
Abstract
Policies about changing gender/sex on identity documents provide insights into definitions of gender/sex, and impact especially transgender and/or nonbinary lives. We investigated these on U.S. driver's licenses and birth certificates to understand variability in these policies, including in comparison to an earlier report in 2014, and to explore what kinds of “bio/logics” (decision rules rooted in biological or biologistic thinking) might be at play. Results show that the most common requirements in 2020 included proof of gender affirming surgery, a letter from a medical doctor, and hormone therapy. Compared to 2014, results showed an increase in requirements for hormone therapy and letters from therapists or medical doctors, and a decrease in requirements for gender affirming surgery. We highlight how this suggests a shift to “pubertal bio/logics”: rooting gender/sex definitions in secondary sex characteristics. This contrasts with previous requirements that pointed to “newborn bio/logics”: rooted in genital definitions of gender/sex affirmed by a surgico-medical authority. Both support policy framings of gender/sex as a biophenomenon, though with different impacts for trans and/or nonbinary livability. Our study provides insights into U.S. state definitions of gender/sex, and their multiple and contradictory biological views on gender/sex, with implications especially for transgender and/or nonbinary individuals’ lives.
The central concern in this article is recent transformations in understandings of gender/sex and gender/sex minorities, 1 alongside changes in policies about gender/sex markers on identity documents, and the requirements inherent in them. We use “gender/sex” to refer to phenomena where gender (socialization, social constructions, and social groups tied to femininity, masculinity, and gender diversity) and sex (biomaterial, bodily/physical, and biological/evolved phenomena tied to maleness, sex diversity, and femininity) are interconnected, entangled, or cannot be easily or at all separated (van Anders, 2014, 2015).
Defining gender and sex can seem like a mundane or obvious task to those who fit social norms. This includes gender/sex majorities1 who are cisgender and binary, that is, women and men whose gender/sex coincides both with the gender/sex they were given at birth and with binary conceptualizations of gender/sex. However, research has demonstrated that there is broad diversity in how people define gender and sex and what aspects they include in them, and this is especially true for gender/sex minorities, including trans, nonbinary, and/or intersex individuals and communities (Frohard-Dourlent et al., 2020; Hyde et al., 2019; Nagoshi et al., 2012; Schudson et al., 2019). Yet, even among majorities, there is broad variation in understandings of what gender and sex mean and include for both their self-understandings and their understanding of the world more generally (e.g., Kuper et al., 2012; Schudson et al., 2019). This reflects empirical reality, that gender and sex are each multifaceted (Fausto-Sterling, 2020; Hyde et al., 2019; Spelman, 1991; Tate et al., 2014; van Anders, 2015, 2022) and can even be understood in terms of their roles and functions (Currah, 2022).
Attempts to “get sex right” via one specific aspect of sex lie in contrast to understandings of gender/sex diversity. These attempts presume there is a singular, universal definition of sex (or gender/sex), and work to identify “the correct” definition of it for policy purposes (Fausto-Sterling, 2020; Kessler, 1998; Stryker & Whittle, 2006). They are usually made with the intention of excluding gender/sex minorities from some spaces, rights, or even the category of full personhood (Currah, 2022). Definitions of gender/sex thus matter for reasons that include theory and knowledge as well as material consequences, as they underlie policies that regulate gender/sex, which has implications for the regulation of actual people, especially those already marginalized (Stryker, 2006).
State policies about gender/sex classification have material impacts on individuals that are frequently unjust (e.g., Cruz, 2010; Greenberg, 1999; Kirkland, 2006; Levi, 2006). As Fischel et al. (2019) state, “Having the wrong sex designation creates obstacles to full and equal participation in whatever egalitarian ideal of social and civic life one holds” (pp. 94–95). Denying people access to changing their gender/sex markers can impact many levels of their lives including health care access and the ability to travel, work, and engage in many public activities without being “outed” and facing direct or indirect consequences (Currah, 2022).
Policies about gender/sex are largely grounded in cisnormative and binaristic assumptions. These include that people have one gender/sex (female/girl/woman or male/boy/man) that is assigned to them at birth and that defines their being. The singularity and static character of this version of gender/sex is one reason why gender/sex markers are on identity documents: identity is seen as a function of gender/sex, and gender/sex is seen as foundational and intrinsic to personhood (e.g., Butler, 1990; Martin & Mason, 2022; Stryker, 2006). However, people experience shifts in their gender/sex and/or the markers that accurately represent their gender/sex. And people experience their gender/sex in ways that do not fit gender binaries, such that identity options of “female” and “male” are incomplete. Increasingly, and as a result of activism and advocacy for social change, recent policies regarding gender/sex markers reflect the possibility of changes in these markers. In this way, many policies make space for the reality that gender/sex markers on identity documents can, do, and need to change (even if only once) to reflect the people they represent and/or regulate.
Changes in gender/sex markers are experienced by many people over their lives, including a number of groups that are internally heterogeneous and sometimes overlapping. One group that can experience shifts in gender/sex markers is transgender people and/or people who have transitioned or accessed gender affirming care, that is, those whose gender/sex is not the gender/sex they were assigned at birth. Another group that can experience such shifts is nonbinary people, whose gender/sex is and/or includes existences beyond one of the two normative categories from a gender binary of woman/girl versus man/boy. Yet another group that can experience these shifts is intersex people, who have aspects of sex that were/are not seen as typical of femaleness/girlhood/womanhood or maleness/boyhood/manhood and are often subject to unwanted and/or nonconsensual medical treatment. Some people exist at the nexus of multiple of these and other groups—and, of course, along with other intersecting axes of oppression or privilege (Cole, 2009; Collins, 2000; Crenshaw, 1989).
The state policies that allow for changes in gender/sex markers on identity documents typically have a set of requirements that individuals must meet to access them. These requirements reveal the de facto definitions of gender/sex of the states that make these policies or, as Paisley Currah (2022) describes it, “sex is as sex does”, referring to the ways that what sex is can be understood by what states use definitions of sex to do (and to whom). Yet policies change over time, as states participate in—or, more rarely, exit—the wild goose chase of attempting to get sex right. These changing requirements have relied on varied aspects of sex, and this reveals the contingency of gender/sex definitions, their construction, and their meaning.
