women were operating, (b) what they felt they had to do to survive within this context, and (c) the meaning they took from these experiences. This framework, along with our phenomenological approach, allowed us to orient to women's accounts and meaning-making around their own experiences, while situating their and our interpretations within the social context they lived in.
To the best of our knowledge, this is the first study to apply a phenomenological approach to the experience of travelling to access abortion abroad. The study approached abortion as a process rather than a single event and attempted to capture participants’ meaning-making at each stage of the process.
Method
The current study sought to explore the experience of having to leave one's country to access abortion care in the context of restrictive legislation. The first author interviewed participants who lived in Ireland, and data were collected in the months following the referendum which legalised abortion. Those who took part had therefore travelled for abortions prior to the change in the law. Interpretative phenomenological analysis (IPA) was used, as it draws upon phenomenology, hermeneutics, and idiography (Pietkiewicz & Smith, 2014). Phenomenology encourages the exploration of the components which make a given phenomenon unique. It encourages a focus on how people perceive and speak about a given event, whilst hermeneutic studies require the researcher to stand in the shoes of participants, with the awareness that it is not possible to gain full insight into the experience of the other (Johnstone & Boyle, 2018). IPA is double hermeneutic; it requires participants to make meaning of an event and for the researcher to make sense of participants’ meaning (Smith & Osborn, 2008). Idiography involves an in-depth analysis of the participants’ perspectives, in their unique contexts (Pietkiewicz & Smith, 2014).
IPA studies conduct case-by-case in-depth analysis on small sample sizes to gain insights into the experiences of individual participants (Smith & Osborn, 2008). This labour-intensive method of interacting with data can be viewed as one limitation of IPA. It requires significant organisation, time, and supervision (Pietkiewicz & Smith, 2014). By employing small sample sizes, this technique allows researchers to explore the experience in depth. IPA was the best fit for the research questions in this study, as it allowed researchers to approach a particular phenomenon and explore how people experienced it, while engaging reflexively with the data collected.
Using semistructured interviews allows sufficient flexibility to establish rapport and then access, insofar as possible, participants’ inner emotional and social landscape (Smith & Osborn, 2008). Consistent with this approach, Callary et al. (2015) recommended the use of open-ended questions and prompts where appropriate to explore participants’ experiences in detail. Our interview schedule, developed in conjunction with psychotherapists and academic supervisors, followed this advice and attended to the person's emotional experience at each part of their story: how they experienced the pregnancy and how they managed the journey. The schedule also attended to how they felt society responded to stories like theirs at the time.
Piloting and participants
The study was advertised through social media. Two pilot interviews were conducted, generating useful feedback and insights into how participants engaged with the interview schedule. For example, having more structure to questioning was identified as useful to support their storytelling. For the next pilot, each question was asked in temporal order. Six people were interviewed (consistent with advice from Turpin et al., 1997), aged between 27 and 47. Five of the women were Irish citizens, and one was a U.K. citizen resident in Ireland. See Table 1 for participant demographics.
Participant demographics.
Note. Pseudonyms are used for all participants.
Ethical considerations
Ethical approval was received from the University of Galway Research Ethics Committee (Ref. 18-Sept-10). Participants gave written consent before commencing the interview and provided demographic information.
Approach to analysis
IPA seeks to develop an understanding of participants’ meaning-making of an experience and to develop an awareness of the content and complexities of respective contexts. As such, the researcher is an active agent in the interpretation of each transcript (Smith & Osborn, 2008). Convergence and divergence of participants’ experiences were explored through the detailed case-by-case analysis of each transcript (Smith & Osborn, 2008). Engward and Goldspink (2020, p. 42) refer to data as “lodgers” because of the way in which the researcher finds herself “living with the words of her participants, and noted the ways in which the lodgers were living with her, in her reflexive experience.” Engward and Goldspink (2020) proposed the following six-step process listed in Table 2 for analysis.
Amended six steps of IPA and building a relationship with the data.
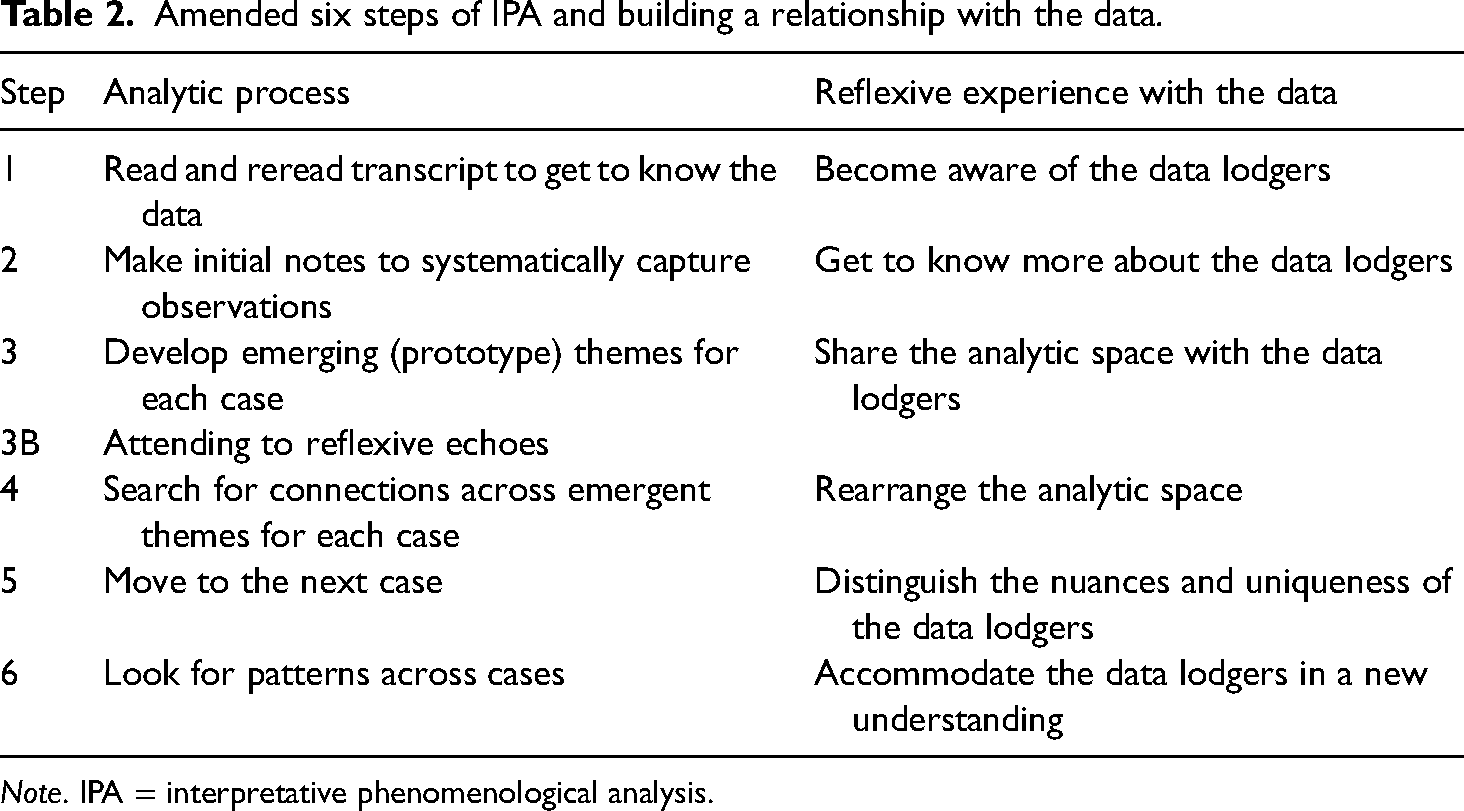
Note. IPA = interpretative phenomenological analysis.