How bio/logics inform gender/sex definitions
In an attempt to define gender/sex for identity documents, governments typically pick and choose specific but differing aspects of sex and, rarely, gender. The logics underlying these decisions can be understood by their functions and state agency goals (Currah, 2022; Spade, 2008). They can also be understood by decision-making processes, like “bio/logics” (van Anders, 2014; van Anders et al., 2014). Bio/logics are “implicit and/or explicit reasoning guides informed by features thought to be natural, corporeal, evolved, and material (e.g., sex over gender)” (van Anders, 2014, p. 33). They refer to biological decisions rules, or rules for making decisions about social phenomena—like gender/sex—that are rooted in biologism. Biologism refers to the belief or ideology that biology is the best and/or only way to know about life-related phenomena (van Anders, 2022). It differs from biology, the science of life-related phenomena, since biology is merely the study of biophenomena and not a positioning of it as superior to other epistemologies, or ways of knowing. Although biologism has a singular goal, it has multiple iterations. When these various iterations are used to inform or justify decision-making about social categories, groups, and rights, they function as bio/logics.
Bio/logics are used in multiple and often conflicting ways, and this incoherence and inconsistency can function to destabilize and undermine the rights of gender/sex minorities (Spade, 2008; van Anders, 2014, 2022; van Anders et al., 2014). For example, legally recognized gender/sex markers have sometimes been overturned or ignored in legal court cases regarding inheritance rights (Greenberg, 2000). These decisions have tended to reflect “interior bio/logics,” wherein biological aspects related to sex that are seen as most “inside” and/or immutable are privileged over other aspects of sex. This makes for a privileging of genes (like XY or XX chromosomes) over aspects of sex like uteri (which are unalterable but removable), which are themselves privileged over other aspects of sex, like genitals (which are alterable).
Another set of bio/logics—“trace bio/logics”—privileges aspects of sex present early in human development as determinants of gender/sex (van Anders, 2014; van Anders et al., 2014). These bio/logics ascribe an immutability or fixity to aspects of sex like genitals or gonads (e.g., ovaries, testes), treating them as present regardless of a current absence (e.g., with ovariectomy). In this way, trace bio/logics render gonad removal or genital surgeries irrelevant to gender/sex categorization because their “original” form is treated as always and still present. These so-called traces of sex are thus taken as sex itself, including in material attributions, as in the belief that early hormones unalterably affect gender/sex and/or sexual development, or conceptual attributions, as with born-genitals used to define individuals for the purposes of gender/sex and/or sexual “complementarity” between women and men (Butler, 1990). As with interior bio/logics, trace bio/logics are used in some legal contexts (e.g., case law) to overturn gender/sex recognitions in other legal contexts (e.g., identity documents).
A third set of bio/logics is “newborn bio/logics.” Newborn bio/logics reflect the medicalized and typically Western ways that newborns are sexed—that is, via a medical doctor (or other health professional) viewing the baby's genitals and deciding what these mean for the individual's lifetime gender/sex. This process is transferred into later life, thereby (re)naturalizing adults’ gender/sex via genitals. There was clear evidence that these were the foundation for definitions of gender/sex on U.S. identity documents in 2014 (van Anders et al., 2014). Accordingly, requirements for shifting gender/sex on birth certificates and driver's licenses largely required genital surgery and/or a surgico-medical authority to “authorize” a person's genital state (van Anders et al., 2014). Other requirements like a therapist letter, hormone therapy, or genetic testing were vastly less common, if required at all. Thus, shifts in adults’ gender/sex markers on identity documents followed the sexing process in newborns as closely as possible: that is, by having a medical authority attest to the person's genital configurations as evidence of gender/sex for categorization and identification purposes.
Researchers have since identified an additional form of bio/logics: “cognitive bio/logics” (Frohard-Dourlent et al., 2020). These naturalize gender/sex not in surgico-medical authority’s sanction, genitals, or the most immutable aspects of sex per se, but in brains. Cognitive bio/logics allow for an internal sense of gender/sex to matter, though one that is understood as being located neurally. Research suggests that some gender/sex minorities will explain their self-understandings in this way (Frohard-Dourlent et al., 2020), which can naturalize and reduce gender/sex to bodies. How this plays out in state policies remains to be empirically addressed.
These various and varied bio/logics open up and foreclose legal recognition, state recognition, and thus some understandings of full personhood for gender/sex minority existences in the US. They are based in cisnormative understandings of gender/sex and also regulate a set of cisnormative transnormativities, meaning that they promote the idea that there is one right or natural way of being transgender. In addition, these bio/logics promote the idea that there is one right reason or explanation for shifts in gender/sex markers on identity documents. For example, interior and trace bio/logics generally foreclose gender/sex shifts altogether on documents and therefore, to some extent, for people. In comparison, newborn bio/logics create space for gender/sex shifts, though arguably those that occur only once and in one “direction” and in such a way that naturalizes and corporealizes gender/sex to bodies and requires considerable financial, temporal, and health resources. Though surgery can obviously happen more than once, newborn bio/logics seem to have the clear intention of rendering gender/sex permanent such that additional or future shifts are preempted, and gender/sex is positioned as singular and unshifting. This precludes gender/sex fluidity that might also need to be recognized on identity documents that have gender/sex markers.
Cognitive bio/logics also open up space for gender/sex shifts. And, by locating gender/sex in the brain, they arguably interface with trace bio/logics to regulate gender/sex as well. Though neural structures can reflect experience and plasticity, cognitive bio/logics do not seem to reflect this understanding of the brain. They seem to be based in the idea that someone has always been the gender/sex they are; gender/sex has always been in their brain or their brain has always had the same gender/sex. In other words, someone's gender/sex was set early, permanently, and biologically, just in the brain rather than in other bodily locations of sex aspects.
Much has changed since the requirements for changing gender/sex markers were reviewed in 2014 (van Anders et al., 2014). That research indicated that newborn bio/logics were used as the basis for definitions of gender/sex in policy about marker changes on U.S. identity documents. For example, Colorado, amongst other states (e.g., California, SB 179 [2017–2018]), has allowed an “X” marker on birth certificates since 2018 (HB18-1046 [2018]). There has also been increasing public recognition and awareness of transgender, nonbinary, and/or intersex identities, existences, and experiences (Minkin & Brown, 2021). These changes may mean that newborn bio/logics no longer undergird gender/sex definitions as reflected in policies about changing gender/sex markers on U.S. identity documents. However, while increased awareness has sometimes led to greater understanding and access to care, it has—in conjunction with transphobia and cisnormativity—also led to restricted access to care, along with increasing backlash and attacks on transgender people and other gender/sex minorities. Still, advocacy by trans people, nonbinary people, and/or intersex people among others has aided in producing changes to state policies about gender/sex markers on identity documents (Koch-Rein et al., 2020).