Analysis
We developed three master themes. Master Theme 1 portrays the burden of concealing the experience, and the fear of being discovered and punished which drove the concealment. Master Theme 2 indicates the overlapping and interwoven challenges of having to leave one's country to access abortion services: lack of access to information, financial burdens, being forced to remain pregnant after making the decision to end the pregnancy, and the impact of all of this against the backdrop of the crisis of unwanted pregnancy. Master Theme 3 shows the processing and meaning-making of the journey; how coming into contact with others who had similar stories informed a more compassionate lens on their own stories and inspired participants, to varying degrees, to become active in the struggle to make Ireland's abortion legislation less restrictive. We used subthemes to allow us to show the richness and variation within each master theme, as shown below.
Master Theme 1: My primary concern was “how do I lie about this?”
This theme addresses the secrecy and shame associated with experiencing unwanted pregnancy in a society where abortion was illegal and viewed as immoral, coupled with a lack of abortion access and aftercare. Participants were unsure whether to confide in friends, family, or healthcare providers, fearing judgment, denial of care, or punishment.
Subtheme 1.1: “Everything you do now is a f***ing secret”
Participants reported significant stress from concealing their travel plans, including anxiety about family, friends, workplaces, and healthcare providers finding out. They experienced loneliness due to feeling sick and not being able to tell anyone. Anne observed early in the process that this “was just something I knew I would have to keep quiet about really.” Similarly, Sharon reported: I was feeling all the symptoms of being pregnant but I couldn’t say anything or do anything about it … I just had to get on and get over it … My mood had dropped and I was getting a bit touchy … I think I just found that tough … I knew I was pregnant, and this was the reason I was like that but … I couldn’t tell anybody else so that was probably the hardest. I had that in my head that someone would put two and two together … I think all of the arrangements that you have to make just contribute to this sense that everything you do now is a f***ing secret.
Participants feared that being discovered would have been a shameful experience or would have had a detrimental impact on their relationships. Grace noted that she couldn’t “turn on the phone, you can’t have anyone know where you are, you basically have to drop off the planet for Friday 4:00 am until midnight.” Sarah and Sharon also mentioned the fear of being called by family and getting “the foreign dial tone” and not being able to explain where they were. In the aftermath of the journey, Sarah: “went through and deleted every trace of ever having gone there and that's why I don’t know where we flew to … because of the secrecy, I don’t remember ever doing that.”
Grace summarised the impact of having to conceal this journey: If you want to hide it, it's so much f***ing easier when you are not getting on an aeroplane. When you are not in another country and hiding the fact that you are in another country. It just exacerbated it so much. His mum had found my pregnancy tests and she found out … I didn’t want any of his family knowing … he is like “oh I can’t talk right now, I’m busy,” and it was because he was comforting his mum. I don’t think I was as supported as I would like somebody to be … But I didn’t have to be keeping secrets from people close to me … I’m not Irish and I have never been Catholic. I think I have much less of a sense of guilt or shame … an Irish Catholic woman of my age would have a lot more baggage to undo to be able to take that decision, I think … and probably a lot more secrecy as well because of family and friends … I have no family that would have been anti-abortion. It was up to me to kind of organise stuff … I wanted to talk about it … I had so much to say and I just … I was confused, I was scared, and he didn’t bring it up and when I tried to bring it up, he wouldn’t talk to me about it.
Subtheme 1.2: “I don’t want to be stopped or get in trouble”
Participants discussed going against cultural norms about abortion and challenges in accessing support. Ciara felt uncertainty about legal implications, compounded by a practitioner's unwillingness to provide direct information on abortion services: It felt very cloak and dagger and like I didn’t even know if I could go to my GP … “what if they stop me … I don’t want to be stopped or get in trouble” … I cried because … like the country … the government were like not even letting people have leaflets about things like, she could lose her licence, like the clinic would get in trouble for giving out a leaflet for people to … I mean … like even ringing I was scared … I thought like they would have to report it or something.
Grace felt the stigma around abortion so strongly that, when she attended the clinic, she “couldn’t actually say to them ‘I need an abortion’, I had to phrase it like ‘I need to not be pregnant!’” Anne noted that she was surprised by how kind the nurses in the clinic were: “I suppose I expected those horrible nun types, like ‘and look what you did!,’ ‘only yourself to blame!’”
Uncertainty regarding the healthcare system's postabortion attitudes meant Julia was unsure whether she could call her GP for help: “I was still bleeding 3 weeks later … if I had been in a clinic in Dublin, I would have had the phone number to ring up.” Grace became very unwell afterwards and was rushed to the hospital, but her main concern was trying to explain her emergency without anyone finding out: “I had a postabortive infection. I was septic … my primary concern was ‘how do I lie about this? How do I make up a story as to why I am in hospital for 4 days?’” Grace also felt profoundly shocked and relieved by the professional response of the case team: “They didn’t seem surprised that I had a postabortive infection. They didn’t seem like it was anything new to them. And that really surprised me.”
Another aspect to this was how alone the women felt. Sharon remarked that: “I did think I was alone, I did think I was the girl that made this decision, that nobody makes this decision.” Grace attributed this to “that shame and guilt that is indoctrinated in us and it comes through generations.” At that time, she didn’t know anyone that had divulged having had an abortion: “It was very much like you’re going so far outside the norm. This is so socially unacceptable what you are doing.” By contrast, Anne was aware that “a few of my friends had had abortions … I knew that there would be some people that didn’t judge me and would understand the decision.”
Knowing someone who had made the journey served a protective function; however, without this, others still sought support from those they were closest to. For example, Sharon asked her best friend, who was morally opposed to abortion, for help. She remarked that “I knew her views on it. But I had no one else to kind of turn to.”
Participants sometimes experienced shame and stigmatisation in close relationships. Ciara described her partner's reaction: “I was blamed completely for it, like it was, especially afterwards … when I got back from England, I got … like he blamed me a lot … eh…. Yeah, he said like I killed a baby.” Anne's best friend was supportive but “she was completely against it.” Sharon stated that the man she had been dating felt so afraid to be seen near the clinic that “he wouldn’t even sit outside it because of the name.”
Participants worried about the social impact of being found out. Anne worked in a Catholic school, and she was anxious about her work finding out: I just remember thinking, “God if only they knew, I would get fired, and if they knew, they would just be horrified.” It's very conservative environment and you know, they would have had people in talking about, you know, the ones that give out the little baby feet and that kind of thing, and what a sin it was, and there had never been any unmarried mothers or anything. I certainly didn’t feel it was an environment where I would be an unmarried mother … or tell people … I would have definitely known and been very aware that I was doing something that most people believed was wrong. Really wrong.
Sarah both expected and experienced protestors at the clinic, which compounded her distress: “There were three old men with rosary beads and placards and yeah … I remember walking past them and they were just shouting and stuff, it was terrible.” Anne described her friend as being very supportive through a similar experience: “She picked me up from the clinic … she hid me from the protesters.”
Master Theme 2: “That's a bit horrible to do to somebody in a crisis”
This theme summarises specific difficulties participants encountered due to having to travel to access healthcare, including inaccessibility of information, costs, and debts. They experienced delays and distress at remaining pregnant long after they had decided to terminate. Participants described being away from the comfort of home, staying in hotel rooms with no privacy, waiting in clinics and airports, and complications from having to take a flight or ferry home postsurgery.
Subtheme 2.1: “Being sent through hoops on purpose”
Navigating having an abortion overseas was difficult for participants. Sarah described the experience as being “sent through hoops on purpose.” Finding information was a challenge in the first instance. Anne spoke about the lack of access to “mobile phone, computers, smartphones, or anything … I went to the library … and I was googling abortion clinics.” Grace described it as: being lost in an airport and you can’t read any of the signs … Like I’m out of my depth, I’m so out of my comfort zone, I don’t know my way around, I can’t do this on my own, it's, it was just, it made me angry and it made me terrified all at the same time.