Our interest in this article is in examining similarities and differences between bio/logics in contemporary patterns and those reported in 2014 (van Anders et al., 2014). How are these reflected in policies and definitions of gender/sex for changing markers on U.S. identity documents? What do these reveal about U.S. state definitions of gender/sex? And, are they still undergirded by newborn bio/logics or have others come to light along with other shifts? Finally, have these definitions moved beyond biologisms and attempts to “get sex right”?
We focused on driver's licenses and birth certificates because of how common these are, and how frequently they are used for other purposes. Other documents, like passports, are clearly important but they are held by a relatively small portion of people in the U.S. A deeper understanding of these policies and the thought processes that underlies them can have profound implications for cultural understandings of gender/sex and the safety and rights of gender/sex minority individuals. These understandings extend to policies in countries that have different gender/sex marker procedures than the U.S. (e.g., the United Kingdom, India), including in countries where the change is not permissible (e.g., Jamaica, the Philippines). As Currah (2022, p. xvi) notes about gender/sex and state policies about identity markers: “We don’t know what a politics of resistance would look like until we understand what it is we’re resisting.”
Method
We examined the requirements for gender/sex markers on birth certificates and driver's licenses issued by state governments in the U.S., following van Anders et al.’s (2014) inquiry into how gender/sex is defined and regulated in the U.S. In the U.S., identity documents are issued not at the federal level but at the level of state (defined as “a legislative authority that is tasked with governing a geographically delimited population”; van Anders et al., 2014, p. 176). We gathered information about the gender/sex markers on birth certificates issued by all 50 U.S. states, as well as the District of Columbia and New York City, which issue their own certificates. For driver's licenses, we focused on 51 states (the 50 U.S. states plus the District of Columbia). We ended our data collection in August 2020. 2
In 2020, information about what was needed to change gender/sex designations on legal documents was much more accessible than it was for van Anders et al. (2014). In contrast to the prior work, which mainly required collecting data by contacting state governments, our current team was able to find information directly on most government websites. When possible, we sourced data from these sites, but when there was no information, we contacted the relevant agency (e.g., a state's Department of Health or equivalent for birth certificates; the state's Department of Motor Vehicles or equivalent for driver's licenses) directly via phone or email (seven states for birth certificates and seven states for driver's licenses). When possible, our team cross-checked the information we sourced from government websites with written policy that we found from online searches. If there were discrepancies between the information online and official written policy, we used the information from the written policy in our data. The first and second authors collected data from these primary sources and ensured consistency of the data together.
We collected data on these items following van Anders et al. (2014): court order for gender/sex change; court order for name change; proof the individual was living as the requested gender/sex full time; whether declaration from a surgeon, a physician/medical doctor, or therapist was required; hormone therapy; and gender affirmation surgery (top and/or bottom). During our data collection, we found it helpful to separate positive requirements into “Yes, mandatory” for cases when a certain item was required, and “Yes, as an option” for cases when change to the gender/sex marker could be made differently according to a list of requirements (e.g., proof of surgery or a therapist letter); in the list of requirements, there would need to be compliance with at least one requirement. We used “No” either when there was a negative requirement for an item or when the requirements were clear enough that it was evident that item was not required. Finally, since nonbinary markers are now a possibility in some states, we also collected data on the options for gender/sex beyond binary markers (i.e., beyond male/man or female/woman).
Each state had policies concerning changes to gender/sex markers on both identity documents, and there were several nuances beyond the stated requirements. For example, not all states made it clear whether or not a requirement from a list was enforced via supplementary documents from other authorities (e.g., whether someone needed an external attestation to “prove” a specific criterion). States had a combination of positive requirements (“you do need this requirement”) and, less frequently, negative requirements (“you do not need this requirement”).
There were also “feeder” requirements in some states, wherein changes to driver's licenses relied upon birth certificates, in effect making the requirements for birth certificates the de facto requirements for driver's licenses. Following van Anders’s (2014) methodology, we documented driver's license requirements that existed via birth certificate requirements separately. Therefore, if birth certificate gender/sex marker change was required for driver's license change, we included the birth certificate requirements in the “Require BC for change on DL” row (BC = birth certificate, DL = driver’s license; see Table 1). There were likely implicit feeder requirements in many if not all states, such as when therapy/counseling was not indicated as a requirement but might be required for hormone therapy or gender affirming surgery, which was listed as a requirement. This is a significant issue but not one we could ascertain, so we did not include it in our analysis.