Subtheme 2.2: “You don’t have that kind of money”
The cost of the journey was a considerable burden. Sarah stated she “would live really frugally, I have a credit phone … so to ring the UK to set up the appointment, that's 20 euro gone straight away … it just starts to become a money thing.” Most participants had to borrow money. Ciara had to tell her mother what was happening “because she loaned me the money for it … that was hard as well because I … we don’t have the best relationship and I don’t like the idea of having to borrow a sum of money from someone.” For Sharon and her partner, “it was using friends’ credit cards to book flights, it was taking out a loan to travel.” Julia calculated: the equivalent of nearly a grand now … that's an awful lot of money … but it was all the extra expense and that extra time and the complications that arose, and I had somebody else look after my child for 3 days.
The costs increased due to time pressures on participants: Sarah noted that even booking the flight: “you’re trying to see what's not 260 euro, you know, cos there are 70 quid flights … so all out of your control.” For Grace, pain relief for the procedure came at a cost: “They gave me an option of 400 euro or 430 euro for with anaesthetic, so I went with anaesthetic.” Anne found the experience less harrowing due to an accessible clinic and a friend to look after her in the UK: “I was grateful that I had the money, that I had a friend in Manchester, that I had the clinic around the corner, you know.”
Participants also navigated work environments, needing time to call clinics, book appointments, and attend compulsory ultrasounds beforehand. Sarah worked “12-hour shifts, so I definitely would have taken a day off work, an entire day off work just to go, just to make that appointment.” Julia described the longer term impact: It's going to take you 3 times longer to pay off this money that you borrowed or to make up the overtime, or you know, do the bits of favours, the sleepovers back and you know, all this kind of thing. So, I guess I’d be a little bit bitter about the fact because it's needless, it's just adding … it's piling on the difficulty…. A huge amount of extra burden that is kind of needless extra on somebody who is, I mean, if it cost money, it cost money, if it takes time, it takes time, and that's a bit horrible to do to somebody in a crisis. 800 euro we had to take for a loan from the credit union, I just … it was hard even to pay that back because we just didn’t have the money. You’re 23, you don’t have that kind of money. I’m very well aware it's a class issue and you know, I’m privileged in that I can surpass some of those barriers in a way that there are definitely women who can’t … if you’ve got access to money and can put on the right accent, and the right voice, and the right clothes and you know … it wasn’t easy, it was difficult, it was just possible.
Subtheme 2.3: “An avoidable wait”
The referral process also caused delays. Sarah described the experience of carrying an unwanted pregnancy while awaiting a requested abortion: You’ve this protracted process that you need to go through just to do it, like, I mean, it did take 6 weeks … by the time that you actually get to go and do this thing you’re well pregnant, it's not a missed period anymore like, it's big. It's a much bigger deal, especially for someone who doesn’t ever want to be pregnant, that's an horrific thing.
Once Ciara had made her mind up, she had to wait a month for her appointment: “So, like I’d sit there … Floating … sit there like, had to deal with that for a month, being like ‘I’m pregnant right now … there is something growing inside me, this … child I don’t want.’” The physical impact was also discussed by Julia: Once you have decided that you want to have a termination, you’re still carrying this, this foetus that is giving you heartburn or causing you to have to go to the toilet all the time and causing you not to be able to take the medication for other things that you need to take.
Grace recalled feeling so awful waiting for the termination that she “spent those 3 weeks trying to smoke and drink myself into a natural miscarriage.” This was the worst aspect of the experience for Sarah: “what was traumatic for me was actually the length of time it took me to access the service, that was literally it.”
Having to wait for appointments and travel to another country meant Julia and Ciara were close to gestational limits 1 by the time they accessed services, which they found very distressing. Julia was “getting quite significantly far on in the pregnancy, and there was that month of walking around pregnant pissed me off, that really did, that felt like, you know, it should have been an avoidable wait.”