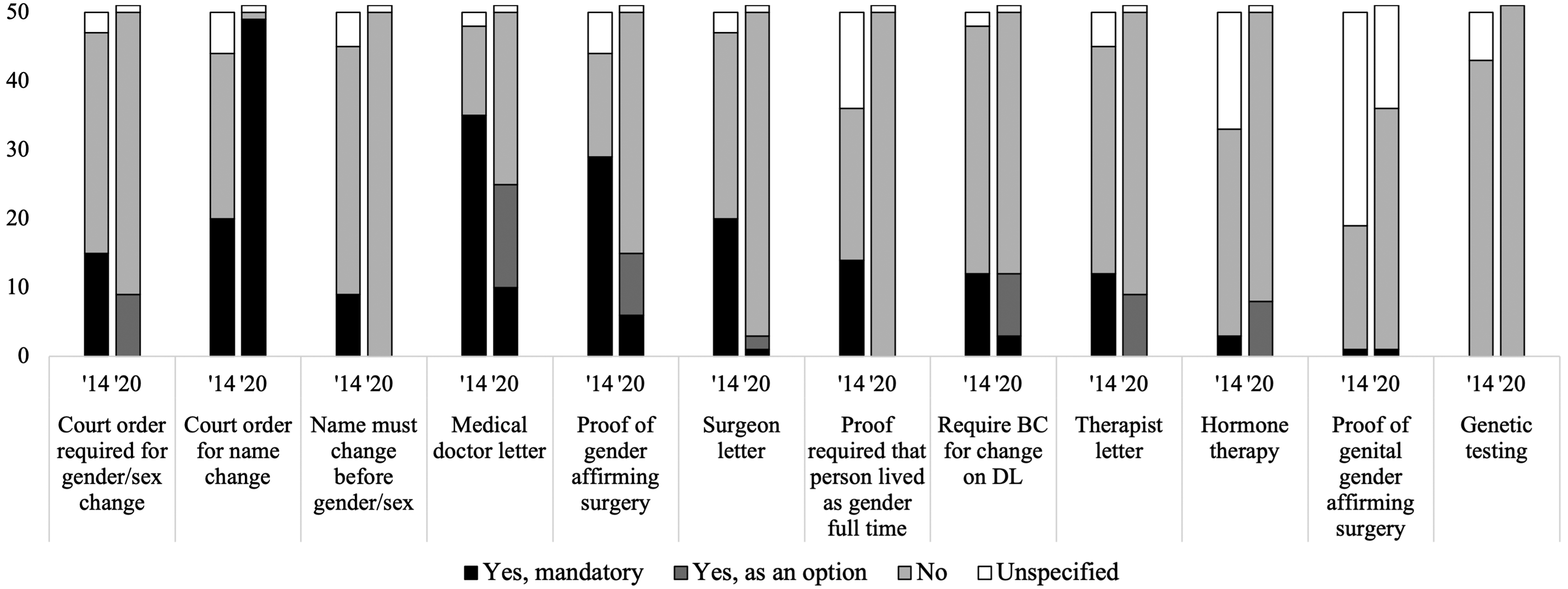
Requirements for gender/sex marker change on driver's licenses (DLs) in 2014 and 2020
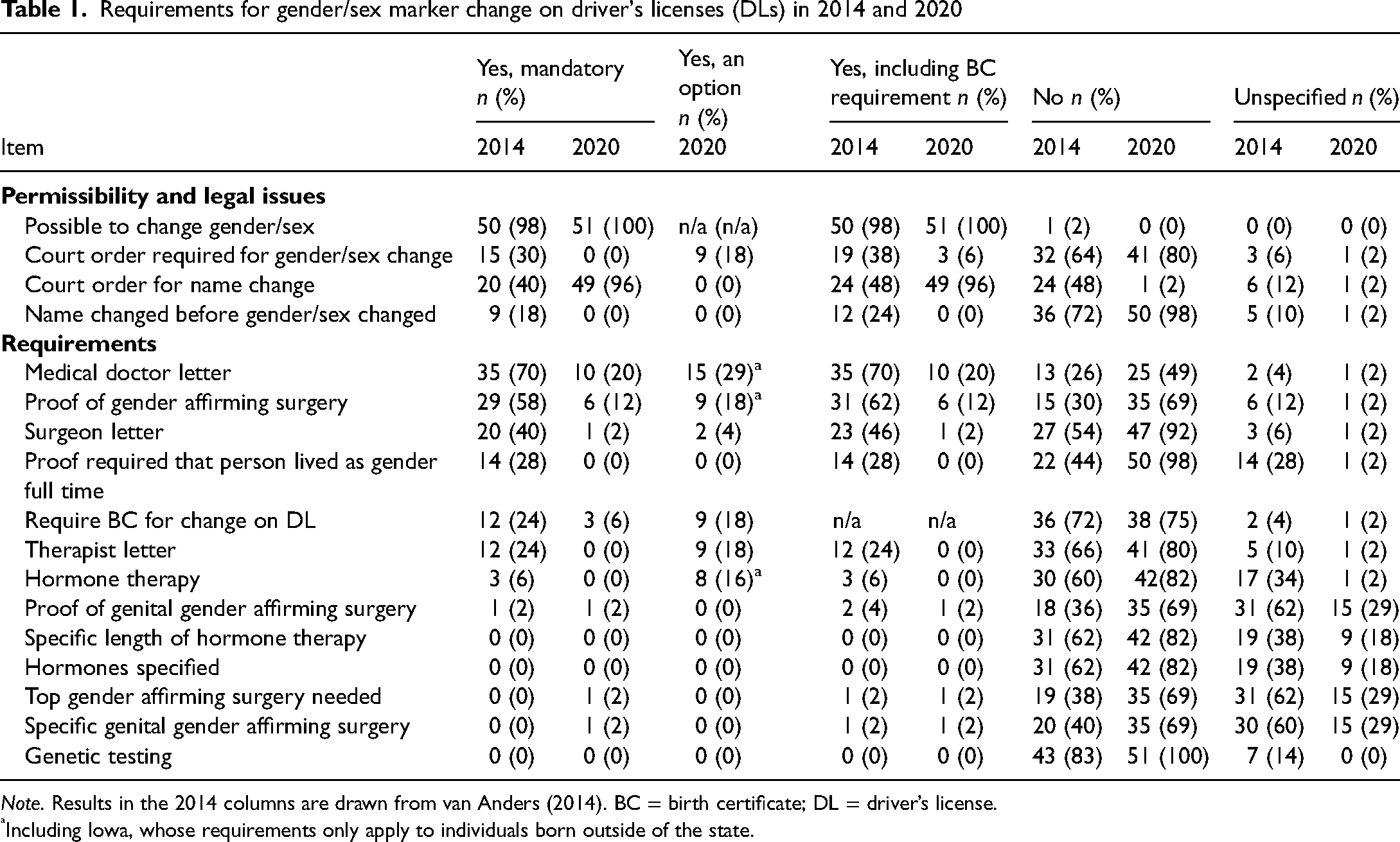
Note. Results in the 2014 columns are drawn from van Anders (2014). BC = birth certificate; DL = driver’s license.
Including Iowa, whose requirements only apply to individuals born outside of the state.
Results
Birth certificates for 2020: Requirements for changing gender/sex markers
The requirements for changing gender/sex on birth certificates were variable and inconsistent by state (see Table 2 and Figure 1). The most consistent finding, however, was that the vast majority (94%) of states allowed a change to gender/sex markers on birth certificates, with three states preventing it (Idaho, Ohio, and Tennessee). For all following results, percentages reflect the proportion of states that allowed changes to gender/sex markers on identity documents (i.e., the denominator was 49, not 52).
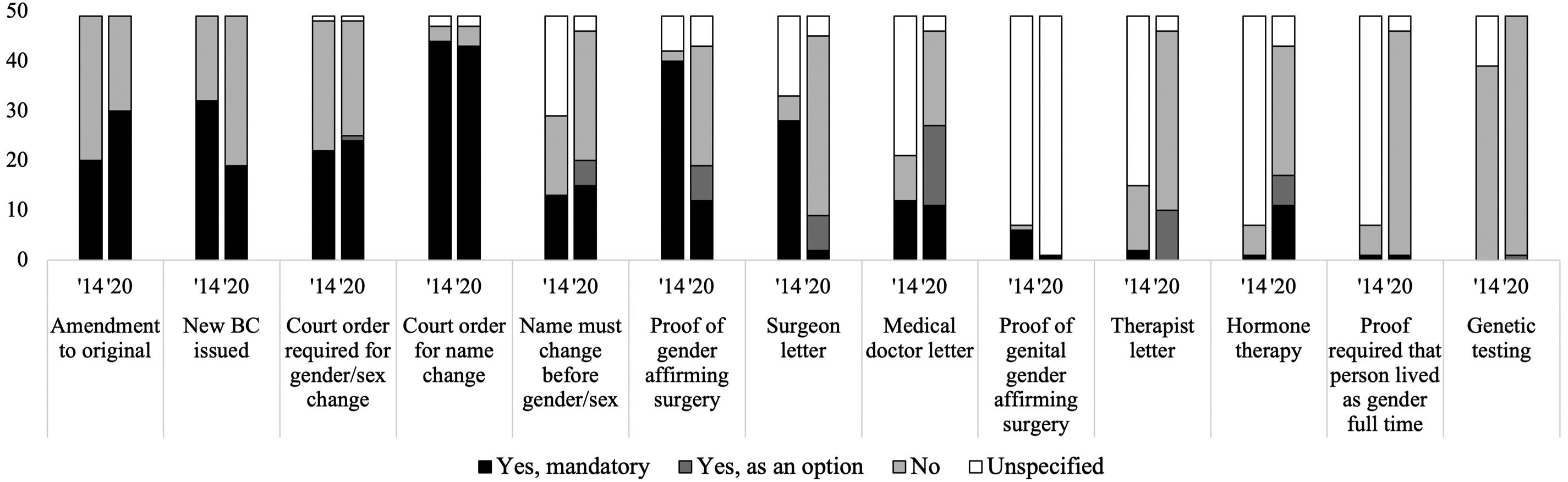
Variables of interest for gender/sex marker changes on birth certificates (BCs) in 2014 (’14) and 2020 (’20).
Requirements for gender/sex marker change on birth certificates (BCs) in 2014 and 2020
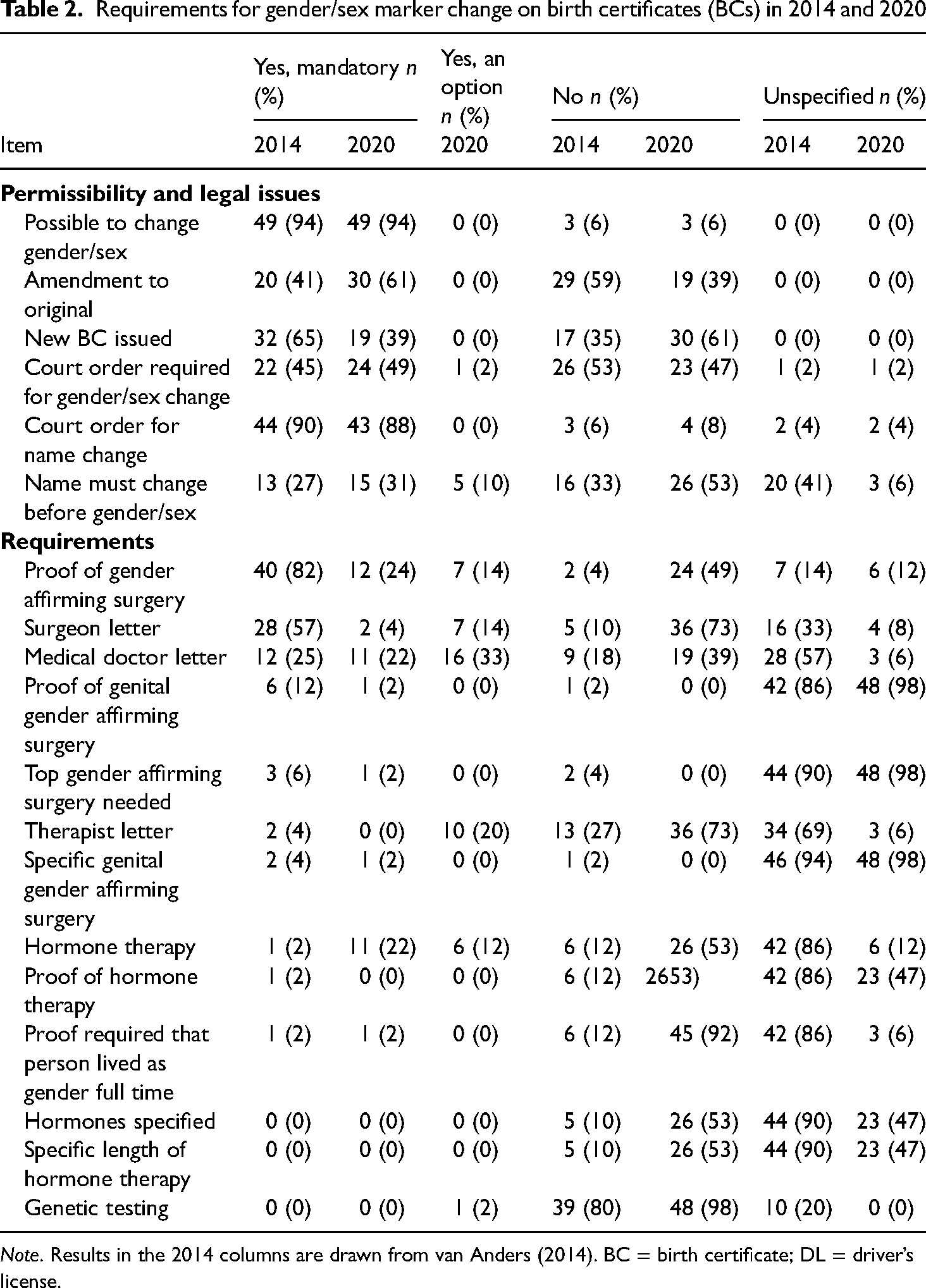
Note. Results in the 2014 columns are drawn from van Anders (2014). BC = birth certificate; DL = driver’s license.