Similarly, Ciara was close to U.K. limits, which meant she had to travel to another clinic. She recalled at her scan: they were saying later term … it shouldn’t have been this way and it's a more complicated procedure … it was basically 2 months later than it would have been if I had been able to, you know, make an appointment at a local clinic directly, myself … I was something like 22 weeks pregnant when I had the surgery instead of being 14 weeks, it felt like, a bit like everything was on hold, like you know, my whole life was on hold waiting for, waiting for this to be sorted.
Julia observed the sense of powerlessness she experienced in this process: “you don’t have that kind of money because you can’t, you don’t have the power to act on the decision yet.”
Subtheme 2.4: “Moaning and crying and f***ing needing things”
The journey itself was distressing. Julia travelled by ferry and felt: sick because I’m pregnant and the boat's flopping about all over the place and yes, I was feeling quite nauseous, I suppose partly from, you know, nerves and unhappiness and uh, you know, but also largely I guess from pregnancy…. The journey was horrific in that the boat was really full.
getting inside of the door of the hotel, I was in the toilet vomiting and getting cramps and various... and from there on, that was probably like, that was probably like 4 or 5 o’clock in the day and that would have went on until at least 4 or 5 o’clock in the morning … moaning and crying and f***ing needing things.
Being away from home compounded this. Sarah was so affected, she reported a trauma reaction to places that remind her of that ensuite bathroom: “if I ever went into a hotel bathroom that wasn’t very private, I would be brought back to that place.” Sharon was left waiting for a flight to go home postprocedure, having travelled early in the morning: “our flight wasn’t until let's say 11 o’clock that night … we were just sitting around the airport. I fell asleep on the chairs, it was just … nowhere to go.” Julia also had significant physical discomfort on the flight back, given that they hadn’t “taken into account the fact that I’d be effectively postsurgery flying back.”
Master Theme 3: “It's okay, it just wasn’t okay in Ireland”
This theme explores participants’ meaning-making, responses to others who made the same journey, and experiences with the abortion referendum in Ireland, plus their psychological shift from shame and secrecy to solidarity and righteous anger, and finally to power and autonomy. Participants acknowledged the importance of not feeling alone through storytelling around the referendum, and took action such as participating in research, wearing pro-choice messages in airports, and fundraising for the referendum.
Subtheme 3.1: “They were one of you, like”
Participants experienced a sense of solidarity and connection with others who had made the journey. In the clinics, both Ciara and Sharon noted the sound of Irish accents: “You could just hear the nurses if they were asking someone if they were okay and the reply of an Irish accent, and you kind of look over and you knew. They were one of you, like.” This was significant for Ciara: “There was kind of like a community of women going through a shit situation but talking it through.” The sense of kinship and compassion participants had for others lessened their sense of isolation and shame. Grace stated: I felt less like this isolated villain of, you know, there was other people here, this was okay, you know, it just wasn’t okay in Ireland … while the campaign was going on, where you know, having somebody in a “Repeal” jumper on the flights, I thought, you know, that was a powerful thing, especially if somebody was travelling and feeling maybe ashamed or isolated.
Participants referenced the pre- and postreferendum landscape. Sharon noted:
“I didn’t think I’d find that vote so hard, but I did because you were hearing all these girls’ stories and you’re like ‘Jesus yeah… that was me… I did that.’” The impact of storytelling through groups such as In Her Shoes and Termination for Medical Reasons (TFMR) was a significant component of stigma reduction for participants. Grace reported: I’ve had 13 years of never regretting it and knowing full well it was always what was right for me. Irish society has changed so much. You know, we have life stories, we have In Her Shoes, we have like TMFR telling genuine reasons like why this is an okay option for you in your life right now. But... and I have also since then met so many people who have such a similar story. So, there is an element of solidarity in that as well, like “shit we did this, like we were f***ing cast aside, and we were told that we were evil and we were wrong, and we couldn’t even consider this.”