For the gender/sex marker options (see Figure 2), where someone would list the gender/sex identity change they were requesting, the majority of states (69%) did not specify options or provided a fill-in-the-blank one, making it unclear if states would honor the gender marker written in. The remainder of states either provided only female/male options (14%) or male/female/nonbinary (e.g., “X”) options (16%). Of the 49 states allowing a change, 61% amended the original birth certificate and 39% issued a new one, and almost half (49%) required a court order for the gender/sex marker to change.
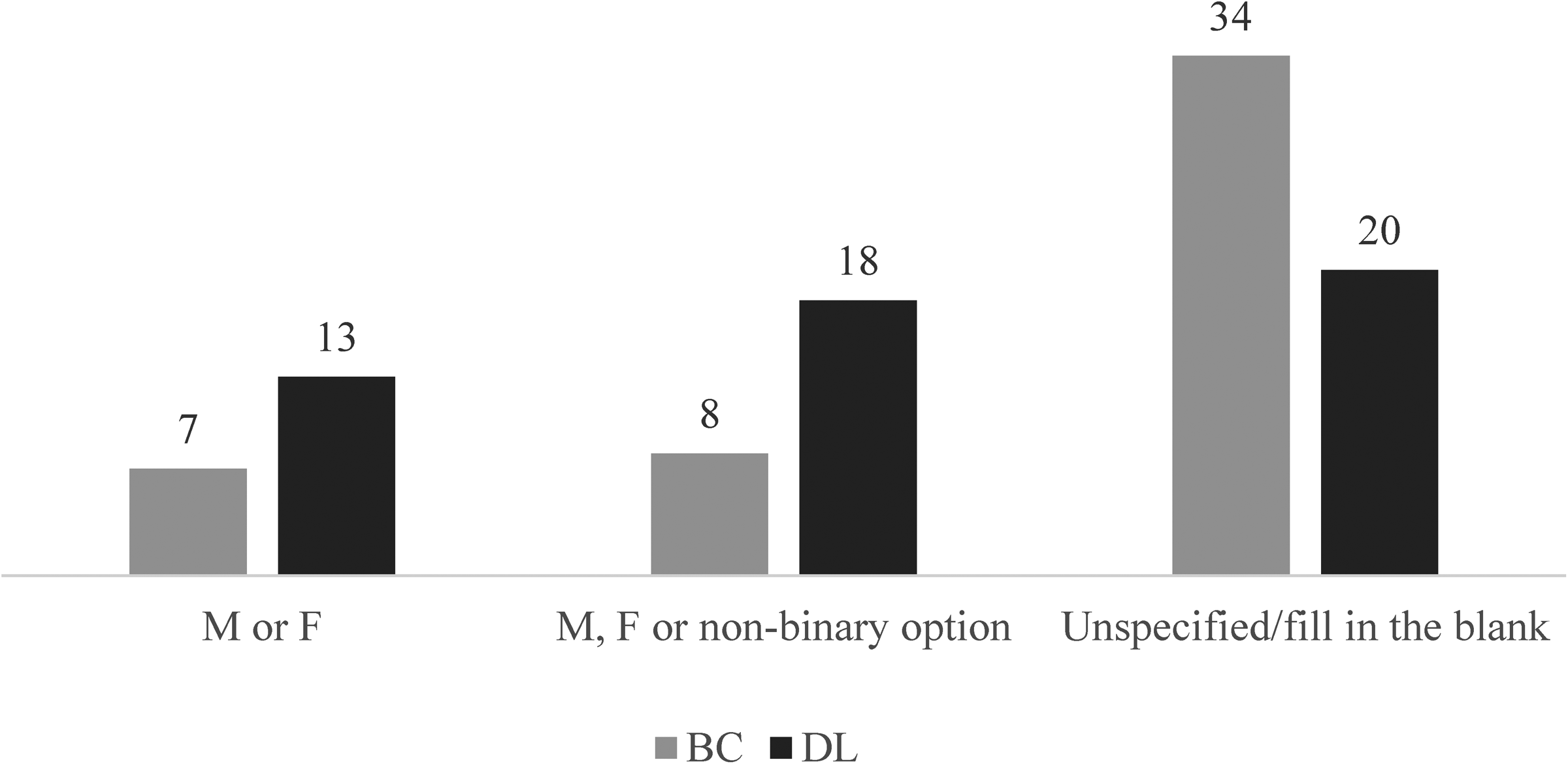
Possible gender/sex markers on birth certificates (BCs) and driver's licenses (DLs) in 2020.
The most common “Yes, mandatory” state requirements for changing gender/sex markers on birth certificates were, in descending order, proof of gender affirming surgery (24%), a letter from a physician (22%), and hormone therapy (22%). Yet all of these also were commonly not required. Proof of gender affirming surgery was not required in 49% of states, a letter from a physician was not required in 39% of states, and hormone therapy was not required in 53% of states. Other items were commonly not required, including a letter from a surgeon in 73% of states and a letter from a therapist in 73% of states. And, almost no states required genetic testing or proof that a person was living as their gender full time. Two items were only presented as an option: a letter from a physician in 33% of states and a letter from a therapist in 20% of states.
Driver's licences for 2020: Requirements for changing gender/sex markers
All 51 states (the 50 U.S. states plus the District of Columbia) allowed gender/sex marker changes on driver's licenses. The largest number of states did not specify options for gender/sex markers (39%), followed closely by those that provided female/male/nonbinary options (35%), followed then by only female/male options (25%; see Figure 2). In terms of feeder documents, only three states (6%) required a birth certificate, with 18% listing this as an option and 81% of states not requiring a court order. The court order was an option, however, for 18% of states (see Table 1 and Figure 3).
Variables of interest for gender/sex marker changes on driver's licenses (DLs) in 2014 and 2020.
The most prevalent requirement for changes to a driver's license was a court order for a name change for 96% of states. Following, a letter from a medical doctor was the most prevalent requirement, with 20% of states having this letter as a mandatory requirement and 29% of states listing it as an option. Concerning gender affirming surgery, 12% of states listed it as a requirement and 18% as an option. Surgeon letters were similarly not commonly required as only 2% of states required them and 4% provided them as an option. In addition, therapist letters were never required for changes, but 18% of states listed them as an option. No states called for the following requirements as mandatory or as optional: proof that a person lives in their gender full time, hormone therapy, and genetic testing.
Birth certificates versus driver's licenses in 2020: Comparing gender/sex marker requirements
There were fewer and less stringent requirements for changes to driver's license compared to birth certificate. For example, though most states allowed changes to gender/sex markers on driver's license, this was not the case for birth certificates (though only three did not). Moreover, no requirement was more common for changing gender/sex markers on driver's licenses than for birth certificates. This was particularly evident when observing surgico-medical requirements for gender/sex marker change. For example, 24% of states required surgery for changing gender/sex markers on birth certificates (with an additional 14% listing it as an option) but only 12% for driver's licenses (with an additional 18% as an option). Similarly, 22% of states required a medical doctor letter for changing gender/sex markers on birth certificates (with an additional 33% listing it as an option), but only 20% for driver's licenses (with an additional 29% listing it as an option). And 22% of states required hormone therapy for changing gender/sex markers on birth certificates (with an additional 12% listing it as an option), but no states required it for driver's licenses (see Table 1 and Figure 3).
There were some similarities in requirements to change gender/sex markers on birth certificates and driver's licenses. For example, no states required therapist letters, and similar numbers listed it as an option for birth certificates (20%) and driver's licenses (18%). No states required the fulfillment of extraneous requirements such as proof of living as gender full time or genetic testing for either document.
Gender/sex markers on identity documents in 2020 versus 2014
Changes over time were evident for gender/sex markers on both birth certificates and driver's licenses from 2014 to 2020. This included whether new birth certificates were offered following a change in gender/sex markers, with a decrease from 65% in 2014 to 39% in 2020. Changes in feeder documents (i.e., birth certificates being used as a prerequisite document for driver's license changes) were also notable. Lastly, in 2014 no states had a nonbinary gender/sex marker option, whereas 35% did in 2020.
Changes over time were also clearly visible for the requirements for changing gender/sex markers on birth certificates. One notable difference was a reduction in the number of states requiring surgery in general from 2014 (82%) compared to 2020 (24%), or a surgeon letter (57% vs. 4%, respectively). Another was that more states accepted a letter from a therapist for changing gender/sex markers in 2020 (20%) compared to 2014 (4%). And hormone therapy became a more widely available requirement with 22% of states making it mandatory in 2020, while only 2% of states required it in 2014 (see Table 2 and Figure 1).
Driver's licenses also showed changes over time in the requirements for changing gender/sex markers. Some of these paralleled changes for birth certificates. For example, 40% of states in 2014 required a surgeon letter but only 2% required it in 2020. This mirrored a decrease in medical doctor letters being required, with a decrease from 70% of states in 2014 to 20% in 2020. Therapist letters also became less commonly required, from 24% of states in 2014 to 0% in 2020 (with 18% putting them as an option). And, the requirement that a person live as their gender/sex full time decreased from 28% to 0% of states (see Table 1 and Figure 3).
Discussion
In this paper, we reported on requirements for changing gender/sex markers on birth certificates and driver's licenses across U.S. states in 2020, in part to explore what kinds of bio/logics, if any, might be apparent. We also explored these patterns in relation to what van Anders et al. found in 2014, finding that requirements for changing gender/sex markers have generally become less onerous, with improvement in some areas and evidence of some notable change.
For changes to gender/sex markers on birth certificates, there were decreases in the number of states requiring surgery and letters from surgeons. For changes to gender/sex markers on driver's licenses, there were also decreases in the number of states holding specific requirements, and this included the use of the birth certificate as a feeder document. In addition, for driver's licenses, there were more gender/sex marker options beyond binary ones for the identity document. It appears that the U.S. state definitions of gender/sex have progressed in some ways to open up rights, but also share some of the same restrictive foundations. For example, the reduction in surgico-medical requirements like surgery and physician letters decreases restrictions, but the continued medicalization of gender/sex changes and rooting of gender/sex in biologies (e.g., by requiring hormone use) reveal similar bio-essentializing of and external authority for conceptions of gender/sex as observed in 2014.
Our results demonstrate that bio/logics continue to be a rationale for gender/sex marker changes on birth certificates and driver's licenses in the US. However, the patterns point to a shift in what kind of bio/logics are at play. In 2014, newborn bio/logics seemed to be influential, with requirements for genital surgery and medical attestation of this, paralleling how gender/sex is assigned at birth. The current pattern of results from 2020 points to a different set of bio/logics: adolescent or pubertal bio/logics. Requirements for changing gender/sex markers in 2020 were much less focused on surgery and genitals but were heavily focused on bodily changes through hormones and medical authority attestation. Thus, there is still a need for a physical change to change gender/sex markers, but it is now focused more on what are often called secondary sex characteristics (as with what is most often called puberty) than primary sex characteristics (as with what is often called genital differentiation).
As an example of the shift to pubertal bio/logics, hormone therapy was only required for changes to gender/sex markers on birth certificates in 2014 in 2% of states; in 2020, this increased to 12% of states having it as an option and 22% requiring it. Though the requirements for hormone therapy likely rely on a binaristic logic, hormone therapy does not have to follow a binary treatment path. For example, a person can use hormones, then stop and start again as it fits them or their needs, assuming the financial resources or health care to do so. And hormones might also be a gender affirming approach of more interest to nonbinary people than surgeries (Richards et al., 2016). The shift from genitals and surgico-medical authority to hormones can thus be seen as somewhat progressive or opening up more space for trans and/or nonbinary livability, given that secondary sex characteristics are more plastic in some ways than primary sex characteristics, and open to more people beyond the gender/sex binary. Karhu (2022) has argued that hormone therapy, gender affirming surgery, and gender dysphoria diagnoses are tools to increase trans and/or nonbinary livability even while they are regulatory practices decided by each state that normalize the medicalization of trans and/or nonbinary identity. The shift towards pubertal bio/logics in some ways reduces the rigidity of these medical standards, increasing trans and/or nonbinary livability relative to the existing status quo (van Anders, 2022).