Why I kind of wanted to do this is because of the 8th amendment, that was when I actually heard about other people and other people's views of going travelling over and just thought, “you can’t bottle things up forever so you may as well talk about it.”
Subtheme 3.2: “A righteous anger”
Another important component was participants’ anger in response to the injustice they experienced. Sarah felt that she “would have a righteous anger, even back then” in response to the way she had felt punished by others. Grace reflected on suffering sepsis after not feeling safe to seek aftercare at home: The shame and stigma of society had made me sick and so that was not going to f***ing happen to anyone else. Because it was unnecessary, it wasn’t that I felt I had been through the wars, it was that it was completely unnecessary. It was nothing but a societal notion and a Catholic shackle attached to society that had caused this, and that had done this to me from the inside. So, it just seemed like it was the absolute ultimate wrong.
By having that societal stigma … by believing from listening to society that I was wrong, that I was evil, that I was a murderer by having a social abortion and not playing the cards I was dealt and whatever, that it took some time, but it made me angry, and it made me angry enough to get active and to find these other women who felt the same as I did, and to make a difference and to make a change.
For Sarah, hearing of the death of Dr Savita Halappanavar “just enraged me.” Dr Halappanavar had requested and been denied an abortion for a nonviable pregnancy due to the 8th amendment in a Galway hospital on October 28, 2012, and consequently died from sepsis.
Subtheme 3.3: “Beginning to change”
After the referendum, Grace noted: I don’t think there's any greater change we could have made on the subject of abortion … It's going to be free for all. That matters so much to me especially since I was first, since I first got engaged, because it was a class issue.
The aftermath, in people's processing, translated to a shift from shame and stigmatisation to solidarity and compassion. Anne reflected that, I don’t think it's right that I should fear judgement, I don’t think it's right that I had to travel, all those kind of things, like if it were to happen to any of my friends or neighbours, or my daughter, or, I think I would want them to be able to access abortion at home and to be able to say “I’ve had an abortion,” you know? Without fear.
Julia spoke of the shift in the understanding of the complexity of people's situations, and how these are “complicated messy situations where there isn’t a right and a wrong, in the way that you have got, you know, the dichotomy of the slag and the virgin … and I think that's kind of beginning to change.” Similarly, Grace felt that a societal shift occurred in the context of the referendum: “part of it was that society moved along with me, that the stories were coming out.”
Discussion
The timing of data collection for this study provided a unique exploration of the impact of the referendum, in terms of people's processing of what happened to them under previous restrictive legislation. Participants experienced both unwanted pregnancy and forced travel, and reflected on their meaning-making of this as the 8th amendment was being repealed with the support of 66.4% of voters. We have categorised this Discussion in line with the power threat meaning framework (Johnstone & Boyle, 2018): what happened to participants, what was the impact on participants, and what sense did they make of it?
What happened to participants?
The specific phenomenon participants experienced was an unwanted pregnancy while living in a country where abortion was illegal, except under very limited circumstances. Prereferendum, unwanted pregnancy was difficult to navigate. Participants spoke about inaccessibility of information, fear of being caught, uncertainty around the legal implications of having an abortion, and the impact of cultural norms of that time.
Participants reported experiencing, anticipating, and internalising stigma. Stigma related to sexuality and abortion experiences is socially constructed, and reliant on inequality and power discrepancies (Kumar et al., 2009). Ireland is a primarily Catholic country; participants spoke of the impact of Catholic shame in shaping attitudes in the population. In Ireland, having sex outside marriage was seen as errant, immoral behaviour—indeed deserving of punishment. Unwanted pregnancies were seen by many as a consequence of a moral transgression; thus, abortions were a morally reprehensible rejection of a deserved outcome—consistent with past research where women felt undeserving of empathy (Kimport et al., 2016).
What was the impact on participants?
The lack of information and access to support in Ireland meant that participants were forced to remain pregnant long after they had decided to terminate, which is an element not much studied in past research. This was one of the worst aspects for many and, in some instances, this delay increased the complexity of the procedure and recovery time. This is consistent with previous findings which highlight how such restrictions may push people towards or past gestational limits (Gerdts et al., 2016; Ona Singer, 2020), and impact the type of procedure required, also increasing risk to the individual (Ona Singer, 2020).
Travelling abroad to access services meant participants were largely denied access to comfort and privacy. Our data include their vivid descriptions of long waits in clinics and airports, and complications associated with taking a flight or ferry home postsurgery.
Additionally, participants were stretched financially, and had to borrow money, disproportionately impacting those already disadvantaged (Bloomer & O’Dowd, 2014; Freeman, 2017). This attests to the argument that those who travelled to access abortion were not doing so as an active choice, but due to a lack of any other option (Inhorn & Patrizio, 2009; Kelly & Tuszynski, 2016; Ona Singer, 2020). Such travel also had negative physical and emotional implications (Kimport & Rasidjan, 2023). Participants noted that taking time off work, arranging childcare, and booking flights at the last minute made access a class issue. Thus, having an abortion was restricted to those who could afford to travel, and had the legal means to do so (Engle, 2022; Gilmartin & White, 2011).
Participants largely hid their abortion journeys from loved ones, colleagues, and their workplaces, navigating their pregnancies in secret. They concealed appointments, ultrasounds, and the need to travel, fearing stigma and legal repercussions, which led to much anxiety. And yet, participants had to disclose the abortion because of the need to travel, as observed by Kimport and Rasidjan (2023). Seeking support was fraught with challenges, including disclosing to those with negative views on abortion. Facing anticipated stigma and navigating clinic protests and uncertainty about legalities added to their distress. This fear and societal stigma, compounded by restrictive laws, hindered their access to healthcare, with one participant nearly losing her life due to complications. It was evident that societal shaming and restrictive legislation around abortion in Ireland impacted participants, who were terrified of being discovered, and were barriers to accessing healthcare.
What sense did participants make of their experiences?
The meaning-making of the event changed over time for participants. Recalling the time of their abortions, most remembered a sense of loneliness and isolation, being forced to leave home and make a journey that no one wants to make. Being forced to leave the county to access abortion care did not change the women's resolve to end the pregnancy, but it did make them feel as though they were being excluded and othered by the society they grew up in (Kimport & Rasidjan, 2023). Participants spoke about the stigmatised identity of women who experienced unwanted pregnancies and chose to terminate (O’Donnell et al., 2018), yet their meaning-making shifted in the context of the referendum—a move from shame and secrecy to compassion, and indeed anger in response to the lack of bodily autonomy in their own country.
Participants were inspired by the referendum, finding resonance in shared stories and the chance to voice their own. The build-up to and the outcome of the referendum were difficult for participants, but marked a shift from shame to empowerment, bolstered by solidarity and online movements like In Her Shoes (McDonnell, 2020). Motivated by injustice, participants engaged to varying degrees, from contributing to research to visibly supporting others by wearing pro-choice badges and jumpers, showing others that they were not alone. Participants described advocating for change to reclaim their identity and reject stigma. This aspect of our analysis adds a new positive note to the literature on forced abortion travel. Our analysis of participants’ meaning-making also adds substantively to our understanding of this phenomenon, building on a small amount of other important work.
Conclusion
Attending to the lived experiences of people who have travelled for an abortion in the context of highly restricted abortion access demonstrates the negative impacts of this journey. While the reaction to ending an unwanted pregnancy is often relief, the impact of the journey itself can be very different. The findings of this study strongly indicate the need for a reduction in wait time for those seeking abortions. They also indicate the need for clear, unbiased support services: accessible, local, and free. The findings support the need for safe zones around locations where people are accessing abortions. For those who still need to travel for abortions, there is a clear need for financial support and assistance with the practicalities of travel.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.