Yet, the conflation of changes in hormones with changes in gender/sex continues to locate gender/sex and gender identity in physical bodies. In a cisnormative society, gender/sex is often assumed to be communicated by physical appearance (Bettcher, 2007). As people's genitals are not often seen by others, physical markers such as facial hair or breasts often matter more for everyday gender/sex attributions (Dozier, 2005). Our results highlight that current public policy in the U.S. reinscribes this emphasis on secondary sex characteristics as conveyors of gender/sex. Perhaps the shift from primary to secondary sex characteristics is the new iteration of “getting sex right,” leaving some flexibility and even increasing it in some ways, but also still reflecting and (re)inscribing cisnormative ideas of gender/sex.
Our findings also indicate that U.S. public policy still relies on professional authority for gender/sex marker changes on identity documents. In van Anders et al.’s 2014 report, this authority was primarily vested in surgeons and doctors. The present data show that therapists are increasingly seen as appropriate authority as well (20% in 2020 for birth certificates, up from 4% in 2014). This could represent a shift toward cognitive bio/logics (Frohard-Dourlent et al., 2020), as therapists generally assess and work with mental health and personality rather than facilitating changes to people's physical bodies. Further, therapists are often more accessible than doctors and surgeons (there are more of them, they can be cheaper, etc.). Accordingly, vesting authority for gender/sex marker changes in therapists could make obtaining gender/sex marker changes easier. However, these requirements for a professional letter continue to locate the authority over individuals’ gender/sexes outside of themselves, limiting people's agency in their own transition (Ashley, 2019a).
Interestingly, though therapist letters are not required to change a gender/sex marker on birth certificates and driver's licenses in most states, they may be a prerequisite for more common requirements like hormones or surgeries in many states. These letters often must state that the person has been diagnosed with gender dysphoria (Ashley, 2019a, 2019b; Stroumsa, 2014; Stroumsa et al., 2022). Using gender dysphoria as a gatekeeping mechanism prioritizes psycho-medical authority over lived experiences. Trans scholars have often criticized the emphasis placed on gender dysphoria diagnoses in general (Ashley, 2019a, 2019b; Lev, 2013). This is because, though the diagnosis can be helpful in some ways (e.g., insurance coverage for transition-related healthcare), it also can marginalize trans people, limit autonomy, and pathologize gender/sex diversity.
Another noteworthy pattern in our results is that there has been an increase in the number of states that amend birth certificates rather than issuing new ones. Unlike new documents, amended documents contain a record of the change. In some ways, this pattern is at odds with the increasing opening up of requirements described above, since it naturalizes birth gender/sex as something to be recorded or permanent. It may be that an increase in amended birth certificates reflects anxieties that a person's gender/sex history must be as available to state institutions as their actual or present gender/sex. That is, government surveillance systems may view issuing new birth certificates without a history of the change as problematically “concealing” birth gender/sex (Moore & Currah, 2015), given that their stated intention may include reflecting their conceptualizations of reality. In a similar way, the increase in court ordered name changes for driver's licenses may reflect governments’ way of policing gender/sex indirectly by requiring a certain level of “proof” (via name changes) of gender/sex transition. These requirements position gender/sex assigned at birth as durably meaningful throughout a person's life even if they attest otherwise, thereby prioritizing government surveillance over individual or community agency.
Finally, we note that there are many kinds of identification procedures, of which we included only two kinds: policies about driver's licenses and birth certificates. But there are clearly other documents that matter for gender/sex markers—and trans, nonbinary, and/or intersex livability—including passports and more. In addition, while policies are intended to shape practice, the two are not always synonymous. Thus, whether required documents are actually sufficient for gender/sex marker changes to occur each time they are requested is not something our data speak to. Whether identity documents are accepted with nonbinary markers is another matter. And, as we reviewed earlier, differing and competing sets of bio/logics mean that, in practice, changes in gender/sex markers on identity documents are not always accepted or given precedence (Spade, 2008). Thus, while we see our findings about policies as being suggestive of opening up possibilities (albeit with restrictions) for practice and lives, the one does not necessarily translate into the other.
Conclusion
Despite a shared focus on underlying assumptions about biologies and external authority over gender/sex between 2020 and 2014, it seems that state understandings of trans and/or nonbinary people and requirements for gender/sex marker change have shifted. Arguably, this shift from newborn bio/logics to pubertal bio/logics reflects a more progressive approach, even as it is still prescriptive, limiting and limited, and reflective of other normativities. There continue to be changes, even since we collected data for the present paper. For example, now almost half of states allow nonbinary options for driver's licenses and a third for birth certificates (Migdon, 2022).
It is unclear what exactly has been the driving force of such rapid changes over this 6-year period, though it is likely a combination of advocacy work by trans, intersex, and/or nonbinary people and communities; changes in public and media perceptions and representations of gender/sex; and political motivations. Regardless of why the transformation in the set of logics and the increase in amended birth certificates, therapist letters, and gender/marker options have occurred, change efforts are still needed. Many government systems, such as administrative and healthcare systems, fail to recognize and incorporate gender/sex diversity, with negative effects on the people who must navigate them (Donald & Ehrenfeld, 2015). And, indeed the question of state control over gender/sex underlies questions about which logics or requirements should be used to gatekeep changes to gender/sex markers (Currah, 2022; Spade, 2008). Should the state be marking people's gender/sexes or determining what is necessary and sufficient for changes to gender/sex markers? Still, we hope our update on gender/sex marker policies, and identification of new bio/logics as a foundation for these, can provide further understanding of how gender/sex is conceptualized and enacted, as well as the ways these systems define gender/sex and their effects on people's everyday lives—especially trans, intersex, and/or nonbinary people—ultimately informing a more just public policy.
Footnotes
Acknowledgements
The authors would like to thank Carolina de Barros and Benjamin Nguyen for help with data management.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was undertaken thanks to funding from the Canada 150 Research Chairs Program to S. M. v. A. Funding also came from the Rackham School of Graduate Studies at the University of Michigan to W. J. B.